Ati maternal newborn final exam
Total Questions : 89
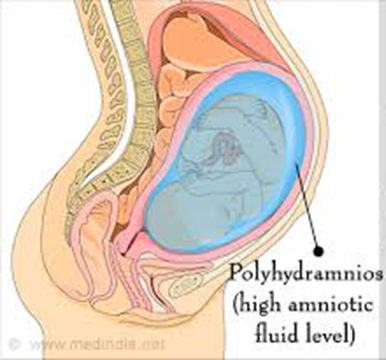
Showing 25 questions, Sign in for moreA nurse is caring for a client who was admitted to the maternity unit at 38 weeks of pregnancy and is experiencing polyhydramnios. The nurse should recognize that this diagnosis indicates which of the following?
Explanation
Choice A reason:
While polyhydramnios can be associated with congenital anomalies or fetal distress, it is not a direct indication of these conditions. Polyhydramnios refers specifically to the excessive accumulation of amniotic fluid. Congenital anomalies may lead to polyhydramnios if they affect the fetus's ability to swallow and process amniotic fluid normally, but the presence of polyhydramnios alone does not confirm these conditions.
Choice B reason:
Elevated levels of alpha-fetoprotein (AFP) in the amniotic fluid can be indicative of neural tube defects or other fetal abnormalities, but they are not a defining characteristic of polyhydramnios. Normal AFP levels in amniotic fluid at 15 to 21 weeks' gestation range from 10 to 150 ng/ml. Polyhydramnios is diagnosed based on the volume of amniotic fluid, not the AFP levels.
Choice C reason:
Carrying more than one fetus can lead to an increased amount of amniotic fluid, potentially resulting in polyhydramnios. However, the diagnosis of polyhydramnios itself does not imply a multiple gestation pregnancy. It simply indicates that there is more amniotic fluid than usual.
Choice D reason:
Polyhydramnios is defined as an excessive amount of amniotic fluid. It is typically diagnosed when the amniotic fluid index (AFI) exceeds 24 cm or the single deepest pocket (SDP) measures more than 8 cm. This condition can occur due to various reasons, including fetal anomalies, maternal diabetes, and other medical conditions.
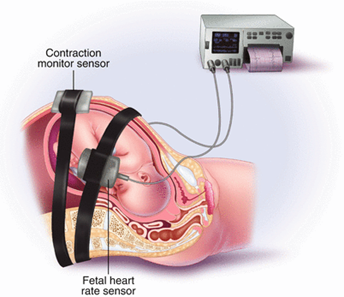
A nurse in the labor and delivery unit is caring for a client who is undergoing external fetal monitoring. The nurse notices that the fetal heart rate starts to decrease after a contraction begins, with the lowest rate occurring after the contraction's peak. What should be the nurse's first action?
Explanation
Choice A reason:
Administering oxygen using a non-rebreather mask is a subsequent step if initial measures do not improve fetal heart rate decelerations. It can help increase the amount of oxygen available to the fetus. Oxygen administration is a supportive measure that can be used if there are signs of fetal distress. In the scenario described, where the fetal heart rate slows after the start of a contraction with the lowest rate occurring after the peak, it suggests late decelerations, which are often associated with uteroplacental insufficiency. Administering oxygen can help increase the fetal oxygen reserve and is a common intervention during labor when there are concerns about fetal well-being.
Choice B reason:
Increasing the rate of maintenance IV infusion is typically considered when there is a concern for maternal hypotension or dehydration, which may not be the immediate cause of the observed fetal heart rate pattern. Increasing the rate of an IV infusion can help improve maternal hydration and blood pressure, which in turn can enhance placental perfusion. However, this intervention is more indirect and may not provide the immediate response needed to address fetal heart rate decelerations. It is typically considered after more direct interventions, such as repositioning the mother, have been attempted.
