Ati fundamentals assessment exam midterm
Total Questions : 53
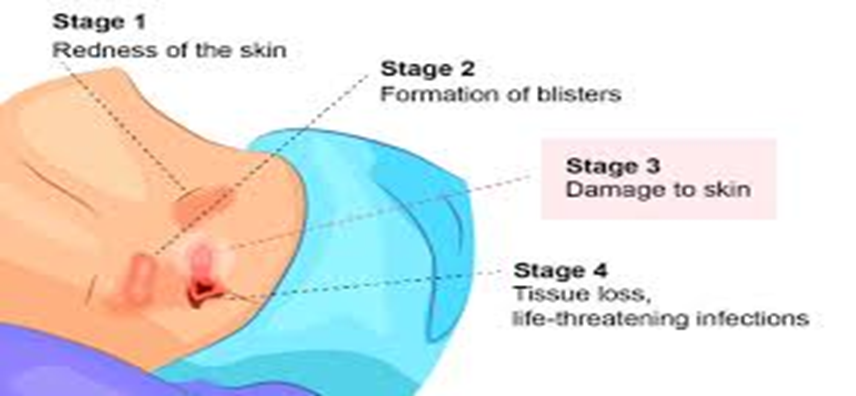
Showing 25 questions, Sign in for moreWhen evaluating an area of broken skin on an older adult client in a long-term care facility, the nurse observes a skin break with redness and a small amount of serosanguineous drainage over the sacrum, with a blister-like appearance. What stage of pressure ulcer would the nurse interpret this finding to indicate?
Explanation
Choice a reason - Stage IV:
Stage IV pressure ulcers are the most severe, with full-thickness skin loss and exposed bone, tendon, or muscle. Signs of stage IV include large-scale tissue loss, possibly including slough or eschar, and may include undermining and tunneling. The scenario described does not indicate such an advanced stage, as there is no mention of exposed deeper tissues or structures.
Choice b reason - Stage III:
Stage III pressure ulcers involve full-thickness skin loss, potentially affecting subcutaneous tissue but not extending to underlying muscle or bone. The wound may have a crater-like appearance. The described condition does not match stage III, as there is no indication of the ulcer extending into subcutaneous tissue.
Choice c reason - Stage I:
Stage I pressure ulcers present with intact skin and non-blanchable redness of a localized area usually over a bony prominence. The skin may be painful, firm, soft, warmer, or cooler compared to adjacent tissue. In the given scenario, the skin is not intact, ruling out stage I.
Choice d reason - Stage II:
Stage II pressure ulcers are characterized by partial-thickness loss of dermis presenting as a shallow open ulcer with a red-pink wound bed, without slough. They may also present as intact or ruptured blisters. The description of the skin condition with erythema, serosanguineous drainage, and a blister-like appearance aligns with a stage II pressure ulcer.
The nurse understands that the purpose of assessing vital signs is to:
Explanation
Choice A Reason:
Assessing vital signs is crucial for evaluating the client's responses to treatment. Changes in vital signs can indicate whether the body is responding positively or negatively to a treatment, allowing healthcare providers to adjust care plans accordingly. For example, a decrease in fever after administering antipyretics would suggest the treatment is effective.
Choice B Reason:
While carrying out orders from the healthcare provider is a responsibility of the nurse, it is not the primary reason for assessing vital signs. Vital signs are assessed to inform clinical decisions, not solely to fulfill orders. Therefore, this choice is not correct in the context of the importance of vital sign assessment.
Choice C Reason:
Monitoring risks for alterations in health is another key reason for assessing vital signs. Vital signs can serve as early indicators of health issues, such as the onset of an infection indicated by a rising temperature or cardiovascular problems suggested by changes in blood pressure or heart rate.
Choice D Reason:
Establishing a baseline is essential when assessing vital signs. It provides a reference point for future comparisons, which is important for detecting any deviations from the client's normal range. This helps in identifying potential health issues early and monitoring the progression of known conditions.
A 45-year-old African-American client visits the clinic with complaints of fatigue, thirst, and frequent urination. During the physical exam, the nurse observes linear hyperpigmentation around the neck and in the axillae (Acanthosis Nigricans). What should the nurse do next?
Explanation
Choice a reason
Referring the client for medical follow-up is the most appropriate action. Acanthosis Nigricans is often associated with insulin resistance and is a risk factor for diabetes mellitus. The client's symptoms of fatigue, thirst, and frequent urination are classic signs of diabetes. Therefore, a comprehensive medical evaluation is necessary to rule out diabetes or other underlying conditions that could be causing these symptoms.
