ATI LPN Fundamentals Exam 1
Total Questions : 59
Showing 25 questions, Sign in for moreA nurse is reinforcing teaching about values to a newly licensed nurse. Which of the following statements by the newly licensed nurse indicates an understanding?
Explanation
Choice A reason: This statement is incorrect because a nurse’s personal values can and do influence ethical decisions. The nurse should be aware of their own values and how they affect their judgment and actions. The nurse should also respect the values of others and avoid imposing their own values on the clients or colleagues.
Choice B reason: This statement is incorrect because value clarification is not related to maintaining clinical competency. Value clarification is a process of identifying, examining, and prioritizing one’s values. It can help the nurse to understand their own values and beliefs, as well as those of the clients and the profession.
Choice C reason: This statement is correct because it is important that the nurse is aware of the client’s values. The nurse should assess the client’s values and preferences, and incorporate them into the plan of care. The nurse should also respect the client’s right to self-determination and autonomy, and support the client in making informed decisions.
Choice D reason: This statement is incorrect because a nurse's behaviors and actions are not called values. Values are the beliefs and principles that guide one’s decisions and actions. A nurse's behaviors and actions are the expressions of their values, as well as their knowledge, skills, and attitudes.
A charge nurse is reinforcing teaching with a newly licensed nurse about the advantages of electronic documentation. Which of the following information should the nurse include in the teaching?
Explanation
Choice A: This is the correct answer. A portal is a secure online platform that enables clients to access their health information, communicate with their providers, request appointments, refill prescriptions, and more. This enhances client satisfaction, engagement, and empowerment.
Choice B: This is incorrect. Same day access to client health record is not an advantage of electronic documentation, but a requirement for any documentation system. Clients have the right to access their health information within a reasonable time frame, regardless of whether it is paper-based or electronic.
Choice C: This is incorrect. The increase of duplicate tests performed on client is not an advantage of electronic documentation, but a disadvantage. Duplicate tests can result from poor communication, lack of interoperability, or human error. Electronic documentation can help reduce duplicate tests by facilitating data sharing, standardizing formats, and alerting providers of previous tests.
Choice D: This is incorrect. Decrease in coordination of client care is not an advantage of electronic documentation, but a disadvantage. Coordination of client care is essential for ensuring quality, safety, and continuity of care. Electronic documentation can improve coordination of client care by allowing multiple providers to access and update the same information, enabling real-time collaboration, and providing decision support tools.
A charge nurse is reinforcing teaching with a newly licensed nurse about accessing a client's medical records. Which of the following should the nurse include in the teaching?
Explanation
Choice A reason: This statement is incorrect because a nurse cannot access the records of any client in the healthcare facility, unless they have a legitimate need to do so. Accessing the records of clients who are not under their care is a violation of the client's privacy and confidentiality, and may result in legal or disciplinary actions.
Choice B reason: This statement is correct because a nurse can only access the records of clients they are actively caring for, as part of their professional duty and responsibility. Accessing the records of clients they are caring for is necessary to provide safe and effective care, and to communicate with other members of the healthcare team.
Choice C reason: This statement is incorrect because a nurse cannot share information from the client’s medical record with immediate family members, unless the client has given consent, or the disclosure is authorized by law. Sharing information from the client's medical record with family members without the client's permission is a breach of the client's privacy and confidentiality, and may cause harm or distress to the client or the family.
Choice D reason: This statement is incorrect because a nurse cannot share information about a client with clients who have a similar diagnosis, unless the client has given consent or the disclosure is authorized by law. Sharing information about a client with other clients without the client's permission is a breach of the client's privacy and confidentiality, and may compromise the client's dignity or safety.
A nurse is obtaining a health history from a client. Which of the following findings should the nurse identify as a nonmodifiable risk factor for disease?
Explanation
Choice A reason: Genetics is a nonmodifiable risk factor for disease because it is determined by the inherited traits from the parents. Genetics can influence the susceptibility, severity, and progression of certain diseases, such as cancer, diabetes, or cardiovascular disease. The nurse cannot change the client's genetic makeup, but can help the client to manage their condition and prevent complications.
Choice B reason: Sunbathing is a modifiable risk factor for disease because it is influenced by the client's behavior and lifestyle. Sunbathing can increase the exposure to ultraviolet (UV) radiation, which can damage the skin cells and cause skin cancer, premature aging, or sunburn. The nurse can educate the client on the importance of sun protection, such as using sunscreen, wearing protective clothing, and avoiding peak hours of sun exposure.
Choice C reason: Smoking is a modifiable risk factor for disease because it is influenced by the client's behavior and lifestyle. Smoking can harm the lungs, heart, blood vessels, and other organs, and increase the risk of various diseases, such as chronic obstructive pulmonary disease (COPD), lung cancer, or coronary artery disease. The nurse can assist the client in quitting smoking, such as providing counseling, nicotine replacement therapy, or pharmacological interventions.
