ATI Custom- Wn23 NS122
Total Questions : 75
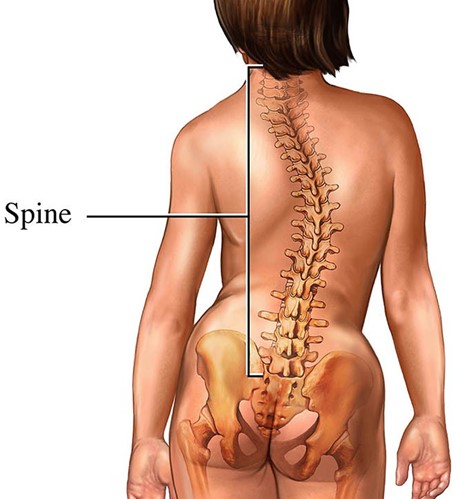
Showing 25 questions, Sign in for moreThe nurse is talking with the caregiver of a 13-year-old diagnosed with scoliosis.
The child has come to the clinic to be fitted with a brace to begin her treatment.
The child appears upset and angry and states, "I hate this brace; I hate it already." In an effort to support this child, which statement would be the most appropriate for the nurse to make to this child's caregiver?
Explanation
Allowing the child to choose an article or two of clothing that she can wear with the brace can help her feel more confident and in control of her appearance.
This can help her feel better about wearing the brace and improve her overall attitude toward the treatment.
Choice B is not the best answer because it focuses on the long-term benefits of the treatment without addressing the child’s immediate concerns and emotions.
Choice C is not the best answer because it suggests that the child should be left alone to deal with her emotions, which may not be helpful in this situation.
Choice D is not the best answer because it suggests comparing the child’s situation to others who are sicker, which may not be helpful or appropriate.
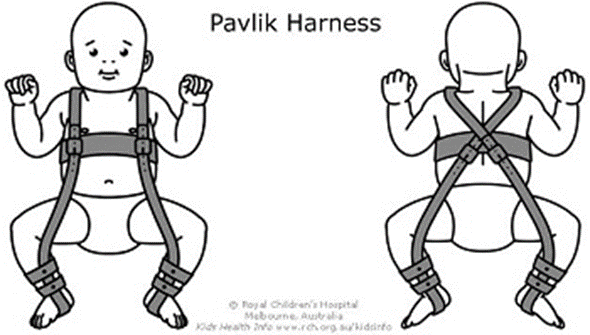
A nurse is reinforcing teaching with the mother of a 2-month-old infant whose provider applied a Pavlik harness 1 week earlier for the treatment of developmental hip dysplasia.
Which of the following statements by the mother indicates an understanding of the teaching?
Explanation
Checking the baby’s skin three times each day can help the mother monitor for any skin irritation or breakdown caused by the harness.
This can help prevent complications and ensure that the harness is being used safely and effectively.
Choice A is not the best answer because the mother should not adjust the harness straps on her own.
This should be done by a healthcare provider to ensure that the harness is properly fitted.
Choice B is not the best answer because the diaper should be placed under the harness, not over it.
Choice C is not the best answer because massaging lotion on the skin around the harness clasps may not be necessary and could potentially cause skin irritation.
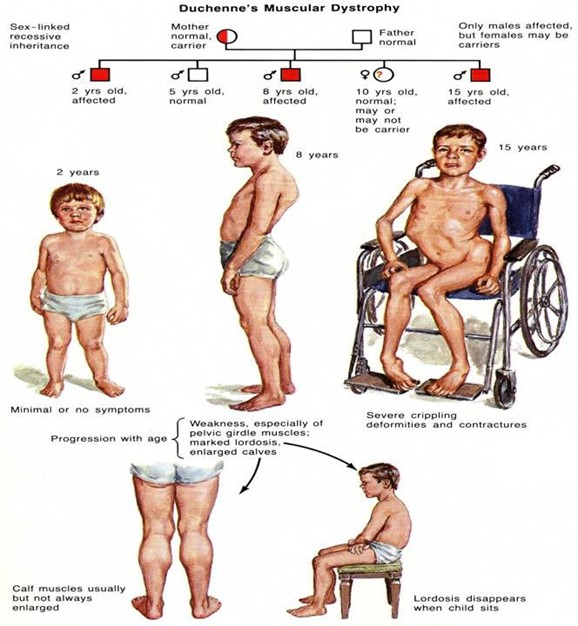
The nurse is teaching family members of a child newly diagnosed with muscular dystrophy about early signs.