Choice b reason
While Acanthosis Nigricans can sometimes be associated with malignancy, it is more commonly linked to insulin resistance and diabetes. The client's presenting symptoms are not typical of cancer but are indicative of diabetes. Therefore, while a family history of cancer is relevant to the client's overall health, it is not the immediate concern based on the current presentation.
Choice c reason
Documenting findings is an essential part of the nursing process; however, the presence of Acanthosis Nigricans, especially when coupled with symptoms of fatigue, thirst, and frequent urination, should not be considered benign without further investigation. These findings warrant further assessment to determine the underlying cause.
Choice d reason
Performing a random blood sugar test could be a part of the initial assessment; however, it should not replace a referral for a comprehensive medical evaluation. A random blood sugar test alone may not be sufficient to diagnose diabetes or determine the cause of the client's symptoms. A full medical follow-up will likely include blood sugar testing along with other diagnostic tests.
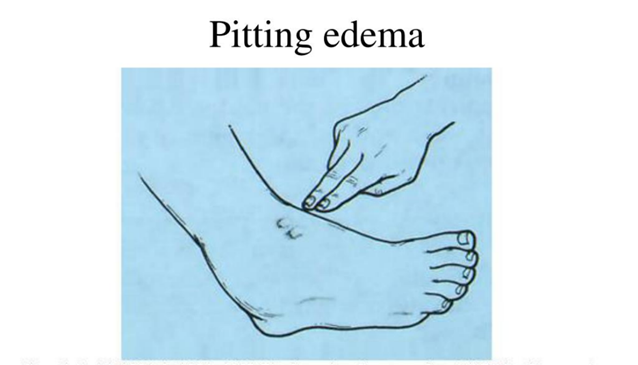
In which disease process should a nurse anticipate observing a patient with pitting edema?
Explanation
Choice A reason:
Diabetes mellitus is not typically associated with pitting edema unless it has led to a comorbid condition such as heart failure or kidney disease. Pitting edema is more commonly associated with fluid retention due to the body's inability to manage fluid balance, which is not a direct consequence of diabetes mellitus itself.
Choice B reason:
Liver disease, particularly cirrhosis, can lead to pitting edema. The liver's inability to produce albumin, a protein that helps maintain oncotic pressure in the blood vessels, and portal hypertension, which is an increase in the blood pressure within the portal vein system, can both contribute to the development of pitting edema.
Choice C reason:
End-stage renal disease can also cause pitting edema due to the kidneys' inability to excrete excess fluid. However, the edema associated with renal disease is often more generalized and not limited to the lower extremities.
Choice D reason:
Colon cancer is not typically associated with pitting edema unless it has metastasized and caused secondary complications that affect the liver or the heart. Pitting edema is not a direct symptom of colon cancer itself.
The nurse evaluates a client's submental lymph nodes. In which part of the client's head should the nurse palpate these lymph nodes?
Explanation
Choice A reason:
Palpating in front of the ear would assess the preauricular lymph nodes, not the submental lymph nodes. The preauricular nodes are located just in front of the ears and are typically examined when there is an infection or inflammation in the eyes, ears, or scalp.
Choice B reason:
The submental lymph nodes are located in the midline, just under the chin, behind the bony prominence of the mandible. This is the correct area for palpation when assessing the submental lymph nodes. These nodes drain the lower lip, the floor of the mouth, the tip of the tongue, and the incisors, and they can become enlarged due to infections or malignancies in these areas.
Choice C reason:
Palpating superficial to the sternomastoid would assess the cervical lymph nodes, specifically the anterior cervical nodes, which are not the submental lymph nodes. The sternomastoid muscle is a landmark for several lymph node groups in the neck, but not for the submental group.
Choice D reason:
Palpating at the angle of the mandible would assess the submandibular lymph nodes, not the submental lymph nodes. The submandibular nodes are located beneath the jawline and can become enlarged due to infections or malignancies in the mouth, throat, and salivary glands.

What eye function is the nurse getting ready to evaluate when the client is asked to stand 20 feet away from a chart mounted on the examination room wall?
Explanation
Choice A reason:
Peripheral vision is the ability to see objects and movement outside of the direct line of vision. This type of vision is assessed using different methods, such as confrontation visual field testing, where the examiner moves objects into the patient's side vision from different angles. Standing 20 feet away from a chart would not be the appropriate method to assess peripheral vision.