Choice D reason: Unhealthy diet is a modifiable risk factor for disease because it is influenced by the client's behavior and lifestyle. Unhealthy diet can lead to obesity, malnutrition, or metabolic disorders, and increase the risk of various diseases, such as diabetes, hypertension, or stroke. The nurse can advise the client on the benefits of a balanced diet, such as eating more fruits, vegetables, whole grains, lean proteins, and healthy fats, and limiting the intake of salt, sugar, and saturated fats.
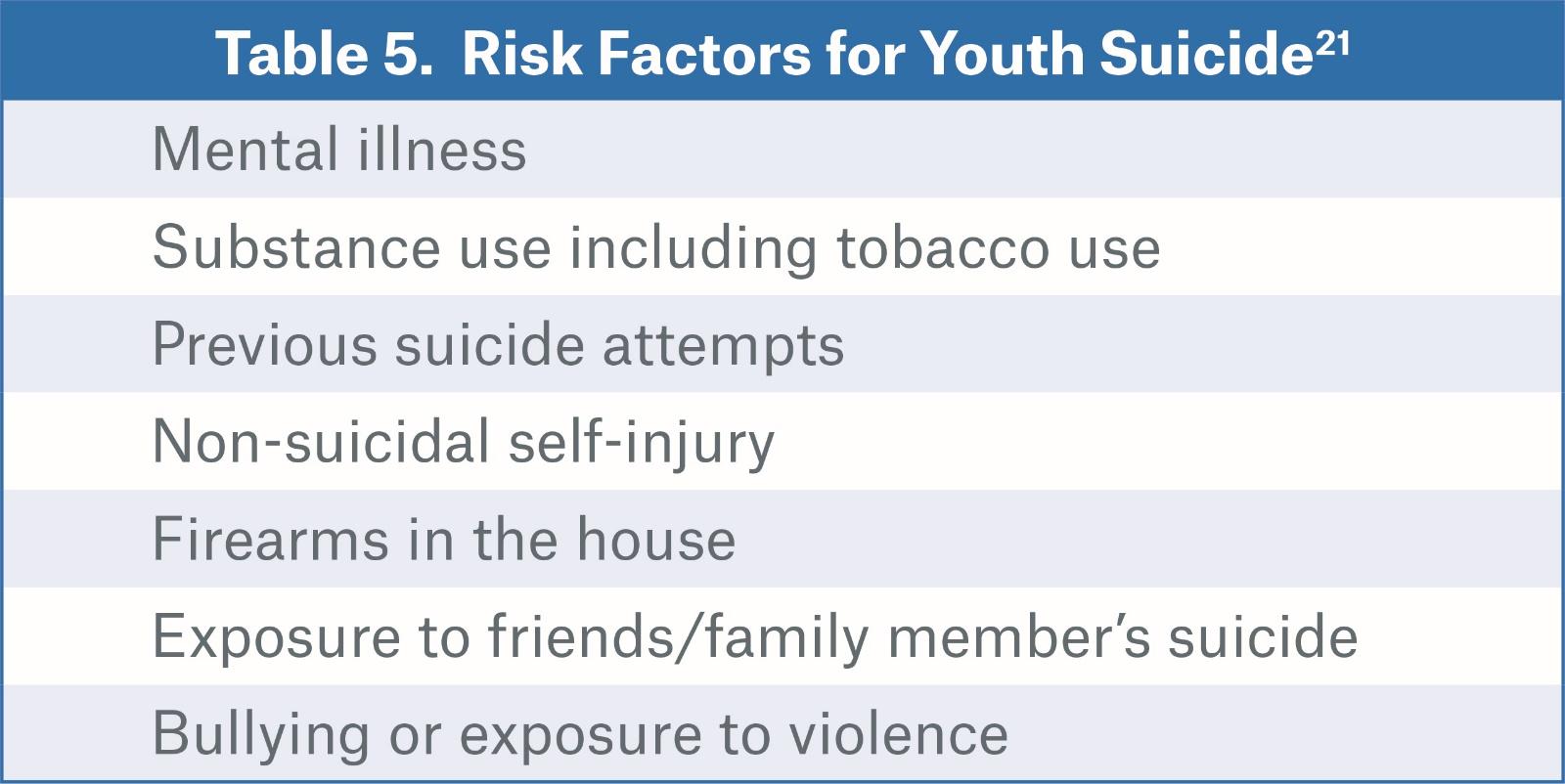
A nurse on an inpatient mental health unit is assisting with the admission of a client who reports feeling depressed, sad, moody, and overly anxious. Which of the following assessments should the nurse make first?
Explanation
Choice A reason: This statement is incorrect because psychiatric history is not the most urgent assessment to make for a client who reports feeling depressed and anxious. Psychiatric history can provide valuable information about the client's diagnosis, treatment, and response, but it is not a priority over the client's safety and wellbeing.
Choice B reason: This statement is correct because suicide risk is the most urgent assessment to make for a client who reports feeling depressed and anxious. Suicide risk can indicate the client's level of hopelessness, despair, and intent to harm themselves. The nurse should assess the client's suicidal thoughts, plans, means, and access, and implement appropriate interventions to prevent self harm or suicide.
