Ati Maternal newborn 2020 with NGN
Total Questions : 59
Showing 25 questions, Sign in for moreA nurse in a prenatal clinic is reinforcing teaching with a client about expected physiological changes during pregnancy. Which of the following statements by the client indicates an understanding of the teaching?
Explanation
The correct answer is d. "I may develop discoloration on my cheeks from hormonal changes."
Choice a rationale:
- Statement:"I should expect to have burning when I urinate during the third trimester."
- Rationale:This statement is incorrect.Burning during urination is not a normal physiological change of pregnancy.It may be a sign of a urinary tract infection (UTI),which is a common infection during pregnancy.If a pregnant client experiences burning during urination,she should report it to her healthcare provider for evaluation and treatment.
Choice b rationale:
- Statement:"I may have an infection if I develop a dark line in the middle of my abdomen."
- Rationale:This statement is incorrect.A dark line in the middle of the abdomen,known as the linea nigra,is a normal physiological change of pregnancy.It is caused by hormonal changes that increase melanin production in the skin.The linea nigra typically appears in the second trimester and fades after delivery.
Choice c rationale:
- Statement:"I should expect my fingers and face to be swollen."
- Rationale:This statement is partially correct.Some swelling in the hands and face is common during pregnancy,especially in the third trimester.This is due to fluid retention caused by hormonal changes.However,excessive swelling,particularly in the hands and face,can be a sign of preeclampsia,a serious pregnancy complication.It's important to report any significant swelling to a healthcare provider.
Choice d rationale:
- Statement:"I may develop discoloration on my cheeks from hormonal changes."
- Rationale:This statement is correct.Hormonal changes during pregnancy can cause a variety of skin changes,including melasma,which is a brownish discoloration that often appears on the cheeks,forehead,and nose.Melasma is more common in women with darker skin tones and usually fades after delivery.
A nurse in a provider's office is collecting data from a client who is requesting a prescription for a transdermal contraceptive patch. The nurse should recognize which of the following client findings is a contraindication for this method of contraception.
Explanation
Rationale:
A) Incorrect - A blood pressure of 120/70 mm Hg is within the normal range and is not a contraindication for the transdermal contraceptive patch.
B) Incorrect - Peptic ulcer disease is not a contraindication for the transdermal contraceptive patch.
C) Correct - A weight of 98 kg (216 lb) is considered a contraindication for the transdermal contraceptive patch due to potential reduced efficacy in women with a body mass index (BMI) over 30. This method might be less effective for individuals with higher body weights.
D) Incorrect - A history of spontaneous abortion is not a contraindication for the transdermal contraceptive patch.
A nurse is auscultating fetal heart tones with a Doppler device for a client who is at 12 weeks of gestation. Where should the nurse expect to auscultate the fetal heart tones?
Explanation
Rationale:
A) Incorrect - The umbilical area is not a typical location for auscultating fetal heart tones.
B) Incorrect - The suprapubic area is not a common location for auscultating fetal heart tones.
C) Correct - At 12 weeks of gestation, the nurse would typically auscultate the fetal heart tones above the left iliac crest, which is in the lower abdomen. This is where the uterus is located at this stage of pregnancy.
D) Incorrect - Auscultating below the liver border on the right abdomen is not a standard practice for fetal heart tone assessment.
A nurse is caring for a client who is postpartum. The client is experiencing excessive vaginal bleeding and has a boggy uterus. Which of the following actions should the nurse take first?
Explanation
Rationale:
A) Incorrect - Applying oxygen is not the priority action in the case of excessive vaginal bleeding and a boggy uterus. Oxygen therapy would be appropriate if there were signs of respiratory distress or decreased oxygen saturation, but it does not directly address the primary concern of uterine atony and bleeding.
B) Incorrect - Administering methylergonovine might be appropriate, but the priority is to address the uterine atony with fundal massage first. Fundal massage helps stimulate uterine contractions and control bleeding, which is crucial in this scenario.
