Ati fundemantal final test exam_2
Total Questions : 71
Showing 25 questions, Sign in for moreThe nurse educator provides developmental testing for kindergarten through third-grade students. Which level of prevention is the nurse performing?
Explanation
Developmental testing for kindergarten through third-grade students is an example of primary prevention. Primary prevention aims to prevent disease or injury before it occurs by promoting healthy behaviors and reducing exposure to risk factors.
The 3 Levels of Prevention: Primary, Secondary , and Tertiary. The 3 levels of prevention wo… | Community health nursing, Nursing school studying, Nursing education
A client who has been blinded as a result of an injury has informed the nurse of her plans to return to her counselling practice and work full-time. The nurse should realize that this client is demonstrating which aspect of values clarification?
Explanation
The correct answer is **Prioritizing**. Values clarification is the process of assisting another to clarify their own values in order to facilitate decision making ¹. In this case, the client who has been blinded as a result of an injury has informed the nurse of her plans to return to her counseling practice and work full-time. This demonstrates that the client has prioritized her values and made a decision based on them.
Samuel Merritt University, School of Nursing - ppt download
A nursing diagnosis of "Risk for Deficient Fluid Volume" related to excessive fluid loss, secondary to diarrhea and vomiting was implemented for a home health client who began with these symptoms 5 days ago. A goal was set that the client's symptoms would be eliminated within 48 hours. The client is being seen after a week and has had no diarrhea or vomiting for the past 5 days. What should the nurse do?
Explanation
The nurse should document that the problem has been resolved and the goal has been met.
The nursing diagnosis was "Risk for Deficient Fluid Volume" related to excessive fluid loss, secondary to diarrhea and vomiting. The goal was set that the client's symptoms would be eliminated within 48 hours. The client is being seen after a week and has had no diarrhea or vomiting for the past 5 days, indicating that the problem has been resolved. Therefore, the nurse should document that the problem has been resolved and the goal has been met.
An unlicensed assistive person (UAP) is working on a rehabilitation unit. Which task would be appropriate for this person to delegate?
Explanation
Taking and recording vital signs.
An unlicensed assistive person (UAP) is a healthcare worker who is not licensed to perform nursing tasks but can assist with basic care under the supervision of a licensed nurse. Taking and recording vital signs is a task that can be delegated to a UAP. Making a bed and assisting with bathing are also tasks that can be delegated to a UAP. However, an unlicensed assistive person may not delegate tasks to others as they are not licensed to do so.
The nurse is identifying outcomes for a client with the nursing diagnosis of Stress Urinary Incontinence. Which outcome would be related to sphincter incompetence?
Explanation
The client will perform four to five isometric squeezes for 5 to 10 seconds.
Stress urinary incontinence is the involuntary loss of urine during physical activity such as coughing, sneezing or exercising. It is often caused by weakness of the pelvic floor muscles and/or the urethral sphincter. An appropriate outcome for a client with this condition would be to improve the strength of these muscles. Performing isometric squeezes, also known as Kegel exercises, can help strengthen the pelvic floor muscles and improve sphincter competence. This can help reduce or prevent episodes of incontinence.
A nurse is educating women on the need for calcium to prevent bone loss. What level of prevention does this represent?
Explanation
Primary prevention.
Primary prevention refers to actions taken to prevent the occurrence of a disease or condition. In this case, the nurse is educating women on the need for calcium to prevent bone loss, which is an example of primary prevention. By providing information on how to maintain strong bones and prevent bone loss, the nurse is helping to reduce the risk of conditions such as osteoporosis.
Can Osteoporosis Be Reversed?
Which of the following statements is true regarding types of health care agencies?
Explanation
Public health agencies are funded by government grants to investigate and manage communicable diseases.
Public health agencies are responsible for protecting and improving the health of communities. They are often funded by government grants and work to prevent the spread of communicable diseases through measures such as vaccination programs, disease surveillance, and public education campaigns. Surgery can be performed in a variety of healthcare settings, not just hospitals. Skilled nursing extended care facilities provide care for individuals who require ongoing medical support, not just older adults whose insurance no longer covers hospital stays. Hospitals provide a range of services, including acute inpatient care as well as outpatient and emergency services.
