Please set your exam date
Puerperium: Lochia, Pain management after birth
Study Questions
Nursing Interventions for Lochia
(select all that apply) A nurse is teaching a breastfeeding client about engorgement prevention and management.
What should the nurse include in the teaching?
No explanation
A nurse is educating a postpartum client about resuming sexual intercourse after delivery.
What information should the nurse provide to the client?
Explanation
The correct answer is choice B. Sexual intercourse may be uncomfortable due to vaginal dryness.According to Mayo Clinic, hormonal changes after pregnancy might leave the vagina dry and tender, especially if the client is breast-feeding.
This can cause pain and discomfort during sex.
The client can use lubricant or try alternative forms of intimacy to ease the discomfort.
Choice A is wrong because sexual intercourse can be resumed after 4 weeks postpartum only if the client feels comfortable and has no complications.The general recommendation is to wait until 6 weeks postpartum or until the provider clears the client for sex.
Choice C is wrong because sexual intercourse should not be avoided until lochia alba stops.
Lochia alba is the last stage of postpartum bleeding that lasts from 10 to 14 days after delivery.The client can resume sex before lochia alba stops if they feel ready and use contraception to prevent pregnancy.
Choice D is wrong because sexual intercourse may not cause uterine bleeding or infection if the client follows proper hygiene and uses protection.The risk of complications is highest during the first two weeks after delivery, but it decreases after that.
A nurse is assessing a client who is 2 days postpartum.
Which of the following findings should the nurse expect?
Explanation
The correct answer is choice A. Lochia rubra.This is because lochia rubra is the first stage of postpartum bleeding and discharge, which lasts for about three to four days after giving birth.Lochia rubra is dark or bright red in color and contains blood, mucus, uterine tissue and other materials from the uterus.
Choice B.Lochia serosa is wrong because lochia serosa is the second stage of postpartum bleeding and discharge, which lasts for four to 12 days after giving birth.Lochia serosa is pinkish brown in color and thinner and more watery than lochia rubra.
Choice C.Lochia alba is wrong because lochia alba is the third and final stage of postpartum bleeding and discharge, which lasts from about 12 days to six weeks after giving birth.Lochia alba is yellowish white in color and contains little to no blood.
Choice D.No lochia is wrong because lochia is a normal part of the postpartum healing process and does not usually cause complications.Lochia helps clear the uterus of any residual tissue, blood and fluid after pregnancy.No lochia may indicate a problem such as infection or retained placenta.
A nurse is caring for a client who is 4 days postpartum and has a vaginal birth with an episiotomy.
The client reports that her perineal area is sore and asks the nurse what she can do to relieve the discomfort.
Which of the following responses should the nurse make?
Explanation
The correct answer is choice C.“Take a warm sitz bath.” A sitz bath is a shallow bath that covers the hips and buttocks and can help reduce swelling and discomfort in the perineal area after delivery.A warm sitz bath can also ease the pain of urination and promote blood flow to the area for faster healing.
Choice A is wrong because applying heat to the perineum can increase inflammation and pain.Choice B is wrong because using an ice pack on the perineum can cause an uncomfortable, sudden sensation of coldness on the skin.Choice D is wrong because using a heating pad on the abdomen has no effect on the perineal area and can also increase inflammation.
A nurse is caring for a client who is 5 days postpartum and has a vaginal birth with an episiotomy.
The client reports that she has pain in her perineal area and asks the nurse what she can do to relieve the discomfort.
Explanation
The correct answer is choice D.“You should avoid straining during bowel movements.” This is because straining can cause pain and bleeding in the perineal area, especially if the client has an episiotomy or hemorrhoids.Straining can also worsen the damage to the pelvic floor muscles or the anal sphincter muscles that might have occurred during delivery.
Choice A is wrong because taking a laxative can cause diarrhea, dehydration, and electrolyte imbalance.Laxatives should only be used if prescribed by a health care provider.
Choice B is wrong because increasing fluid intake alone is not enough to prevent or treat constipation.Fluid intake should be combined with adequate fiber intake and physical activity.
Choice C is wrong because increasing fiber intake alone is not enough to prevent or treat constipation.Fiber intake should be combined with adequate fluid intake and physical activity.
Normal ranges for fluid intake are about 2 to 3 liters per day for a lactating woman and about 1.5 to 2 liters per day for a non-lactating woman.Normal ranges for fiber intake are about 25 to 35 grams per day for adults.Normal ranges for physical activity are about 150 minutes of moderate-intensity exercise per week for healthy adults.
A nurse is caring for a client who is 5 days postpartum and has a vaginal birth with an episiotomy.
The client reports that she has pain in her perineal area and asks the nurse what she can do to relieve the discomfort.
Which of the following responses should the nurse make?
Explanation
The correct answer is choice C.“Take a warm sitz bath.” A sitz bath is a shallow bath that covers the perineal area and can help relieve pain and swelling after a vaginal birth with an episiotomy.A sitz bath can also promote healing and prevent infection by keeping the area clean.
Choice A is wrong because applying heat to the perineum can increase swelling and inflammation.Choice B is wrong because ice packs should only be applied for 10 to 20 minutes at a time and removed for at least 10 minutes before reapplying.Ice packs are most effective in the first 24 to 72 hours after birth.
Choice D is wrong because using a heating pad on the abdomen has no effect on the perineal pain.Heating pads can also cause burns if used for too long or at a high temperature.
A nurse is caring for a client who is 1 week postpartum and has a vaginal birth with an episiotomy.
The client reports that she has pain in her perineal area and asks the nurse what she can do to relieve the discomfort.
Which of the following responses should the nurse make?
Explanation
The correct answer is choice C.“Take a warm sitz bath.” A sitz bath is a shallow bath that covers the perineum and can help relieve pain and swelling after a vaginal birth with an episiotomy.A sitz bath can also promote healing and prevent infection by keeping the area clean.
Choice A is wrong because applying heat to the perineum can increase inflammation and delay healing.Choice B is wrong because using an ice pack on the perineum is only recommended for the first 24 hours after delivery to reduce swelling.After that, ice can cause tissue damage and slow down blood flow to the area.Choice D is wrong because using a heating pad on the abdomen has no effect on the perineal pain and can also cause burns or overheating.
Normal ranges for postpartum perineal pain vary depending on the type and degree of injury, but generally it should improve within a few weeks.If the pain persists or worsens, or if there are signs of infection such as fever, foul-smelling discharge, or redness, it is important to seek medical attention.
A nurse is assessing the amount, color, odor, consistency, and presence of clots or tissue in the lochia of a postpartum client.
Which of the following findings should the nurse report as abnormal?
Explanation
The correct answer is choice D. Large clots on day 3 postpartum.This is because large clots indicate excessive bleeding and may be a sign of postpartum hemorrhage, which is a rare but potentially fatal condition that requires immediate medical attention.
Choice A is wrong because lochia rubra, which is dark or bright red blood, is normal for the first three to four days after birth.
Choice B is wrong because lochia serosa, which is pinkish brown discharge that’s less bloody looking, is normal for four to 12 days after birth.
Choice C is wrong because lochia alba, which is yellowish white discharge with little to no blood, is normal from about 12 days to six weeks after birth.