Choice C reason:
Elevating the client's legs can help improve venous return to the heart, potentially increasing maternal cardiac output and blood flow to the placenta. While this can be beneficial, it is not the primary intervention for late decelerations. Repositioning the mother to improve uteroplacental circulation is generally the first step.
Choice D reason:
Placing the client in the lateral position is often the first action taken when late decelerations are observed. This position helps improve uteroplacental blood flow and can quickly address potential issues related to fetal oxygenation. This position helps to relieve pressure on the inferior vena cava and aorta, which can be compressed by the gravid uterus, especially in the supine position. Relieving this pressure helps to improve uteroplacental circulation and can quickly address the cause of late decelerations, which is often related to compromised blood flow to the placenta.
A nurse is caring for a client with severe preeclampsia who is receiving an IV infusion of magnesium sulfate at a rate of 2 g/hr. Which of the following observations would indicate that it is safe for the nurse to continue the infusion?
Explanation
Choice A reason:
Magnesium sulfate is used in the management of severe preeclampsia primarily for seizure prophylaxis. One of the key side effects of magnesium sulfate is its impact on neuromuscular transmission, leading to diminished deep-tendon reflexes as serum magnesium levels rise. The therapeutic range for anticonvulsant prophylaxis is typically between 5-8 mg/dL. Reflexes may begin to diminish when serum levels reach 8-12 mg/dL, indicating potential magnesium toxicity. Therefore, diminished reflexes are a warning sign to reassess the infusion rate and possibly reduce or discontinue the medication.
Choice B reason:
A respiratory rate of 16 breaths per minute falls within the normal adult range and suggests that the client's respiratory system is not being adversely affected by the magnesium sulfate infusion. Respiratory rate is a critical parameter to monitor during magnesium sulfate therapy, as respiratory depression is a serious side effect of magnesium toxicity. Maintaining a normal respiratory rate indicates that it is safe to continue the infusion at the current rate.
Choice C reason:
While a urine output of 50 mL/hr is on the lower end of the normal range, it is still considered adequate for most adults. In the setting of magnesium sulfate therapy for severe preeclampsia, maintaining adequate urine output is essential for ensuring that the kidneys can excrete the magnesium to prevent accumulation and toxicity. If urine output decreases significantly, it may necessitate reevaluation of the infusion rate or additional interventions to support renal function.
Choice D reason:
A heart rate of 56 beats per minute is slightly bradycardic but may not be clinically significant if the client is asymptomatic. However, magnesium has a direct effect on cardiac function, and high levels can lead to bradycardia and other cardiac conduction abnormalities. It is important to monitor the client's heart rate and rhythm during magnesium sulfate therapy to detect any early signs of cardiac involvement due to magnesium toxicity.
A nurse at a family planning clinic is caring for a 17-year-old female client who is requesting oral contraceptives. The client expresses that she is nervous because she has never had a pelvic exam. Which of the following responses should the nurse provide?
Explanation
Choice A reason:
Telling a client that a pelvic exam is required for birth control pills is not accurate. Current medical guidelines indicate that a pelvic exam is not necessary to prescribe oral contraceptive medications, hormonal contraceptives can be safely prescribed based on medical history and blood pressure measurement without the need for a pelvic or breast examination.
Choice B reason:
While offering support is important, simply telling the client not to worry does not address her specific concerns or provide her with information about the process and her options.
Choice C reason:
Advising the client to relax does not acknowledge the validity of her feelings or provide her with any concrete information or support to help alleviate her anxiety.
Choice D reason:
Asking the client what part of the exam makes her most nervous is an open-ended question that invites dialogue. It allows the nurse to provide targeted information and reassurance, addressing the client's specific concerns and promoting a sense of control and participation in her own health care decisions.
A nurse is observing a new mother as she bathes her newborn son for the first time. Which of the following actions would require the nurse to intervene?
Explanation
Choice A Reason:
Using a cotton-tipped swab to clean a newborn's nares can be dangerous. It can push debris further into the nose, cause mucosal damage, bleeding, or even introduce germs. Instead, the nurse should advise the mother to use a bulb syringe for gentle suction if necessary.
