Ati adult med Surg nurs 4292 exam
Total Questions : 71
Showing 25 questions, Sign in for moreA nurse is attending to a client with a T-4 spinal cord injury. Which of the following observations should the nurse recognize as a possible trigger for autonomic dysreflexia?
Explanation
Choice A reason: A distended bladder is a common cause of autonomic dysreflexia. It can trigger an exaggerated response from the autonomic nervous system, leading to a rapid increase in blood pressure. This is because the full bladder sends signals to the spinal cord, which then attempts to send signals to the brain. However, due to the injury, these signals cannot pass through, resulting in a reflex that increases blood pressure.
Choice B reason: While a severe headache is a symptom of autonomic dysreflexia, it is not a cause. The headache results from the body's response to a triggering stimulus, such as a distended bladder, which leads to the high blood pressure characteristic of autonomic dysreflexia.
Choice C reason: Nasal congestion is not typically a cause of autonomic dysreflexia. The condition is usually triggered by a noxious stimulus below the level of the spinal cord injury, such as a full bladder or bowel, skin irritation, or other types of physical discomfort.
Choice D reason: Elevated blood pressure is a symptom, not a cause, of autonomic dysreflexia. The condition itself causes a sudden spike in blood pressure due to an uncontrolled reflex sympathetic discharge in response to a triggering stimulus below the level of the injury.
A nurse is preparing a care plan for a patient receiving enteral feedings via a nasogastric (NG) tube. Which of the following actions should the nurse prioritize?
Explanation
Choice A reason: Labeling the feeding bag with the date and time is important for tracking, but it is not the first action to take. The priority is to ensure that the NG tube is correctly placed and the stomach contents can be aspirated to verify placement before administering the feeding.
Choice B reason: Aspirating the client's stomach contents is the first action the nurse should take. This is to confirm the correct placement of the NG tube to prevent complications such as aspiration pneumonia. It is a critical step before starting any enteral feeding.
Choice C reason: Hanging the feeding bag 30 cm (12 inches) above the client is necessary for gravity feeding, but it comes after verifying the NG tube placement through aspiration of stomach contents.
Choice D reason: Warming the feeding to room temperature is a comfort measure and helps to prevent gastrointestinal discomfort. However, it is not the first action to take. The priority is to check the tube placement.
A patient with a history of angina is being admitted to the emergency department with a suspected myocardial infarction (MI). Which of the following observations will assist the nurse in differentiating stable angina from an MI?
Explanation
Choice A reason: Myocardial infarction (MI) is not limited to occurrences with exertion. While stable angina typically occurs during physical activity or emotional stress, MI can happen at any time, even at rest. The underlying cause of an MI is the complete blockage of blood supply to a part of the heart muscle, usually due to a blood clot in a coronary artery. This blockage can lead to the death of heart muscle tissue, a condition that requires immediate medical attention.
Choice B reason: Stable angina does not typically last for more than 30 minutes. It is characterized by chest pain or discomfort that occurs predictably with exertion or emotional stress and is relieved within minutes by rest or nitroglycerin. In contrast, the pain from an MI is more prolonged and severe, and it is not relieved by rest or nitroglycerin. If chest discomfort lasts longer than 15 minutes and is not alleviated by rest or nitroglycerin, it is a warning sign that the individual may be experiencing an MI.
Choice C reason: This is the distinguishing feature between stable angina and an MI. Stable angina is usually relieved within 3-5 minutes by rest or nitroglycerin, which helps to dilate the coronary arteries and improve blood flow to the heart muscle. Nitroglycerin is ineffective in relieving the symptoms of an MI because the problem is not just reduced blood flow but a complete blockage that nitroglycerin cannot overcome.
Choice D reason: The pain associated with an MI typically lasts for more than 15 minutes and can be quite severe. Unlike stable angina, the pain of an MI is not relieved by rest or nitroglycerin. The duration and severity of the pain, along with other symptoms such as shortness of breath, sweating, nausea, or lightheadedness, help differentiate an MI from stable angina.

A nurse is taking a health history from a client with chronic pancreatitis. Which of the following points suggests the main cause of the client's condition?