C) Incorrect - Encouraging the client to empty her bladder is important, but it is not the first action to take in the case of excessive bleeding and uterine atony. Immediate intervention to control the bleeding takes precedence.
D) Correct - Initiating fundal massage is the priority action in this situation. A boggy uterus with excessive vaginal bleeding indicates uterine atony, which is a potentially life-threatening condition requiring immediate intervention to prevent further bleeding.
Fundal massage helps the uterus contract and control bleeding. Addressing uterine atony is critical to prevent further hemorrhage and stabilize the client's condition.

A nurse is reinforcing teaching about perineal care to a client who is 2 hr postpartum and has an episiotomy and hemorrhoids. Which of the following statements by the client indicates an understanding of the teaching?
Explanation
A) Incorrect- Applying a heat pack to the area might increase inflammation and discomfort. Heat is generally not recommended for healing episiotomies and hemorrhoids.
B) Correct - "I will apply witch hazel pads after urination" is the correct statement. Witch hazel pads have a cooling and soothing effect that can provide relief from discomfort associated with episiotomies and hemorrhoids.
C) Incorrect- Using a numbing spray before cleansing might not be necessary and could interfere with proper cleansing. It's generally recommended to cleanse the area before applying any products.
D) Incorrect- Remaining in a sitz bath for 10 minutes is beneficial for perineal care, but it doesn't specifically address the use of witch hazel pads or understanding of the overall perineal care regimen. Furthermore, prolonged sitz baths, as can interfere with healing and increase the risk of infection.
A nurse is collecting data from a client at a 6-week postpartum checkup. The client tells the nurse, "I am breastfeeding and would like to use a birth control pill." Which of the following statements should the nurse make?
Explanation
A) Correct - "Progestin-only birth control pills are preferred for contraception during lactation." Progestin-only pills are generally considered safer for breastfeeding mothers as they are less likely to affect milk supply.
B) Incorrect- There is no strong evidence suggesting that taking birth control pills while breastfeeding increases the risk of breast cancer.
C) Incorrect- While breastfeeding can have contraceptive effects, relying solely on breastfeeding for contraception is not a foolproof method. It's recommended to use additional birth control methods if desired.
D) Incorrect- Birth control pills are not contraindicated for breastfeeding clients, especially if they are progestin-only pills. The preferred method, however, is progestin-only rather than combined hormonal pills.
A nurse is reinforcing teaching with a client about how to minimize nausea in the first trimester of pregnancy. Which of the following instructions should the nurse give to the client?
Explanation
A) Incorrect- Having a high-fat snack before bed might exacerbate nausea. It's generally recommended to have a light snack if needed.
B) Incorrect- Eating small, frequent snacks between meals can help manage nausea by preventing an empty stomach.
C) Incorrect- Drinking water with meals might not necessarily help with nausea and might worsen the feeling of fullness.
D) Correct - "Eat a slice of dry toast before getting out of bed" can help alleviate morning sickness in the first trimester. Eating a small, bland snack before rising can prevent an empty stomach, which can contribute to nausea.
A nurse is caring for a client who has hyperemesis gravidarum. The nurse should identify that the client is at risk for which of the following conditions?
Explanation
A) Incorrect- Elevated blood pressure is not a primary risk associated with hyperemesis gravidarum.
B) Incorrect- Leukopenia (low white blood cell count) is not a common consequence of hyperemesis gravidarum.
C) Correct - Hyperemesis gravidarum, severe nausea, and vomiting during pregnancy can lead to dehydration, which may affect amniotic fluid levels and result in hydramnios (excessive amniotic fluid).
D) Incorrect- Ketonuria (presence of ketones in the urine) is a possible consequence of excessive vomiting, but it's not the primary concern associated with hyperemesis gravidarum.
A nurse is caring for a client who is at 34 weeks of gestation and is preparing to undergo a nonstress test. Which of the following actions should the nurse take?
Explanation
A) Incorrect- Oxytocin is not typically administered during a nonstress test.
