Ati growth and development exam
Total Questions : 41
Showing 25 questions, Sign in for moreA nurse is helping to teach a class on prenatal development. The nurse should explain that advanced maternal age raises the risk for which of the following conditions?
Explanation
Choice A reason: Asthma is a chronic condition characterized by respiratory symptoms such as wheezing, shortness of breath, and coughing due to airway inflammation and constriction. While genetic and environmental factors contribute to the development of asthma, there is no direct correlation between advanced maternal age and an increased risk of asthma in offspring. Asthma's etiology is multifactorial and more closely related to family history, exposure to allergens, and respiratory infections during early childhood.
Choice B reason: Spina bifida is a neural tube defect that occurs when the spine and spinal cord don't form properly. It's associated with factors such as folic acid deficiency during early pregnancy, certain medications, diabetes, and obesity. Although advanced maternal age may slightly increase the risk of chromosomal abnormalities, it is not considered a significant risk factor for spina bifida. Adequate intake of folic acid before conception and during early pregnancy is the most effective prevention strategy.
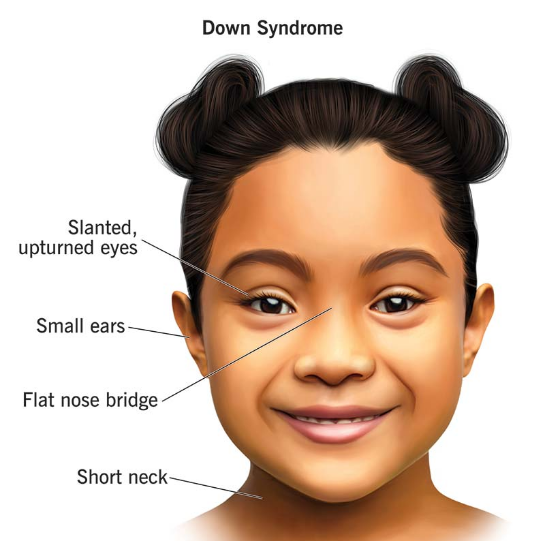
Choice C reason: Down syndrome is a genetic disorder caused by the presence of an extra copy of chromosome 21 (trisomy 21). The risk of conceiving a child with Down syndrome increases with maternal age, particularly after age 35. This is due to the higher likelihood of nondisjunction events during cell division in older eggs, leading to an abnormal number of chromosomes. Advanced maternal age is a well-established risk factor for Down syndrome, and prenatal screening is recommended to assess the risk.
Choice D reason: Facial malformations, such as cleft lip or palate, are congenital anomalies that can affect the appearance and function of a child's face. These conditions are influenced by genetic and environmental factors, including certain medications, nutritional deficiencies, and exposure to harmful substances during pregnancy. While advanced maternal age may contribute to an increased risk of chromosomal abnormalities, it is not specifically linked to an increased risk of isolated facial malformations.
A nurse is helping to assess a client's understanding of the teaching regarding insomnia. Which of the following client statements demonstrates an understanding of the information provided?
Explanation
Choice A reason: Going to bed at the same time every night, even when not feeling tired, can help regulate the body's clock and aid in falling asleep at a regular time. However, lying in bed awake can lead to frustration and should be avoided. If sleep does not come within 20 minutes, it's recommended to get up and do something relaxing until feeling sleepy.
Choice B reason: Exercising can increase alertness and endorphin levels which can make it difficult to fall asleep if done too close to bedtime. Stopping exercise at least 2 hours before bedtime allows the body to wind down and prepare for sleep, making this statement correct and indicative of an understanding of good sleep hygiene practices.
Choice C reason: Watching television or engaging in other stimulating activities in the bedroom can associate the space with wakefulness rather than sleep. The light from screens can also suppress melatonin production, making it harder to fall asleep. Therefore, this statement does not reflect an understanding of the teaching on good sleep practices.
Choice D reason: Taking long naps, especially in the late afternoon or evening, can interfere with nighttime sleep. If naps are necessary, they should be limited to 20-30 minutes and taken earlier in the day. This statement suggests a misunderstanding of the impact of napping on sleep quality at night.
A nurse is caring for a client who reports feeling stressed due to the inability to balance work demands and caregiving for an ill family member. The nurse should recognize that the client is experiencing which of the following self-concept stressors?