Explanation
Choice A reason: Weight gain is not typically a direct cause of chronic pancreatitis. While obesity can be a risk factor for developing pancreatitis, it is not considered a primary cause.
Choice B reason: The use of alcohol is the most common cause of chronic pancreatitis. Long-term alcohol misuse can lead to the development of chronic pancreatitis, accounting for about 70% of cases³.
Choice C reason: Abdominal pain that is relieved with food or antacids is more indicative of conditions like peptic ulcers rather than chronic pancreatitis.
Choice D reason: Exposure to occupational chemicals has not been established as a primary cause of chronic pancreatitis. While certain toxins can affect the pancreas, they are not a common cause of chronic pancreatitis.
A nurse is attending to a patient with valvular heart disease who is at risk for left-sided heart failure. Which of the following symptoms should alert the nurse that the patient is developing this condition?
Explanation
Choice A reason: Anorexia, or loss of appetite, is not typically a direct manifestation of left-sided heart failure. While it can be associated with many medical conditions and may occur in the context of heart failure due to overall decreased well-being, it is not a specific indicator of left-sided heart failure.
Choice B reason: Weight gain can be associated with heart failure, but it is more commonly a sign of right-sided heart failure, where fluid accumulates in the body tissues, causing swelling and weight increase. In left-sided heart failure, weight gain is not as prominent because the primary issue is the backup of blood into the lungs, not fluid retention in the tissues.
Choice C reason: A distended abdomen can occur in heart failure due to fluid accumulation; however, it is more characteristic of right-sided heart failure, where the failure of the right ventricle leads to systemic congestion, including the abdominal area. In left-sided heart failure, the primary effect is on the lungs, not the abdomen.
Choice D reason: Dyspnea, or difficulty breathing, is a hallmark symptom of left-sided heart failure. It occurs due to the backup of blood in the pulmonary circulation, which leads to pulmonary congestion and reduced oxygen exchange. Patients may experience shortness of breath, especially during exertion or when lying flat (orthopnea), and may wake up at night with shortness of breath (paroxysmal nocturnal dyspnea).
Left-sided heart failure, often caused by conditions like valvular heart disease, leads to a decrease in the heart’s ability to pump blood effectively. This results in a buildup of pressure in the lungs, manifesting as dyspnea, which is an important symptom for nurses and other healthcare providers to recognize and manage promptly.
A nurse is caring for a patient who has recently developed a pulmonary embolism. Which of the following medications should the nurse expect to administer?
Explanation
Choice A reason: Atropine is not typically used for the treatment of pulmonary embolism. It is an anticholinergic drug that is primarily used to treat bradycardia (slow heart rate) and as part of the management of organophosphate poisoning. It does not have a role in the management of pulmonary embolism, which requires anticoagulation to prevent further clot formation.
Choice B reason: Furosemide is a loop diuretic commonly used to treat fluid overload conditions such as heart failure or edema. While it can help relieve symptoms associated with fluid accumulation, it does not treat the underlying cause of a pulmonary embolism, which is a blood clot in the pulmonary arteries.
Choice C reason: Heparin is an anticoagulant medication that is commonly used in the initial treatment of pulmonary embolism. It works by preventing the formation of new blood clots and stopping existing clots from getting bigger. Heparin is often administered intravenously or subcutaneously and is a key component in the management of pulmonary embolism.
Choice D reason: Dexamethasone is a corticosteroid that is used to reduce inflammation in various conditions, such as allergic reactions, asthma, and certain types of arthritis. It is not used as a primary treatment for pulmonary embolism, as it does not have anticoagulant properties.