Choice B reason:
The assessment of external eye structures involves examining the physical appearance and condition of the eyelids, sclera, conjunctiva, and surrounding areas. This is typically done at a close range and does not require the patient to stand at a distance from a chart. The nurse would inspect these structures directly, often with the aid of a penlight for better visibility.
Choice C reason:
Distant vision is the ability to see objects far away, and it is what the nurse is preparing to assess when the client is asked to stand 20 feet from a chart. This distance is standard for the Snellen eye chart, which is used to measure visual acuity. The chart has rows of letters that decrease in size, and the patient is asked to read the smallest line of letters they can see clearly. The Snellen chart is the most common method used by eye doctors to measure visual acuity.
Choice D reason:
Near vision is the ability to see objects that are close to the eyes clearly. It is assessed using different charts, such as the Jaeger eye chart, which contains blocks of text in various type sizes. The patient is asked to read the text at a close range, typically around 14 inches, not 20 feet. Therefore, standing 20 feet away from a chart would not be the method to assess near vision.
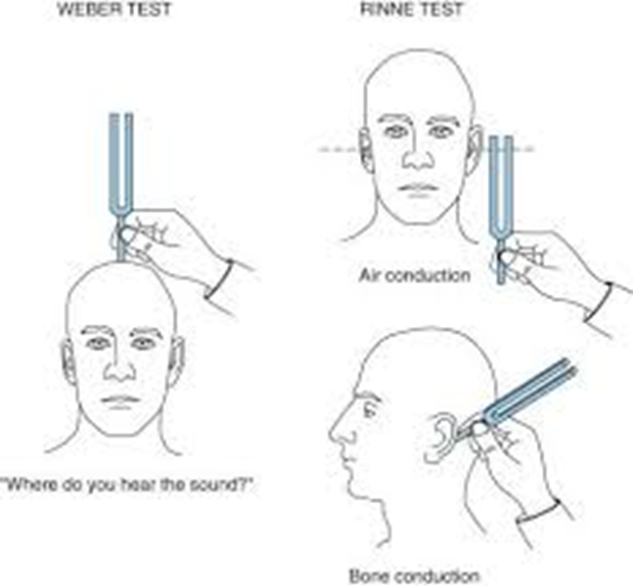
A client has been undergoing intravenous antibiotic treatment (ototoxic) for several weeks. What prevention strategy would be most appropriate for the nurse to suggest for this client?
Explanation
Choice A reason:
A formal hearing test, or audiometry, is the most comprehensive method for assessing hearing loss, which can be a side effect of ototoxic medications. These tests can detect both conductive and sensorineural hearing loss, providing a detailed profile of hearing function across different frequencies. For clients receiving ototoxic antibiotics, regular monitoring through formal hearing tests is recommended to detect any early signs of hearing impairment and to implement timely interventions.
Choice B reason:
The rubbing fingers test is a rudimentary hearing screening method where the examiner rubs their fingers together near the patient's ear, asking them to indicate when they hear the sound. While this test can be used as a quick check for hearing loss, it is not as sensitive or specific as formal audiometry and may not detect early or mild hearing loss caused by ototoxic drugs.
Choice C reason:
Tuning fork tests, such as the Weber and Rinne tests, are used to differentiate between conductive and sensorineural hearing loss. These tests can be useful in a clinical setting to provide immediate information about the type of hearing loss; however, they are not as comprehensive as formal hearing tests and may not be sufficient for monitoring cytotoxicity.
Choice D reason:
The whisper hearing test involves the examiner whispering words or numbers and asking the patient to repeat them. This test can be useful for detecting significant hearing loss but may not be sensitive enough to detect the early stages of ototoxicity. Moreover, the test's accuracy can be affected by the examiner's voice level and the testing environment.
The clinical nurse is mentoring a group of students, and one student asks, "What is the main purpose of a health assessment?" What would be the most suitable response from the clinical nurse?
Explanation
Choice A reason:
The primary purpose of health assessment is to collect, analyze, and interpret data to identify the patient’s health status and needs, as well as to develop and implement appropriate nursing interventions to address these needs. It is a systematic process that is fundamental in promoting the health and well-being of patients. This involves a comprehensive evaluation of the patient's physical, psychological, and social health. Gathering this information is crucial for creating a care plan that addresses the individual needs of the client.