Choice C reason: This statement is incorrect because support systems are not the most urgent assessment to make for a client who reports feeling depressed and anxious. Support systems can provide emotional, social, and practical assistance to the client, but they are not a priority over the client's safety and wellbeing.
Choice D reason: This statement is incorrect because coping abilities are not the most urgent assessment to make for a client who reports feeling depressed and anxious. Coping abilities can reflect the client's strategies and skills to manage their stress and emotions, but they are not a priority over the client's safety and wellbeing.
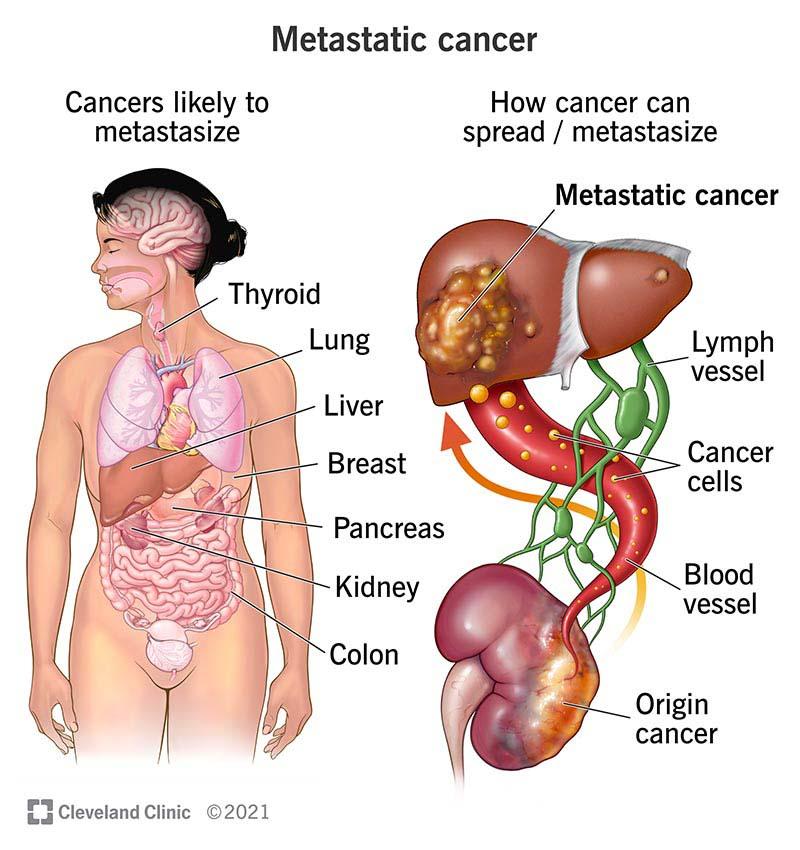
A nurse is assisting with teaching a class about medically futile treatment. The nurse should include which of the following as an example of medically futile treatment?
Explanation
Choice A reason: This statement is incorrect because administering an antiemetic to a client who has post chemotherapy nausea is not medically futile. It is a supportive measure that can help the client to manage the side effects of chemotherapy and improve their comfort and quality of life.
Choice B reason: This statement is incorrect because administering a narcotic analgesic to a client who has end stage cancer is not medically futile. It is a palliative measure that can help the client to relieve their pain and suffering and improve their comfort and quality of life.
Choice C reason: This statement is incorrect because administering oral care for a client who has post chemotherapy mucositis is not medically futile. It is a preventive measure that can help the client to avoid infections and complications and improve their oral health and hygiene.
Choice D reason: This statement is correct because administering chemotherapy to a client who has metastatic cancer is medically futile. It is a curative measure that has no reasonable chance of achieving its intended goal of eradicating the cancer or prolonging the client's survival. It may also cause harm or distress to the client by exposing them to unnecessary risks and side effects.
A nurse is assisting with teaching a class about client advocacy. The nurse should include which of the following as an example of client advocacy?
Explanation
Choice A reason: This statement is incorrect because protecting a client’s personal health information is not an example of client advocacy, but a legal and ethical obligation of the nurse. The nurse should follow the principles of confidentiality and privacy, and only share the client’s information with authorized persons or entities, or with the client’s consent.
Choice B reason: This statement is incorrect because keeping a promise to return to a client’s room is not an example of client advocacy, but a professional and courteous behavior of the nurse. The nurse should be honest, reliable, and respectful to the client, and follow through with their commitments and expectations.
Choice C reason: This statement is incorrect because accepting responsibility for their own actions is not an example of client advocacy, but a personal and professional accountability of the nurse. The nurse should be aware of their scope of practice, standards of care, and code of ethics, and act accordingly. The nurse should also admit their mistakes, report errors, and seek help when needed.