Which of the following nursing pioneers established the Red Cross in the United States in 1882?
Explanation
Clara Barton was a pioneering nurse who is best known for founding the American Red Cross in 1881. She was a hospital nurse during the American Civil War and later worked to provide aid to soldiers and civilians affected by war and natural disasters. In 1881, she established the American Red Cross to provide humanitarian assistance during times of crisis. The organization continues to provide disaster relief and support to this day.
The client is admitted to the nurse's unit with a diagnosis of heart failure. His heart is not pumping effectively, which is resulting in edema and coarse crackles in his lungs. The term for this condition is:
Explanation
Heart failure is a condition in which the heart is unable to pump blood effectively, leading to a buildup of fluid in the body. This can result in edema (swelling) and fluid accumulation in the lungs, causing coarse crackles when breathing. The term for this condition is fluid volume excess, which refers to an excessive amount of fluid in the body. Myocardial infarction is a heart attack, atelectasis is a collapse of lung tissue, and fluid volume deficit refers to a lack of fluid in the body.
During discharge planning, the nurse is responsible for teaching the client how to maintain comfort, promote healing, and restore wellness. However, one of the actions listed below is not correct.
Explanation
Instruct the client to report promptly to the practitioner any decreased redness, swelling, pain, or discharge from the incision or drain sites.
During discharge planning, the nurse is responsible for teaching the client how to maintain comfort, promote healing, and restore wellness. This includes instructing the client to report promptly to the practitioner any **increased** redness, swelling, pain, or discharge from the incision or drain sites. These symptoms may indicate an infection or other complication that requires medical attention. The other actions listed are correct and important for promoting healing and wellness after discharge.
A discharge goal for a client is to have improved mobility. Which outcome statement did the nurse write appropriately?
Explanation
An appropriate outcome statement for a client with a discharge goal of improved mobility should be specific, measurable, achievable, relevant, and time-bound. In this case, the outcome statement "Client will ambulate without a walker by 6 weeks" meets these criteria. It specifies the desired outcome (ambulating without a walker), provides a measurable goal (6 weeks), is achievable and relevant to the client's goal of improved mobility, and includes a time frame for achieving the goal. The other statements are not specific or measurable enough to be considered appropriate outcome statements.
A client recovering from surgery asks the nurse why turning, deep breathing, and coughing exercises need to be done. What should the nurse respond?
Explanation
Turning, deep breathing, and coughing exercises are important for clients recovering from surgery as they help prevent the development of pneumonia. After surgery, clients may have difficulty taking deep breaths and coughing due to pain or discomfort. This can lead to the accumulation of mucus in the lungs, increasing the risk of pneumonia. By performing these exercises, clients can help clear their lungs and reduce their risk of developing this complication. While these exercises may also help prevent other complications such as thrombophlebitis, the primary reason for performing them is to prevent pneumonia.