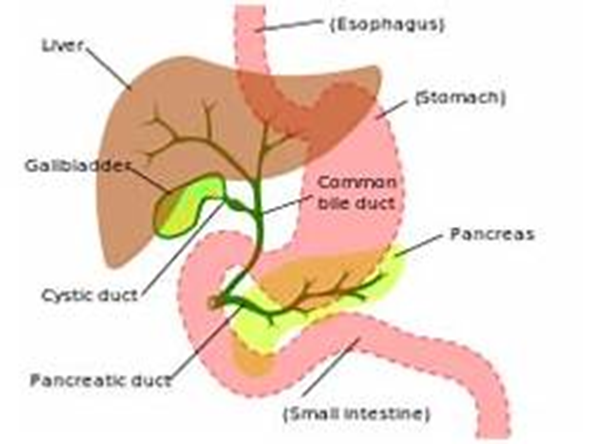
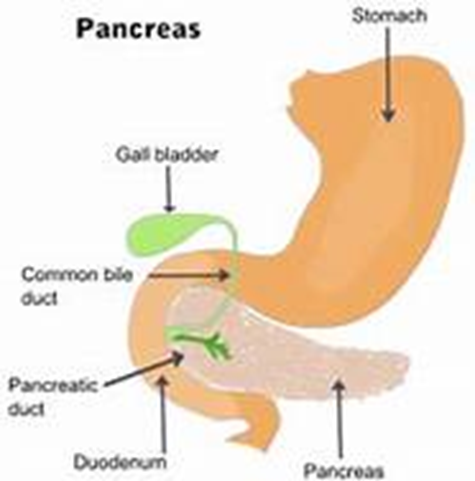
A nurse is evaluating a patient with a common bile duct obstruction due to chronic cholecystitis. Which of the following symptoms should the nurse anticipate?
Explanation
Choice A reason: Tenderness in the left upper abdomen is not typically associated with an obstruction of the common bile duct. This symptom is more commonly related to conditions affecting the stomach, pancreas, or spleen. The common bile duct is in the right upper quadrant of the abdomen, and tenderness in this area might be expected with its obstruction.
Choice B reason: Ecchymosis of the extremities is not a common finding in common bile duct obstruction. Ecchymosis, or bruising, is usually due to trauma, blood disorders, or other causes of fragile blood vessels and is not related to bile duct issues.
Choice C reason: Pale-colored urine is the opposite of what might be expected with common bile duct obstruction. Typically, the urine may become dark due to increased bilirubin levels that are excreted by the kidneys when the bile duct is obstructed.
Choice D reason: Fatty stools, or steatorrhea, are a classic finding in common bile duct obstruction. When bile flow is blocked, fats are not properly digested and absorbed, leading to stools that are bulky, greasy, and often have a foul odor. This occurs because bile is necessary for the emulsification and absorption of dietary fats in the intestine.
A patient is brought to the emergency room with kidney stones. During the assessment, which of the following symptoms should the nurse anticipate?
Explanation
Choice A reason: Bradycardia, which is a slower than normal heart rate, is not a common finding associated with renal calculi. Renal calculi, or kidney stones, typically cause symptoms related to the urinary system rather than directly affecting the heart rate.
Choice B reason: Bradypnea, or abnormally slow breathing, is also not a typical symptom of renal calculi. Patients with kidney stones may experience changes in urination patterns, such as frequency or urgency, but not typically changes in respiratory rate.
Choice C reason: Severe pain is indeed the most common symptom associated with renal calculi. This pain, known as renal colic, is often sudden in onset, very severe, and may radiate from the back down to the lower abdomen or groin. The pain is caused by the stone moving into the ureter and causing a blockage, which leads to increased pressure and stretching of the kidney or ureter. Renal calculi can cause a range of symptoms, with severe pain being the most prominent and often the first symptom that leads individuals to seek medical care. The pain is typically very intense and can be accompanied by other symptoms such as nausea, vomiting, and hematuria (blood in the urine).
Choice D reason: Nocturia, or frequent urination at night, can be a symptom of renal calculi, especially if the stones affect the bladder or cause urinary tract infections. However, the most characteristic symptom of renal calculi is severe pain, not necessarily nocturia.
A nurse is caring for a patient who is receiving continuous enteral nutrition and has developed refeeding syndrome. Which of the following lab results should the nurse anticipate?