Normal ranges for lochia are:
• Lochia rubra: lasts for three to four days, flows like a heavy period, small clots are normal.
• Lochia serosa: lasts for four to 12 days, flow is moderate, less clotting or no clots.
• Lochia alba: lasts from about 12 days to six weeks, light flow or spotting, no clots.
A nurse is caring for a postpartum client who has a boggy uterus.
Which of the following actions should the nurse take?
Explanation
The correct answer is choice B. Encourage the woman to empty her bladder regularly.A boggy uterus is a condition that occurs when the uterus fails to contract properly after childbirth, leading to excessive bleeding and possible postpartum hemorrhage.One of the causes of a boggy uterus is bladder distension, which can prevent the uterus from contracting and returning to its normal position.Therefore, encouraging the woman to empty her bladder regularly can help reduce the risk of a boggy uterus and postpartum hemorrhage.
Choice A is wrong because administering oxytocics as prescribed is not an action that the nurse should take, but rather the physician or midwife.Oxytocics are medications that stimulate uterine contractions and are used to treat a boggy uterus when other methods fail.
Choice C is wrong because providing a peri-bottle with warm water for cleansing after each voiding or bowel movement is not an action that can prevent or treat a boggy uterus.It is a hygiene measure that can help prevent infection and promote healing of the perineal area after childbirth.
Choice D is wrong because advising the woman to avoid tampons is not an action that can prevent or treat a boggy uterus.It is a precautionary measure that can help prevent infection and irritation of the vaginal canal after childbirth.Tampons should be avoided for at least six weeks after delivery.
A nurse is assessing a postpartum client’s lochia and notes that it has an unpleasant odor.
Which of the following actions should the nurse take?
Explanation
The correct answer is choice C. Palpate the fundus for firmness.This is because an unpleasant odor of lochia (postpartum vaginal discharge) can indicate an infection or retained placental fragments in the uterus.Palpating the fundus can help assess the uterine involution and detect any abnormalities.
Choice A is wrong because documenting the finding is not enough to address the potential problem.The nurse should also notify the provider and take further actions as ordered.
Choice B is wrong because encouraging the woman to empty her bladder regularly is not related to the odor of lochia.It is a general measure to prevent urinary tract infections and promote uterine contraction.
Choice D is wrong because administering oxytocics as prescribed is not a nursing action for lochia with an unpleasant odor.Oxytocics are drugs that stimulate uterine contractions and are used to prevent or treat postpartum hemorrhage.
They do not affect the infection or retention of placental fragments.
Normal ranges for lochia are:
• Lochia rubra: dark or bright red blood, lasts for 3 to 4 days, flows like a heavy period, small clots are normal.
• Lochia serosa: pinkish brown discharge, lasts for 4 to 12 days, thinner and more watery than lochia rubra, moderate flow, less or no clots.
• Lochia alba: yellowish white discharge, lasts from 12 days to 6 weeks, light flow or spotting, no clots.
Lochia should have a stale, musty or metallic odor like menstrual blood.It should not smell fishy or foul, which can indicate an infection.
A nurse is caring for a postpartum client who reports heavy bleeding and large clots in her lochia.
Which of the following actions should the nurse take?
Explanation
The correct answer is choice C. Palpate the fundus for firmness.This is because uterine atony is the most common cause of postpartum hemorrhage and palpating the fundus can help assess the tone of the uterus and stimulate contractions.If the fundus is boggy or soft, the nurse should massage it gently until it becomes firm.
Choice A is wrong because documenting the finding in the client’s chart is not an immediate action to stop the bleeding and may delay the treatment.
Choice B is wrong because encouraging the woman to empty her bladder regularly is a preventive measure for postpartum hemorrhage, not a treatment.A full bladder can displace the uterus and prevent it from contracting properly.
Choice D is wrong because notifying the provider is not enough to manage postpartum hemorrhage.The nurse should initiate interventions such as oxytocin administration, uterine massage, bimanual compression, fluid replacement, and blood transfusion as needed.
Notifying the provider should be done after or along with these interventions.
A nurse is teaching a postpartum client about lochia and when to report abnormal findings.
Which of the following statements by the client indicates an understanding of the teaching?
Explanation
The correct answer is choice C.“I should report foul odor.” This indicates an understanding of the teaching because foul odor is a sign of infection and should be reported to the healthcare provider.Lochia is the normal vaginal discharge after childbirth that contains blood, mucus, uterine tissue and other materials.It has three stages: lochia rubra (red), lochia serosa (pinkish brown) and lochia alba (yellowish white).Lochia usually lasts for four to eight weeks.
Choice A is wrong because heavy bleeding is expected for the first few days after delivery and then gradually decreases.However, if the bleeding is excessive or does not slow down, it could indicate a postpartum hemorrhage and should be reported immediately.
Choice B is wrong because abdominal pain is normal after delivery as the uterus contracts and shrinks back to its pre-pregnancy size.However, if the pain is severe or does not improve with pain medication, it could indicate a complication such as infection or retained placenta and should be reported.
Choice D is wrong because perineal itching is common after delivery due to healing of the tissues and stitches.However, if the itching is accompanied by redness, swelling, discharge or fever, it could indicate an infection and should be reported.
Postpartum Infections
A nurse is caring for a client who has postpartum endometritis.
Which of the following clinical manifestations should the nurse expect?
Explanation
The correct answer is choice C. Abdominal pain.
Postpartum endometritis is an infection of the lining of the uterus that usually occurs after delivery.It can cause symptoms such as uterine tenderness, abdominal or pelvic pain, fever, malaise, and sometimes discharge.
Choice A is wrong because bradycardia is not a typical sign of postpartum endometritis.The infection can cause tachycardia, which is a fast heart rate.
Choice B is wrong because hypotension is not a common manifestation of postpartum endometritis.The infection can cause hypertension, which is high blood pressure, especially if it is complicated by sepsis or shock.
Choice D is wrong because clear vaginal discharge is not indicative of postpartum endometritis.The infection can cause foul-smelling or purulent discharge, which is a sign of bacterial involvement.
A nurse is caring for a client who has postpartum endometritis.
Which of the following interventions should the nurse include in the plan of care?
Explanation
The correct answer is choice A. Administer antibiotics as prescribed.
Postpartum endometritis is an infection of the lining of the uterus that can occur after delivery, especially after cesarean section.Antibiotics are the main treatment for this condition, as they can help eliminate the bacteria that cause the infection.
Choice B. Encourage ambulation as tolerated is wrong because ambulation may not be appropriate for a client with endometritis, as it may increase the risk of spreading the infection or causing bleeding.Ambulation is more beneficial for clients who have had uncomplicated vaginal deliveries or who are at risk of thromboembolism.
Choice C. Encourage the client to perform kegel exercises is wrong because kegel exercises are not helpful for endometritis, as they do not affect the uterine lining.
Kegel exercises are more useful for clients who have had vaginal deliveries or who have urinary incontinence
More questions
(from search results) A nurse discovers a postpartum client with a boggy uterus, displaced above the right of the umbilicus.
What nursing action is indicated?