Choice B Reason:
Leaving the yellow exudate on the circumcision site is actually recommended. This exudate is part of the normal healing process and does not need to be removed. It acts as a natural barrier to infection and will clear up as the circumcision heals.
Choice C Reason:
Cleaning the umbilical cord with tap water is generally considered safe and can help keep the area clean. However, the nurse should ensure that the mother dries the area thoroughly afterward to prevent moisture from promoting bacterial growth.
Choice D Reason:
Cleaning the newborn's eyes from the inner canthus outwards is the correct technique. It prevents contamination from the outer part of the eye to the inner part and helps to clear any discharge or debris effectively.
A nurse is caring for a client who is starting to breastfeed her newborn after delivery. The new mother says, "I don't want to take any pain medication because I'm breastfeeding." Which of the following responses should the nurse provide?
Explanation
Choice a) reason:
Timing the administration of pain medication can help minimize the amount of medication that passes into the breast milk. By scheduling pain relief around breastfeeding times, the nurse can ensure that the peak concentration of the medication in the blood (and therefore potentially in the milk) does not coincide with the baby's feeding times. This approach helps manage the mother's pain while also protecting the newborn from unnecessary exposure to medication.
Choice b) reason:
While managing pain is important for the mother's comfort and recovery, stating that she needs to take medication without considering her concerns about breastfeeding may not be supportive or respectful of her wishes. It's essential to address her concerns and provide options that align with her breastfeeding goals.
Choice c) reason:
It is true that all medications can be found in breast milk to some extent; however, the levels can vary widely based on the medication's properties. The nurse should provide information about the specific medication's safety during breastfeeding and discuss any potential risks with the mother.
Choice d) reason:
Informing the mother that she has the option of not taking pain medication addresses her autonomy in decision-making. However, it's also important for the nurse to discuss the potential consequences of untreated pain, such as impaired ability to care for the newborn and delayed recovery.
A nurse at a clinic is educating the mother of a 4-month-old infant who has been breastfed. The mother intends to transition her baby to an iron-fortified formula. Which of the following points should be included in the teaching?
Explanation
Choice A Reason:
Iron is not poorly absorbed in infants; in fact, infants absorb iron quite efficiently. Breast milk contains a small amount of iron, but it is highly bioavailable and well-absorbed. When switching to formula, it is important to use iron-fortified options to prevent iron deficiency anemia.
Choice B Reason:
While iron is essential for overall growth and development, including bone growth, it is not the primary reason for emphasizing iron in infant nutrition. The key concern with iron, especially when transitioning from breastfeeding, is the prevention of iron deficiency anemia, which can affect cognitive and motor development.
Choice C Reason:
This is the correct information to include in the teaching. Infants are born with a reserve of iron that begins to deplete around 4 to 6 months of age. It is crucial to introduce iron-fortified formula at this time to ensure the infant continues to receive adequate iron for development and to prevent iron deficiency anemia.
Choice D Reason:
Iron does play a role in the development of the nervous system, which can indirectly affect vision, but it is not specifically known for facilitating the development of vision in infants. The primary concern with iron intake in infants relates to its role in preventing anemia and supporting overall growth and development.
A nurse is educating a pregnant client who has phenylketonuria (PKU). Which of the following foods should the nurse advise the client to remove from her diet?
Explanation
Choice A Reason:
Peanut butter should be eliminated from the diet of a pregnant client with PKU. It is a high-protein food that contains phenylalanine, an amino acid that individuals with PKU cannot metabolize properly¹. The accumulation of phenylalanine can lead to serious health issues for both the mother and the developing fetus, including the risk of intellectual disability in the child.
Choice B Reason:
Potatoes are generally safe for individuals with PKU to consume. They are not high in protein and thus do not contain large amounts of phenylalanine. However, portion sizes and overall dietary balance should be monitored by a healthcare professional to ensure proper nutrition.
