LPN ATI fundamental exam
Total Questions : 53
Showing 25 questions, Sign in for moreA nurse is contributing to the plan of care for a client who has a positive throat culture for streptococci. Which of the following interventions should the nurse recommend to be included in the plan of care?
Explanation
The correct answer is Choice B.
Choice A rationale: Placing the client in a room with another client who has pharyngitis is not recommended. Pharyngitis can be caused by various different pathogens, not just streptococci. Co-housing clients with different infections can lead to cross-infection, complicating both clients’ conditions. Therefore, this choice is not the best option.
Choice B rationale: Ensuring that the client wears a surgical mask during transportation throughout the facility is the correct choice. Streptococcal infections are spread through respiratory droplets. A surgical mask can help prevent the spread of these droplets, protecting other clients and healthcare workers in the facility. This is a standard precaution in infection control.
Choice C rationale: Limiting the client’s visitors to visitations of 30 minutes is not necessarily beneficial. The duration of the visit does not significantly impact the risk of transmission as much as the precautions taken during the visit, such as hand hygiene and wearing a mask. Therefore, while limiting visitation time might reduce exposure, it is not the most effective measure to prevent the spread of infection.
Choice D rationale: Providing the client a room with negative pressure airflow of six air exchanges per hour is not necessary for a client with a streptococcal infection. Negative pressure rooms are typically used for clients with airborne diseases, such as tuberculosis. A streptococcal infection is spread through droplets, not airborne transmission, so a negative pressure room would not provide any additional benefit.
A nurse is reinforcing teaching with a client about the use of crutches. Which of the following actions by the client indicates an understanding of the teaching?
Explanation
A: Incorrect. Leaning on the crutches for support while standing still is not the correct way to use crutches. It can lead to discomfort and instability.
B: Correct. The client should advance the unaffected leg first while climbing stairs when using crutches. This technique ensures better stability and safety during stair ascent.
C: Incorrect. Standing 5 cm (2 in) from the front of a chair before sitting is not directly related to the use of crutches.
D: Incorrect. Bearing weight on the axilla while standing in the tripod position is not the correct way to use crutches. The tripod position is used for resting, not weight bearing.
A nurse is assisting with the plan of care for four clients. Which of the following tasks should the nurse assign to an assistive personnel (AP)?
Explanation
A: Incorrect. Ensuring a client can use crutches before discharge requires clinical judgment and skilled assessment, so it should not be delegated to assistive personnel.
B: Incorrect. Checking a client's ability to swallow following a stroke involves assessing the client's airway and potential risk of aspiration, which is a complex nursing task and should not be delegated to assistive personnel.
C: Incorrect. Obtaining a client's pain rating prior to physical therapy requires understanding the client's pain and its management, which should not be delegated to assistive personnel.
D: Correct. Assisting a client to get out of bed after a breathing treatment can be safely delegated to assistive personnel. It involves helping the client move, which is within the scope of their training.
A nurse is reinforcing teaching with a client about the use of crutches. Which of the following actions by the client indicates an understanding of the teaching?
Explanation
A: Incorrect. Leaning on the crutches for support while standing still is not the correct way to use crutches. It can lead to discomfort and instability.
B: Correct. The client should advance the unaffected leg first while climbing stairs when using crutches. This technique ensures better stability and safety during stair ascent.
C: Incorrect. Standing 5 cm (2 in) from the front of a chair before sitting is not directly related to the use of crutches.
D: Incorrect. Bearing weight on the axilla while standing in the tripod position is not the correct way to use crutches. The tripod position is used for resting, not weight bearing.

A nurse is caring for a postoperative client who is at risk for thrombus formation. Which of the following interventions should the nurse delegate to an assistive personnel (AP)?
Explanation
A: Correct. Applying thromboembolic stockings (compression stockings) to the client's legs is a task that can be safely delegated to assistive personnel. The nurse should provide clear instructions on how to apply them properly.
B: Incorrect. Monitoring the circulation in all four extremities requires clinical judgment and skilled assessment, and it should not be delegated to assistive personnel.
C: Incorrect. Recording the condition of the client's skin requires observation and assessment, which should not be delegated to assistive personnel.
