Exam Review
ATI PN Comprehensive Predictor 2023 - Exam 1
Total Questions : 180
Showing 10 questions, Sign in for moreA nurse on a pediatric unit is caring for a toddler who has poor dietary intake.
Which of the following actions should the nurse take first?
Explanation
In this scenario, the nurse should take the action of obtaining the child's dietary history first. By gathering information about the toddler's current dietary intake, the nurse can assess the specific problems and challenges the child may be facing.
This information will be crucial in developing an appropriate plan of care to address the poor dietary intake. Once the nurse has a clear understanding of the child's dietary habits, they can then proceed with other actions such as encouraging the family to be present during mealtimes, offering nutritious snacks, and providing instructions on praising the child when they eat.
However, obtaining the dietary history will provide essential information for the nurse to make informed decisions and interventions.
A nurse is reinforcing teaching with a client who is postpartum about the measles, mumps, and rubella (MMR) vaccine.
Which of the following instructions should the nurse include in the teaching?
Explanation
Explanation:
Avoid pregnancy for at least 28 days after receiving the vaccine: This is a crucial instruction for women of childbearing age. The MMR vaccine is a live attenuated vaccine, and women should avoid becoming pregnant for at least 28 days after receiving it to reduce the theoretical risk to the developing fetus. Pregnant women should not receive the MMR vaccine, and women who receive the vaccine should avoid getting pregnant for at least 28 days afterward.
Incorrect:
A- Avoid breastfeeding for 3 days after receiving the vaccine: This statement is not accurate. Breastfeeding is not contraindicated after receiving the MMR vaccine. In fact, breastfeeding is safe and can be continued as usual.
B- Your partner should also receive the MMR vaccine: While it is essential for individuals to be vaccinated against measles, mumps, and rubella for their own protection and to contribute to herd immunity, it is not a specific instruction given to the postpartum client.
C- If you are allergic to gluten, you should not receive this vaccine: The MMR vaccine does not contain gluten, and a gluten allergy is not a contraindication for receiving the vaccine.
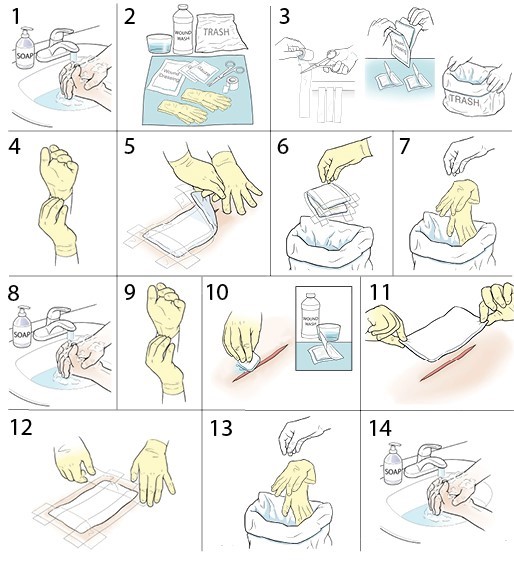
A nurse is preparing to perform a wet-to-dry dressing change for a client who has an infected abdominal wound.
Which of the following techniques should the nurse use when performing this dressing change?
Explanation
When removing the dressing and cleaning the wound, it is important to start from the center of the wound and work towards the outer edges. This technique helps prevent contamination of the wound by minimizing the risk of dragging bacteria or debris from the surrounding skin into the wound.
The other options listed are not recommended for this specific procedure:
When removing the tape, it is generally recommended to pull it parallel to the skin surface rather than pulling from the center of the dressing. This technique reduces the risk of causing trauma or disrupting the wound.
While it is important to maintain aseptic technique during dressing changes, wearing sterile gloves is not necessary for a wet-to-dry dressing change. Clean, non-sterile gloves are typically sufficient for this procedure, as the dressing material itself is not sterile.
In a wet-to-dry dressing change, the dressing is typically applied moist and allowed to dry over time. Therefore, moistening the dressing before removal is not necessary. The primary goal is to remove the dry dressing, which may adhere to the wound bed, and then clean the wound before applying a fresh dressing.
A nurse is reinforcing teaching with a female client about contraception.
Which of the following statements by the client indicates an understanding of the teaching?
Explanation
Explanation:
Using condoms correctly and consistently during intercourse is an effective method of contraception. It provides a barrier that prevents sperm from reaching the egg and also reducesthe risk of sexually transmitted infections (STIs). When both the client and their partner use a condom, it increases the effectiveness of contraception and provides protection against STIs.