Explanation
The correct answer is choice D. Both A and B.A boggy uterus is a uterus that is enlarged, soft, and tender due to the failure of the uterus to contract sufficiently after delivery.This condition is called uterine atony and it is the most common cause of postpartum hemorrhage.Postpartum hemorrhage is excessive bleeding after childbirth that can lead to shock and death if not treated promptly.
The nursing actions indicated for a boggy uterus are:
• Perform immediate fundal massage: This helps to stimulate uterine contractions and reduce bleeding.
• Ambulate to the bathroom or use bedpan to empty bladder: This helps to reduce bladder distension and allow the uterus to contract and descend into the pelvis.
Choice A is partially correct but not sufficient by itself.
Choice B is also partially correct but not sufficient by itself.Choice C is incorrect because administering oxytocin alone may not be effective in restoring uterine tone if there are other factors contributing to uterine atony, such as overdistension, prolonged labor, or infection.Oxytocin is a hormone that stimulates uterine contractions.
(from search results) What factor places the postpartum client at risk for thromboembolism?
Explanation
The correct answer is choice A. Increased clotting factors.Increased clotting factors are a physiological adaptation to pregnancy that reduces the risk of hemorrhage during delivery, but also increases the risk of venous thromboembolism (VTE) in pregnancy and postpartum.The risk of VTE is highest in the first week after delivery and gradually declines over the next 12 weeks.
Choice B is wrong because decreased blood volume is not a risk factor for VTE.In fact, blood volume increases by about 50% during pregnancy to meet the increased metabolic demands of the mother and fetus.
Choice C is wrong because increased cardiac output is not a risk factor for VTE.
Cardiac output also
(select all that apply, from search results) What are three signs of positive bonding between parents and newborn?
Explanation
The correct answer is choices A, B and C.These are three signs of positive bonding between parents and newborn.
Calling infant by name shows recognition and affection.
Exploration of newborn head-to-toe shows curiosity and interest.
In face position shows eye contact and communication.
Choice D is wrong because avoiding eye contact with newborn is a sign of detachment or depression.Choice E is wrong because holding newborn close to chest may prevent eye contact and facial expressions.
Positive bonding is essential for a baby’s healthy development and attachment.
It makes parents want to shower their baby with love and care, and it makes babies feel secure and confident.Bonding can happen at any time, but it usually starts right after birth or adoption.
A nurse is assessing a client who delivered an infant vaginally 2 days ago and notes that the fundus is firm, midline, and at the level of the umbilicus, lochia rubra is moderate, and there are no clots present in the lochia flow.
Which of the following actions should the nurse take?
Explanation
The correct answer is choice A) Document findings as normal.
The fundus is the upper part of the uterus that contracts after delivery to prevent bleeding.The fundus should be firm, midline, and at the level of the umbilicus or lower on the second postpartum day.Lochia rubra is the normal bloody discharge that occurs for the first few days after delivery and should not contain large clots.The normal range of lochia rubra is scant to moderate.
Choice B) Massage fundus until it becomes firm is wrong because the fundus is already firm and does not need further stimulation.
Choice C) Administer oxytocin (Pitocin) is wrong because oxytocin is a medication that helps the uterus contract and is not indicated for a firm fundus.
Choice D) Increase IV fluid rate is wrong because IV fluids are not related to the assessment of the fundus and lochia and may cause fluid overload.
A nurse is caring for a client who delivered an infant vaginally 2 days ago and notes that there are no clots present in the lochia flow, but there is moderate bleeding with bright red blood and small clots present when massaging the fundus which is firm, midline, and at the level of the umbilicus.
Explanation
The correct answer is choice C) Administer oxytocin (Pitocin).Oxytocin is a hormone that stimulates uterine contractions and helps reduce postpartum bleeding by closing off the blood vessels that were attached to the placenta.
The nurse should administer oxytocin as ordered by the provider to help the client’s uterus contract and prevent hemorrhage.
Choice A) Document findings as normal is wrong because moderate bleeding with bright red blood and small clots is not normal for lochia flow 2 days after delivery.Lochia is the vaginal discharge that occurs after birth and consists of blood, tissue, mucus and bacteria.Lochia should be dark or bright red for the first 3 to 4 days, but the flow should be light and there should be no clots.Moderate bleeding with bright red blood and small clots indicates that the client may have retained placental fragments or uterine atony.
Choice B) Massage fundus until it becomes firm is wrong because the fundus is already firm, midline and at the level of the umbilicus, which indicates that the uterus is contracted properly.Massaging the fundus when it is already firm can cause more bleeding and pain.
Choice D) Increase IV fluid rate is wrong because increasing IV fluid rate will not stop the bleeding or address the underlying cause.Increasing IV fluid rate may also cause fluid overload or dilutional coagulopathy.The nurse should monitor the client’s vital signs, urine output and hematocrit levels to assess for signs of hypovolemia or anemia due to blood loss.
A nurse is assessing a postpartum client who delivered vaginally 2 days ago and notes that her fundus is boggy and displaced to the right side of her abdomen.
Which of the following actions should the nurse take first?
Explanation
The correct answer is choice D. Massage her fundus.
This is because a boggy and displaced fundus indicates uterine atony, which is the failure of the uterus to contract sufficiently after delivery.
This can lead to excessive bleeding and postpartum hemorrhage.Massaging the fundus can help stimulate uterine contractions and reduce blood loss.
Choice A is wrong because administering oxytocin is not the first action the nurse should take.Oxytocin is a medication that can also help the uterus contract, but it should be given after massaging the fundus and assessing the bleeding.
Choice B is wrong because assisting with ambulation is not appropriate for a client with a boggy and displaced fundus.Ambulation can increase bleeding and cause orthostatic hypotension due to blood loss.
Choice C is wrong because encouraging frequent voiding is not the first action the nurse should take.
A full bladder can displace the uterus and prevent effective contractions, so voiding can help the uterus return to its normal position.However, this should be done after massaging the fundus and assessing the bleeding.
A nurse is caring for a postpartum client who reports heavy vaginal bleeding and passing large clots since delivery 2 days ago.
Which of the following actions should the nurse take first?
Explanation
The correct answer is choice B. Palpate fundus.The nurse should first assess the tone of the uterus by palpating the fundus, as uterine atony is the most common cause of postpartum hemorrhage.
If the uterus is boggy or soft, the nurse should massage it gently until it becomes firm and contracts.
This will help control the bleeding from the placental site.
Choice A is wrong because assessing vital signs is not the first priority in this situation.Vital signs may not reflect the severity of blood loss until late in the process of hemorrhage.
The nurse should monitor vital signs after ensuring that the uterus is contracted.
Choice C is wrong because administering oxytocin as prescribed is not the first action the nurse should take.
Oxytocin is a medication that stimulates uterine contractions and reduces bleeding, but it should be given
A nurse is caring for a postpartum client who delivered vaginally yesterday and has been experiencing heavy vaginal bleeding since delivery.
Which of the following actions should the nurse take first?
Explanation
The correct answer is B. Palpate fundus.
The nurse should first assess the fundus to determine if it is firm and at the expected level of involution.
A boggy or displaced fundus can indicate uterine atony, which is the most common cause of postpartum hemorrhage.
By massaging the fundus, the nurse can stimulate uterine contractions and reduce bleeding.