Choice D reason: This statement is correct because communicating a client’s wishes to their provider is an example of client advocacy. The nurse should act as a liaison between the client and the provider, and ensure that the client’s needs, preferences, and values are respected and considered in the decision-making process. The nurse should also support the client’s right to self-determination and informed consent.
A nurse is preparing to delegate tasks to an assistive personnel (AP). The nurse should identify which of the following as one of the five rights of delegation?
Explanation
Choice A reason: This statement is incorrect because right documentation is not one of the five rights of delegation. Right documentation is a responsibility of the nurse and the AP, but it is not a criterion for deciding what tasks to delegate and to whom. The five rights of delegation are right task, right circumstance, right person, right direction, and right supervision.
Choice B reason: This statement is correct because right communication is one of the five rights of delegation. Right communication means that the nurse provides clear, concise, and specific instructions to the AP, and that the AP acknowledges and understands the instructions. Right communication also involves feedback, reporting, and documentation between the nurse and the AP.
Choice C reason: This statement is incorrect because right time is not one of the five rights of delegation. Right time is a factor that affects the delegation process, but it is not a criterion for deciding what tasks to delegate and to whom. The five rights of delegation are right task, right circumstance, right person, right direction, and right supervision.
Choice D reason: This statement is incorrect because right room is not one of the five rights of delegation. Right room is a factor that affects the delegation process, but it is not a criterion for deciding what tasks to delegate and to whom. The five rights of delegation are right task, right circumstance, right person, right direction, and right supervision.
A charge nurse is assisting in providing an in-service to a group of nurses about the benefits of an interprofessional team. Which of the following information should the nurse include in the teaching?
Explanation
Choice A reason: This statement is incorrect because an interprofessional team does not necessarily decrease the number of visits to client by staff. In fact, an interprofessional team may increase the frequency and quality of communication and interaction between the client and the staff, as each member of the team contributes their expertise and perspective to the client's care. This can enhance the client's satisfaction, engagement, and education.
Choice B reason: This statement is correct because an interprofessional team can improve the efficiency in client care services. An interprofessional team can coordinate and integrate the care delivery across different disciplines, settings, and levels of care, reducing the duplication, fragmentation, or gaps in the services. This can also lower the costs and risks of care, and improve the outcomes and quality of care.
Choice C reason: This statement is incorrect because an interprofessional team does not increase the length of stay for client. On the contrary, an interprofessional team can reduce the length of stay for client by providing timely, appropriate, and effective care that meets the client's needs and goals. This can also prevent the readmission or complication of the client, and facilitate the transition and discharge of the client.
Choice D reason: This statement is incorrect because an interprofessional team does not decrease the number of referrals needed for client. Rather, an interprofessional team can enhance the referral process by ensuring that the client receives the right service from the right provider at the right time. An interprofessional team can also collaborate and communicate with the referral sources, and follow up on the client's progress and response to the service.
A nurse is preparing to complete an occurrence report for a client who fell at the facility. Which of the following actions should the nurse take?
Explanation
Choice A reason: This statement is correct because the nurse should use objective terminology when documenting the occurrence. Objective terminology means using factual, unbiased, and verifiable information, such as the date, time, location, witnesses, and events of the occurrence. The nurse should avoid using subjective, opinionated, or judgmental language, such as blaming, criticizing, or speculating about the occurrence.
Choice B reason: This statement is incorrect because the nurse should not wait at least 12 hours to report the occurrence. The nurse should report the occurrence as soon as possible, preferably within an hour of the incident. The nurse should also notify the appropriate personnel, such as the charge nurse, the provider, and the risk manager. Delaying the report may compromise the client's safety and wellbeing, and the accuracy and completeness of the documentation.
Choice C reason: This statement is incorrect because the nurse should not omit the name of the individuals involved in the occurrence. The nurse should include the name of the client, the staff, and any other relevant parties, such as family members or visitors. The nurse should also document the role and actions of each individual, and their response to the occurrence. Omitting the name of the individuals may affect the accountability and follow-up of the occurrence.
Choice D reason: This statement is incorrect because the nurse should not document completion of the report in the client’s medical record. The nurse should document the occurrence report separately from the client’s medical record, and follow the facility's policy and procedure for filing and storing the report. The nurse should also document the occurrence in the client’s medical record, but only the facts and the nursing actions, not the details or the existence of the report. Documenting completion of the report in the client’s medical record may expose the facility to legal liability or litigation.
A nurse in an emergency department is assisting with the care of a client who is unconscious and has trauma to multiple systems following a motor vehicle crash. Which of the following actions should the nurse take first?
Explanation
Choice A reason: This action is correct because airway protection is the first priority for a client who is unconscious and has trauma to multiple systems. The nurse should assess the client's airway patency, breathing, and oxygenation, and intervene as needed to secure and maintain the airway. The nurse should also monitor the client for signs of aspiration, bleeding, or obstruction, and suction the airway as needed.