Explanation
Choice A reason: Identity refers to how individuals perceive themselves, including their beliefs, qualities, and expressions. It is the understanding of oneself as a distinct individual. In the context of the client's situation, while stress can impact one's sense of identity, the primary issue described does not directly relate to the client's identity but rather to their ability to fulfill expected roles.
Choice B reason: Role performance stressors arise when individuals feel they cannot meet the expectations associated with their social or work roles. In this case, the client is stressed due to the difficulty in balancing work responsibilities with the demands of caring for an ill family member. This indicates a conflict in role performance, as the client struggles to adequately fulfill the roles of both employee and caregiver.
Choice C reason: Body image pertains to one's perception of the physical self and the feelings associated with this perception. It includes how individuals view their own body and how they believe others perceive it. The client's stress does not stem from concerns about body image but from the pressures of their responsibilities.
Choice D reason: Self-esteem is the value one places on oneself, encompassing feelings of worthiness or unworthiness. It is influenced by various factors, including personal achievements and recognition from others. Although self-esteem can be affected by stress, the scenario provided specifically highlights the client's stress related to role fulfillment, not their self-worth.
A nurse is caring for a client who says, "I didn't take my medication because my partner forgot to remind me." The nurse should recognize that the client is exhibiting which of the following defense mechanisms?
Explanation
Choice A reason: Rationalization is a defense mechanism where an individual justifies behaviors or feelings with plausible but inaccurate explanations to avoid confronting the true underlying motives or facts. In this scenario, the client is rationalizing their failure to take medication by blaming their partner's forgetfulness, rather than accepting personal responsibility for their health management.
Choice B reason: Projection involves attributing one's own unacceptable thoughts, feelings, or motives to another person. If the client had accused their partner of being irresponsible with medication as a reflection of their own behavior, it would be an example of projection. However, in this case, the client is not projecting their own forgetfulness onto their partner but rather shifting the blame.
Choice C reason: Repression is an unconscious mechanism employed by the ego to keep disturbing or threatening thoughts from becoming conscious. It involves pushing uncomfortable thoughts or memories into the unconscious mind. The client's statement does not suggest they are unconsciously forgetting to take their medication; instead, they are consciously aware of their action and providing a justification for it.
Choice D reason: Regression is a return to earlier stages of development and abandoned forms of gratification belonging to them, prompted by dangers or conflicts arising at one of the later stages. A client demonstrating regression might exhibit childlike behaviors when faced with stress. The client's statement does not indicate a regression to more infantile behaviors or coping mechanisms.
A nurse is helping to teach a class about Piaget's stages of cognitive development. The nurse should emphasize that abstract thinking emerges during which of the following stages?
Explanation
Choice A reason: The formal operational stage is the fourth and final stage of Jean Piaget's theory of cognitive development. It begins at approximately age 11 and continues into adulthood. During this stage, individuals develop the ability to think about abstract concepts. Skills such as logical thought, deductive reasoning, and systematic planning also emerge during this stage. This is the stage where individuals move beyond concrete experiences and begin to think abstractly, reason logically, and draw conclusions from the information available, as well as apply all these processes to hypothetical situations.
Choice B reason: The sensorimotor stage is the first of Piaget's stages, which lasts from birth to about age 2. During this stage, infants learn about the world through their senses and their motor actions. At this stage, children learn about their environment by manipulating objects, but they do not yet understand abstract concepts.
Choice C reason: The preoperational stage spans ages 2 to 7. In this stage, children start to engage in symbolic play and learn to manipulate symbols, but they do not yet understand concrete logic. Abstract thinking is not developed in this stage; children are focused on the concrete, tangible aspects of their environment and their immediate perceptions.
Choice D reason: The concrete operational stage occurs between ages 7 to 11. Children in this stage begin to think logically about concrete events. They gain a better understanding of the concept of conservation and other mathematical concepts. However, their thinking is still very concrete; they have not yet developed the ability to think abstractly.
A nurse is caring for a client with a terminal diagnosis who says, "I am ready to update my will." The nurse should recognize that the client is in which of the following Kübler-Ross stages of grief?
Explanation
Choice A reason: Denial is the first stage of the Kübler-Ross model of grief. In this stage, individuals believe the diagnosis is somehow mistaken, and cling to a false, preferable reality. It is a defense mechanism that buffers the immediate shock of the loss, numbing us to our emotions.