B) Incorrect- A nonstress test is used to assess fetal well-being and does not indicate Down syndrome.
C) Correct - A lateral tilt position (usually left lateral tilt) is recommended during a nonstress test to prevent compression of the vena cava and maintain proper blood flow to the uterus, which can optimize fetal heart rate monitoring.
D) Incorrect- NPO status is not typically required for a nonstress test. Nonstress tests are non-invasive and do not involve fasting.

A nurse is collecting data from a newborn who was born 2 hr ago. Which of the following findings should the nurse report to the provider?
Explanation
A) Incorrect- Overlapping suture lines in a newborn are common and usually resolve as the baby grows. This finding is not typically concerning.
B) Incorrect- Acrocyanosis, bluish discoloration of the hands and feet, is common in newborns and is a normal physiological response to adjusting to the outside environment.
C) Incorrect- Hypotonia, or decreased muscle tone, can be present in newborns and may improve over time. It's important to monitor but may not necessarily require immediate reporting.
D) Correct - A blood glucose level of 40 mg/dL in a newborn is considered low and requires intervention. Hypoglycemia in a newborn can have serious consequences and should be promptly addressed.
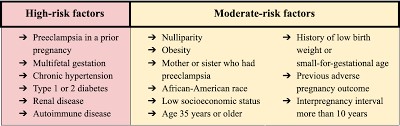
A nurse is reinforcing teaching about risk factors for preeclampsia with a group of clients who are pregnant. Which of the following risk factors should the nurse include in the teaching?
Explanation
A) Correct - Chronic hypertension is a significant risk factor for developing preeclampsia during pregnancy. Preeclampsia is characterized by high blood pressure and organ damage, typically occurring after 20 weeks of pregnancy.
B) Incorrect- Maternal age of 30 years is not a specific risk factor for preeclampsia.
However, maternal age over 40 is considered a risk factor.
C) Incorrect- A prepregnancy BMI of 19 falls within the healthy weight range and is not typically associated with an increased risk of preeclampsia.
D) Incorrect- Having a third pregnancy is not inherently a strong risk factor for preeclampsia. Women experiencing their first pregnancy are at a slightly higher risk.
A nurse is caring for a client who is postpartum and experiencing excessive vaginal bleeding. Which of the following medications should the nurse plan to administer?
Explanation
A) Incorrect- Nifedipine is a calcium channel blocker used for conditions like high blood pressure, not for controlling postpartum bleeding.
B) Incorrect- Terbutaline is a bronchodilator and is not typically used for postpartum bleeding.
C) Correct - Oxytocin is a uterotonic medication often used to control excessive bleeding after childbirth. It helps the uterus contract and reduces the risk of postpartum hemorrhage.
D) Incorrect- Betamethasone is a corticosteroid used to enhance fetal lung maturity when given to pregnant clients at risk of preterm birth

A nurse is reinforcing teaching about laboratory testing with a client who is at 6 weeks of gestation. Which of the following statements should the nurse include?
Explanation
A) Correct - Group B streptococcus (GBS) screening is typically performed around 36 weeks of gestation to identify colonization. It helps determine whether antibiotic prophylaxis is necessary during labor to prevent transmission to the newborn.
B) Incorrect- Producing a clean catch urine specimen every 2 months is not a standard recommendation during pregnancy. Urine testing is common but does not usually occur this frequently.
C) Incorrect- Maternal serum alpha-fetoprotein screening is typically done around 15-20 weeks of gestation, not 6 weeks.
D) Incorrect- Screening for gestational diabetes typically occurs between 24 and 28 weeks of gestation, not 12 weeks.
A nurse is collecting data from a client who is receiving epidural anesthesia. Which of the following findings indicates an adverse effect of this method of pain management?
Explanation
A) Incorrect- Tachycardia (elevated heart rate) can be a common physiological response to pain or other factors and is not necessarily indicative of an adverse effect of epidural anesthesia.
B) Incorrect- Fever might be related to various factors, including infection, and is not directly indicative of an adverse effect of epidural anesthesia.