The nurse knows that teaching was successful when a parent states that which of the following signs may indicate the condition early?
Explanation
Difficulty climbing stairs is an early sign of muscular dystrophy.
This is because the condition causes progressive muscle weakness, which can make it difficult for the child to perform physical activities that require muscle strength.
Choice A is not the best answer because high fevers and tiredness are not specific to muscular dystrophy and can be caused by many other conditions.
Choice B is not the best answer because muscular dystrophy causes muscle weakness, not increased muscle strength.
Choice C is not the best answer because respiratory infections and obesity are not specific to muscular dystrophy and can be caused by many other conditions.
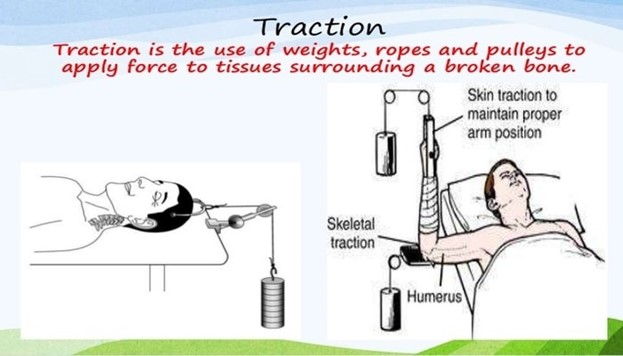
An infant suffered from a fracture of the humerus and requires traction that uses pins, wires, and tongs.
What type of traction is this?
Explanation
Skeletal traction is a type of traction that uses pins, wires, or tongs to apply a pulling force directly to the bone.
This can help align and stabilize a fracture while it heals.
Choice B is not the best answer because muscle traction is not a type of traction.
Choice C is not the best answer because joint traction is not a type of traction.
Choice D is not the best answer because skin traction uses adhesive strips or elastic bandages to apply a pulling force to the skin, rather than directly to the bone.
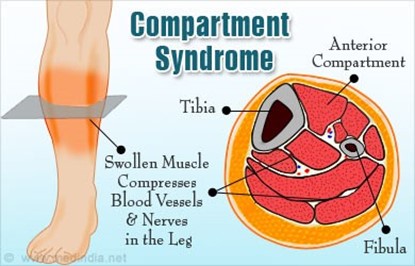
The nurse caring for a child who has been put into a leg cast must be on alert for signs of nerve and muscle damage.
Which symptom might be an early warning signal that the child has developed compartment syndrome?
Explanation
Compartment syndrome is a condition where increased pressure within a muscle compartment causes muscle and nerve damage along with pain.
One of the symptoms of compartment syndrome is severe pain that increases with the stretching of muscles.
Choice A is not correct because blue-looking nail beds on the toes are not a symptom of compartment syndrome.
Choice B is not correct because a weak femoral pulse is not a symptom of compartment syndrome.
Choice C is not correct because the inability to plantarflex the foot is not a symptom of compartment syndrome.
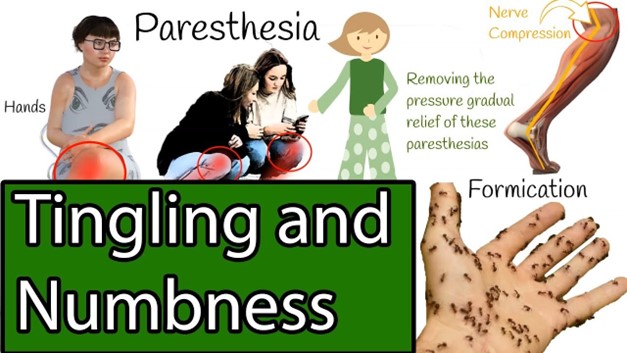
The nurse is doing neurovascular checks on a child who has had a cast applied to treat a fracture.