Let's analyze the other statements:
A- "My partner will use condoms with spermicides": While using condoms with spermicides can provide additional contraceptive protection by immobilizing or killing sperm, it is not as effective as using condoms alone. Spermicides alone are not reliable enough to be used as a sole method of contraception.
C- "I will be able to remove my contraceptive sponge immediately after intercourse": The contraceptive sponge is a barrier method that is inserted into the vagina before intercourse. It should be left in place for at least 6 hours after intercourse to ensure effectiveness. Removing it immediately after intercourse would decrease its contraceptive effectiveness.
D- "My partner and I will use petroleum jelly with latex condoms": Petroleum jelly, along with other oil-based lubricants, should not be used with latex condoms. Oil-based substances can degrade latex, making the condom more prone to breakage. Water-based lubricants are recommended for use with latex condoms to ensure their integrity and effectiveness.

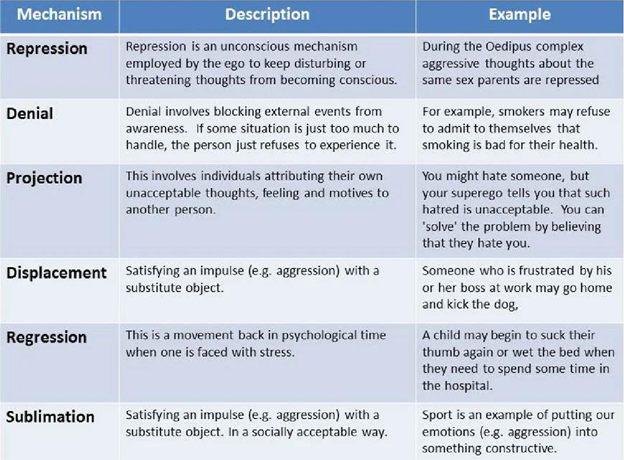
A nurse is caring for a client who has bipolar disorder. The client yells at the nurse whenever medication changes are prescribed by the client's provider.
The nurse should identify that the client is using which of the following defense mechanisms?
Explanation
Explanation:
Displacement is a defense mechanism in which an individual redirect their emotions or impulses from their original target to a less threatening or safer target. In this scenario, the client yells at the nurse when medication changes are prescribed by the provider. The client may be feeling angry or frustrated about the medication changes but is unable to express those emotions directly towards the provider. Instead, the client displaces those feelings onto the nurse, who may be seen as a safer or more accessible target. The yelling behavior directed at the nurse is a way for the client to release and express their emotions indirectly.
Let's briefly discuss the other defense mechanisms mentioned:
A- Conversion: Conversion involves the expression of psychological distress or conflict through physical symptoms or ailments. It is not applicable in this scenario since the client's behavior does not involve physical symptoms.
B- Splitting: Splitting is a defense mechanism characterized by a black-and-white thinking pattern, where individuals perceive others or situations as all good or all bad. It does not directly apply in this scenario as the client's behavior is not indicative of splitting.
D- Sublimation: Sublimation is a defense mechanism in which an individual channel their unacceptable or potentially harmful impulses into socially acceptable outlets, such as creative or productive activities. It is not evident in this scenario as the client's behavior does not involve transforming the emotions into a more positive or socially acceptable form.
A nurse is providing care to a client who is immunocompromised.
Which of the following should the nurse identify as a possible source of infection?
Explanation
Placing soiled linens on the floor can lead to cross-contamination and the spread of infectious agents. This can pose a risk to the immunocompromised client, who may be more susceptible to infections.
Lining waste containers with single bags helps contain potentially infectious waste and facilitates proper disposal. This reduces the risk of contamination and exposure to infectious materials.
Using dampened cloths for dusting helps minimize the spread of dust and airborne particles. Dampening the cloth can help capture the dust and prevent it from becoming airborne, reducing the potential for respiratory exposure.
Placing uncapped sharps in a puncture-resistant container is an essential practice to prevent needlestick injuries and the transmission of bloodborne pathogens. This ensures safe disposal of sharps and reduces the risk of accidental needlestick injuries to healthcare workers and clients.
A nurse is caring for a client who has peptic ulcer disease and is scheduled to undergo an esophagogastroduodenoscopy.
Which of the following actions should the nurse take prior to the procedure?
Explanation
Before any invasive procedure, it is essential to ensure that the client has given informed consent. Informed consent involves providing the client with detailed information about the procedure, its risks and benefits, and alternatives. The client should have the opportunity to ask questions and fully understand the procedure before giving consent.
Oral contrast solutions are typically used for imaging procedures such as CT scans or X-rays, not for esophagogastroduodenoscopy. This procedure involves the insertion of a flexible tube with a camera into the esophagus, stomach, and duodenum to visualize the upper gastrointestinal tract.