Explanation
Choice A reason: Hypermagnesemia, or high levels of magnesium in the blood, is not typically associated with refeeding syndrome. Instead, refeeding syndrome can lead to hypomagnesemia, which is a low level of magnesium in the blood, due to shifts of magnesium into the cells during insulin secretion in the refeeding process.
Choice B reason: Hyponatremia, or low levels of sodium in the blood, is not a hallmark of refeeding syndrome. While fluid shifts can affect sodium levels, the key electrolyte disturbances in refeeding syndrome involve phosphorus, potassium, and magnesium.
Choice C reason: Hyperkalemia, or high levels of potassium in the blood, is not a common finding in refeeding syndrome. Similar to magnesium, potassium can shift into cells during refeeding, which can actually lead to hypokalemia, or low levels of potassium in the blood.
Choice D reason: Hypophosphatemia, or low levels of phosphorus in the blood, is the hallmark of refeeding syndrome. When a malnourished individual is refed, insulin secretion is stimulated by the increased carbohydrate intake. Insulin promotes cellular uptake of glucose, which is accompanied by phosphate, potassium, and magnesium, leading to a decrease in the serum levels of these electrolytes. Phosphorus is critical for cellular processes, and its deficiency can lead to muscle weakness, respiratory failure, hemolysis, and impaired cardiac function. During refeeding, careful monitoring of electrolytes is essential to prevent and manage refeeding syndrome. Hypophosphatemia is the most significant laboratory finding to anticipate in a patient with refeeding syndrome, and it requires prompt recognition and treatment to prevent serious complications.
The healthcare provider prescribes lactulose for a patient with hepatic encephalopathy. What should the nurse monitor to evaluate the effectiveness of this medication?
Explanation
Choice A reason: Lactulose is used in hepatic encephalopathy primarily to lower blood ammonia levels. It works by converting ammonia in the intestines into ammonium, which is then excreted³. Therefore, a decrease in ammonia levels would indicate the effectiveness of the medication.
Choice B reason: While lactulose can relieve constipation due to its laxative effect, relief of constipation is not the primary indicator of its effectiveness in treating hepatic encephalopathy³.
Choice C reason: Decreased liver enzymes are not a direct measure of lactulose's effectiveness in hepatic encephalopathy. Liver enzymes are indicators of liver function, not ammonia levels³.
Choice D reason: Relief of abdominal pain is not a specific indicator of lactulose's effectiveness in hepatic encephalopathy. The medication's primary role is to reduce ammonia levels, not to alleviate pain³.
A nurse is evaluating a patient with a pneumothorax who has a chest tube in place. Which of the following observations should prompt the nurse to notify the provider immediately?
Explanation
Choice A reason: Bubbling in the water seal chamber with exhalation can be normal, indicating that air is being evacuated from the pleural space.
Choice B reason: Crepitus, or subcutaneous emphysema, can indicate that air is leaking into the tissue around the chest tube site, which is a serious complication that requires immediate attention.
Choice C reason: Movement of the trachea toward the unaffected side can indicate tension pneumothorax, a life-threatening condition that also requires immediate attention.
Choice D reason: If the eyelets of the chest tube are not visible, it may simply mean that the tube is inserted fully, which is not an immediate cause for concern unless other symptoms are present.
A nurse is evaluating a patient with chronic kidney disease for signs of fluid volume increase. Which of the following is a reliable indicator of fluid retention?
Explanation
Choice A reason: Sodium level is not a direct measure of fluid volume. While sodium balance can influence fluid status, the serum sodium level can be affected by various factors and does not reliably indicate fluid volume increase on its own.
Choice B reason: Intake and output records are important for managing fluid balance, especially in a hospital setting. However, they can be influenced by many factors, such as incomplete recording or insensible losses, and do not provide a direct measure of fluid retention.
Choice C reason: Daily weight is considered the most reliable measure of fluid retention. Weight changes can reflect fluid balance accurately because 1 liter of fluid is roughly equivalent to 1 kilogram of body weight. In clients with chronic kidney disease, daily weight monitoring can help detect fluid volume increases or decreases promptly. For a client with chronic kidney disease, daily weight monitoring is a key assessment tool for detecting fluid volume changes. It provides a quantifiable and objective measure that can guide interventions to manage fluid balance effectively.