The nurse observes for diminished or absent sensation and numbness or tingling. In doing this, the nurse is monitoring which symptom?
Explanation
Paresthesia refers to an abnormal sensation of the skin, such as numbness, tingling, or burning.
When the nurse observes for diminished or absent sensation and numbness or tingling, they are monitoring for paresthesia.
Choice A is not correct because pain is not the symptom being monitored in this case.
Choice B is not correct because paralysis is not the symptom being monitored in this case.
Choice D is not correct because pallor refers to the paleness of the skin and is not the symptom being monitored in this case.
The nurse is monitoring a client who is 3 hours postpartum. On assessment, the nurse notes a temperature of 102.4°F.
Which action should the nurse prioritize?
Explanation
A postpartum fever is defined as a temperature greater than 100.4 degrees F (38.0 degrees C) on at least two occasions.
These fevers cannot be ignored as they can represent serious infections. The first task is to identify the source.
Choice A is not correct because continuing to monitor for another hour may delay necessary treatment.
Choice B is not correct because administering an antipyretic may only treat the symptom and not address the underlying cause of the fever.
Choice C is not correct because assisting the client in ambulation does not address the underlying cause of the fever.
A nurse is assisting in the care of a client who is in the second stage of labor.
Which of the following findings should the nurse report to the provider?
Explanation
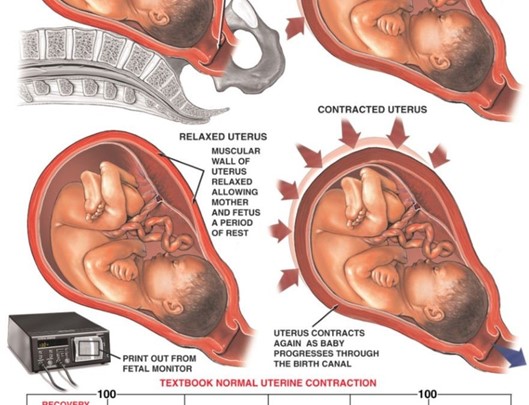
This is a sign of uterine hyperstimulation, which can cause fetal distress and excessive bleeding12.
The nurse should report this finding to the provider and monitor the fetal heart rate and maternal vital signs.
Choice B.
Early decelerations in the FHR are incorrect, as this is a normal finding during the second stage of labor, indicating head compression.
Choice C.
Pelvic pressure with contractions is incorrect, as this is an expected finding during the second stage of labor, indicating that the baby is descending through the birth canal.
Choice D.
Bloody show from the vagina is incorrect, as this is also an expected finding during the second stage of labor, indicating cervical dilation and effacement13.
Therefore, choice A is the best answer.
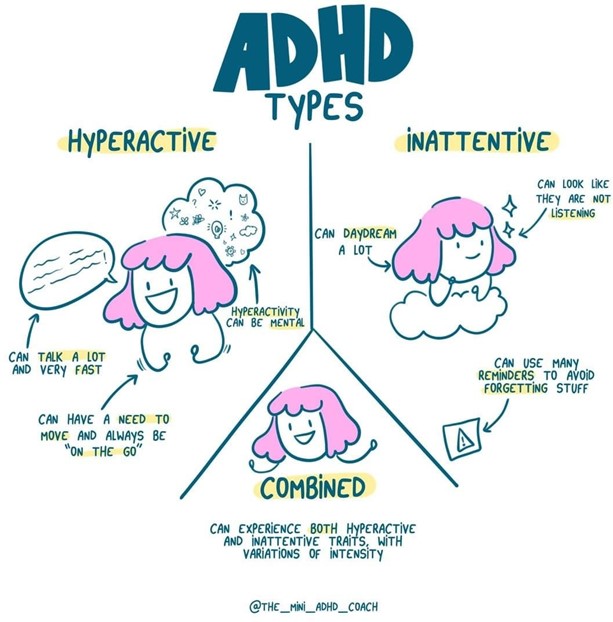
A nurse is collecting data on an adolescent client who has attention deficit hyperactivity disorder (ADHD).