Choice B reason: Anger is the second stage of grief. As the masking effects of denial begin to wear off, reality and its pain re-emerge. The intense emotion is deflected from our vulnerable core, redirected and expressed instead as anger. The anger may be aimed at inanimate objects, complete strangers, friends, or family.
Choice C reason: Bargaining is the third stage. It involves the hope that the individual can avoid a cause of grief. Usually, the negotiation for an extended life is made with a higher power in exchange for a reformed lifestyle.
Choice D reason: Acceptance is the final stage of grief. In this stage, individuals embrace mortality or the inevitable future, or that of a loved one, or other tragic event. People dying may precede the survivors in this state, which typically comes with a calm, retrospective view for the individual, and a stable condition of emotions.
A nurse is helping to teach a class about cultural bias in healthcare. The nurse should mention that which of the following can result from cultural bias?
Explanation
Choice A reason: Cultural bias can negatively impact data collection by causing healthcare providers to make assumptions based on stereotypes rather than individual assessments. This can lead to incomplete or inaccurate data, as certain symptoms or health issues may be overlooked or misattributed to cultural factors.
Choice B reason: Cultural bias can significantly impair the therapeutic relationship between healthcare providers and clients. When providers have preconceived notions about a patient's culture, they may communicate less effectively, make incorrect assumptions, or fail to build trust. This can result in a lack of adherence to treatment plans and decreased patient satisfaction.
Choice C reason: While spending more time with each client could be seen as beneficial, cultural bias does not inherently lead to this outcome. In fact, bias may cause providers to spend less time with clients from certain backgrounds due to misconceptions or communication barriers.
Choice D reason: Cultural bias is a known contributor to healthcare disparities, not a solution to them. Biases can lead to unequal treatment, access, and outcomes across different cultural groups.
A nurse is caring for a client who is unresponsive and nearing the end of life. Which of the following actions should the nurse perform?
Explanation
Choice A reason: Continue to talk to the client as if they are awake.Even when a client is unresponsive, they may still be able to hear and benefit from hearing a familiar voice. Continuing to talk to the client can provide comfort and reassurance during the end-of-life stage.
Choice B reason: Whisper when talking in the client's room.Whispering can create a sense of secrecy and exclusion. It is important to communicate in a normal tone, respecting the client's presence and dignity.
Choice C reason: Limit the client's visitors to one at a time.Limiting visitors can be appropriate in certain situations to maintain a calm environment; however, it should be based on the client's wishes and needs, not as a general practice.
Choice D reason: Avoid touching the client.Appropriate touch can be comforting to an unresponsive client, conveying care and presence. It should not be avoided unless there is a specific reason to do so, such as pain or discomfort.
A nurse is helping to educate a client about over-the-counter medications for treating insomnia. The nurse should mention that which of the following is an adverse reaction of diphenhydra
Explanation
Choice A reason: Dry mouth, also known as xerostomia, is a common side effect of diphenhydramine, an antihistamine used to treat insomnia among other conditions. It occurs because diphenhydramine has anticholinergic properties, which means it inhibits the action of the neurotransmitter acetylcholine. This inhibition can reduce saliva production, leading to a feeling of dryness in the mouth.
Choice B reason: Hypertension, or high blood pressure, is not a typical side effect of diphenhydramine. While some medications, particularly decongestants, can raise blood pressure, diphenhydramine does not usually have this effect. However, individuals with pre-existing heart conditions should consult a healthcare provider before using it.
Choice C reason: Memory loss is not commonly listed as a side effect of diphenhydramine. However, because it can cause drowsiness and has sedative effects, it may lead to temporary forgetfulness or confusion, especially in older adults or when taken in higher doses.
Choice D reason: 'Medications' is not an adverse reaction but rather a general term for drugs used to diagnose, treat, or prevent illness. In the context of diphenhydramine, it would be more appropriate to discuss specific side effects or adverse reactions related to its use.
A nurse is helping to teach a class on cultural bias in healthcare. The nurse should include that which of the following outcomes can result from cultural bias?
Explanation
Choice A reason: Cultural bias does not typically result in an increased amount of time spent with each client. In fact, cultural bias can lead to unequal time allocation, where some clients may receive less attention due to preconceived notions or stereotypes.
Choice B reason: Improved data collection on clients.Cultural bias can negatively affect the quality of data collection on clients. It can lead to assumptions that overlook individual client needs and circumstances, resulting in incomplete or inaccurate health records.