Choice B reason: This action is incorrect because stabilizing cardiac arrhythmias is not the first priority for a client who is unconscious and has trauma to multiple systems. The nurse should assess the client's circulation, blood pressure, and pulse, and intervene as needed to treat any arrhythmias, shock, or hemorrhage. However, this is not a priority over the client's airway, which is essential for survival.
Choice C reason: This action is incorrect because preventing musculoskeletal disability is not the first priority for a client who is unconscious and has trauma to multiple systems. The nurse should assess the client's mobility, sensation, and alignment, and intervene as needed to prevent or treat any fractures, dislocations, or nerve injuries. However, this is not a priority over the client's airway, which is essential for survival.
Choice D reason: This action is incorrect because decreasing intracranial pressure is not the first priority for a client who is unconscious and has trauma to multiple systems. The nurse should assess the client's level of consciousness, pupillary response, and neurological status, and intervene as needed to prevent or treat any increased intracranial pressure, cerebral edema, or brain injury. However, this is not a priority over the client's airway, which is essential for survival.
A nurse is working with an RN to admit a new client. Which of the following steps of the nursing process is the nurse using when assisting to formulate goals for a positive outcome?
Explanation
Choice A reason: This statement is correct because planning is the step of the nursing process that involves formulating goals and outcomes for a positive outcome. The nurse and the RN should collaborate with the client and other members of the healthcare team to identify the client's needs, priorities, and preferences, and develop a plan of care that is realistic, measurable, and client centered.
Choice B reason: This statement is incorrect because evaluation is the step of the nursing process that involves measuring the effectiveness of the plan of care and the achievement of the goals and outcomes. The nurse and the RN should compare the actual results with the expected results, and determine if the plan of care needs to be modified, continued, or terminated.
Choice C reason: This statement is incorrect because data collection is the step of the nursing process that involves gathering information about the client's health status, history, and environment. The nurse and the RN should use various sources and methods of data collection, such as interviewing, observing, examining, and reviewing records, and organize and document the data in a systematic and accurate way.
Choice D reason: This statement is incorrect because implementation is the step of the nursing process that involves carrying out the plan of care and providing the interventions. The nurse and the RN should perform the actions that are necessary to achieve the goals and outcomes, such as administering medications, providing education, or coordinating referrals, and document the interventions and the client's response.
A nurse is teaching a client about the benefits of an electronic health record. Which of the following information should the nurse include in the teaching?
Explanation
Choice A: This is the correct answer. An electronic health record (EHR) is a digital version of a client's medical history and other health information that can be accessed by authorized providers and the client. A personal health record (PHR) is a subset of an EHR that allows the client to view and manage their own health information, such as medications, allergies, test results, and appointments. A PHR can enhance the client's satisfaction, engagement, and empowerment in their health care.
Choice B: This is incorrect. Provides providers client information to track for research studies is not a benefit of an electronic health record, but a potential use of it. EHRs can facilitate health research by providing large and diverse data sets that can be analyzed for various purposes, such as clinical trials, epidemiology, and quality improvement. However, this use of EHRs must comply with ethical and legal standards, such as informed consent, privacy, and confidentiality.
Choice C: This is incorrect. Grants significant other access to client information is not a benefit of an electronic health record, but a matter of the client's preference and consent. EHRs must protect the client's privacy and confidentiality rights, and only disclose their information to authorized parties, such as health care providers, insurers, or public health agencies. The client can choose to share their information with their significant other or anyone else, but they must give explicit permission to do so.
Choice D: This is incorrect. Coordinates all healthcare client has received into one platform is not a benefit of an electronic health record, but a goal of it. EHRs aim to improve the coordination and continuity of care by allowing multiple providers to access and update the same information, enabling real-time collaboration, and providing decision support tools. However, this goal is not fully achieved yet, as there are still challenges and barriers to the interoperability and integration of EHRs across different settings and systems.
A nurse is collecting data on a client who has had diarrhea for several days. Which of the following findings should the nurse expect?
Explanation
Choice A reason: This statement is incorrect because a rigid abdomen is not a common finding for a client who has had diarrhea for several days. A rigid abdomen may indicate peritonitis, which is an inflammation of the abdominal lining, usually caused by an infection or a perforation of an organ. A client with peritonitis may also have severe abdominal pain, fever, nausea, and vomiting.
Choice B reason: This statement is correct because dehydration is a common finding for a client who has had diarrhea for several days. Dehydration occurs when the body loses more fluid than it takes in, which can happen with frequent and watery stools. A client with dehydration may also have dry mouth, thirst, decreased urine output, dark urine, low blood pressure, increased heart rate, and confusion.
Choice C reason: This statement is incorrect because hypothermia is not a common finding for a client who has had diarrhea for several days. Hypothermia occurs when the body temperature drops below 35°C (95°F), usually due to exposure to cold environments or inadequate clothing. A client with hypothermia may also have shivering, slow breathing, slow pulse, drowsiness, and loss of consciousness.
Choice D reason: This statement is incorrect because decreased bowel sounds are not a common finding for a client who has had diarrhea for several days. Decreased bowel sounds may indicate ileus, which is a temporary paralysis of the intestinal movement, usually caused by surgery, medication, or inflammation. A client with ileus may also have abdominal distension, constipation, nausea, and vomiting.