Which of the following manifestations should the nurse expect to find?
Explanation
ADHD primarily causes symptoms related to inattention, hyperactivity-impulsivity, or a combination of both.
With ADHD, someone may experience difficulties paying attention and staying organized.
Choice A is not correct because difficulty in acquiring reading skills is not a specific symptom of ADHD.
Choice B is not correct because difficulty using words in context is not a specific symptom of ADHD.
Choice D is not correct because difficulty performing self-grooming activities is not a specific symptom of ADHD.
A pregnant woman is experiencing nausea in the early morning.
What recommendations would the nurse offer to alleviate this symptom?
Explanation
A nurse would recommend having crackers handy at the bedside and eating a few before getting out of bed to alleviate nausea in the early morning for a pregnant woman 1.
Eating foods that don’t aggravate your stomach, such as crackers, can help limit morning sickness.
Choice A is not an answer because eating three well-balanced meals per day and limiting snacks may not help alleviate nausea.
Eating small meals can help limit morning sickness.
Choice C is not an answer because drinking a full glass of fluid at the beginning of each meal may not help alleviate nausea.
Drinking throughout the day, not just when you are thirsty, can help limit morning sickness.
Choice D is not an answer because eating a bland diet and avoiding concentrated sweets may not help alleviate nausea.
Eating foods that don’t aggravate your stomach can help limit morning sickness.
A nurse is collecting data from a 6-month-old infant in the well-child clinic.
Which of the following findings should the nurse expect?
Explanation
A nurse collecting data from a 6-month-old infant in the well-child clinic should expect that the infant sits well without support.
Choice A is not an answer because lateral incisors may not be present in a 6- month-old infant.
Choice B is not an answer because the posterior fontanel may not be closed in a 6-month-old infant.
Choice C is not an answer because a 6-month-old infant’s birth weight may not be tripled.
A nurse is caring for a toddler who had a cast applied 2 hours ago due to multiple fractures of the right hand.
Which of the following findings should the nurse report immediately to the charge nurse?
Explanation
A nurse caring for a toddler who had a cast applied 2 hours ago due to multiple fractures of the right hand should report immediately to the charge nurse if the fingers on the right hand have a capillary refill of 4 seconds.
This could indicate that there is a problem with circulation.
Choice A is not an answer because it is not unusual for a child to not attempt to move her right arm or fingers after having a cast applied.
Choice B is not an answer because it is not unusual for the fingertips of the right hand to be swollen and bruised after having a cast applied.
Choice D is not an answer because it is not unusual for a child to not keep their arm elevated on a pillow after having a cast applied.
A nurse is caring for a toddler who had a cast applied 2 hours ago due to multiple fractures of the right hand.
Which of the following findings should the nurse report immediately to the charge nurse?
Explanation
A nurse caring for a toddler who had a cast applied 2 hours ago due to multiple fractures of the right hand should report immediately to the charge nurse if the fingers on the right hand have a capillary refill of 4 seconds.
This could indicate that there is a problem with circulation.
Choice A is not an answer because it is not unusual for a child to not attempt to move her right arm or fingers after having a cast applied.
Choice B is not an answer because it is not unusual for the fingertips of the right hand to be swollen and bruised after having a cast applied.
Choice D is not an answer because it is not unusual for a child to not keep their arm elevated on a pillow after having a cast applied.
The nurse is caring for a 4-week-old baby. Mom reports the baby is breech.
What screening test would help rule out a hip problem related to babies who are breech?
Explanation
The Ortolani test is a screening test that would help rule out a hip problem related to babies who are breech.
It is used to check for developmental dysplasia of the hip (DDH).
Choice A is not an answer because bracing is a treatment for DDH, not a screening test.
Choice B is not an answer because genu valgum is a condition where the knees angle in and touch each other when the legs are straightened, and it is not a screening test for DDH.
Choice C is not an answer because the Adams test is used to screen for scoliosis, not DDH.