Choice C reason: Increased disparities in health care.Cultural bias in health care can lead to increased disparities. It affects how healthcare providers perceive and interact with patients from different cultural backgrounds, potentially resulting in unequal treatment, misdiagnosis, and reduced access to care for certain groups.
Choice D reason: Improved therapeutic communication with clients.Cultural bias can impair therapeutic communication with clients. When healthcare providers harbor unconscious biases, it can hinder effective communication, leading to misunderstandings and a lack of trust.
A nurse is helping to teach a class about sources of stress. The nurse should mention that which of the following is an example of a physiological stressor?
Explanation
Choice A reason: Change in marital status.A change in marital status is considered a social stressor rather than a physiological one. It relates to the personal and emotional aspects of one's life, impacting mental and emotional well-being rather than directly causing a physiological response
.
Choice B reason: Financial difficulties.Financial difficulties are categorized as social stressors. They can lead to significant stress but do not directly cause a physiological response. Instead, they can indirectly affect health over time through sustained stress.
Choice C reason: Academic pressure.Academic pressure is a psychological stressor. It involves cognitive and emotional challenges that can lead to stress but is not a direct physiological stressor.
Choice D reason: Burn injury.A burn injury is a physiological stressor. It causes an immediate physical response in the body, triggering pain receptors, inflammatory responses, and the need for physical healing processes.
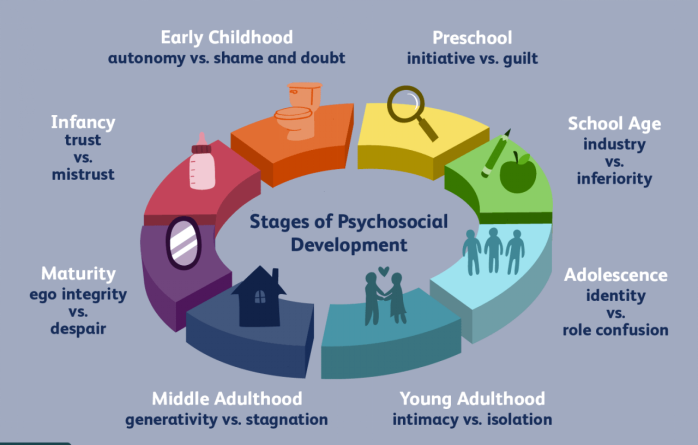
A nurse is caring for an infant whose caregiver immediately comforts them when they cry. The nurse should recognize that the client is in which of the following stages of Erikson's theory of psychosocial development?
Explanation
Choice A reason: Trust vs. Mistrust.The stage of Trust vs. Mistrust is the first stage of Erikson's theory of psychosocial development, occurring from birth to approximately 18 months of age. In this stage, the infant is uncertain about the world and looks towards their primary caregiver for stability and consistency of care. If the caregiver is reliable, consistent, and nurturing, the child will develop a sense of trust, believing that the world is safe and that people are dependable and affectionate. This sense of trust allows the child to feel secure even when threatened and extends into their other relationships, maintaining their sense of security amidst potential threats.
Choice B reason: Autonomy vs. Shame and Doubt.The stage of Autonomy vs. Shame and Doubt is the second stage of Erikson's theory, spanning the toddler years from 18 months to three years. In this stage, toddlers begin to assert their independence by making choices and taking control over their actions. Success in this stage leads to feelings of autonomy, while failure results in feelings of shame and doubt. However, this stage is not applicable to the scenario described, as it involves an infant, not a toddler.
Choice C reason: Identity vs. Role Confusion.Identity vs. Role Confusion is the fifth stage, occurring during the teen years from 12 to 18. This stage is characterized by the exploration of personal identity and the development of a sense of self. The scenario provided does not pertain to an adolescent, so this stage is not relevant to the infant's experience.
Choice D reason: Integrity vs. Despair.The stage of Integrity vs. Despair is the eighth and final stage of Erikson's theory, occurring in older adulthood from 65 to death. This stage involves reflecting on one's life and either concluding it with a sense of integrity and fulfillment or with a sense of despair over a life misspent. This stage is not applicable to the infant described in the scenario.
A nurse is helping to educate a client about the sleep-wake cycle. The nurse should mention that which of the following factors can disrupt the sleep-wake cycle?