While it is important to provide the client with information about the duration of the procedure, stating a specific time frame may not be accurate or helpful. The duration of an esophagogastroduodenoscopy can vary depending on factors such as the complexity of the procedure and the client's individual circumstances.
Having a full bladder is not necessary for an esophagogastroduodenoscopy procedure. This requirement may be relevant for other procedures, such as pelvic ultrasound, but it is not applicable in this case.

A nurse is assisting in the care of a client. Nurses' Notes 2000:
Client presents to emergency department and states, "I have been assaulted." Client was immediately placed in a treatment room.
2015:
"Client states they were out with friends this evening and had "a little too much to drink." Client states that they fell asleep at their friend's house and when they woke up all of their clothes were off and their genitals were sore. The client states, "I think someone had sex with me, but I don't remember anything." Client reports history of depression. Client is a full-time college student who lives with roommates. Client admits to drinking socially but denies illicit drug use and tobacco use.
Which of the following interventions should the nurse plan to implement?
Select all that apply.
Explanation
Case management can be beneficial in situations involving assault to help coordinate and provide ongoing support and resources for the client. This intervention is appropriate in this scenario.
Ensuring a safe and private environment is crucial to protect the client's confidentiality and provide a supportive atmosphere during this difficult time. This intervention is necessary. Since the client reports being assaulted and has sore genitals, it is important to consider the risk of sexually transmitted infections (STIs). Administering STI prophylaxis can help prevent potential infections.
The client may benefit from additional support services such as counseling or support groups. Providing resources for local support services can help the client access the necessary help and support they need.
Contacting children and youth services is not applicable in this scenario as the client is a full-time college student and not a child or youth.
While the client mentioned drinking, it is not explicitly stated that they have an alcohol addiction or problem. Therefore, providing resources for Alcoholics Anonymous may not be the most appropriate intervention at this time.
A nurse is contributing to the plan of care for a client who has leukemia and is experiencing chronic fatigue.
Which of the following interventions should the nurse plan to include?
Explanation
Explanation:
Chronic fatigue is a common symptom experienced by clients with leukemia due to various factors, including the disease process, treatment side effects, and anemia. Encouraging strength- training exercises can be beneficial in managing fatigue in these clients. Engaging in regular physical activity, especially strength-training exercises, has been shown to improve muscle strength, endurance, and overall energy levels.
Strength-training exercises help build muscle mass and improve cardiovascular fitness, which can combat fatigue and enhance the client's ability to perform activities of daily living. However, it is essential to individualize the exercise plan based on the client's current physical abilities and energy levels. The nurse should work closely with the client and, if available, a physical therapist or exercise specialist to develop a safe and appropriate exercise program.
Let's briefly discuss the other options:
A- Increase protein in the diet: While a balanced diet that includes an adequate amount of protein is essential for overall health, increasing protein alone may not directly address the issue of chronic fatigue in leukemia clients. While adequate nutrition is important, simply increasing protein intake is not the most effective intervention for managing fatigue in this context.
B- Increase the client's fluids to 4 L per day: Adequate hydration is essential for overall health, but there is no evidence to suggest that increasing fluids alone will directly alleviate chronic fatigue in leukemia clients. The nurse should encourage adequate hydration based on the client's individual needs but should also consider other interventions to address fatigue.
C- Encourage the client to have continual bed rest: Although rest and sleep are important for individuals with leukemia to manage fatigue, promoting continual bed rest can lead to deconditioning and further exacerbate fatigue. Encouraging a balance between rest and physical activity is crucial to managing fatigue effectively.
A nurse is collecting data from a client who has placenta previa. Which of the following findings should the nurse expect?
Explanation
Placenta previa is a condition where the placenta partially or completely covers the cervix, leading to vaginal bleeding. The bleeding is typically painless and bright red in color. This is an important finding that should be assessed and monitored closely.
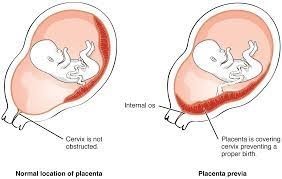
A rigid abdomen is not a characteristic finding of placenta previa. It could be a sign of another condition such as placental abruption or uterine rupture, which are separate complications. Fetal movement is not directly related to placenta previa. It is a normal finding and can vary depending on the gestational age and individual fetal patterns.
Placenta previa is not typically associated with persistent uterine contractions. However, it is important to monitor for any signs of preterm labor or other complications that could cause uterine contractions.
Sign Up or Login to view all the 180 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