Choice C Reason:
Apple juice is also safe for individuals with PKU. It does not contain protein and therefore is not a significant source of phenylalanine. It can be included in the diet as part of the fluid intake.
Choice D Reason:
Broccoli is a low-protein vegetable and is typically allowed in the diets of individuals with PKU. It contains some phenylalanine, but in much lower amounts compared to high-protein foods. As with all foods, it should be consumed in moderation according to dietary guidelines provided by a healthcare professional.
A nurse is caring for multiple clients. The nurse should identify which of the following clients it is safe to administer tocolytic therapy to?
Explanation
Choice A Reason:
Tocolytic therapy is not indicated for a client with a post-term pregnancy. Tocolytics are medications used to suppress premature labor, and a pregnancy at 42 weeks is considered post-term, not preterm.
Choice B Reason:
Braxton-Hicks contractions are normal occurrences during pregnancy and do not indicate preterm labor. They are often referred to as "false labor" because they do not lead to cervical dilation or effacement. Therefore, tocolytic therapy is not necessary.
Choice C Reason:
Administering tocolytic therapy in the case of fetal death is not appropriate. Tocolytics are used to delay preterm labor to allow for fetal maturation or to prolong pregnancy to administer corticosteroids for fetal lung development, which is not applicable in this scenario.
Choice D Reason:
Tocolytic therapy is appropriate for a client experiencing preterm labor at 26 weeks of gestation. The goal of tocolytic therapy is to delay delivery to allow for the administration of corticosteroids to accelerate fetal lung maturity or to transfer the client to a facility equipped for premature infants.
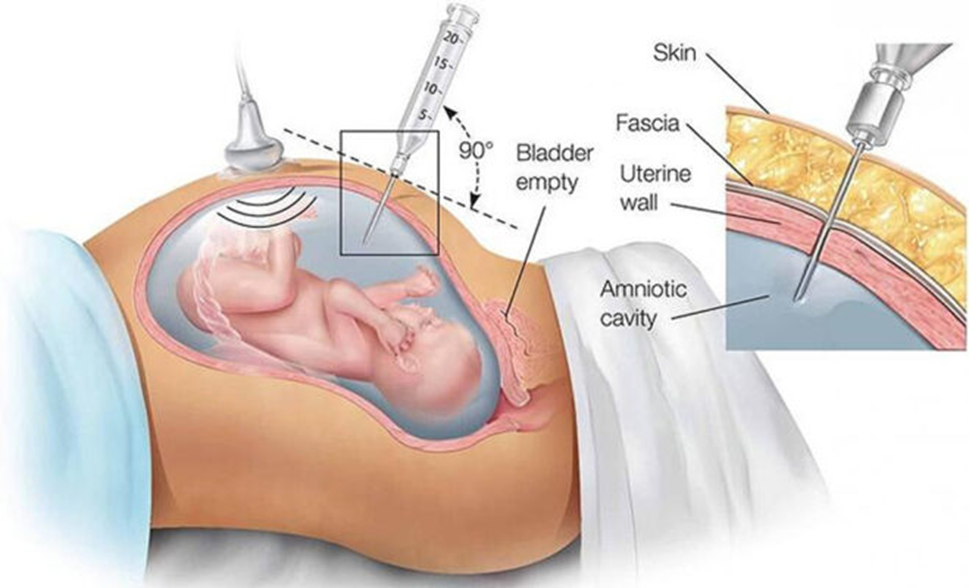
A nurse is educating a client who is 23 weeks pregnant and is scheduled to return to the facility in 2 days for an amniocentesis. Which of the following instructions should the nurse provide to the client?
Explanation
Choice A Reason:
It is not necessary to avoid food and fluids the day of the procedure unless specifically instructed by the healthcare provider. Amniocentesis does not typically require fasting; however, some facilities may have different protocols.