A. Assess vital signs.
This statement is wrong because assessing vital signs is not the first action the nurse should take.
Vital signs can indicate the severity of blood loss and shock, but they do not address the cause of bleeding.
C. Administer oxytocin as prescribed.
This statement is wrong because administering oxytocin is not the first action the nurse should take.
Oxytocin is a medication that can enhance uterine contractions and reduce bleeding, but it should be given after assessing and massaging the fundus.
D. Check perineal pad.
This statement is wrong because checking perineal pad is not the first action the nurse should take.
Checking perineal pad can help estimate the amount of blood loss, but it does not address the cause of bleeding.
A nurse is caring for a client who has postpartum endometritis and is receiving IV antibiotics.
Which of the following findings indicates that the treatment is effective? A) Decreased vaginal bleeding.
Explanation
The correct answer is D) Decreased white blood cell count.Postpartum endometritis is an infection of the lining of the uterus that causes fever, abdominal pain, uterine tenderness and sometimes discharge.It is usually caused by bacteria from the lower genital or gastrointestinal tract.White blood cell count is a marker of inflammation and infection, so a decreased white blood cell count indicates that the treatment is effective and the infection is resolving.
A) Decreased vaginal bleeding is not a sign of effective treatment for postpartum endometritis.
Vaginal bleeding after delivery is normal and gradually decreases over time.It is not related to the infection of the uterus.
B) Increased abdominal pain is a sign of worsening infection, not effective treatment.Abdominal pain is one of the symptoms of postpartum endometritis and should improve with antibiotic therapy.
C) Increased temperature is also a sign of worsening infection, not effective treatment.Fever is another symptom of postpartum endometritis and should decrease with antibiotic therapy.
A nurse is caring for a client who has postpartum endometritis and is receiving IV antibiotics.
Which of the following instructions should the nurse include in the plan of care? A) Encourage fluid intake to promote hydration.
Explanation
The correct answer is choice A) Encourage fluid intake to promote hydration.
This is because hydration helps to flush out the infection and prevent dehydration from fever.
Fluid intake also supports milk production for breastfeeding.
Choice B) Instruct the client to avoid ambulation until symptoms resolve is wrong because ambulation promotes blood circulation and prevents thrombosis.
Ambulation also helps to expel lochia and reduce uterine cramping.
Choice C) Administer analgesics as prescribed to manage pain is correct but not the best answer.
Pain management is important for comfort and healing, but it does not address the underlying infection.
Choice D) Instruct the client to avoid breastfeeding until symptoms resolve is wrong because breastfeeding helps to contract the uterus and prevent bleeding.
Breastfeeding also provides immunity and nutrition to the newborn.
The infection is not transmitted through breast milk.
Choice E) Encourage frequent voiding is correct but not the best answer.
Frequent voiding helps to prevent urinary tract infections and bladder distension.
However, it does not directly affect the endometrial infection.
A nurse is caring for a client who has postpartum endometritis and is receiving IV antibiotics.
Which of the following findings indicates that the client is experiencing an adverse effect of the medication?
Explanation
The correct answer is choice A) Nausea and vomiting.This is because nausea and vomiting are common adverse effects of many antibiotics, especially clindamycin and gentamicin, which are often used to treat postpartum endometritis.Nausea and vomiting can also indicate a more serious complication of antibiotic therapy, such as Clostridioides difficile infection.
Choice B) Increased appetite is wrong because antibiotics do not typically affect appetite, and postpartum endometritis may cause loss of appetite due to fever, pain, and inflammation.
Choice C) Increased urine output is wrong because antibiotics do not usually increase urine output, and postpartum endometritis may cause dehydration due to fever and vomiting.
Choice D) Decreased heart rate is wrong because antibiotics do not generally lower heart rate, and postpartum endometritis may cause tachycardia due to fever, infection, and sepsis.
Question 48.
A client who has undergone a cesarean section is experiencing abdominal pain and tenderness.
Which of the following should the nurse assess for?
Explanation
The correct answer is choice E) Signs of peritonitis.
Peritonitis is an inflammation of the lining of the abdominal cavity that can be caused by an infection or a perforation of an organ.
It can cause severe abdominal pain and tenderness, fever, nausea, vomiting, and decreased bowel sounds.Peritonitis is a medical emergency that requires immediate treatment with antibiotics and surgery
Choice A) Bowel sounds is wrong because bowel sounds are normal and expected after a cesarean section.
They indicate that the intestines are functioning properly and moving food and gas through the digestive tract.Bowel sounds may be decreased or absent if there is an obstruction, ileus, or peritonitis
Choice B) Lochia amount is wrong because lochia is the vaginal discharge that occurs after childbirth.
It consists of blood, mucus, and tissue from the uterus.
Lochia amount is not related to abdominal pain and tenderness after a cesarean section.
Lochia amount may vary depending on the stage of lochia (rubra, serosa
A nurse is caring for a postpartum client who has an episiotomy wound infection.
Which of the following should the nurse do? (Select all that apply.) A) Administer antibiotics as prescribed.
Explanation
The correct answer is choice A, B, C and D. Antibiotics, wound monitoring, wound care and wound culture are all appropriate interventions for a postpartum client who has an episiotomy wound infection.According to Mayo Clinic, an episiotomy wound infection can cause pain, fever, pus and wound breakdown.According to SpringerLink, an episiotomy wound infection is usually caused by a polymicrobial infection of Gram-negative and Gram-positive bacteria.
Therefore, administering antibiotics as prescribed can help treat the infection and prevent complications.
Monitoring wound healing can help detect any signs of worsening infection or dehiscence.
Teaching wound care can help the client prevent further contamination and promote healing.
Culturing the wound if indicated can help identify the causative organisms and guide antibiotic therapy.
Choice E is wrong because applying heat to the wound can increase inflammation and pain.According to NCBI, there is no evidence that heat therapy is beneficial for episiotomy wounds.
Instead, cold therapy may be more effective in reducing swelling and discomfort.
A nurse is assessing a postpartum client for signs of infection.
Which of the following should the nurse report immediately? A) Lochia with clots.
Explanation
The correct answer is choice E) Temperature greater than 38°C for more than 48 hours.This is because a fever higher than 38°C that lasts for more than two days can indicate a postpartum infection, which is a potentially serious complication that requires immediate medical attention.A postpartum infection can affect various parts of the body, such as the uterus, the breast, or the urinary tract.
Choice A) Lochia with clots is wrong because lochia is the normal vaginal discharge that occurs after childbirth and may contain some blood clots.However, if the lochia is foul-smelling, excessive, or bright red, it may be a sign of infection.
Choice B) Fundus firmness is wrong because a firm fundus (the top of the uterus) indicates that the uterus is contracting well and preventing excessive bleeding.A soft or boggy fundus can be a sign of infection or hemorrhage.
Choice C) Abdominal distension is wrong because some abdominal swelling is normal after delivery and may take several weeks to subside.However, if the abdomen is very tender, painful, or hard, it may be a sign of infection or other complications.
Choice D) Breast tenderness is wrong because some
(Select all that apply) A nurse is monitoring a postpartum woman who is taking codeine for severe pain after birth.