Explanation
Choice A reason: Drinking caffeinated beverages in the evening.Caffeine is a stimulant that can significantly disrupt the sleep-wake cycle. Consuming caffeinated beverages in the evening can lead to difficulty initiating sleep because caffeine blocks the action of adenosine, a chemical that promotes sleep. The effects of caffeine can last several hours, thus affecting the quality and duration of sleep.
Choice B reason: Emotional stress activates the body's stress response, causing the release of hormones like cortisol, which increases alertness and can delay the onset of sleep. Chronic stress can lead to a hyperarousal state, making it difficult to fall asleep and stay asleep.
Choice C reason: Bright light.Exposure to bright light, especially blue light from screens, can interfere with the production of melatonin, the hormone that signals the body to prepare for sleep. This can shift the circadian rhythm and disrupt the sleep-wake cycle, making it harder to fall asleep at the usual time.
Choice D reason: A short nap during the day, typically 20-30 minutes, can be beneficial and usually does not interfere with nighttime sleep. However, longer or later naps can make it more difficult to fall asleep at night
A nurse is helping to teach a class on Kohlberg's theory of moral development. The nurse should emphasize that which of the following stages involves questioning rules that infringe on the rights of others?
Explanation
Choice A reason: The "Good boy-nice girl" orientation is part of Kohlberg's Conventional level of moral development. In this stage, individuals are motivated by the desire to maintain relationships and gain approval from others. They make decisions based on what will please others and show concern for others by being "nice." This stage does not typically involve challenging rules but rather adhering to them to maintain social harmony.
Choice B reason: The "Punishment and obedience" orientation is the first stage of Kohlberg's Preconventional level. Here, the focus is on direct consequences to the individual: actions are judged as good if they help avoid punishment. This stage is characterized by a literal obedience to rules and authority to avoid negative consequences, not by challenging them.
Choice C reason: The "Law and order" orientation is the fourth stage, also within the Conventional level. In this stage, individuals are oriented to abiding by the law and respecting authority. They believe in maintaining the social order by following rules and laws. Challenging rules is not a characteristic of this stage; instead, there is a focus on upholding laws as they are.
Choice D reason: The "Social contract" orientation is part of the Postconventional level of moral development, specifically the fifth stage. Individuals in this stage believe that rules and laws are flexible instruments for furthering human purposes. They can argue for the legality or principle behind the rule and may challenge rules that infringe on the rights of individuals. They understand that laws are created by people and can be changed by them. This stage involves the recognition that individual rights sometimes need to be upheld over and above the law.
A nurse is caring for a client with impaired speech. Which of the following actions should the nurse perform?
Explanation
Choice A reason: Allow extra time to communicate with the client.Allowing extra time to communicate is essential when caring for clients with impaired speech. This approach respects the client's pace and supports their efforts to express themselves, which can be a time-consuming process. It also helps to reduce frustration and anxiety that the client may feel if rushed.
Choice B reason: Ask open-ended questions.Asking open-ended questions to a client with impaired speech can be challenging for them to answer and may lead to frustration. Instead, it's recommended to ask yes/no questions or provide choices to facilitate easier communication.
Choice C reason: Finish sentences for the client.Finishing sentences for a client with impaired speech is generally discouraged as it can lead to miscommunication and may make the client feel disempowered. It's important to allow the client to express themselves in their own words and time.
Choice D reason: Avoid using visual aids for communication.Using visual aids can be very helpful for clients with impaired speech. Visual aids such as pictures, gestures, or writing can support understanding and expression, making communication more effective.
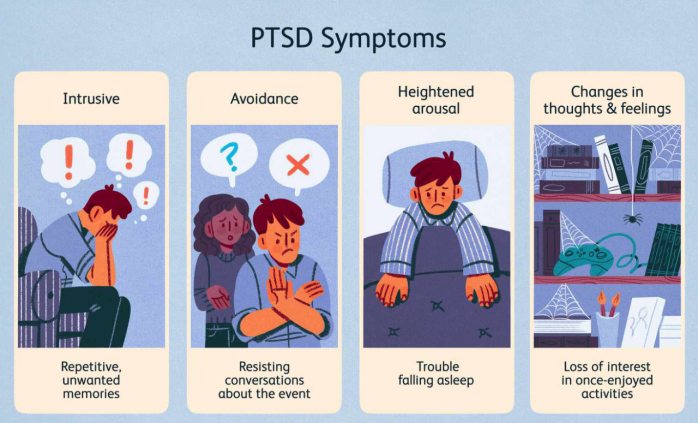
A nurse is caring for a client who reports having flashbacks of a traumatic event that happened a year ago. The nurse should recognize that the client is experiencing which of the following stress-related disorders?