A nurse is reinforcing teaching about health promotion with a group of young adult clients.
Which of the following information should the nurse include?
Explanation
A: Correct. Regular dental assessments every 6 months are recommended for all individuals, including young adults, to maintain good oral health and detect any potential issues early.
B: Incorrect. Testicular examinations are important for young adult males, but they should be performed monthly as part of testicular self-examination, not every 5 years.
C: Incorrect. Young adult females should have a routine physical examination annually, not every 4 years, to monitor their overall health and address any potential health concerns.
D: Incorrect. While tuberculosis screening is essential in certain populations, such as healthcare workers or individuals at high risk of exposure, a tuberculosis skin test every 3 years is not a standard recommendation for all young adults.
A nurse is caring for a client who is postoperative following abdominal surgery. Nurses Notes:
Neurological findings, incisional drainage, Urinary cutout, Client received from PACU with initial vital signs recorded. The client is drowsy but aroused by verbal stimuli. The client is oriented to person, place, and time. The client can move all extremities. Hypoactive bowel sounds. Abdominal dressing is intact with drainage noted. An indwelling urinary catheter is in place and draining yellow urine. Infusing lactated Ringer's solution at 100 mL/hr to the right forearm. The client is positioned for comfort and side rails are up x 2. The call light is within reach of the client.
Select the findings the nurse should report to the provider.
Explanation
A: The neurological findings were already noted in the nurse's initial assessment, and the client's orientation and movement of extremities are within the expected range postoperatively.
Therefore, it does not require immediate reporting.
B: Incisional drainage is a significant finding, and any change or concern in the drainage should be reported to the provider to assess for signs of infection or other complications.
C: Monitoring urinary output is essential, especially in a postoperative client, as it helps assess renal function and hydration status. Any significant changes in urinary output should be reported to the provider promptly.
D: The client's reported pain level of 6 on a scale of 0 to 10 indicates moderate pain, and the provider should be informed to address the pain and consider adjustments to the pain management plan.
A nurse is using Maslow's hierarchy of needs in assisting with discharge planning for a client.
Which of the following activities should the nurse recommend as the priority for this client?
Explanation
A: While volunteering at a local food pantry can be a meaningful activity, it is not the priority when considering Maslow's hierarchy of needs. Physiological needs, such as nutrition and exercise, take precedence.
B: Correct. Attending an exercise program addresses the client's physiological needs (specifically the need for physical activity and health) and takes priority over other options in this context.
C: Finding an enjoyable hobby addresses the client's need for self-fulfillment and self-esteem, which comes at a higher level in Maslow's hierarchy. It is not the immediate priority during discharge planning.
D: Supporting environmental conservation aligns with self-actualization, which is a higher-level need in Maslow's hierarchy. It is not the priority during discharge planning.
A nurse is assisting with the admission of a client who has brought their medications to the facility.
Which of the following actions should the nurse take?
Explanation
A: Allowing the client to continue taking medications as they did at home without verifying the prescriptions can be unsafe and is not within the scope of nursing practice.
B: Taking the medications from the client and discarding them is inappropriate. The nurse should not dispose of the client's medications without proper assessment and verification.
C: Correct. The nurse should compare the medications the provider has prescribed with the medications the client brought from home to ensure accuracy and safety. This is a crucial step during admission to prevent errors or omissions in the medication regimen.
D: Placing the medications in the medication cart and administering them without verification is unsafe and against best practices for medication administration.
A nurse is preparing to transfer a client from an acute care facility to a long-term care facility.
Which of the following information should the nurse plan to include in the transfer report?
Explanation
A: Discontinued medications should be documented in the client's medical records and communicated during the transfer report, but it is not the priority information to include in the report.
B: While resolved health conditions are relevant information, it is not the priority during transfer. The long-term care facility should be informed of the current health status and ongoing care needs of the client.
C: Correct. The frequency of vital sign collection is essential for monitoring the client's health status and any changes in their condition. This information helps the receiving facility to continue appropriate monitoring and interventions.