Choice B reason:
While health assessments can aid physicians in diagnosing illness, they are not solely for the purpose of diagnosis without further testing. Health assessments may indicate the need for additional tests to confirm a diagnosis. The nurse's role includes supporting the diagnostic process, but it is not the primary purpose of health assessment.
Choice C reason:
Health assessments are not meant to be subjective or based on the nurse's personal views and beliefs. The assessments are conducted to objectively determine the health status of a client, which then informs evidence-based practice and care planning. Personal biases should not influence the management of a client's illness.
Choice D reason:
Making judgments about a client's lifestyle and behaviors is not the primary purpose of health assessment. While lifestyle and behaviors may be assessed as part of understanding the client's overall health status, the goal is not to judge but to understand how these factors may impact the client's health and to provide education and support for healthy changes if needed.
Before finishing the physical examination of a patient after a motor vehicle crash, the ER nurse confirms that the client is awake, alert, and oriented. How does this information relate to the general survey?
Explanation
Choice A reason:
Facial expression is an important aspect of the general survey as it can provide clues about a patient's emotional state and possible pain. However, it is not directly related to the patient's level of consciousness. After a motor vehicle crash, assessing facial expression is crucial to identify any signs of distress, trauma, or neurological impairment.
Choice B reason:
Level of consciousness is a critical component of the general survey, especially in the context of trauma or potential neurological injury. It refers to the patient's awareness and responsiveness to the environment. Assessing the level of consciousness involves determining if the patient is awake, alert, and oriented to time, place, and person, which is essential for establishing a baseline cognitive function and detecting any changes that may indicate deterioration or improvement in their condition.
Choice C reason:
Posture, gait, motor activity, and speech are assessed to evaluate the musculoskeletal and neurological systems. While these are important in the context of a motor vehicle crash, they are not specifically related to the level of consciousness. These assessments help identify any deficits that may result from injuries sustained during the crash, such as fractures, dislocations, or neurological damage affecting movement and coordination.
Choice D reason:
The apparent state of health is a broad assessment that includes the patient's overall appearance and any signs that may indicate acute or chronic illness. In the emergency setting, this may involve observing for signs of trauma, shock, or other life-threatening conditions. While it is an essential part of the general survey, it is not specifically focused on the level of consciousness but rather on the patient's general well-being and any obvious health concerns.
A 75-year-old female patient came to the office for her annual wellness visit. During the nurse's assessment, the patient reports experiencing bilateral knee pain for the past eleven months. Given the duration of the symptoms, how would the nurse classify the patient's pain?
Explanation
Choice A reason:
Acute pain is typically sudden in onset and is usually the result of a specific injury or illness. It is characterized by its sharp quality and tends to last for a short duration, generally not longer than six months. Since the patient's knee pain has persisted for eleven months, it does not fall under the category of acute pain.
Choice B reason:
Intermittent pain is pain that comes and goes at intervals. Although the patient's pain could be intermittent, the classification based on duration would not be described as intermittent. This term refers more to the pattern of the pain rather than its chronicity or cause.
Choice C reason:
Chronic pain is defined as pain that persists for longer than six months, often continuing even after the injury or illness that caused it has healed. The patient's bilateral knee pain has been present for eleven months, which exceeds the six-month threshold, thus categorizing it as chronic pain.
Choice D reason:
Idiopathic pain refers to pain that arises without a clear cause. It is not categorized based on the duration of the pain but rather on the absence of an identifiable underlying reason. Since the patient's pain has a specific duration, it is not appropriate to classify it as idiopathic without further information regarding its cause.
A nurse is evaluating a client with a pressure ulcer. What finding should the nurse identify as indicative of a stage 3 pressure ulcer?
Explanation
Choice A reason:
Reddened intact skin is typically associated with a stage 1 pressure ulcer, where the skin is not yet broken but shows signs of redness. This stage indicates that the skin is under pressure and may be at risk for further breakdown if the pressure is not relieved.
Choice B reason:
A stage 3 pressure ulcer involves full-thickness skin loss that extends into the subcutaneous tissue layer but does not involve underlying muscle or bone. The ulcer presents as a deep crater, and there may be slough or eschar present. It is important to manage these ulcers carefully to prevent further deterioration and complications such as infection.
Choice C reason:
Skin loss involving up to the dermis layer is characteristic of a stage 2 pressure ulcer. In this stage, the epidermis and part of the dermis are lost, creating a shallow open wound or blister. This stage is less severe than stage 3 and requires different management strategies to promote healing and prevent progression.