A nurse is assisting with discharge planning for a client who has a sacral pressure injury and has a prescription for daily dressing changes. Which of the following resource referrals should the nurse anticipate from the provider for this client?
Explanation
Choice A reason: Home care is the most appropriate resource referral for this client, as they will need skilled nursing care to perform wound care and monitor the healing process. Home care can also provide education and support for the client and their family.
Choice B reason: Assisted living is not a suitable resource referral for this client, as they do not provide skilled nursing care or wound care. Assisted living facilities are designed for clients who need assistance with activities of daily living, but not medical care.
Choice C reason: Long-term care is not a necessary resource referral for this client, as they do not have a chronic or terminal condition that requires 24hour nursing care. Long-term care facilities are intended for clients who are unable to live independently due to physical or cognitive impairments.
Choice D reason: Hospice care is not an appropriate resource referral for this client, as they do not have a terminal illness or a life expectancy of less than six months. Hospice care provides palliative care and comfort measures for clients who are dying and their families.
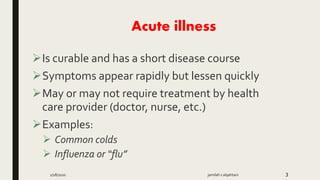
A nurse is caring for a client who reports sneezing, productive cough, muscle aches, headache, and fever that has progressed over the last 4 days. Which of the following stages of infection is the client likely experiencing?
Explanation
Choice A reason: The prodromal stage is the period between the exposure to the infectious agent and the onset of specific symptoms. During this stage, the person may experience mild and nonspecific signs of infection, such as fatigue or lowgrade fever. The client in the question has already developed specific symptoms of infection, such as sneezing, productive cough, and fever, which indicate that they have passed the prodromal stage.
Choice B reason: The period of convalescence is the stage of recovery after the infection. During this stage, the person's symptoms gradually subside, and their immune system eliminates the infectious agent from the body. The client in the question is still experiencing symptoms of infection, which suggest that they have not reached the period of convalescence yet.
Choice C reason: The acute illness stage is the peak of the infection, when the person exhibits the most severe and specific symptoms of the disease. During this stage, the person's immune system fights against the infectious agent, and the outcome of the infection is determined. The client in the question is likely in the acute illness stage, as they have been experiencing symptoms of infection for 4 days, and their condition has worsened over time.
Choice D reason: The incubation stage is the time between the entry of the infectious agent into the body and the appearance of the first symptoms of infection. During this stage, the person does not feel ill, but the infectious agent is multiplying in the body. The client in the question has already developed symptoms of infection, which indicate that they have left the incubation stage.
A nurse is reinforcing information with a nursing colleague about sentinel events. Which of the following statements by the nursing colleague indicates an understanding?
Explanation
Choice A reason: A sentinel event is a serious adverse event that results in death, permanent harm, or severe temporary harm to a patient. Administering incompatible blood products to a client is a sentinel event because it can cause fatal hemolytic reactions.
Choice B reason: Administering client medications 30 minutes late is not a sentinel event, unless it leads to a serious adverse outcome for the patient. Medication errors are common and preventable, and they should be reported and analyzed to improve patient safety.
Choice C reason: Documenting vital signs at the wrong time in the client’s electronic health record is not a sentinel event, unless it leads to a serious adverse outcome for the patient. Documentation errors are also common and preventable, and they should be corrected and avoided to ensure accurate and timely information.
Choice D reason: Administering a prescribed sedative to a client for insomnia is not a sentinel event, unless it leads to a serious adverse outcome for the patient. Sedatives are commonly used to treat insomnia, and they should be prescribed and administered with caution and monitoring⁵.
A nurse is instructing a newly licensed nurse about the scope and standards of nursing practice. Which of the following describes standards of practice?
Explanation
Choice A reason: Providing competencies for the nurses to achieve before licensure is not a description of standards of practice, but rather a function of the nursing education and accreditation system. Standards of practice are authoritative statements that define the expected level of performance for nurses after they obtain their license.
Choice B reason: Establishing a protocol for care to provide for a specific health problem is not a description of standards of practice, but rather a function of the clinical practice guidelines and evidence based practice. Standards of practice are broader and more general statements that apply to all nurses regardless of their specialty or setting.
Choice C reason: Specifying that nurses provide care that reflects current and competent level of behavior when providing client care is a description of standards of practice, as it captures the essence of what standards of practice are and why they are important. Standards of practice are based on the best available evidence and professional consensus, and they guide nurses in delivering safe, quality, and ethical care to their clients.
Choice D reason: Listing a set of skills that all nurses should be competent in performing, outlining responsibilities that every nurse is expected to provide regardless of their role is not a description of standards of practice, but rather a function of the scope of practice. Scope of practice describes the services that a qualified health professional is deemed competent to perform, and permitted to undertake, in keeping with the terms of their professional license..