Choice B Reason:
A bowel prep protocol is not required for an amniocentesis. This procedure is unrelated to the gastrointestinal tract, and bowel preparation is more commonly associated with procedures like colonoscopy.
Choice C Reason:
Emptying the bladder immediately prior to the procedure is important. A full bladder can obstruct the view of the uterus during ultrasound, which is used to guide the amniocentesis needle. Additionally, an empty bladder reduces the risk of accidental puncture during the procedure.
Choice D Reason:
Washing the abdomen with soap and water the morning of the procedure is a good hygiene practice but is not specifically required for amniocentesis. The area will be cleaned with antiseptic by the healthcare provider before the procedure.
A nurse at a prenatal clinic is educating a group of clients about nutritional needs during lactation. Which of the following statements should the nurse provide?
Explanation
Choice A Reason:
The recommended intake of iron does not necessarily increase during lactation. In fact, the iron requirement may decrease because menstruation usually ceases, reducing iron loss. However, maintaining adequate iron intake is still important for overall health and to support the baby's growth.
Choice B Reason:
Zinc is crucial for immune function, cell division, and growth, making it an important nutrient during lactation. The recommended dietary allowance (RDA) for zinc for lactating women is indeed higher than for non-pregnant, non-lactating women, with an RDA of about 12 mg per day.
Choice C Reason:
While calcium is important for bone health, the recommended intake for lactating women is not as high as 2,000 mg per day. The RDA for calcium for lactating women is about 1,000 mg per day, similar to that for non-lactating women.
Choice D Reason:
The recommended intake of folic acid does not remain the same as for pregnant women. During pregnancy, the RDA for folic acid is higher to prevent neural tube defects. While folic acid is still important during lactation for cell growth and DNA synthesis, the requirement is slightly lower than during pregnancy.
A nurse is caring for a client in active labor and observes late decelerations on the fetal monitor. What is the priority nursing action?
Explanation
Choice A reason:
Administering oxygen via face mask is a common intervention for late decelerations; however, it is not the first-line action. Oxygen is given to improve fetal oxygenation, but repositioning the mother has a more immediate effect on improving uteroplacental blood flow and, consequently, fetal oxygenation12.
Choice B reason:
Increasing the infusion rate of IV fluid is an intervention used to expand maternal blood volume, which can improve placental perfusion. However, this is not the primary action to be taken when late decelerations are noted, as it may take time for the increased fluid to affect the uteroplacental circulation.
Choice C reason:
Elevating the client’s legs can help increase venous return to the heart, potentially improving uteroplacental circulation. Nonetheless, this is not the most immediate action to take for late decelerations, as it does not directly address the potential compression of the vena cava or aorta.
Choice D reason:
Positioning the client on her side, particularly the left side, is the priority nursing action for late decelerations. This position helps relieve pressure on the inferior vena cava, enhancing maternal cardiac output and increasing blood flow to the placenta, which can quickly improve fetal oxygenation and resolve late decelerations
A nurse in a clinic is evaluating a client who is 8 weeks pregnant and experiencing hyperemesis gravidarum. Which of the following findings should the nurse anticipate? (Select all that apply)
Explanation
Choice a) Reason: History of migraines
Women with a history of migraines may experience an improvement or worsening of their migraine symptoms during pregnancy. Hyperemesis gravidarum, a condition characterized by severe nausea and vomiting, can be associated with migraines due to hormonal changes, stress, or dehydration that pregnancy may exacerbate.
Choice b) Reason: History of gestational hypertension
Gestational hypertension typically develops after 20 weeks of gestation, so it would not be expected in a client at 8 weeks of gestation. Additionally, there is no direct correlation between gestational hypertension and hyperemesis gravidarum.
Choice c) Reason: Twin gestations
Twin or multiple gestations can increase the likelihood of hyperemesis gravidarum due to higher levels of hCG (human chorionic gonadotropin) and other pregnancy-related hormones. These elevated hormone levels are associated with more severe nausea and vomiting.