The nurse knows that codeine can pass through breastmilk and cause adverse effects in the baby.
Which signs and symptoms should the nurse watch for in the baby?
Explanation
Increased sleepiness and difficulty waking up are signs of central nervous system (CNS) depression in breastfed infants exposed to codeine through breast milk.Codeine is converted into morphine in the body, which can pass into breast milk and cause adverse effects in the baby.Codeine use by breastfeeding mothers can cause CNS depression in breastfed infants.
Therefore, the nurse should watch for increased sleepiness and difficulty waking up in the baby.
Choice A is wrong because increased alertness and activity are not signs of CNS depression.
They are more likely to be signs of stimulation or agitation.
Choice B is wrong because decreased appetite and weight gain are not specific signs of codeine exposure.
They can be caused by many other factors, such as illness, infection, or poor latch.
Choice C is wrong because increased respiratory rate and depth are not signs of CNS depression.
They are more likely to be signs of respiratory distress or infection.
Choice D is wrong because decreased heart rate and blood pressure are not signs of CNS depression.
They are more likely to be signs of shock or hypovolemia.
Normal ranges for vital signs in newborns are:
• Heart rate: 100 to 160 beats per minute
• Respiratory rate: 30 to 60 breaths per minute
A nurse is evaluating a postpartum woman’s knowledge about pain management after birth.
The nurse asks the woman what she would do if she has uterine cramping while breastfeeding her baby.
Which response by the woman indicates a need for further teaching?
Explanation
The correct answer is choice D. I would stop feeding my baby until the pain goes away.This response indicates a need for further teaching because stopping breastfeeding can worsen the uterine cramping and also affect the milk supply and the baby’s nutrition.Uterine cramping or “afterpains” are normal after delivery and are caused by the uterus contracting and shrinking back to its normal size.Breastfeeding can trigger these contractions because it stimulates the release of oxytocin, a hormone that helps the uterus contract.
Choice A is wrong because ibuprofen is a safe and effective pain reliever for postpartum women and can be taken before feeding the baby.Choice B is wrong because massaging the abdomen gently during feeding can help ease the afterpains by stimulating blood flow and relaxing the muscles.Choice C is wrong because relaxation and breathing techniques can also help reduce the pain by lowering stress and tension levels.These are some of the self-help treatments that can be used along with medications to manage postpartum pain.
A nurse is preparing a discharge plan for a postpartum woman who had a vaginal delivery with a second-degree perineal tear.
The nurse includes instructions on how to care for the perineum at home.
Which statement by the woman indicates that she understands the instructions?
Explanation
The correct answer is choice A.The woman should change her perineal pad every time she uses the bathroom to prevent infection and promote healing of the perineal area.
Some possible explanations for the other choices are:
• Choice B is wrong because the woman should wipe her perineum from front to back after urinating or defecating to avoid introducing bacteria from the anus to the vagina or urethra.
• Choice C is wrong because the woman should apply ice packs on her perineum for the first 24 hours after birth, not for the first week.
Ice packs help reduce swelling and pain in the per
A nurse is providing discharge teaching to a client who had a vaginal delivery with a midline episiotomy.
Which of the following instructions should the nurse include in the teaching? (Select all that apply.)
Explanation
The correct answer is choice A, C, D and E. These are the instructions that the nurse should include in the teaching for a client who had a vaginal delivery with a midline episiotomy.
• Choice A is correct because using a sitz bath three times per day and after each bowel movement can help reduce pain, swelling and infection of the perineum.
• Choice C is correct because applying ice packs to the perineum for the first 24 hours can help reduce inflammation and bleeding.
• Choice D is correct because performing Kegel exercises several times per day can help strengthen the pelvic floor muscles and improve urinary continence.
• Choice E is correct because reporting any increase in redness, swelling or discharge from the episiotomy site can help detect signs of infection or wound breakdown.
• Choice B is wrong because wiping from back to front after voiding or having a bowel movement can increase the risk of infection by introducing bacteria from the anal area to the vaginal area.The correct way to wipe is from front to back.
A nurse is caring for a client who received meperidine (Demerol) IV for pain relief during labor 2 hours ago and is now ready to deliver vaginally.
Which of the following medications should the nurse have available to reverse respiratory depression in the newborn?
Explanation
Naloxone (Narcan) is a specific opiate antagonist that can reverse respiratory depression in newborn infants that may be due to transplacentally acquired opiates.It can be given intravenously, intramuscularly, intraosseously or subcutaneously.The recommended dose is 100 microgram/kg.
Choice B is wrong because nalbuphine (Nubain) is a mixed opiate agonist-antagonist that can cause respiratory depression and withdrawal symptoms in opioid-dependent mothers and infants.
Choice C is wrong because butorphanol (Stadol) is another mixed opiate agonist-antagonist that can have similar effects as nalbuphine.
Choice D is wrong because fentanyl (Sublimaze) is a synthetic opioid that can cause respiratory depression and sedation in both mothers and infants.
Normal ranges for respiratory rate in newborn infants are 30 to 60 breaths per minute.
Normal ranges for oxygen saturation in newborn infants are 90% to 100%.
entanyl (Sublimaze) is a synthetic opioid that can cause respiratory depression and sedation in both mothers and infants.
Normal ranges for respiratory rate in newborn infants are 30 to 60 breaths per minute.
Normal ranges for oxygen saturation in newborn infants are 90% to 100%.
Explanation
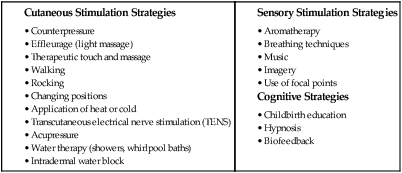
The correct answer is choice A, C, D and E. These are all non-pharmacological methods of pain relief that can be used during labor.They work by providing natural pain relief, increasing endorphins, creating competing impulses in the nervous system, or reducing muscle tension and anxiety.
Choice B, biofeedback, is wrong because it is a technique that involves monitoring and controlling physiological responses such as heart rate, blood pressure, muscle tension, and brain waves.It requires special equipment and training and is not commonly used during labor.
Normal ranges for pain during labor vary depending on the individual, the stage of labor, and the method of pain relief.Some factors that can influence pain perception are fear, anxiety, fatigue, previous experiences, expectations, and coping skills.
Exams on Puerperium: Lochia, Pain management after birth
Custom Exams
Login to Create a Quiz
Click here to loginLessons
Notes Highlighting is available once you sign in. Login Here.
Introduction
Introduction
-
Puerperium is the period of time from the delivery of the placenta to the return of the reproductive organs to their pre-pregnancy state, usually lasting 6 to 8 weeks.
-
Lochia is the vaginal discharge that occurs after birth, consisting of blood, mucus, tissue, and white blood cells. It changes in color, amount, and odor over time as the uterus heals and contracts.