Choice D reason:
Exposed bone is indicative of a stage 4 pressure ulcer, which is the most severe stage. It involves full-thickness skin loss with extensive destruction, possibly including muscle, tendon, or bone exposure. These ulcers are at high risk for serious infections, including osteomyelitis, and require aggressive medical and surgical intervention to heal.
A nurse is evaluating a client with myxedema. Which of the following findings should the nurse anticipate?
Explanation
Choice A reason:
Tachycardia, or an abnormally rapid heart rate, is not a typical finding in myxedema. Myxedema is associated with hypothyroidism, which usually presents with bradycardia, or a slower than normal heart rate, due to the decreased metabolic demands on the body.
Choice B reason:
Diarrhea is not commonly associated with myxedema. Instead, patients with hypothyroidism and myxedema often experience constipation due to slowed gastrointestinal motility.
Choice C reason:
Facial edema, particularly around the eyes, is a classic sign of myxedema. Myxedema is a severe form of hypothyroidism that can cause mucopolysaccharide deposition in the skin, leading to non-pitting edema. This can be particularly noticeable in the face and periorbital area.
Choice D reason:
Heat intolerance is more commonly associated with hyperthyroidism, not hypothyroidism. Patients with myxedema typically have cold intolerance due to a decrease in basal metabolic rate and reduced heat production.
A drug rehabilitation nurse is taking the health history. When would be the most appropriate time to inquire about the client’s alcohol use?
Explanation
Choice A reason:
Discussing reactions to allergens typically focuses on environmental or food triggers that may cause allergic reactions. While it's important to understand a client's allergies, this topic is not closely related to alcohol use, which has different implications for health and lifestyle choices.
Choice B reason:
Asking about alcohol use naturally follows the discussion about cigarette smoking because both involve substance use and have potential health risks. It allows the nurse to transition smoothly from one lifestyle factor to another, which can impact the client's overall health. This approach also helps in creating a comprehensive picture of the client's habits that may contribute to or affect their current health status.
Choice C reason:
Reviewing current medications is an essential part of the health history, as it can reveal potential interactions with alcohol. However, it might be more appropriate to ask about alcohol use after discussing other lifestyle habits such as smoking, as they are more directly related. Once the client's substance use habits are established, the nurse can then discuss how these might interact with prescribed medications.
Choice D reason:
Asking about previous surgeries is important for understanding a client's medical history, but it is not directly related to the client's current lifestyle habits like alcohol use. Therefore, it would be more natural to ask about alcohol use in the context of other substance use discussions rather than after surgical history.
What should the nurse do before performing a physical examination of a client? (Select all that apply)
Explanation
Choice a reason:
Obtaining and checking the needed equipment is essential before conducting a physical examination. This ensures that all necessary tools are functional and readily available, which facilitates a smooth and efficient assessment process. It also minimizes interruptions that could cause discomfort or anxiety for the client.
Choice b reason:
While turning on relaxing music of the client's choice may create a calming environment, it is not a standard procedure before a physical examination. Music preferences are subjective, and what is relaxing for one person may be distracting for another. Additionally, music could interfere with the ability to hear heart, lung, or bowel sounds during auscultation.
Choice c reason:
Identifying ways to ensure client privacy is a fundamental nursing responsibility. It respects the client's dignity and promotes a sense of safety and comfort. Privacy can be ensured by closing curtains, securing the area, and making sure the examination is conducted in a private setting.
Choice d reason:
Washing hands is a critical step before any physical examination. It is a primary measure for infection control, protecting both the nurse and the client from potential transmission of microorganisms.
Choice e reason:
Dimming the lighting to promote comfort is not typically recommended before a physical examination. Adequate lighting is crucial for the inspection phase of the examination, allowing the nurse to observe the client's general appearance, skin color, and other physical characteristics accurately.
The nurse is preparing to teach a group of adolescents about preventing traumatic brain injuries. What should be included in these instructions?
Explanation
Choice a reason:
Wearing nonslip shoes in the house can prevent falls, which are a common cause of traumatic brain injuries (TBIs) in adolescents. Falls often occur due to slippery surfaces, and nonslip shoes provide better traction, reducing the risk of such accidents.
Choice b reason:
Supervised use of guns by an adult is crucial to prevent accidental shootings, which can result in TBIs or even more severe outcomes. Adolescents may not fully understand the risks associated with handling firearms, and adult supervision ensures that safety measures are followed.