Explanation
Choice A reason: Irritable bowel syndrome (IBS).IBS is a gastrointestinal disorder characterized by a group of symptoms including abdominal pain and changes in the pattern of bowel movements without any evidence of underlying damage. It is not typically related to flashbacks or stress-related disorders.
Choice B reason: Posttraumatic stress disorder (PTSD).PTSD is a mental health condition triggered by a terrifying event, either experiencing it or witnessing it. Symptoms include flashbacks, nightmares, severe anxiety, and uncontrollable thoughts about the event. The client's experience of flashbacks is a characteristic symptom of PTSD.
Choice C reason: Acute stress disorder (ASD).ASD is characterized by the development of severe anxiety, dissociation, and other symptoms that occur within one month after exposure to an extreme traumatic stressor. As the client reports flashbacks of an event from a year ago, ASD would not be the correct diagnosis due to the time frame.
Choice D reason: Episodic acute stress.Episodic acute stress refers to frequent episodes of acute stress, not necessarily related to flashbacks or a specific traumatic event. It is more about the reaction to the demands of life and is not characterized by flashbacks of a traumatic event.
A nurse is helping to teach a class about physiological changes that happen during sleep. The nurse should mention that which of the following changes occur during non-rapid eye movement (NREM) sleep?
Explanation
Choice A reason: Increase in basal metabolic rate.During NREM sleep, particularly in the deeper stages, the basal metabolic rate (BMR) actually decreases. This reduction in BMR is part of the restorative processes that occur during sleep, conserving energy for the body to use in repair and growth.
Choice B reason: Reduced secretion of growth hormones.Contrary to this statement, the secretion of growth hormones increases during NREM sleep, particularly during the deep stages (stage N3). These hormones play a crucial role in tissue growth and muscle repair.
Choice C reason: Decrease in body temperature.During NREM sleep, there is a decrease in body temperature as part of the body's thermoregulation process. This helps to conserve energy and is a characteristic physiological change during this phase of sleep.
Choice D reason: Constriction of peripheral blood vessels.Peripheral blood vessels do not typically constrict during NREM sleep. Instead, there is generally a decrease in sympathetic nervous system activity, which can lead to the dilation of blood vessels and a decrease in blood pressure.
A nurse is reinforcing education with a client who has diabetes mellitus about diabetic retinopathy. Which of the following statements should the nurse provide?
Explanation
Choice A reason: Have an eye exam every 2 years.For individuals with diabetes, it is recommended to have an eye exam annually, not every two years, due to the high risk of developing diabetic retinopathy and the need for early detection and treatment.
Choice B reason: It is caused by an increase in intraocular pressure.Diabetic retinopathy is not caused by an increase in intraocular pressure; that is more characteristic of glaucoma. Diabetic retinopathy is caused by damage to the blood vessels in the retina due to high blood sugar levels.
Choice C reason: Clouding of the lens is a manifestation of diabetic retinopathy.Clouding of the lens is a manifestation of cataracts, not diabetic retinopathy. Diabetic retinopathy involves changes to the blood vessels in the retina, not the lens of the eye.
Choice D reason: "Seeing spots is a manifestation of diabetic retinopathy.""Seeing spots," or floaters, can indeed be a manifestation of diabetic retinopathy. This occurs when blood vessels in the retina are damaged and leak blood or other fluids, causing these spots to appear in the vision.
A nurse is caring for a client with a new diagnosis of bladder cancer. Which of the following interventions should the nurse implement to enhance comfort?
Explanation
Choice A reason: Provide limited explanations of procedures needed for the client.Providing limited explanations of procedures can increase anxiety and discomfort for clients, especially those facing a new cancer diagnosis. It is important to give comprehensive information to help them understand their condition and the treatments they will undergo.
Choice B reason: Provide honest answers to the client's questions.Providing honest answers to the client's questions is crucial in promoting comfort and trust. It allows the client to make informed decisions about their care and helps them to prepare mentally and emotionally for the treatments and their potential outcomes.
Choice C reason: Avoid eye contact with the client during care.Avoiding eye contact can make the client feel isolated and unimportant. Maintaining eye contact is a non-verbal way of showing respect, concern, and willingness to engage with the client.