Choice d) Reason: Nulliparous
Nulliparity (having never given birth) is not directly associated with an increased risk of hyperemesis gravidarum. However, first-time pregnancies can be unpredictable, and the condition can occur regardless of parity.
Choice e) Reason: Oligohydramnios
Oligohydramnios refers to a decreased amount of amniotic fluid and is not typically associated with hyperemesis gravidarum. It is more commonly related to conditions affecting the placenta or fetal kidneys.
A nurse is caring for a postpartum client and notes that the fundus is slightly boggy and shifted to the right. Based on these observations, which of the following actions should the nurse take?
Explanation
Choice a Reason: Encourage the client to move to the left lateral position
Moving to the left lateral position is often recommended to improve circulation and prevent compression of the vena cava by the uterus in a pregnant client. However, in the case of a boggy fundus postpartum, this position is not the primary action to be taken.
Choice b Reason: Ask the client to rate her pain
While assessing pain is important in the postpartum period, it is not the immediate action required for a boggy fundus. A boggy fundus indicates that the uterus is not contracting properly, which can lead to excessive bleeding.
Choice c Reason: Assist the client to the bathroom to void
A boggy fundus that is displaced to the right often indicates a full bladder, which can prevent the uterus from contracting effectively. Assisting the client to the bathroom to void can help the uterus contract and reduce the risk of hemorrhage.
Choice d Reason: Encourage the client to perform Kegel exercises
Kegel exercises are beneficial for strengthening the pelvic floor muscles after childbirth. However, they are not the immediate action to take for a boggy fundus postpartum
A nurse is preparing to give methylergonovine IM to a client who has had a vaginal delivery. The nurse should inform the client that the purpose of this medication is to prevent which of the following conditions?
Explanation
Choice a reason:
Methylergonovine is a medication used to prevent postpartum hemorrhage, which is excessive bleeding following childbirth. It works by causing the uterine muscles to contract, thereby reducing blood loss. Postpartum hemorrhage is a significant cause of maternal morbidity and mortality worldwide, and methylergonovine is one of the medications used as a prophylactic measure to manage this risk.
Choice b reason:
While postpartum infections are a concern after childbirth, methylergonovine is not used to prevent infections. Postpartum infections can occur in different parts of the body, such as the uterus (endometritis), the urinary tract, or the site of an episiotomy or cesarean section incision. Prevention of postpartum infections typically involves hygiene practices, antibiotic prophylaxis when indicated, and monitoring for signs of infection.
Choice c reason:
Thromboembolic events, which include deep vein thrombosis and pulmonary embolism, are also a risk during the postpartum period. However, methylergonovine is not used to prevent these conditions. Prevention of thromboembolic events in the postpartum period may involve the use of anticoagulants, mechanical methods such as compression stockings, and early mobilization.
Choice d reason:
Hypertension, or high blood pressure, may be observed during the postpartum period, but methylergonovine is not indicated for the prevention of hypertension. Management of postpartum hypertension typically includes antihypertensive medications and monitoring of blood pressure levels. Methylergonovine can actually cause an increase in blood pressure as a side effect, so it must be used cautiously in individuals with hypertension.
A nurse is caring for a client who is 40 weeks pregnant and in labor. An ultrasound examination shows that the fetus is small for gestational age (SGA). Which of the following interventions should be included in the newborn's care plan?
Explanation
Choice a reason:
Observing for meconium in respiratory secretions is crucial for SGA newborns because they are at increased risk for meconium aspiration syndrome (MAS). MAS occurs when a newborn breathes in meconium-stained amniotic fluid into their lungs, which can cause respiratory distress. It is more common in full-term or post-term babies, and early detection and treatment are vital for improving outcomes.
Choice b reason:
Monitoring for hyperglycemia is important as SGA newborns are at risk for blood sugar imbalances. Hyperglycemia in newborns can be due to various factors, including stress, and requires careful management to prevent complications. However, it is not the primary concern immediately post-delivery for SGA newborns compared to the risk of MAS.