D: Completed nursing interventions are important but may not be as urgent as the frequency of vital sign collection. Information about ongoing nursing care and interventions should also be included in the transfer report.
A nurse is caring for a client who has recently undergone a total bilateral mastectomy.
Which of the following statements by the client requires immediate action by the nurse?
Explanation
A: The client's statement reflects feelings of confusion but does not indicate immediate harm or danger to themselves. It requires therapeutic communication and support but not immediate action.
B: The client's statement expresses concern about their future relationships but does not indicate immediate harm or danger to themselves. It requires support and counseling but not immediate action.
C: Correct. The client's statement suggests significant emotional distress and a potential risk for self-harm or suicidal ideation. Immediate action is required to assess the client's safety and provide appropriate interventions, such as involving a mental health professional.
D: The client's statement indicates dissatisfaction or regret about the mastectomy decision but does not indicate immediate harm or danger to themselves. It requires supportive communication and addressing concerns but not immediate action.
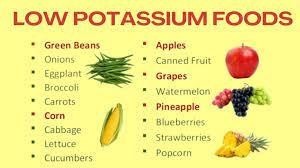
A nurse is reinforcing dietary teaching with a client who has chronic kidney disease and requires a lowpotassium diet. Which of the following food by the client demonstrates an understanding of the teaching?
Explanation
A: Cantaloupe is relatively high in potassium and is not a suitable choice for a low-potassium diet.
B: Baked potatoes are high in potassium and should be avoided in a low-potassium diet.
C: Banana chips are also high in potassium and should not be included in a low-potassium diet.
D: Correct. Applesauce is a low-potassium food and is an appropriate choice for a client with chronic kidney disease following a low-potassium diet.
A nurse is caring for a client who is refusing medical treatment. Which of the following actions should the nurse take?
Explanation
A: While explaining the negative consequences of refusal is important, it may not change the client's decision, and respect for the client's autonomy must be upheld.
B: Discussing the treatment with the client's partner without the client's consent may breach patient confidentiality and privacy.
C: Correct. The nurse should document the client's refusal of the medical treatment in the client's medical record. This documentation is essential for legal and ethical purposes and to ensure that the refusal is adequately communicated to the healthcare team.
D: Trying to convince the client to undergo the treatment is not appropriate and may violate the principle of informed consent. The client has the right to refuse treatment after being adequately informed of the risks and benefits.
A nurse is calculating the intake and output for a client over the last 8 hr. The client is receiving a continuous IV infusion at 150 mL/hr and had 4 oz of juice and 0.5 L of water.
How many mL of fluid should the nurse document as the client's intake for the last 8 hr? (Round your answer to the nearest whole number.)
Explanation
Total intake = IV fluid + Juice + Water
Total intake = (150 mL/hr) x (8 hr) + 4 oz + 500 mL Total intake = 1200 mL + 118.29 mL + 500 mL Total intake ≈ 1818.29 mL
The nurse should document the client's intake as approximately 1818 mL.
A nurse is collecting data from an older adult client. Which of the following findings should the nurse report to the provider?
Explanation
A: Correct. The presence of smooth, brown, irregular lesions on the back of each hand may indicate a concerning skin condition, such as melanoma or other types of skin cancer. The nurse should report this finding to the provider for further assessment and evaluation.
B: The presence of glossy, white arches around the periphery of the corneas is a normal finding, known as arcus senilis, which is commonly seen in older adults and not typically a cause for concern.
C: Urinary incontinence is a common issue in older adults and may require assessment and interventions but does not necessarily need immediate reporting unless there are specific acute changes or concerns related to the client's urinary function.
D: A decreased sense of taste is a common age-related change and may not require immediate reporting unless it is associated with other symptoms or significant nutritional issues.
A nurse is speaking with a client who has type 2 diabetes mellitus and a prescription for insulin. The client verbalizes anger about having to take insulin. Which of the following responses should the nurse make?
Explanation
A: Asking the client why they are angry may come across as confrontational and defensive, potentially escalating the situation. It does not promote open communication or therapeutic rapport.
B: Sharing personal information about diabetes running in the nurse's family is not relevant to the client's feelings or concerns and may not be helpful in addressing the client's anger.