Choice D reason: Avoid giving the client choices regarding their care.Avoiding giving choices can lead to a feeling of loss of control, which can be distressing for clients. It is important to involve clients in decisions about their care to promote their autonomy and comfort.
A nurse is helping to teach a class about vulnerable populations at risk for health disparities. The nurse should mention that a client living in a crowded apartment building is at risk for which of the following conditions?
Explanation
Choice A reason: Deep vein thrombosis (DVT) is a condition where a blood clot forms in a deep vein, usually in the legs. While certain factors like immobility, surgery, and certain medications can increase the risk of DVT, living in a crowded apartment building is not typically associated with an increased risk of developing this condition.
Choice B reason: Crowded living conditions can increase the risk of the spread of infectious diseases. This is due to the close proximity of individuals, which facilitates the transmission of pathogens through respiratory droplets, shared surfaces, and common areas. Diseases such as respiratory infections, meningococcal disease, rheumatic fever, and tuberculosis are particularly associated with crowded living conditions.
Choice C reason: Rheumatoid arthritis is an autoimmune disorder characterized by chronic inflammation of the joints. It is not directly linked to living conditions but can be influenced by genetic factors and possibly environmental triggers. However, there is no established connection between crowded living conditions and the development of rheumatoid arthritis.
Choice D reason: While weight gain can be influenced by a variety of factors including diet, exercise, and genetics, there is no direct correlation between living in a crowded apartment and weight gain. However, it's worth noting that socioeconomic factors and limited access to healthy food options or safe areas for physical activity, which can be associated with crowded living conditions, may indirectly contribute to weight gain.
A nurse is caring for an adolescent client who reports starting to rebel against their caregivers and spending more time with friends. The nurse should recognize that the client is in which of the following stages of Erikson's theory of psychosocial development?
Explanation
Choice A reason: The stage of Autonomy vs. Shame and Doubt typically occurs during the toddler years, from 18 months to three years. In this stage, children begin to assert their independence. If they are encouraged and supported in their increased independence, they become more confident and secure in their ability to survive in the world. If children are criticized, overly controlled, or not given the opportunity to assert themselves, they begin to feel inadequate in their ability to survive and may become overly dependent upon others, lack self-esteem, and feel a sense of shame or doubt in their abilities.
Choice B reason: Identity vs. Role Confusion is the fifth stage of Erikson's theory and occurs during the adolescent years, from 12 to 18. In this stage, adolescents search for a sense of self and personal identity, through an intense exploration of personal values, beliefs, and goals. The adolescent mind is essentially a mind or moratorium, a psychosocial stage between childhood and adulthood, and between the morality learned by the child, and the ethics to be developed by the adult. This stage is characterized by the adolescent's struggle to find a balance between developing a unique, individual identity while still being accepted and "fitting in" with their peers and society. The rebellion against caregivers and increased time spent with friends, as mentioned in the scenario, are typical behaviors associated with this stage of development.
Choice C reason: Integrity vs. Despair is the eighth and final stage of Erikson's theory, which occurs during late adulthood, from age 65 to death. In this stage, individuals reflect on their lives and accomplishments. They develop a sense of integrity if they believe that they have led a successful, meaningful life. If they look back on a life of disappointments and unachieved goals, they may instead fall into despair over their past and fear of death.
Choice D reason: Trust vs. Mistrust is the first stage of Erikson's theory, occurring from birth to approximately 18 months. In this stage, infants learn to trust that their caregivers will meet their basic needs. If caregivers provide reliability, care, and affection, the child will develop a sense of trust which they will carry with them to other relationships, and they will be able to feel secure even when threatened. If these needs are not consistently met, mistrust, suspicion, and anxiety may develop.
A nurse is reinforcing education with a client who has diabetic neuropathy regarding foot care. Which of the following instructions should the nurse provide?
Explanation
Choice A reason: Applying lotion between the toes is not recommended for individuals with diabetic neuropathy. Moisture can accumulate in these areas, creating an environment conducive to fungal infections. Instead, lotion should be applied to the tops and bottoms of the feet to keep the skin moisturized and prevent cracking, but the areas between the toes should be kept dry.
Choice B reason: Wearing open-toed shoes is generally not advised for patients with diabetic neuropathy. Open-toed shoes can expose the feet to injuries, which can go unnoticed due to the loss of sensation associated with neuropathy. It's important for individuals with diabetic neuropathy to wear well-fitting, closed-toed shoes that protect the feet from external injuries.