-
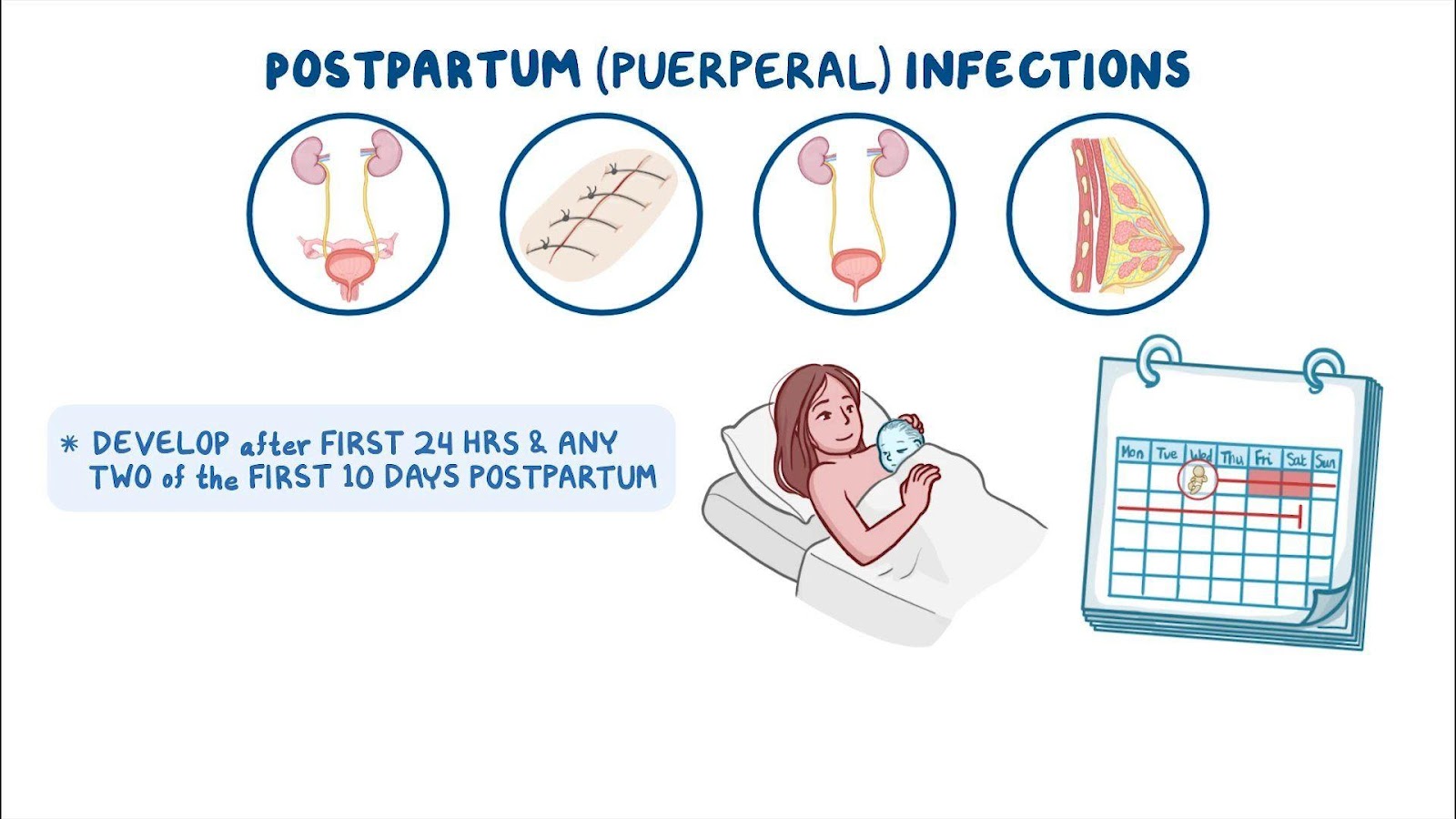
Postpartum infections and complications are common causes of maternal morbidity and mortality, especially in low-resource settings. They include excessive uterine bleeding, endometritis, salpingitis, pelvic abscess, peritonitis, wound infection, mastitis, breast abscess, urinary tract infection, sepsis, and thromboembolism.
-
Pain management after birth is essential for the woman’s comfort, recovery, mobility, breastfeeding, and bonding with her baby. It involves a combination of pharmacological and non-pharmacological methods tailored to the woman’s needs an
Objectives
Objectives
-
Define puerperium and lochia and describe their normal characteristics and variations.
-
Identify the common causes and risk factors of postpartum infections and complications.
-
Explain the nursing interventions and management for preventing and treating postpartum infections and complications.
-
Describe the pharmacological and non-pharmacological methods of pain relief after birth and their indications, contraindications, and side effects.
-
Educate the woman and her partner on self-care, hygiene, breastfeeding, warning signs, and follow-up care after birth.
-
Promote maternal-infant bonding and attachment and provide emotional support to the woman and her partner.
Nursing Interventions for Lochia
-
Assess the amount, color, odor, consistency, and presence of clots or tissue in the lochia at least every 8 hours or more frequently if indicated.
-
Monitor vital signs, especially temperature and pulse, for signs of infection or hemorrhage.
-
Palpate the fundus for firmness, height, position, and tenderness. Massage gently if boggy or displaced by a full bladder. Administer oxytocics as prescribed to enhance uterine contraction.
-
Encourage the woman to empty her bladder regularly and maintain good perineal hygiene. Provide a peri-bottle with warm water for cleansing after each voiding or bowel movement. Change pads frequently and wash hands before and after.
-
Teach the woman about the normal changes in lochia and when to report abnormal findings such as heavy bleeding, large clots, foul odor, fever, chills, abdominal pain, or pelvic tenderness.
-
Advise the woman to avoid tampons, douching, sexual intercourse, tub baths, swimming pools, or hot tubs until the lochia has stopped and the cervix is closed.
Postpartum Infections
-
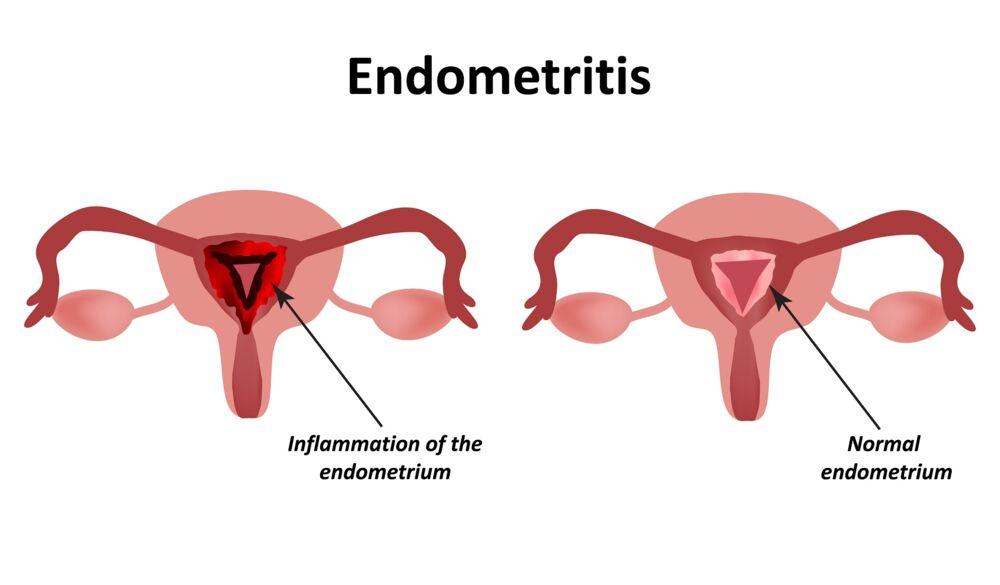
Postpartum endometritis: inflammation of the uterine lining caused by bacterial infection that ascends from the vagina or cervix during labor or delivery. It is more common after cesarean section, instrumental delivery, prolonged rupture of membranes, prolonged labor, multiple vaginal examinations, retained placenta, or manual removal of placenta.