C: Correct. Acknowledging the client's feelings of anger and offering to sit down and talk provides an opportunity for therapeutic communication. This response demonstrates empathy and a willingness to listen and address the client's concerns about insulin therapy.
D: While it is true that insulin therapy can help reduce the risk of complications in type 2 diabetes, this response may come across as dismissive of the client's feelings and concerns. It does not address the emotional aspect of the client's anger.
A nurse is assisting with the care of a client who is receiving a unit of packed RBCs.
Vital Signs 0800:
Blood pressure 112/64 mm Hg Heart rate 80/min
Respiratory rate 18/min
Temperature 37.1° C (98.8" F Oxygen saturation 97% on room air 08151
Blood pressure 106/54 mm Hg Heart rate 100/min Respiratory rate 22/min Temperature 37° C (98,6°F) Oxygen saturation 95% on room air
Complete the following sentence by using the lists of options.
Complete the following sentence by using the lists of options. The client has manifestations of an _______as evidenced by the _________
Explanation
Allergic reaction: The client is at risk of blood transfusion reaction as evidenced by an increase in respiratory rate to 22 and an increase in heart rate from 88 to 100.
Itching: itching is an immediate symptom of type 1 hypersensitivity reactions that are common with blood transfusion.
A nurse is caring for a client who has a prescription for a potassium supplement. The client tells the nurse that the pill is too large to swallow and refuses to take it. The nurse offers to break the pill into two smaller pieces. The nurse is demonstrating which of the following ethical principles?
Explanation
A: Autonomy refers to respecting the client's right to make their own decisions about their healthcare, even if it differs from the nurse's recommendation. By offering the client the option to break the pill into two smaller pieces, the nurse is respecting the client's autonomy and promoting their ability to make regarding their care.
B: Beneficence refers to the nurse's duty to act in the client's best interest and promote their wellbeing. In this scenario, the nurse is not necessarily promoting the client's well-being but rather facilitating their ability to make a decision about the medication.
C: Justice refers to fairness and equal treatment of clients. It is not directly applicable in this scenario.
D: Nonmaleficence refers to the nurse's duty to do no harm to the client. In this case, breaking the pill into smaller pieces is not harmful to the client; however, it is not the primary ethical principle demonstrated in this situation.
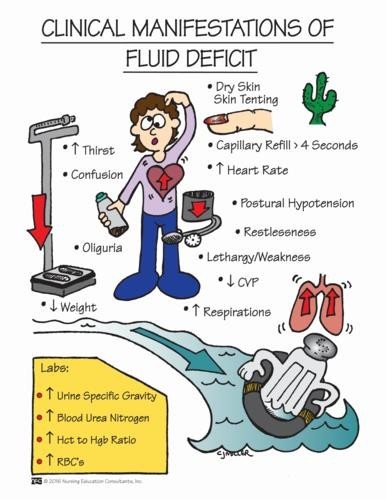
A nurse is caring for a client who is postoperative and is experiencing nausea and vomiting. The nurse should identify which of the following findings as indications that the client has fluid volume deficit. (Select all that apply.)
Explanation
A: A full bounding pulse is a sign of increased fluid volume or fluid overload, not fluid volume deficit.
B: Cool extremities can be an indication of decreased peripheral perfusion, which may occur in fluid volume deficit.
C: Moist crackles in the lungs are an indication of fluid volume excess or pulmonary congestion, not fluid volume deficit.
D: Orthostatic hypotension, which is a drop in blood pressure when changing from lying to standing, can be a sign of fluid volume deficit due to inadequate blood volume.
E: Flat neck veins are an indication of decreased venous return and can occur in fluid volume deficit.
A nurse is reviewing the medical records of a client who has heart failure. The nurse should identify which of the following laboratory results as an indication that the client has fluid volume excess.
Explanation
A: A urine specific gravity of 1.015 indicates dilute urine, which is consistent with fluid volume excess.
B: A hematocrit of 42% is within the normal range and does not specifically indicate fluid volume excess.
C: A urine pH of 6.5 is within the normal range and does not specifically indicate fluid volume excess.