A nurse is reinforcing teaching with a new mother about the purpose of administering vitamin K to her newborn following delivery.
The nurse should explain that the purpose of administering vitamin K is to prevent which of the following complications?
Explanation
The purpose of administering vitamin K to a newborn following delivery is to prevent bleeding.
Vitamin K helps blood to clot and is essential in preventing serious bleeding in infants.
Choice A is not an answer because administering vitamin K does not prevent infection.
Choice B is not an answer because administering vitamin K does not prevent potassium deficiency.
Choice D is not an answer because administering vitamin K does not prevent hyperbilirubinemia.
Mary is a one-month-old infant.
When reviewing Mary's chart, the nurse confirms that at birth, Mary received what vaccine?
Explanation
B. This is the vaccine for hepatitis B, a viral infection that can cause liver damage and cancer.
The CDC recommends that all newborns receive the first dose of this vaccine within 24 hours of birth, followed by two more doses at 1 to 2 months and 6 to 18 months of age.
Choice A.
MMR is incorrect, as this is the vaccine for measles, mumps, and rubella, which is not given at birth but at 12 to 15 months and 4 to 6 years of age.
Choice B.
Varicella is incorrect, as this is the vaccine for chickenpox, which is also not given at birth but at 12 to 15 months and 4 to 6 years of age.
Choice C.
DTaP is incorrect, as this is the vaccine for diphtheria, tetanus, and pertussis (whooping cough), which is not given at birth but at 2, 4, 6, and 15 to 18 months and 4 to 6 years of age.
Therefore, choice D is the best answer to this question.
A client in her third trimester reports sleeping poorly: sleeping on her back results in lightheadedness and dizziness and lying on her side results in no sleep.
Which suggestion for sleeping should the nurse prioritize for this client?
Explanation
This is a variation of the side-lying position, which is recommended for pregnant women in the third trimester to improve blood flow to the uterus and the baby12.

Sleeping on the right side with a pillow under the hip can also help relieve pressure on the inferior vena cava, a large vein that carries blood from the lower body to the heart.
Sleeping on the back can cause lightheadedness and dizziness because of this pressure, as well as increase the risk of stillbirth1.
Choice B.
Without a pillow is incorrect, as this can make sleeping on the side uncomfortable and cause back pain or leg cramps.
Choice C.
with a pillow under her shoulders is incorrect, as this can elevate the upper body and worsen heartburn, a common problem in pregnancy.
Choice D.
with a pillow under both hips is incorrect, as this can make sleeping on the back more likely, which is not advised for pregnant women in the third trimester1.
Therefore, choice A is the best answer.
A client arrives at the clinic very excitedly and reports a positive home pregnancy test.
The nurse cautions that the home pregnancy test is considered a presumptive sign and will assess the client for which sign to confirm pregnancy.
Explanation
The proof of pregnancy is in the pregnancy test.
A positive office pregnancy test would confirm the pregnancy.

Choice A, Chadwick’s sign, is not correct because it is not a definitive sign of pregnancy.
Choice B, Hegar’s sign, is also not correct because it is not a definitive sign of pregnancy.
Choice D, Fetal movement felt by the examiner, is not correct because it is not a definitive sign of pregnancy.
The nurse is teaching parents about adolescent health issues and the topic of anorexia is discussed.
Which of the following is true?
Explanation
Anorexia nervosa is an eating disorder characterized by abnormally low body weight, an intense fear of gaining weight, and a distorted perception of weight.
People with anorexia place a high value on controlling their weight and shape, using extreme efforts that tend to significantly interfere with their lives.
Choice B, Lack of motivation, don’t like to do things perfectly, is not correct because it is not a characteristic of anorexia.
Choice C, Would rather watch TV all day than exercise, is not correct because it is not a characteristic of anorexia.
Choice D Only affects females is not correct because anorexia can affect both males and females.
A pregnant vegan reports eating lots of dark green leafy vegetables, legumes, citrus fruits, and berries.
To ensure that her infant's nervous system will develop properly, what foods should the nurse recommend that she add to her diet?