Choice c reason:
The consistent use of seat belts in vehicles is one of the most effective ways to prevent TBIs during car accidents. Seat belts keep occupants from being ejected or hitting the interior of the car, significantly reducing the risk of head injuries.
Choice d reason:
Avoiding risky activities such as snowboarding without proper safety measures can prevent sports-related TBIs. While snowboarding, wearing a helmet and other protective gear is essential to protect the head during falls or collisions.
A nurse is conducting a respiratory physical examination on a healthy patient. When using the percussion technique, what should the lung percussion note be?
Explanation
Choice a reason:
Resonance is the expected percussion note when percussing over normal, healthy lung tissue. This sound is produced due to the presence of air in the lung parenchyma, which allows for the transmission of sound waves through the air-filled spaces. In a healthy individual, the resonance indicates that the lungs are free from any significant abnormalities that could alter the sound, such as fluid or solid masses.
Choice b reason:
Tympanic notes are typically heard over hollow, air-containing structures like the stomach. This sound is not expected in lung percussion unless there is a large, air-filled cavity within the lung tissue, which would be abnormal and indicative of a pathological condition such as a pneumothorax.
Choice c reason:
A flat percussion note is usually heard over dense tissues where air is not present, such as over the thigh muscles or areas of the chest where lung tissue has been replaced by something more solid, like in the case of a pleural effusion or a lung mass.
Choice d reason:
Dullness on percussion usually indicates that the lung is not air-filled and may be suggestive of underlying conditions such as pneumonia, tumor, or atelectasis. It is a higher-pitched sound compared to flatness and is typically found in areas of the lung that are filled with fluid or solid tissue rather than air.
A patient has been diagnosed with left ear unilateral sensorineural hearing loss. During the Weber test, where does the nurse expect the sound or vibration to lateralize?
Explanation
Choice a reason:
The left temporal bone would be the expected site of lateralization for sound in a Weber test if the patient had conductive hearing loss in the left ear. However, with unilateral sensorineural hearing loss, the sound typically lateralizes to the opposite ear, which is the ear with better hearing.
Choice b reason:
Lateralization to both ears equally during the Weber test would suggest either normal hearing or symmetrical hearing loss. In the case of unilateral sensorineural hearing loss, the sound is not perceived as equal in both ears because the affected ear does not hear as well as the unaffected ear.
Choice c reason:
In a patient with unilateral sensorineural hearing loss in the left ear, the Weber test will lateralize to the right ear, which is the ear with normal hearing. This occurs because the inner ear on the affected side is not able to transmit the sound as effectively as the unaffected side, making the sound seem louder in the ear with better hearing.
Choice d reason:
Lateralization to the left ear in the Weber test would indicate conductive hearing loss in the left ear, not sensorineural hearing loss. In sensorineural hearing loss, the sound vibrates to the ear with better cochlear function, which would be the right ear in this case.
A nurse is organizing an educational session on the importance of oral hygiene. What teaching tip should be included in the part about preventing gingivitis?
Explanation
Choice a reason:
A firm toothbrush is not recommended for plaque removal as it can damage the gums and tooth enamel. Soft-bristled toothbrushes are preferred because they are effective at removing plaque while being gentle on the gums and enamel.
Choice b reason:
Brushing more than twice per day does not necessarily irritate the gums unless done with improper technique or with a hard-bristled toothbrush. It is important to brush gently with a soft-bristled toothbrush and to use fluoride toothpaste to maintain oral hygiene and prevent gingivitis.
Choice c reason:
Ensuring that dental restorations such as fillings and crowns fit well is crucial in preventing gingivitis. Poorly fitted restorations can trap food particles and bacteria, leading to plaque buildup and gum inflammation. Regular dental check-ups can help ensure that restorations remain intact and do not contribute to gingivitis.
Choice d reason:
Flossing should not be avoided even if there is bleeding at the gumline. Bleeding can be a sign of gingivitis, and flossing can help remove the plaque and bacteria causing the inflammation. If bleeding persists, it is important to consult a dentist.
A client reports experiencing hoarseness for the past 3 weeks, along with fatigue and noticeable weight gain over the last month. What cause should the nurse consider as most likely?