Choice D reason: Tissue turgor, which refers to the skin’s elasticity, is not a reliable measure of fluid volume. It can be influenced by age, edema, and other factors, and changes in turgor may not accurately reflect fluid status in the body.
A nurse in the emergency department is looking after a client who has taken three nitroglycerin tablets sublingually for chest pain. The client reports that the chest pain has subsided but now has a headache. What should the nurse say?
Explanation
Choice A reason: A headache is not typically an indication of an allergy to nitroglycerin. Allergic reactions are more likely to present with symptoms such as rash, itching, or difficulty breathing.
Choice B reason: Headaches are a well-known side effect of nitroglycerin, due to its vasodilating effects, which can cause dilation of cerebral arteries.
Choice C reason: While anxiety can cause headaches, in this context, where the client has taken nitroglycerin, it is more likely that the headache is a side effect of the medication rather than anxiety.
Choice D reason: Tolerance to medication would reduce the effectiveness of the drug, not typically cause a headache. The headache is a common side effect, not an indication of tolerance.
A nurse is admitting a client with a history of duodenal ulcer. To determine if the client's current symptoms are connected to this condition, the nurse should check for which signs of a duodenal ulcer?
Explanation
Choice A reason: Pain that is relieved by food intake is a classic symptom of duodenal ulcers, as eating can neutralize stomach acid temporarily, providing relief.
Choice B reason: Pain radiating down the right arm is not a typical symptom of a duodenal ulcer; it is more commonly associated with cardiac issues.
Choice C reason: Nausea and vomiting can be associated with duodenal ulcers, but they are not as specific as pain relief by food intake.
Choice D reason: Weight loss can occur with duodenal ulcers due to pain and eating avoidance, but the key symptom that relates directly to the ulcer is pain relief after food intake.
A nurse is reviewing the lab results of a patient after a hemodialysis session. The nurse should anticipate a decrease in which of the following laboratory values?
Explanation
Choice A: The red blood cell (RBC) count is not typically decreased by hemodialysis. Hemodialysis does not remove cells from the blood. However, patients with chronic kidney disease often have anemia, which is a low RBC count, due to a decrease in the production of erythropoietin by the kidneys. Erythropoietin is a hormone that stimulates the bone marrow to produce RBCs. Anemia in these patients is treated with erythropoiesis-stimulating agents, not dialysis.
Choice B: Protein levels are not directly affected by hemodialysis. However, patients on hemodialysis may have lower protein levels due to dietary restrictions or protein loss during the treatment. It is important for patients to manage their protein intake to prevent malnutrition and maintain overall health.
Choice C: Potassium levels are expected to decrease following hemodialysis. Potassium is an electrolyte that is normally filtered out by the kidneys. In patients with kidney failure, potassium levels can build up in the blood and cause serious heart problems. Hemodialysis removes excess potassium from the blood, which helps to prevent complications such as cardiac arrhythmia. The normal range for serum potassium is 3.5 to 5.0 mmol/L. After a hemodialysis treatment, a nurse should expect to find a decrease in potassium levels in the laboratory data of a client. This is because hemodialysis effectively removes excess potassium, which can accumulate in the blood due to reduced kidney function. Maintaining proper potassium levels is crucial for preventing heart complications in patients with kidney failure.
Choice D: Calcium levels are not typically decreased by hemodialysis. In fact, calcium levels can be affected by the dialysate used during hemodialysis. Some dialysates contain calcium, and this can actually increase the patient’s blood calcium levels. Patients with kidney failure may also have secondary hyperparathyroidism, which affects calcium levels, and they may be treated with calcium supplements or vitamin D analogs to manage their calcium levels.
A client is receiving continuous enteral nutrition via a nasogastric small-bore silicone feeding tube. What should the nurse prepare for when the client is scheduled to have a computed tomography (CT) scan?
Explanation
Choice A reason: Rescheduling the scan is not necessary unless there are other contraindications or scheduling conflicts.
Choice B reason: Sending a suction catheter is a precautionary measure, but it does not address the management of the feeding tube during the scan.