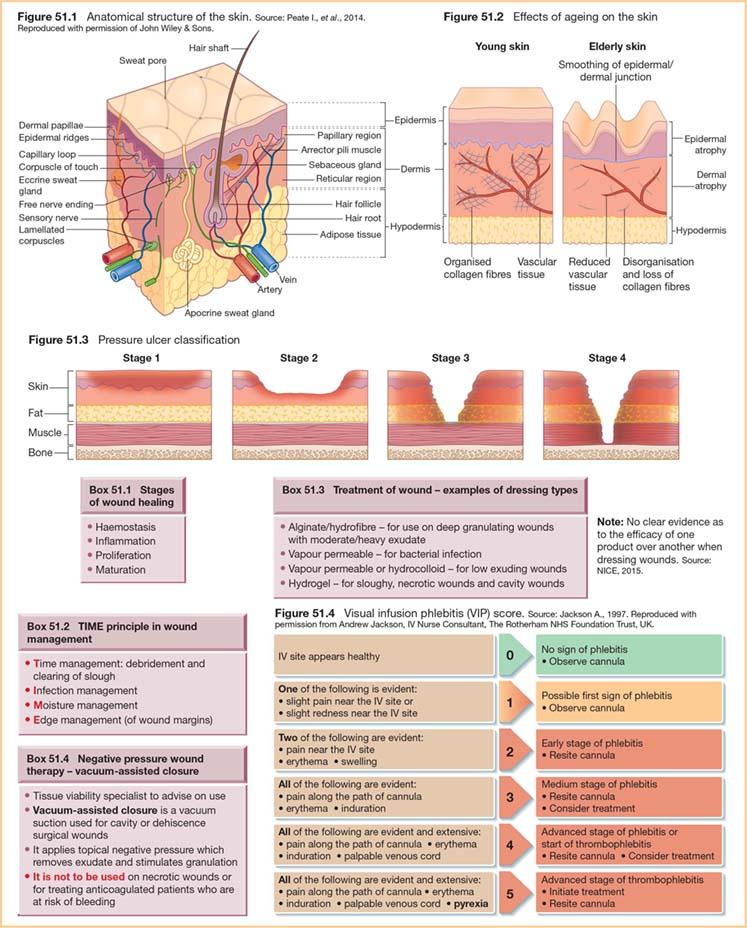
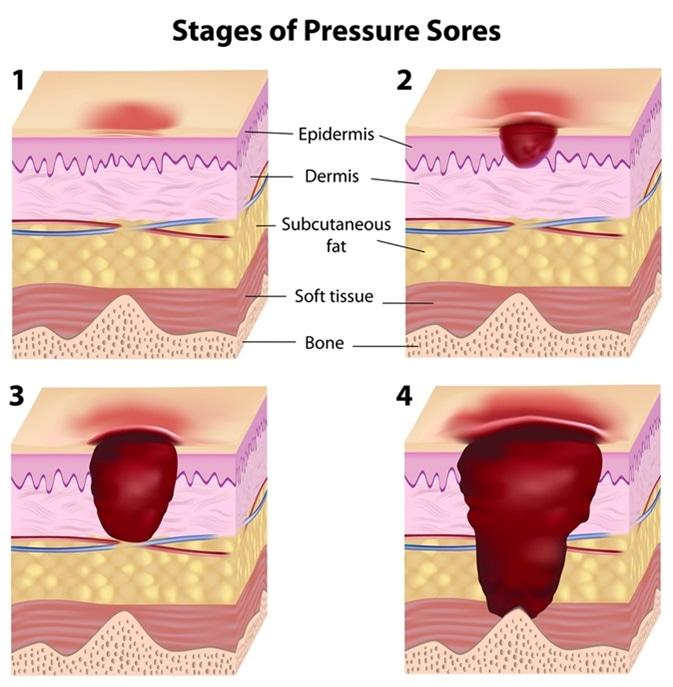
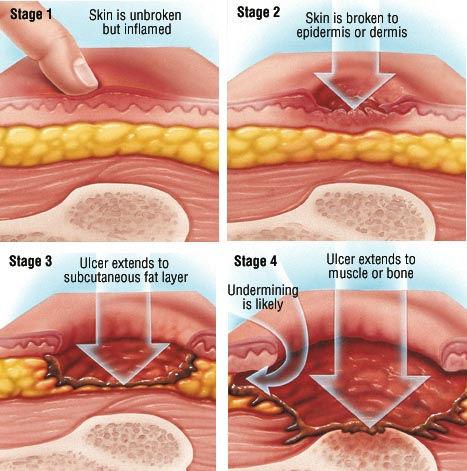
The client has a documented stage II pressure ulcer on the right hip. What NANDA nursing diagnosis problem statement is most appropriate to use with this client?
Explanation
A stage II pressure ulcer is a wound that involves partial-thickness loss of skin. The most appropriate NANDA nursing diagnosis problem statement for a client with this condition would be Impaired Skin Integrity. This diagnosis reflects the fact that the client's skin has been damaged and is no longer intact. Risk for Injury, Altered Tissue Perfusion, and Impaired Tissue Integrity are also NANDA nursing diagnoses, but they are not as specific or relevant to the client's condition as Impaired Skin Integrity.
A nurse is caring for a client in the introductory (orientation) phase of the nurse-client relationship. Which of the following communication techniques should the nurse use during this phase?