Explanation
Choice a reason:
Hypothyroidism is a condition where the thyroid gland does not produce enough thyroid hormones. This can lead to a variety of symptoms, including hoarseness, fatigue, and weight gain. The hoarseness can be due to the effect of hormone deficiency on the vocal cords, while fatigue and weight gain are common due to the slowed metabolism associated with hypothyroidism.
Choice b reason:
Gingivitis is inflammation of the gums and does not typically cause hoarseness, fatigue, or weight gain. It is more commonly associated with symptoms like red, swollen gums and bleeding during brushing or flossing.
Choice c reason:
Aphthous ulcers, also known as canker sores, are small, shallow lesions that develop on the soft tissues in the mouth or at the base of the gums. While they can be painful and cause difficulty with eating and speaking, they do not cause systemic symptoms such as hoarseness, fatigue, or weight gain.
Choice d reason:
Dysphagia, or difficulty swallowing, can lead to hoarseness if there is an associated throat disorder. However, it is not typically associated with systemic symptoms like fatigue and weight gain unless it is part of a broader condition that affects the body's metabolism or energy levels.
The nurse in an outpatient GI clinic is performing a physical examination of the abdomen. What is the best action for the nurse to take to ensure she can hear bowel sounds?
Explanation
Choice a reason:
Assisting the client to a sitting position is not the best action to ensure that bowel sounds can be heard. For abdominal auscultation, the patient should be lying down in a supine position to relax the abdominal muscles, which facilitates the hearing of bowel sounds.
Choice b reason:
Percussion of the abdomen before auscultation is not recommended as the best initial action. Percussion can stimulate bowel motility, which may alter the natural bowel sounds that the nurse is attempting to assess.
Choice c reason:
Reducing all environmental noise is the best action to ensure that bowel sounds can be heard clearly. Environmental noise can mask the subtle sounds of bowel motility, and minimizing distractions allows for a more accurate assessment of bowel activity.
Choice d reason:
Palpating the region before auscultating is not the best action because palpation can also stimulate bowel motility and potentially alter the bowel sounds. Auscultation should be performed before palpation during the abdominal examination to avoid this issue.
A nurse is evaluating a client with asthma. Which area should the nurse assess as the most dependable indicator of central cyanosis?
Explanation
Choice a reason:
The oral mucosa is the most reliable area to evaluate for central cyanosis in a client with asthma. Central cyanosis reflects a decrease in arterial oxygenation and is best assessed where the blood flow is high and the skin is thin, which is the case with the oral mucosa. It is less likely to be affected by peripheral factors such as temperature and is therefore a more accurate indicator of oxygen saturation in the central circulation.
Choice b reason:
While ear lobes can show signs of cyanosis, they are not the most reliable indicator of central cyanosis because they are more prone to peripheral cyanosis. Peripheral cyanosis can occur in the ear lobes due to local vasoconstriction or decreased blood flow, which may not reflect central oxygenation levels.
Choice c reason:
The soles of the feet are not a reliable indicator of central cyanosis, especially in a client with asthma. The skin on the soles is thicker and has less blood flow compared to the oral mucosa, making it a poor site for assessing central cyanosis. Additionally, the soles can be affected by peripheral factors like pressure and temperature.
Choice d reason:
Conjunctivae are not the most reliable indicator of central cyanosis. While they can show signs of cyanosis, the assessment can be affected by environmental factors and the presence of blood vessels in the conjunctiva that may not accurately reflect central oxygenation levels.
The nurse is getting ready to examine the floor of a client's mouth. To move the tongue to one side for this examination, which tool should the nurse use?
Explanation
Choice a reason:
A penlight is used to provide illumination during an examination, not to move the tongue. It helps the nurse to visualize the mouth floor and other areas by casting light, but it does not have the physical structure to manipulate the tongue.
Choice b reason:
Gloves are worn by healthcare professionals to maintain hygiene and protect both the patient and the nurse from the transmission of infectious agents. They are not used to move the tongue to one side during an examination.
Choice c reason:
A gauze pad is the correct tool to use when the nurse needs to move the tongue to one side during an examination of the mouth floor. The nurse can wrap the gauze pad around the tongue for a better grip, which allows for safe and effective retraction of the tongue without causing discomfort to the patient.
Choice d reason:
A tongue blade, also known as a tongue depressor, is typically used to depress the tongue to examine the back of the throat, not to move the tongue to one side. It is used to hold the tongue down so that the nurse can inspect the oropharynx and other structures.
A client with a history of COPD is undergoing an assessment. When the nurse percusses the client's chest, what characteristic sound should be expected?