Choice C reason: Washing feet in hot water is unsafe for those with diabetic neuropathy because they may not be able to accurately gauge the temperature due to reduced sensation, leading to burns. The water temperature should be warm, and individuals should always test it with their hands or a thermometer before immersing their feet.
Choice D reason: Walking barefoot is risky for individuals with diabetic neuropathy because they may not feel cuts, scrapes, or other injuries due to decreased sensation in their feet. These injuries can lead to infections and ulcers if not treated promptly. Therefore, it is crucial to avoid walking barefoot and to always wear protective footwear, even indoors.
A nurse is performing postmortem care for a client. Which of the following actions should the nurse carry out?
Explanation
Choice A reason: Removing the client's dentures is not typically a part of immediate postmortem care. Dentures are usually left in place to maintain the natural shape of the client's face, especially if the family will view the body.
Choice B reason: Increasing the lights in the client's room is not a standard procedure in postmortem care. The focus is on creating a respectful and dignified environment, which may include dimming the lights if it contributes to a peaceful setting.
Choice C reason: Placing the head of the client's bed flat is a standard practice in postmortem care. This helps to prevent blood pooling and discoloration of the body. It is part of the process of preparing the body for family viewing or transfer to a mortuary.
Choice D reason: Washing the client's body is indeed a part of postmortem care. The body should be gently cleansed, which helps to present a respectful appearance and also serves to remove any soiling that occurred at the time of death.
A nurse is caring for a client who is nearing the end of life and experiencing dyspnea. Which of the following actions should the nurse perform?
Explanation
Choice A reason: Administering an opioid narcotic can be an effective measure for managing dyspnea in end-of-life care. Opioids, such as morphine, can reduce the sensation of breathlessness and improve comfort without significantly affecting oxygen saturation levels. The use of opioids is a well-established practice in palliative care for the relief of dyspnea, particularly when other causes of dyspnea have been addressed and managed appropriately.
Choice B reason: Increasing the heat in the client's room is not a recommended action for managing dyspnea and may actually worsen the client's comfort. Patients experiencing dyspnea often feel better in a cooler environment, as warm temperatures can make breathing feel more labored.
Choice C reason: Placing the head of the client's bed flat is not advisable for managing dyspnea. Elevating the head of the bed can help ease breathing by reducing pressure on the diaphragm and allowing for better lung expansion. A semi-upright position, such as Fowler's or semi-Fowler's position, is typically recommended for patients experiencing dyspnea.
Choice D reason: Nasotracheal suctioning is a procedure used to clear secretions from the airway. While it may be necessary in some cases, it is not a standard action for managing dyspnea in end-of-life care unless there is a specific indication, such as excessive secretions that the patient cannot clear on their own. It can be uncomfortable and distressing for the patient and should be used judiciously.
A nurse is caring for a client who has just been diagnosed with diabetes mellitus. The client says, "I will never be able to follow the prescribed diet." Which of the following responses should the nurse provide?
Explanation
Choice A reason: This response is patient-centered and collaborative. It acknowledges the client's concerns and preferences, which is crucial in managing diabetes effectively. By involving the client in the decision-making process, the nurse empowers the client to take an active role in their health care. This approach can lead to better adherence to dietary recommendations and improved glycemic control. It is also aligned with the principles of effective communication with patients living with diabetes, which emphasize understanding, empathy, and cultural competency.
Choice B reason: This statement is accusatory and could make the client feel guilty or blamed for their condition. It is not constructive and does not contribute to a positive therapeutic relationship. Diabetes mellitus is a complex disease with multiple risk factors, including genetics, lifestyle, and environmental factors. It is not helpful to oversimplify the cause of the disease to one factor, such as diet alone.
Choice C reason: While this statement may be true for some, it does not acknowledge the individual challenges the client may face in adjusting to a new diet. It is important to recognize that each person's experience with diabetes and dietary changes is unique. A more supportive approach would be to offer guidance and resources to help the client gradually adapt to the changes.
Choice D reason: This statement is presumptive and does not take into account the client's current feelings or potential difficulties they may encounter. While a healthier diet can lead to better health outcomes, it is essential to validate the client's feelings and provide support and education to help them understand the benefits of the dietary changes.
Sign Up or Login to view all the 41 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