Choice C reason: Shutting off the feeding 30-60 minutes before the scan is a standard practice to reduce the risk of aspiration and to ensure that the stomach contents do not interfere with the imaging.
Choice D reason: Connecting the feeding tube to continuous suction is not typically required unless there is a specific concern for aspiration or gastric content management during the scan.
A nurse in the emergency department is caring for a patient who experienced a seizure and became unresponsive after reporting a sudden, severe headache. The patient's vital signs are as follows: blood pressure of 198/110 mm Hg, pulse of 82/min, respirations of 24/min, and a temperature of 38.2° C (100.8° F). Which neurological disorder should the nurse suspect?
Explanation
Choice A reason: An embolic stroke is caused by an embolus, often a blood clot, that travels to the brain from another part of the body. It does not typically present with a sudden, severe headache.
Choice B reason: A thrombotic stroke occurs when a blood clot forms inside one of the brain's arteries. While it can cause a headache, it is not usually characterized by a sudden, severe headache.
Choice C reason: A transient ischemic attack (TIA) is often called a mini-stroke and symptoms are temporary. A sudden, severe headache is more indicative of a hemorrhagic stroke.
Choice D reason: A hemorrhagic stroke, which involves bleeding within the brain, is most likely to cause a sudden, severe headache, and can lead to seizures and changes in consciousness.
The nurse should be most concerned about a lipid emulsion prescription for a patient with which condition?
Explanation
Choice A reason: A fractured femur, while a serious injury, does not inherently contraindicate the use of lipid emulsions. These patients may require additional nutrition if they are unable to eat adequately by mouth, and lipid emulsions can be part of their parenteral nutrition regimen if needed.
Choice B reason: Severe anorexia nervosa is a condition that can lead to malnutrition and may necessitate the use of parenteral nutrition, including lipid emulsions, to provide essential nutrients. However, care must be taken to avoid refeeding syndrome, a potentially fatal condition that can occur when malnourished patients begin to refeed too quickly.
Choice C reason: Gastrointestinal obstruction is a condition that could be exacerbated by the administration of lipid emulsions. In cases of obstruction, enteral or parenteral nutrition may need to be carefully managed or avoided until the obstruction is resolved to prevent further complications. While lipid emulsions are a valuable component of parenteral nutrition, their use must be carefully considered in the context of the patient’s overall clinical condition. In the case of gastrointestinal obstruction, the nurse would be most concerned about the prescription of a lipid emulsion due to the potential for exacerbating the obstruction and complicating the patient’s condition.
Choice D reason: Chronic diarrhea and vomiting can lead to dehydration and electrolyte imbalances, but they do not directly contraindicate the use of lipid emulsions. However, the underlying cause of these symptoms should be addressed, and fluid and electrolyte balance should be carefully monitored.
The nurse is examining laboratory test results for a client with liver disease and observes that the client's albumin level is low. Which nursing assessment would suggest low albumin levels?
Explanation
Choice A reason: Asterixis, also known as “liver flap,” is a type of tremor characterized by rapid, nonrhythmic extensions and flexions in the wrist and fingers. It is associated with hepatic encephalopathy, a condition that can occur with severe liver disease, but it is not a direct indicator of low albumin levels.
Choice B reason: Peripheral edema is a common clinical finding in patients with hypoalbuminemia, which is a low level of albumin in the blood. When albumin levels are low, fluid from the bloodstream can leak into body tissues, causing swelling, especially in the lower limbs. When assessing a client with liver disease and low albumin levels, palpating for peripheral edema would be the most relevant nursing assessment, as it directly correlates with the effects of hypoalbuminemia on fluid balance in the body. Albumin is a protein made by the liver that helps keep fluid in your blood vessels and plays a role in transporting substances throughout your body. Low levels of albumin can lead to fluid leaking out of blood vessels into tissues, causing swelling or edema.
Choice C reason: Decreased level of consciousness can be a sign of various conditions, including hepatic encephalopathy or other complications of liver disease, but it is not specifically indicative of low albumin levels.