C) Correct - Tachypnea (rapid breathing) can be an adverse effect of epidural anesthesia.
It can indicate that the anesthesia has spread too high in the spinal column, potentially affecting the respiratory muscles and causing respiratory distress.
D) Incorrect- Hypertension might be a side effect of epidural anesthesia, but tachypnea is a more specific indication of an adverse effect in this context.
A nurse in a clinic is reinforcing teaching about signs of effective breastfeeding with a client who has a 5-day-old newborn. Which of the following statements by the client demonstrates an understanding of the teaching?
Explanation
A) Correct- Feeling the baby's swallowing during breastfeeding indicates that the baby is effectively transferring milk from the breast. It suggests that the baby is latched on correctly and is receiving milk.
B) Incorrect- Moderate tenderness during breastfeeding is common initially, but it should not be persistent or severe.
C) Incorrect- While bowel movements are important, having at least one bowel movement every day is not necessarily an indicator of effective breastfeeding.
D) Incorrect- While wet diapers are important to ensure adequate hydration, having at least six wet diapers every day is not the primary sign of effective breastfeeding.
A nurse is caring for a client who had a vaginal delivery 1 day ago. The nurse determines that the client's fundus is firm, located 2 fingerbreadths above the umbilicus, and deviated to the left. Which of the following actions should the nurse take first?
Explanation
A) Incorrect- While notifying the provider might be necessary, addressing bladder distention takes precedence in this scenario.
B) Incorrect- Administering an analgesic might be indicated for pain relief, but addressing bladder distention is the priority.
C) Correct - Assisting the client to empty her bladder is the first action to take. A full bladder can prevent the uterus from contracting properly and can lead to excessive bleeding.
D) Incorrect- Monitoring perineal pads for clots is important but not the first action to take when bladder distention is present.
A nurse is collecting data from a newborn who is 1 hr old and was born at 43 weeks of gestation. Which of the following findings should the nurse expect? (Select all that apply.)
Explanation
A) Incorrect- Dry, cracked skin is not typically associated with a newborn born at 43 weeks of gestation. It's more common in post-term babies.
B) Correct - Hypotonia (low muscle tone) is a possible finding in post-term newborns due to the aging placenta and potential decrease in amniotic fluid.
C) Correct - Excessive lanugo (fine, downy hair) is more likely to be present in post-term babies as they have less vernix to protect their skin.
D) Incorrect- Absent vernix might be more characteristic of a post-term newborn, but its presence or absence varies widely.
E) Correct - Long, hard nails can be a characteristic of post-term babies, as they have had more time for nail growth in the womb.
A nurse is reinforcing teaching about home safety precautions with the guardian of a newborn. Which of the following instructions should the nurse include?
Explanation
A) Incorrect- The water heater temperature should be set to 49.4°C (120°F) or below to prevent scalding. The given temperature is slightly too high.
B) Incorrect- Soft bumper pads in cribs can pose a suffocation risk and are not recommended.
C) Correct - Washing the newborn's face with a warm, soapy washcloth is a safe way to cleanse the baby's face. Harsh chemicals or strong soaps should be avoided.
D) Incorrect- Pillows should not be placed under a newborn's head during naps to reduce the risk of suffocation. The baby's sleep environment should be free of soft bedding.
A nurse is assisting with a prenatal class discussion about newborn safety. Which of the following statements by a participant indicates an understanding of the teaching?
Explanation
A) Incorrect- Elevating a baby's head with a cushion during sleep is not recommended, as it can increase the risk of sudden infant death syndrome (SIDS) and obstructed breathing.
B) Correct - "I should replace the batteries in my smoke detector twice per year." Regularly replacing smoke detector batteries helps ensure they function properly in case of a fire emergency.
C) Incorrect- Setting the hot water heater to 130°F (54.4°C) is too hot and can cause scalding burns. The recommended temperature is 120°F (48.9°C) or lower.
D) Incorrect- Baby powder is not recommended for use with diaper changes, as it can be inhaled by the baby and lead to respiratory issues.