A nurse is reinforcing teaching with a client who has a terminal illness and is considering palliative care services. Which of the following statements by the client indicates an understanding?
Explanation
Choice A reason: This statement indicates an understanding of palliative care services, as they aim to improve the quality of life of people with serious or life altering illnesses by providing symptom relief, emotional support, and spiritual care.
Choice B reason: This statement does not indicate an understanding of palliative care services, as they do not directly provide respite care for caregivers. However, palliative care services may help caregivers cope with the stress and burden of caring for a terminally ill person, and may refer them to other resources that can offer respite care.
Choice C reason: This statement does not indicate an understanding of palliative care services, as they do not require the person to go to a skilled facility. Palliative care services can be provided in various settings, such as hospitals, nursing homes, outpatient clinics, or at home.
Choice D reason: This statement does not indicate an understanding of palliative care services, as they do not provide meal management for the person. However, palliative care services may include nutritionists who can offer dietary advice and guidance for the person, and may coordinate with other services that can help with meal preparation and delivery.
A nurse is discussing informatics with a newly licensed nurse. The nurse identifies that informatics is defined as the use of information and technology for which of the following?
Explanation
Choice A reason: Managing knowledge is one of the goals of informatics, as it involves collecting, organizing, analyzing, and sharing data, information, and wisdom in nursing practice.
Choice B reason: Producing clinical pathways is not a definition of informatics, but rather an application of informatics. Clinical pathways are evidence based tools that guide the care of specific patient populations. Informatics can help create, implement, and evaluate clinical pathways.
Choice C reason: Providing a safe place to provide care is not a definition of informatics, but rather an outcome of informatics. Informatics can enhance patient safety by improving communication, documentation, decision support, and error prevention.
Choice D reason: Preventing burnout is not a definition of informatics, but rather a benefit of informatics. Informatics can reduce burnout by streamlining workflows, reducing cognitive load, and increasing satisfaction.
A nurse is assisting with preparing an educational session at a community health center about the social determinants of health (SDOH). Which of the following information should the nurse include?
Explanation
Choice A reason: This statement is true and should be included in the educational session. SDOH are the nonmedical factors that influence health outcomes, such as income, education, housing, food security, social inclusion, and access to health services. SDOH can affect a person's physical, mental, and social wellbeing, as well as their risk of developing certain diseases.
Choice B reason: This statement is false and should not be included in the educational session. SDOH are not determined by an individual’s ethnic background, but rather by the broader social, economic, and political context in which they live. However, ethnic background can influence how a person experiences SDOH, as some ethnic groups may face discrimination, racism, and marginalization that affect their access to resources and opportunities.
Choice C reason: This statement is false and should not be included in the educational session. Identifying SDOH does not increase disparities in health care, but rather helps to address them. Disparities in health care are the differences in the quality and accessibility of health services among different populations⁵. Identifying SDOH can help to understand the root causes of these disparities, and to design interventions that target the most vulnerable and disadvantaged groups.
Choice D reason: This statement is false and should not be included in the educational session. SDOH do not include psychological factors, but rather affect them. Psychological factors are the individual characteristics and behaviors that influence a person's mental health and wellbeing, such as personality, coping skills, self-esteem, and stress management. SDOH can influence psychological factors by creating stressful or supportive environments, and by facilitating or hindering access to mental health services.
A nurse is providing a handoff report using the introduction, situation, background, assessment, recommendation, and readback (ISBARR) on a client. Which of the following information should be included in the situation component?
Explanation
Choice A reason: This statement belongs to the recommendation component, as it describes an action that the nurse has taken or suggests to take regarding the client's care.
Choice B reason: This statement also belongs to the recommendation component, as it expresses a need or a request for the client's treatment.
Choice C reason: This statement belongs to the situation component, as it summarizes the current problem or issue that the client is facing.
Choice D reason: This statement belongs to the background component, as it provides relevant information about the client's medical history or diagnosis.
A nurse is discussing time management strategies with another nurse. The nurse should include which of the following as an example of a time management strategy?
Explanation
Choice A reason: Planning time for disruptions is a time management strategy, as it allows the nurse to anticipate and cope with unexpected events that may interfere with their schedule. By allocating some buffer time for potential delays, emergencies, or interruptions, the nurse can avoid stress and maintain their productivity.
Choice B reason: Offering to complete another nurse’s task is not a time management strategy, but rather a sign of poor boundary setting. While helping others is commendable, the nurse should not take on more responsibilities than they can handle, as this may compromise their own work quality and wellbeing. The nurse should learn to say no politely and focus on their own priorities.
Choice C reason: Skipping a meal break to catch up on charting is not a time management strategy, but rather a counterproductive habit. Taking regular breaks is essential for the nurse to replenish their energy, reduce fatigue, and prevent burnout. Skipping breaks may impair the nurse’s concentration, memory, and decision-making, and increase the risk of errors.