D: A BUN (blood urea nitrogen) level of 8 mg/dL is within the normal range and does not specifically indicate fluid volume excess.
A nurse is preparing to administer oxygen to a client who has heart failure and is having severe difficulty breathing. Which of the following oxygen delivery equipment should the nurse select to provide the highest concentration of oxygen to the client?
Explanation
A: A nasal cannula provides a low to moderate concentration of oxygen and is not suitable for a client experiencing severe difficulty breathing.
B: A simple face mask provides a higher concentration of oxygen than a nasal cannula but may not deliver a high enough concentration for a client experiencing severe respiratory distress.
C: A Venturi mask can provide a precise and adjustable concentration of oxygen but may not deliver the highest concentration needed in this scenario.
D: A nonrebreather mask can deliver the highest concentration of oxygen (up to 100%) and is the most appropriate choice for a client experiencing severe difficulty breathing.
A nurse is moving a client up in bed with the assistance of a second nurse. Which of the following actions should the nurse take?
Explanation
A: Standing facing the center of the bed at the client's side allows the nurse to maintain proper body mechanics and use their body weight to assist in moving the client.
B: Placing feet apart with the foot nearest the head of the client's bed in front of the other foot also helps the nurse maintain stability and leverage while moving the client.
C: Keeping knees and hips straight while bending at the waist toward the client is incorrect body mechanics and can put a strain on the nurse's back.
D: Encouraging the client to keep their legs straight and remain still is not appropriate. The client should be actively involved in the movement, assisting as much as possible, to ensure their safety and cooperation.
A nurse is caring for a client who has just died and practiced the Islamic faith. Which of the following cultural practices should the nurse expect?
Explanation
A. The client's body should be placed on the floor: This is not a specific cultural practice in Islam. In Islamic tradition, the deceased person is usually placed on a raised surface, like a table or bed, to allow family and friends to gather around for prayers and final respects.
B. The client's oldest child will bathe the body: This is not a specific cultural practice in Islam.
In Islamic tradition, the body is usually washed by individuals of the same gender who are experienced in the ritual washing of the deceased, known as "Ghusl."
C. The client's face should be turned toward Mecca: Correct. In Islamic tradition, when a person dies, it is customary to position the body with the head facing the Kaaba in Mecca, which is the holy city in Islam and the direction toward which Muslims pray.
D. The client's body will be adorned with amulets: This is not a specific cultural practice in Islam. While some individuals in various cultures may use amulets or charms for protection, it is not a universal Islamic practice for the deceased.
A nurse at a long-term care facility is caring for a client who is alert.
Which of the following actions should the nurse take to protect the client's privacy?
Explanation
A. Place the client's medication record on the bedside table while ambulating the client: This action does not relate to protecting the client's privacy. It might actually compromise confidentiality by leaving sensitive information exposed.
B. Give a report about the client's status while standing at the nurses' station: This action does not protect the client's privacy. Discussing sensitive information in a public area can lead to breaches of confidentiality.
C. Speak with the client about their condition after visitors have left: Correct. Protecting the client's privacy is essential, and discussing personal health information in private with the client respects their right to confidentiality.
D. Place a message board in the client's room to post dietary information: This action does not relate to protecting the client's privacy. Posting dietary information may be helpful for staff, but it doesn't address the client's privacy concerns.
A nurse is reinforcing preoperative teaching with a client who speaks a different language than the nurse. Which of the following actions should the nurse take?
Explanation
A. Ask a family member who speaks the client's primary language to interpret: While involving family members may seem helpful, it is not the most effective way to ensure accurate and complete communication. There may be language barriers or misunderstandings.
B. Plan a long teaching session initially to introduce the necessary material: Lengthy teaching sessions may overwhelm the client and reduce their ability to absorb and retain information, especially when there is a language barrier.
C. Provide the least important information first: This approach is not recommended because it does not prioritize the client's understanding of essential preoperative instructions.
D. Provide handouts written in the client's primary language: Correct. Providing written materials in the client's primary language allows them to review the information at their own pace and increases the likelihood of understanding important preoperative instructions.
Sign Up or Login to view all the 53 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