Choice D reason: Petechiae are small red or purple spots caused by bleeding into the skin and may be associated with various conditions, including liver disease, but they are not a specific sign of low albumin levels.
A patient is admitted to the medical unit with acute pancreatitis. When planning care for this patient, which of the following interventions should the nurse include? (Select all that apply).
Explanation
Choice A: Administer antiemetics as needed Reason: Acute pancreatitis often causes severe nausea and vomiting. Antiemetics are administered to control these symptoms and prevent further complications such as dehydration and electrolyte imbalance.
Choice B: Administer analgesics as needed Reason: Pain management is a crucial part of the treatment for acute pancreatitis. The condition can cause severe abdominal pain, and analgesics are administered to provide relief.
Choice C: NPO (nothing by mouth) until pain-free Reason: The goal in treating acute pancreatitis is to allow the pancreas to rest and recover from the inflammation3. Keeping the patient NPO (nothing by mouth) helps achieve this by reducing the stimulation and workload of the pancreas.
Choice D: Monitor blood glucose and provide insulin as needed Reason: Acute pancreatitis can affect the pancreas’ ability to produce insulin, leading to elevated blood glucose levels. Therefore, monitoring blood glucose levels and administering insulin as needed is an important part of the management plan.
Choice E: Side-lying or fetal position Reason: While the side-lying or fetal position might help some patients with abdominal pain, it is not a standard intervention for acute pancreatitis. Therefore, this option is not correct.
Choice F: Monitor hydration status Reason: Patients with acute pancreatitis are at risk of dehydration due to symptoms like vomiting and decreased oral intake. Monitoring hydration status is crucial to ensure appropriate fluid replacement.
A nurse is conducting an assessment of a patient with a gastric ulcer. Which of the following findings should the nurse anticipate? (Select all that apply.)
Explanation
Choice A reason: Pain occurring 30 to 60 minutes after a meal is a common symptom of gastric ulcers due to the increased gastric acid secretion during digestion that can aggravate the ulcer.
Choice B reason: Pain at night is also typical for gastric ulcers as the circadian rhythm can influence acid secretion, potentially leading to increased discomfort during the night.
Choice C reason: A sensation of bloating can be associated with gastric ulcers due to delayed gastric emptying or increased sensitivity of the stomach lining.
Choice D reason: Pain relieved by eating is indicative of gastric ulcers because food can act as a buffer to stomach acid, temporarily relieving pain².
Choice E reason: Pain upon palpation of the epigastric region is expected in clients with gastric ulcers due to the localized inflammation and sensitivity of the stomach lining².
A nurse is attending to a patient with acute respiratory failure (ARF). The nurse should observe the patient for which of the following signs of this condition? (Select all that apply.)
Explanation
Choice A reason: Hypoxemia, or low oxygen levels in the blood, is a primary indicator of ARF as the lungs are unable to adequately oxygenate the blood.
Choice B reason: Confusion can result from hypoxemia or hypercapnia (high carbon dioxide levels) as the brain is sensitive to changes in blood gas levels.
Choice C reason: Dyspnea, or difficulty breathing, is a hallmark symptom of ARF as the lungs struggle to maintain adequate gas exchange.
Choice D reason: Bradycardia, or a slow heart rate, is not typically associated with ARF. Tachycardia, or a fast heart rate, is more common as the body attempts to compensate for hypoxemia.
Choice E reason: Hypocarbia, or low carbon dioxide levels, can occur in ARF if the body is attempting to compensate for hypoxemia by hyperventilating.
A nurse is educating a patient with diabetes mellitus about peritoneal dialysis. The nurse emphasizes the importance of adhering to the prescribed dwell time for dialysis to avoid the risk of which complication?