A home health nurse is caring for a client who has unilateral mastitis and is experiencing discomfort in the affected breast. Which of the following Instructions should the nurse include?
Explanation
A) Incorrect- Hydrocortisone ointment is not typically recommended for treating mastitis, as it might not address the underlying infection.
B) Incorrect- Wearing a well-fitting, supportive nursing bra can actually help alleviate discomfort and is not typically contraindicated in cases of mastitis.
C) Correct - Applying warm compresses to the affected breast can help reduce pain and discomfort associated with mastitis. Warmth can improve blood flow and promote milk flow.
D) Incorrect- Encouraging the client to limit oral fluid intake to decrease milk production is not a recommended approach, as maintaining proper hydration is important, especially when dealing with infection.

A nurse is assisting in the care of a client who is in labor and whose membranes ruptured 6 hr ago. Which of the following is an appropriate nursing intervention for this client?
Explanation
A) Correct - Monitoring for infection is an appropriate nursing intervention for a client whose membranes have ruptured, as there is an increased risk of infection after the amniotic sac has ruptured for an extended period.
B) Incorrect- Positioning the client supine is not generally recommended for a client in labor, especially if the client's membranes have ruptured.
C) Incorrect- Obtaining consent for a cesarean birth is not indicated solely based on the information provided.
D) Incorrect- Preparing for a forceps delivery is not indicated solely based on the information provided.
A nurse is caring for a newborn whose mother has gestational diabetes. The newborn has a blood glucose level of 30 mg/dL and is asymptomatic. Which of the following actions should the nurse take?
Explanation
A) Incorrect- Checking urine for ketones is not necessary if the newborn's blood glucose level is low but stable and the baby is asymptomatic.
B) Incorrect- Administering glucagon is not indicated for an asymptomatic newborn with a low but stable blood glucose level.
C) Correct - Encouraging additional feeding is appropriate for an asymptomatic newborn with a low blood glucose level. Regular feeding can help increase blood glucose levels.
D) Incorrect- Waiting 4 hours to recheck blood glucose might not be appropriate if the baby's blood glucose is currently low. Addressing the low blood glucose level is more immediate.
A nurse is collecting data from a client who is receiving terbutaline to treat preterm labor.
Which of the following findings should the nurse report to the provider?
Explanation
A) Correct - Reporting crackles is important because they can indicate fluid retention in the lungs, which can be a serious adverse effect of terbutaline.
B) Incorrect- Dizziness is a common side effect of terbutaline and might not warrant immediate reporting unless severe.
C) Incorrect- Nausea is a common side effect of terbutaline and might not warrant immediate reporting unless severe.
D) Incorrect- Tremors are a common side effect of terbutaline and might not warrant immediate reporting unless severe.
A nurse in a prenatal clinic is reinforcing teaching with a client who is at 20 weeks of gestation and has a low calcium level. Which of the following foods should the nurse recommend the client increase in her diet?
Explanation
A) Correct - Yogurt is a good source of calcium and is a suitable recommendation for a client with low calcium levels during pregnancy.
B) Incorrect- Avocados contain healthy fats and other nutrients, but they are not a particularly high source of calcium.
C) Incorrect- Peanut butter is a source of protein and healthy fats but does not provide a significant amount of calcium.
D) Incorrect- Long-grain rice is a carbohydrate source but does not contribute much to calcium intake.
A nurse is collecting data from a term newborn who is 12 hr old. Which of the following findings should the nurse report to the provider?
Explanation
A) Incorrect- Abdominal breathing is a normal pattern in newborns and does not require immediate reporting.
B) Correct - Grunting is a sign of respiratory distress in a newborn and should be reported to the provider for further evaluation.
C) Incorrect- A respiratory rate of 55/min is within the normal range for a newborn and does not require immediate reporting.
D) Incorrect- Irregular respirations are common in newborns and may not necessarily be indicative of a problem.
Sign Up or Login to view all the 59 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