Choice D reason: Completing the easiest tasks first is not a time management strategy, but rather a form of procrastination. The nurse should prioritize their tasks based on their importance and urgency, not their difficulty or preference. Completing the easiest tasks first may create a false sense of accomplishment, while leaving the most critical or challenging tasks for later, when the nurse may have less time or motivation.
A nurse is caring for a client who acquired hepatitis A from consuming contaminated food. The client’s mouth is an example of which of the following links in the chain of infection?
Explanation
Choice A reason: The reservoir is the environment or habitat where the infectious agent lives and multiplies. The client's mouth is not a reservoir, but rather a part of the susceptible host. The reservoir for hepatitis A is usually the feces of an infected person.
Choice B reason: The susceptible host is the person who is at risk of getting the infection. The client's mouth is not a susceptible host, but rather a part of the susceptible host. The susceptibility to hepatitis A depends on factors such as age, immunity, hygiene, and exposure.
Choice C reason: The portal of entry is the opening or route through which the infectious agent enters the susceptible host. The client's mouth is a portal of entry, as it is where the contaminated food entered the client's body and caused the infection. Hepatitis A is transmitted through the fecaloral route, meaning that the virus is ingested from contact with objects, food, or water contaminated by the feces of an infected person.
Choice D reason: The infectious agent is the microorganism that causes the infection. The client's mouth is not an infectious agent, but rather a portal of entry for the infectious agent. The infectious agent for hepatitis A is a virus that affects the liver and causes inflammation, jaundice, and fever.
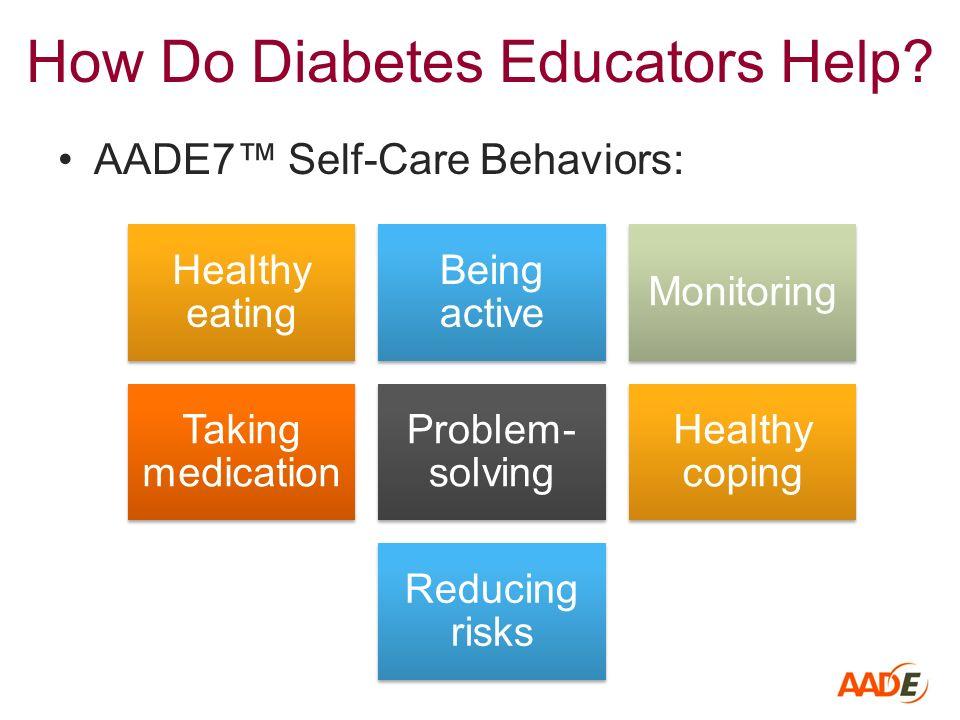
A nurse is reinforcing teaching with a client who has been newly diagnosed with diabetes mellitus. Which of the following information demonstrates health literacy by the client?
Explanation
Choice A reason: This statement does not demonstrate health literacy by the client, but rather a need for more health education. Health literacy is the ability to obtain, process, and understand basic health information and services needed to make appropriate health decisions. Requesting further information to improve their health indicates that the client may lack some knowledge or skills related to their condition.
Choice B reason: This statement demonstrates health literacy by the client, as it shows that they have learned and applied an important selfcare behavior for diabetes management. Taking blood glucose daily is a way to monitor and control blood sugar levels, which can prevent or delay complications of diabetes.
Choice C reason: This statement does not demonstrate health literacy by the client, but rather a need for more communication with their provider. Health literacy is not only about acquiring information, but also about using it effectively to make informed decisions. Asking to speak with their provider suggests that the client may have some questions or concerns that need to be addressed.
Choice D reason: This statement does not demonstrate health literacy by the client, but rather a need for more nutritional guidance. Health literacy is not only about understanding information, but also about acting on it to improve health outcomes. Requesting to speak with a nutritionist implies that the client may need some assistance with planning and following a healthy diet for diabetes.
Sign Up or Login to view all the 59 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