-
Clinical features: fever (higher than 38°C for more than 48 hours), abdominal or pelvic pain, foul-smelling or purulent vaginal discharge, uterus enlarged, soft, painful when mobilized; open cervix; swelling in the posterior fornix
-
Management: admit to inpatient department; administer antibiotherapy such as amoxicillin/clavulanic acid IV plus gentamicin IM or ampicillin IV plus metronidazole IV plus gentamicin IM; continue treatment 48 hours after resolution of fever and other signs; look for retained placenta and perform uterine evacuation after 24 to 48 hours of antibiotherapy; if haemodynamically unstable due to hemorrhage or infection, perform uterine evacuation immediately
Pelvic abscess or peritonitis: complication of untreated puerperal endometritis/salpingitis; involves collection of pus in the pelvic cavity or inflammation of the peritoneum
-
Clinical features: abdominal guarding or spasm, ileus, pelvic mass
-
Management: laparotomy or colpotomy to drain the abscess; same antibiotherapy as for postpartum endometritis and salpingitis
-
Wound infection: infection of the surgical site (cesarean section) or episiotomy/laceration repair
-
Clinical features: fever, redness, swelling, pain, purulent drainage, dehiscence or separation of wound edges
-
Management: clean wound with sterile saline; apply sterile dressing; culture wound if indicated; administer antibiotics as prescribed; monitor wound healing; teach wound care.

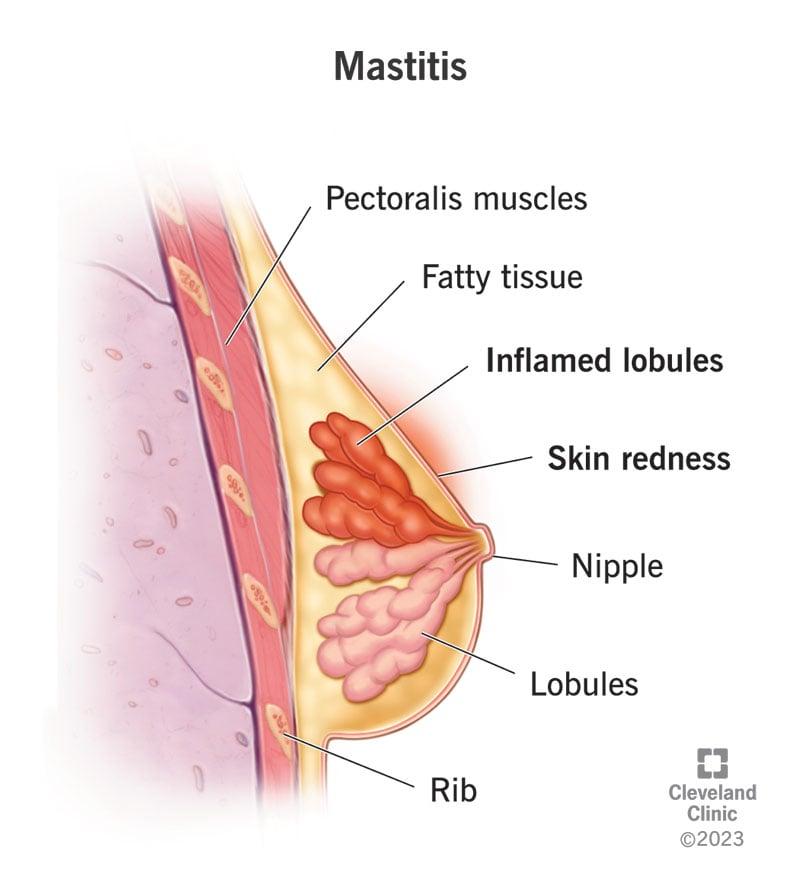
Mastitis: inflammation of the breast tissue caused by bacterial infection that enters through cracked nipples; usually affects one breast; more common in lactating women
-
Clinical features: fever, chills, malaise, headache, breast pain, tenderness, redness, swelling, hardness or induration of affected area
-
Management: continue breastfeeding or pumping from both breasts; apply warm compresses before feeding; massage affected area gently during feeding; vary breastfeeding positions; ensure proper latch-on technique; wear supportive bra; avoid tight clothing; change breast pads frequently; maintain good hygiene; drink plenty of fluids; rest; take analgesics as prescribed; take antibiotics as prescribed
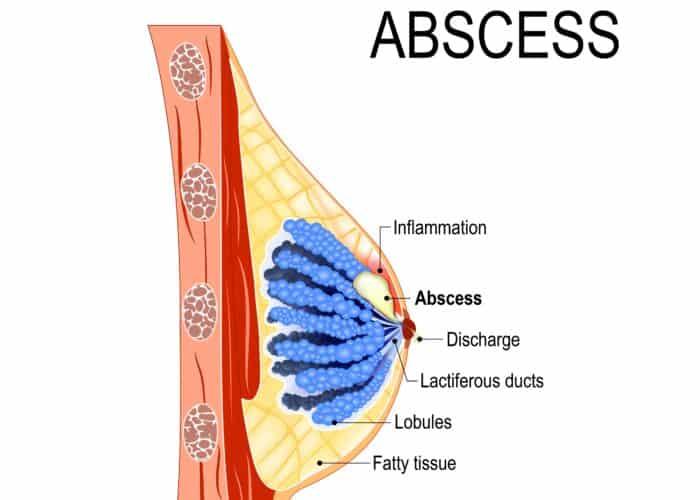
Breast abscess: complication of untreated mastitis; involves collection of pus in the breast tissue
-
Clinical features: fever, chills, malaise, headache, breast pain, tenderness, redness, swelling, hardness or induration of affected area; fluctuant mass; purulent drainage or fistula formation
-
Management: incision and drainage of abscess under local anesthesia; culture pus if indicated; apply sterile dressing; change dressing daily; administer antibiotics as prescribed; continue breastfeeding or pumping from unaffected breast; express milk manually from affected breast until healed
Nursing Interventions for Postpartum Infections
Nursing Interventions for Postpartum Infections
-
Assess vital signs every 4 hours or more frequently if indicated; report fever higher than 38°C for more than 48 hours or other signs of infection such as tachycardia, hypotension, tachypnea or dyspnea
-
Assess lochia for amount, color, odor, consistency and presence of clots or tissue; report heavy bleeding, large clots, foul odor or purulent discharge
-
Assess fundus for firmness, height, position and tenderness; massage gently if boggy or displaced by full bladder; administer oxytocics as prescribed to enhance uterine contraction
-
Assess abdomen for distension, guarding or spasm; auscultate bowel sounds; report ileus or signs of peritonitis such as rebound tenderness or rigidity
-
Assess wound for redness, swelling, pain, purulent drainage or dehiscence; clean wound with sterile saline; apply sterile dressing; culture wound if indicated; administer antibiotics as prescribed; monitor wound healing; teach wound care
-
Assess breasts for pain, tenderness, redness, swelling or hardness; palpate for fluctuant mass; express milk manually from affected breast until healed; culture pus if indicated; administer antibiotics as prescribed; monitor abscess healing; teach breast care
-
Encourage fluid intake of at least 3 liters per day unless contraindicated; offer nutritious diet rich in protein, vitamins and minerals to promote healing and immunity
-
Provide comfort measures such as analgesics (paracetamol), antipyretics (ibuprofen), cold or warm compresses on perineum or breasts (depending on preference), sitz bath (after episiotomy), ice packs on perineum (for first 24 hours), pillow support for abdomen (after cesarean section) or breasts (when engorged)
-
Educate the woman and her partner on self-care measures such as emptying bladder regularly; maintaining good perineal hygiene; changing pads frequently; washing hands before and after; avoiding tampons,douching,tub baths,pools,hottubs until lochia stops
Pain Management After Birth
Pain Management After Birth
-
Pain after birth can be caused by various factors, such as uterine contractions, perineal trauma, breast engorgement, nipple soreness, wound healing, or infection. Pain can affect the woman’s comfort, recovery, mobility, breastfeeding, and bonding with her baby.