Explanation
During the introductory (orientation) phase of the nurse-client relationship, the nurse should focus on establishing trust and rapport with the client. One way to do this is by eliciting information from the client through active listening and open-ended questioning. This allows the nurse to gather important information about the client's health status, needs, and concerns, and helps to establish a foundation for the therapeutic relationship. Reviewing progress toward personal objectives and encouraging self-exploration are more appropriate for later phases of the relationship. Talking with others who have information about the client may also be helpful, but it is important to prioritize direct communication with the client during this phase.
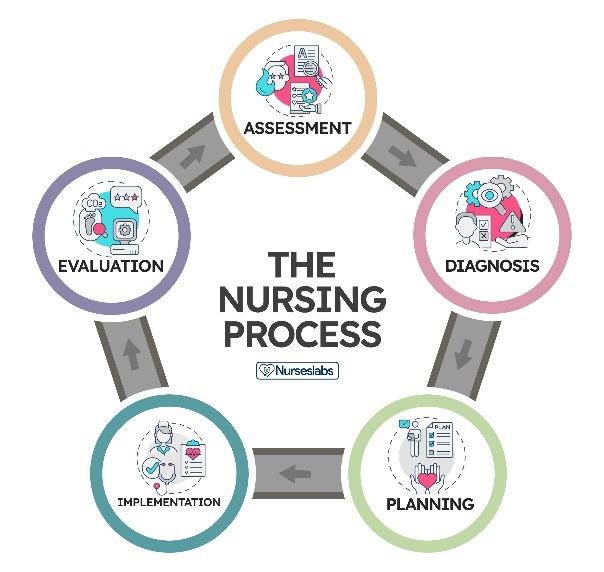
While conducting a dressing change, the nurse notes a new area of skin breakdown that was caused from the tape used to secure the dressing. In which phase of the nursing process is the nurse working?
Explanation
The nursing process consists of five phases: assessment, diagnosis, planning, implementation, and evaluation. During the assessment phase, the nurse gathers information about the client's health status and needs. In this scenario, the nurse is conducting a dressing change and notes a new area of skin breakdown. This observation is part of the assessment phase of the nursing process, as the nurse is gathering information about the client's condition. The other phases of the nursing process involve analyzing the information gathered during assessment (diagnosis), developing a plan of care (planning), carrying out interventions (implementation), and evaluating the effectiveness of care (evaluation).
While performing a bed bath, the nurse notes an area of tissue injury on the client's sacral area. The wound presents as a shallow open ulcer with a red-pink wound bed and partial thickness loss of dermis. What is the correct name of this wound?
Explanation
A stage II pressure ulcer is a wound that presents as a shallow open ulcer with a red-pink wound bed and partial thickness loss of dermis. This type of wound is caused by unrelieved pressure on the skin, resulting in damage to the underlying tissue. In this scenario, the nurse notes an area of tissue injury on the client's sacral area that matches the description of a stage II pressure ulcer. Stage I pressure ulcers are characterized by non-blanchable erythema of intact skin, while stage III and IV pressure ulcers involve full-thickness tissue loss and may expose underlying muscle, bone, or other structures.
A client needs a test to determine the amount of residual urine. The nurse realizes that this assessment is used for which reason(s)? Select all that apply.
Explanation
A test to determine the amount of residual urine is used to measure the amount of urine that remains in the bladder after voiding. This assessment can be used for several reasons, including to determine the need for medications that can help improve bladder emptying and to evaluate the amount of retained urine after voiding. Retained urine can increase the risk of urinary tract infections and other complications. This test is not typically used to evaluate fluid volume status, glomerular filtration rate, or the extent of renal failure.
A client is hospitalized with numerous acute health problems. According to Maslow's hierarchy of needs model, which nursing diagnosis should the nurse identify as being the highest priority for this client?