Explanation
Pregnant vegans should ensure they are getting enough vitamin B12, which is essential for the development of the infant’s nervous system.
Vitamin B12 is found almost exclusively in animal products, so vegans should consume fortified foods such as cereals or take a supplement to ensure they are getting enough of this important nutrient.
Choice B, Milk, and cheese, is not correct because it is not vegan.
Choice C, Nuts, seeds, and chocolate, is not correct because it does not address the need for vitamin B12.
Choice D, Carrots, sweet potatoes, and mangoes, is not correct because it does not address the need for vitamin B12.
The nursing instructor is illustrating the circulatory flow between the mother and fetus.
The instructor determines the session is successful when the class correctly chooses which structure with which route.
Explanation
The umbilical vein carries oxygen-rich blood to the fetus from the placenta.
The umbilical vein is an important part of fetal circulation and carries oxygenated blood from the placenta into the growing fetus.
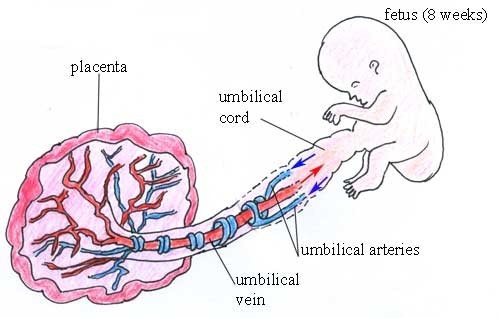
Choice B is incorrect because the two umbilical arteries carry deoxygenated blood from the fetus to the placenta23.
Choice C is incorrect because there are not two umbilical veins, but only one12.
Choice D is incorrect because it is not the one umbilical artery that carries oxygen-rich blood to the fetus from the placenta, but rather the one umbilical vein14.
A nurse is caring for a client who is 4 hr postpartum.
The nurse finds a small amount of lochia rubra on the client's perineal pad.
The fundus is midline and firm at the umbilicus.
Which of the following actions should the nurse take?
Explanation
The nurse should check for blood under the client’s buttocks.
A small amount of lochia rubra on the client’s perineal pad 4 hours postpartum is normal.
The fundus being midline and firm at the umbilicus is also a normal finding.
Choice A is incorrect because assisting the client to ambulate is not necessary at this time.
Choice B is incorrect because there is no need to increase the rate of IV fluids.
Choice D is incorrect because performing a fundal massage is not necessary since the fundus is already firm and midline.
A nurse is reinforcing nutritional teaching with a client who is at 8 weeks of gestation.
Which of the following statements should the nurse include?
Explanation
The nurse should include in their teaching that the client should increase their folic acid intake during pregnancy.
Choice A is incorrect because a pregnant woman at 8 weeks of gestation does not need to increase her daily calorie intake by 750 calories.
Choice C is incorrect because a pregnant woman should not limit her iron intake during her first trimester.
Choice D is incorrect because a pregnant woman should not stop taking her prenatal vitamin if she experiences nausea.
A nurse is assisting with the care of a newly-admitted client who has acute osteomyelitis.
Which of the following interventions is the priority for the nurse to implement?
Explanation
The priority intervention for a newly-admitted client who has acute osteomyelitis is antibiotic therapy.

Choice A is incorrect because antipyretic therapy is not the priority intervention.
Choice C is incorrect because optimal nutrition and hydration are not the priority intervention.
Choice D is incorrect because surgical debridement of necrotic tissue is not the priority intervention.
A nurse is reinforcing teaching with the parents of an 8-month-old infant who will be admitted for surgery. Which of the following instructions should the nurse include in the teaching?
Explanation
The nurse should instruct the parents to bring the infant’s favorite blanket to the hospital.
This can provide comfort and a sense of familiarity for the infant during their hospital stay.
Choice A is incorrect because reading a story about hospitalization to an 8- month-old infant may not be developmentally appropriate.
Choice C is incorrect because parents are usually allowed to stay with their infant during hospitalization.
Choice D is incorrect because manipulating the infant’s bedtime based on the hospital’s visiting hours is not necessary.
Sign Up or Login to view all the 75 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