-
Pain management after birth involves a combination of pharmacological and non-pharmacological methods tailored to the woman’s needs and preferences. The choice of pain relief depends on the type, intensity, and duration of pain, as well as the woman’s medical history, allergies, contraindications, and side effects.
-
Pharmacological methods of pain relief include:
-
Paracetamol: an over-the-counter analgesic and antipyretic that is safe to take while breastfeeding. It can be used for mild to moderate pain such as headache, backache, or perineal discomfort. The usual dose is 500 to 1000 mg every 4 to 6 hours as needed, not exceeding 4 g per day.
-
Ibuprofen: an over-the-counter nonsteroidal anti-inflammatory drug (NSAID) that has analgesic, antipyretic, and anti-inflammatory effects. It can be used for moderate to severe pain such as uterine cramping, perineal swelling, or wound inflammation. It is also safe to take while breastfeeding. The usual dose is 200 to 400 mg every 4 to 6 hours as needed, not exceeding 1.2 g per day.
-
Codeine: a prescription opioid analgesic that can be used for severe pain that is not relieved by paracetamol or ibuprofen. It can be combined with paracetamol or ibuprofen for enhanced pain relief. It can pass through breastmilk and cause sedation or respiratory depression in the baby, so it should be used with caution and only for a short period of time. The usual dose is 30 to 60 mg every 4 to 6 hours as needed, not exceeding 240 mg per day.
-
-
Non-pharmacological methods of pain relief include:
-
Relaxation and breathing techniques: the same methods used during labor can help alleviate pain after birth as well. They include deep breathing, progressive muscle relaxation, guided imagery, meditation, music therapy, aromatherapy, or hypnosis.
-
Cold or warm compresses: applying cold packs on the perineum for the first 24 hours after birth can reduce swelling and inflammation. Applying warm compresses on the perineum after the first day or on the breasts before feeding can increase blood flow and ease pain.
-
Sitz bath: soaking the perineum in warm water for 10 to 15 minutes several times a day can help clean the area, promote healing, and relieve discomfort. It can be done after an episiotomy or a perineal tear.
-
Ice packs: applying ice packs on the breasts after feeding can reduce engorgement and inflammation. A bag of frozen peas makes a nice ice pack.
-
Massage: gently massaging the affected area during feeding can help drain the milk ducts and prevent clogging. Massaging the abdomen can also help stimulate uterine contractions and reduce bleeding.
-
Pillow support: using pillows to support the abdomen after a cesarean section or the breasts when engorged can reduce pressure and pain.
-
Mobility: starting to walk soon after birth can help improve circulation, prevent thrombosis, reduce gas pain, and enhance recovery. However, avoid strenuous activity or lifting heavy objects until fully healed.
-
Nursing Interventions for Pain Management After Birth
Nursing Interventions for Pain Management After Birth
-
Assess the woman’s level of pain using a valid and reliable pain scale such as the numeric rating scale (0 to 10) or the visual analog scale (a line with anchors such as “no pain” and “worst pain”). Ask about the location, frequency, duration, quality, and aggravating or relieving factors of pain
-
Administer analgesics as prescribed or advise on over-the-counter options; monitor for effectiveness and side effects; educate on dosage, frequency, and precautions
-
Provide comfort measures such as relaxation and breathing techniques, cold or warm compresses, sitz bath, ice packs, massage, pillow support, or mobility; assist as needed or teach how to perform
-
Encourage breastfeeding or pumping from both breasts; ensure proper latch-on technique; vary breastfeeding positions; offer nipple care products such as lanolin cream or hydrogel pads; refer to lactation consultant if needed
-
Educate the woman and her partner on self-care measures such as drinking plenty of fluids; eating a nutritious diet; resting when possible; avoiding tight clothing; changing breast pads frequently; maintaining good hygiene; reporting signs of infection or complications
Conclusion
Conclusion
Puerperium is a period of physical and emotional adjustment for the woman and her baby. Lochia is a normal vaginal discharge that reflects the healing process of the uterus. Postpartum infections and complications are potential threats to maternal health that require prompt diagnosis and treatment. Pain management after birth is essential for the woman’s comfort, recovery, mobility, breastfeeding, and bonding with her baby. It involves a combination of pharmacological and non-pharmacological methods tailored to the woman’s needs and preferences.
-
The nursing role in caring for women during puerperium includes preventing the spread of infection, promoting healing, improving attachment/bonding of parent and infant, providing education and support, and facilitating referrals if needed.
Summary
Summary;
-
Puerperium: period from delivery of placenta to return of reproductive organs to pre-pregnancy state (6 to 8 weeks)
-
Lochia: vaginal discharge after birth (blood,mucus,tissue,WBCs); changes in color (rubra-serosa-alba), amount (decreases), odor (fleshy-mild-slight) over time; should not be excessive,foul-smelling,purulent; report abnormal findings
-
Postpartum infections: common causes of maternal morbidity/mortality; include uterine bleeding,endometritis,salpingitis,pelvic abscess/peritonitis,wound infection,mastitis,breast abscess; signs include fever,pain,foul discharge,purulent drainage; management includes antibiotherapy,wound care,culture,dressing change,lactation support; report signs of sepsis or thromboembolism
-
Pain management after birth: essential for comfort,recovery,mobility,breastfeeding,bonding; involves pharmacological (paracetamol/ibuprofen/codeine) and non-pharmacological (relaxation/cold/warm compresses/sitz bath/ice packs/massage/pillow support/mobility) methods; assess level/location/frequency/duration/quality/factors of pain; administer analgesics; monitor effectiveness/side effects; provide comfort measures; educate on self-care
Nursingprepexams
Videos
Login to View Video
Click here to loginTake Notes on Puerperium: Lochia, Pain management after birth
This filled cannot be empty