Explanation
According to Maslow's hierarchy of needs model, physiological needs such as food, water, and shelter are the most basic and fundamental needs that must be met before higher-level needs can be addressed. In this scenario, the nursing diagnosis of Altered Nutrition, Less Than Body Requirements related to inability to absorb nutrients addresses a fundamental physiological need and should be identified as the highest priority for this client. The other nursing diagnoses listed address important needs related to safety, self-care, and psychological well-being, but these needs are considered higher-level needs according to Maslow's hierarchy and should be addressed after the client's basic physiological needs have been met.

Which of the following principles does the nurse use in selecting interventions for the care plan?
Explanation
When selecting interventions for a care plan, the nurse should consider several principles. One important principle is that actions should address the underlying cause (etiology) of the nursing diagnosis. By addressing the root cause of the problem, interventions can be more effective in achieving the desired outcomes. There is not necessarily one "best" intervention for each goal or outcome, as different clients may have different needs and respond differently to interventions. Interventions can include both "doing" actions and monitoring, and both independent and collaborative interventions may be appropriate depending on the situation.
While in the dining room at the hospital, the nurse notes a visitor has forceful coughs. Which actions would the nurse take to assist this visitor?
Explanation
If a visitor in the dining room at the hospital has forceful coughs, the nurse should first allow the visitor to continue coughing. Coughing is a natural reflex that helps clear the airway of foreign objects or mucus. The nurse should also assess the effectiveness of the cough. If the cough is weak or ineffective, further intervention may be necessary. Starting cardiopulmonary resuscitation (CPR) or performing the Heimlich maneuver would only be appropriate if the visitor is choking and unable to breathe. Assisting the client to a sitting position on the floor may not be necessary and could potentially cause harm.
A client is prescribed a diuretic for swelling of the lower extremities. The nurse should teach the client about the effect of the medication on the client's urinary output.
Explanation
A diuretic is a medication that increases the production of urine by the kidneys. This can help reduce swelling (edema) by removing excess fluid from the body. If a client is prescribed a diuretic for swelling of the lower extremities, the nurse should teach the client that the medication will increase their urinary output. This means that the client will need to urinate more frequently and may produce more urine than usual. The color and odor of the urine may also change, but these changes are not directly related to the effect of the medication on urinary output.

A client has the goal statement "Client will be able to state two positive aspects of rehab therapy by the end of the week." One of the following statements demonstrates that the nurse appropriately evaluated this goal.
Explanation
This statement demonstrates that the nurse appropriately evaluated the goal because it shows that the client was able to meet the goal of stating two positive aspects of rehab therapy by the end of the week. The other statements indicate that the outcome was either not met, incomplete or only partially met.
While conducting a dressing change, the nurse notes a new area of skin breakdown that was caused from the tape used to secure the dressing. In which phase of the nursing process is the nurse working?
Explanation
The nursing process consists of five phases: assessment, diagnosis, planning, implementation, and evaluation. During the assessment phase, the nurse gathers information about the client's health status and needs. In this scenario, the nurse is conducting a dressing change and notes a new area of skin breakdown. This observation is part of the assessment phase of the nursing process, as the nurse is gathering information about the client's condition. The other phases of the nursing process involve analyzing the information gathered during assessment (diagnosis), developing a plan of care (planning), carrying out interventions (implementation), and evaluating the effectiveness of care (evaluation).
A nurse is caring for an older adult client who is at risk for skin breakdown. The nurse should use which of the following interventions to help maintain the integrity of the client's skin?
Explanation
A diet high in protein can help maintain skin integrity in older adults ⁵. Protein is essential for tissue repair and wound healing. The other options may not be as effective in maintaining skin integrity. For example, repositioning the client every 3 hours may not be frequent enough to prevent pressure ulcers ³. Applying cornstarch to keep the skin dry may not be the best option as it is important to keep the skin moisturized ⁴. Massaging bony prominences to promote circulation may not be recommended as it could cause damage to fragile skin ³.
A client is experiencing hypoxia. The nursing diagnosis that would be appropriate is:
Explanation
Anxiety is a nursing diagnosis that would be appropriate for a client experiencing hypoxia. Hypoxia can cause shortness of breath and difficulty breathing, which can lead to feelings of anxiety. The other options (Hypothermia, Nausea, and Pain) are not directly related to hypoxia.
Sign Up or Login to view all the 71 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