Explanation
Choice A: Hyperglycemia
The reason hyperglycemia is a risk when the prescribed dwell time is not maintained is due to the glucose present in the dialysate. The dialysate used in PD often contains glucose, which acts as an osmotic agent to facilitate fluid removal from the blood. If the dwell time is too short, there may not be enough time for the glucose to be absorbed, leading to higher levels of glucose in the blood. Conversely, if the dwell time is too long, excessive glucose absorption can occur, also leading to hyperglycemia. For patients with diabetes mellitus, maintaining the prescribed dwell time is essential to manage their blood glucose levels effectively. The normal range for fasting blood glucose is typically between 70 to 99 mg/dL, and for diabetes patients, maintaining blood glucose levels as close to the normal range as possible is crucial to prevent complications.
Choice B: Disequilibrium Syndrome
Disequilibrium syndrome is characterized by neurological symptoms resulting from rapid changes in the composition of extracellular fluids during dialysis. This condition is more commonly associated with hemodialysis due to the rapid shifts that can occur with this modality. In PD, the risk of disequilibrium syndrome is significantly lower because the exchange of solutes and fluids is more gradual. Therefore, while important to consider, it is not the primary complication associated with the maintenance of dwell time in PD.
Choice C: Peritonitis
Peritonitis, an infection of the peritoneal cavity, is a serious complication of PD but is not directly related to the duration of dwell time. It is typically caused by contamination during the exchange process or catheter-related infections. While proper technique and hygiene are critical in preventing peritonitis, the dwell time itself does not influence the risk of developing this infection.
Choice D: Hyperphosphatemia
Hyperphosphatemia refers to elevated levels of phosphate in the blood and is a concern in patients with renal failure due to the kidneys’ inability to excrete phosphate effectively. The dwell time in PD may affect the removal of phosphate to some extent; however, it is not the primary concern related to the maintenance of dwell time. Phosphate binders and dietary restrictions are commonly used to manage phosphate levels in PD patients.
A student nurse is studying the clinical signs of chronic kidney disease. Which of the following findings align with this diagnosis? (Select all that apply.)
Explanation
Choice A: Hypokalemia, or low potassium levels in the blood, is not typically associated with CKD. In fact, patients with advanced CKD are more likely to experience hyperkalemia, which is an elevated potassium level, due to the kidneys’ decreased ability to excrete potassium. The normal range for serum potassium is 3.5 to 5.0 mmol/L.
Choice B: Anemia is a common finding in CKD and is due to the kidneys’ reduced production of erythropoietin, a hormone that stimulates the bone marrow to produce red blood cells. Symptoms of anemia include fatigue, weakness, and pale skin. The normal range for hemoglobin in adults is 13.8 to 17.2 grams per deciliter for men and 12.1 to 15.1 grams per deciliter for women.
Choice C: Hypertension, or high blood pressure, is both a cause and a complication of CKD. The kidneys play a crucial role in regulating blood pressure, and as their function declines, hypertension becomes more common. The normal range for blood pressure is typically considered to be 120/80 mmHg.
Choice D: Crackles in the lungs Crackles in the lungs are not a direct manifestation of CKD, but they can occur if the condition leads to fluid overload and heart failure, resulting in pulmonary edema. This is a secondary complication rather than a direct symptom of CKD.
Choice E: Lethargy and a general feeling of malaise are common in CKD due to the buildup of toxins and waste products in the blood that the kidneys can no longer effectively filter out. This can also lead to decreased mental sharpness and a reduced quality of life.
Choice F: Proteinuria, or the presence of excess protein in the urine, is a hallmark sign of CKD. It indicates damage to the kidneys’ filtering units, allowing protein that would normally be retained to leak into the urine. Persistent proteinuria is a sign of chronic kidney damage.
A nurse is instructing an ACLS class and covering heart rhythms and their treatment. Which of the following rhythms would signal the need for defibrillation?
Explanation
Choice A reason: Atrial fibrillation is not typically treated with defibrillation; it is usually managed with medication or other forms of rhythm control.
Choice B reason: Supraventricular tachycardia does not usually require defibrillation; it may be treated with vagal maneuvers or medication.
Choice C reason: Asystole, or the absence of a heartbeat, is not treated with defibrillation as there is no electrical activity to reset.
Choice D reason: Ventricular fibrillation is a life-threatening heart rhythm that requires immediate defibrillation to restore a normal heart rhythm.
Sign Up or Login to view all the 71 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