Explanation
Choice a reason:
Tympany is a drum-like, resonant sound that is typically heard over air-filled structures, such as the gastric bubble, not the chest. It is not a sound associated with the lungs, especially in the context of COPD.
Choice b reason:
Hyperresonance is an abnormally loud, lower-pitched sound than normal resonance heard over hyperinflated areas of the lung, such as in cases of COPD. This is due to the increased air content within the lungs, often because of overdistension or destruction of alveolar tissue, as seen in emphysema, a common type of COPD.
Choice c reason:
Resonance is the normal sound heard over healthy lung tissue when percussed. However, in the case of COPD, particularly emphysema, the destruction of lung tissue leads to hyperinflation and thus a hyperresonant sound rather than the normal resonance.
Choice d reason:
Dullness is heard when fluid or solid tissue replaces air in the lung or occupies the pleural space, as in the case of pneumonia or pleural effusion. This is not characteristic of COPD, where there is an increase in air due to the breakdown of alveolar walls.
A nurse educator is speaking at a continuing education seminar for nurses, focusing on preventing skin breakdown in immobile patients who have had a stroke. What level of prevention is the nurse educator addressing?
Explanation
Choice a reason:
Educational Prevention is not a recognized level of prevention in healthcare. While education is a key component in all levels of prevention, it is not a standalone category. Education is typically included in primary prevention as it involves informing the public about health practices to prevent the onset of disease.
Choice b reason:
Tertiary Prevention is the level of prevention that aims to manage and treat an existing disease to prevent further complications or deterioration. In the case of immobile stroke patients, tertiary prevention would involve measures to prevent skin breakdown and other complications associated with immobility and the stroke's long-term effects.
Choice c reason:
Secondary Prevention involves early detection and prompt intervention to prevent the progression of a disease. For stroke patients, secondary prevention might include monitoring for signs of skin breakdown so that early treatment can be initiated. However, the scenario described focuses on managing an existing condition rather than early detection.
Choice d reason:
Primary Prevention aims to prevent the disease or injury before it occurs. This would involve strategies to prevent strokes in the first place, such as controlling high blood pressure or encouraging healthy lifestyle changes. It does not directly relate to the prevention of skin breakdown in patients who have already had a stroke.
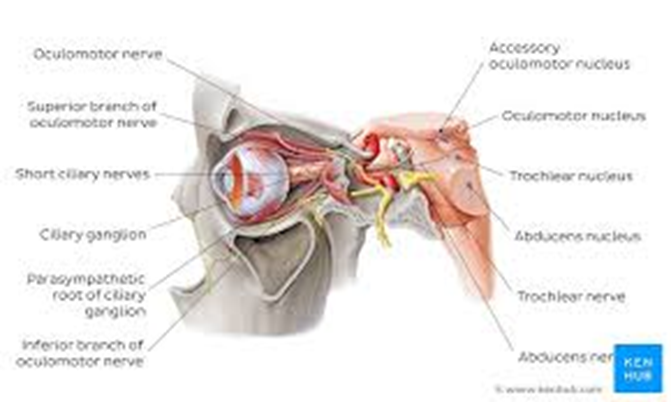
The nurse reviewed the patient’s health history and observed cranial nerve III oculomotor paralysis. What symptoms should the nurse anticipate?
Explanation
Choice a reason:
The inability of the eye to look outward, known as lateral rectus palsy, is associated with cranial nerve VI, the abducens nerve, not the oculomotor nerve. The oculomotor nerve does not control the lateral rectus muscle which governs this movement.
Choice b reason:
Myopia, or nearsightedness, is a refractive error of the eye where distant objects appear blurry while close objects can be seen clearly. It is not related to oculomotor nerve paralysis, which affects eye movements and pupil response, not the shape of the eyeball or the refractive properties of the lens.
Choice c reason:
Ptosis, or drooping of the upper eyelid, and an absence of pupillary constriction are classic signs of oculomotor nerve paralysis. The oculomotor nerve controls most of the eye's movements, including lifting the eyelid via the levator palpebrae superioris muscle and constricting the pupil through the circular muscles of the iris.
Choice d reason:
Normal eye movement would not be expected in a patient with oculomotor nerve paralysis. This nerve controls the majority of the eye's movements, so paralysis would lead to abnormal eye movement, such as the inability to move the eye upward, downward, or inward.
Sign Up or Login to view all the 53 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