Choice c reason:
Monitoring for hyperthermia is less commonly a primary concern for SGA newborns immediately after birth. Hyperthermia can lead to dehydration and increase metabolic demands, which can be harmful to newborns. However, the immediate risk of hyperthermia is not as high as the risk of MAS for SGA newborns.
Choice d reason:
Identifying manifestations of anemia is important in newborn care. Anemia in newborns can present as pale skin, irritability, and a fast heart rate. While it is a condition that requires attention, the immediate post-delivery concern for SGA newborns is typically the risk of MAS rather than anemia.
A nurse is caring for a client who is a primigravida at term, experiencing contractions, but is unsure if she is "truly in labor." Which of the following should the nurse identify as a sign of true labor?
Explanation
Choice a reason:
The pattern of contractions can be a sign of true labor when they are regular, frequent, and increase in intensity and duration over time. In true labor, contractions do not subside with rest or hydration and become progressively more organized. However, contractions alone can be misleading, as Braxton Hicks contractions may also present a pattern but do not lead to cervical changes.
Choice b reason:
The station of the presenting part refers to the position of the baby's head (or presenting part) in relation to the ischial spines of the mother's pelvis. While the station can indicate how far labor has progressed, it is not a definitive sign of true labor. The station changes as labor progresses, but it can also be affected by other factors such as the baby's position.
Choice c reason:
Rupture of the membranes, commonly known as water breaking, can occur before or during labor. While it is a sign that labor may be imminent, it does not confirm true labor. Some women may experience premature rupture of membranes without contractions or cervical changes.
Choice d reason:
Changes in the cervix, including effacement (thinning) and dilation (opening), are the most reliable signs of true labor. Effacement is measured in percentages, and dilation is measured in centimeters. The cervix must be 100% effaced and dilated to 10 centimeters for childbirth to occur. These changes are a direct result of true labor contractions and indicate that the body is preparing for delivery.
A nurse is getting ready to administer magnesium sulfate IV to a client experiencing preterm labor. Which of the following is the priority nursing assessment for this client?
Explanation
Choice a reason:
Temperature monitoring is important in preterm labor to detect infections or inflammations that could complicate the pregnancy. However, while maternal temperature is a vital sign that should be monitored, it is not the priority in this context. The priority is to assess the well-being of the fetus, which is directly indicated by the FHR.
Choice b reason:
Bowel sounds are assessed to ensure gastrointestinal function and to detect potential complications such as ileus or bowel obstruction. In the context of preterm labor, while bowel sounds are part of a comprehensive assessment, they are not the priority over fetal well-being and maternal respiratory status, especially when administering magnesium sulfate, which does not primarily affect gastrointestinal function.
Choice c reason:
Respiratory rate is a critical assessment when administering magnesium sulfate due to the risk of respiratory depression as a side effect of the medication. It is essential to monitor because maternal oxygenation directly affects fetal oxygenation. However, the FHR is a more direct measure of fetal distress and therefore takes priority in this specific assessment.
Choice d reason:
Fetal heart rate (FHR) monitoring is the priority nursing assessment when administering magnesium sulfate IV to a client in preterm labor. Magnesium sulfate can affect uterine contractions and, by extension, fetal oxygenation and well-being. FHR is the most direct indicator of fetal distress, which can occur if the uterus becomes too relaxed and compromises placental blood flow or if there are side effects affecting the mother's cardiovascular status. Therefore, continuous monitoring of FHR is crucial to ensure the fetus is not experiencing distress.
A nurse in a prenatal clinic is caring for a client who is 38 weeks pregnant and reports heavy, red vaginal bleeding that began spontaneously in the morning without any contractions. The client is not in distress and mentions that she can "feel the baby moving." An ultrasound is scheduled right away. The nurse should inform the client that the purpose of the ultrasound is to determine which of the following?
Explanation
Choice a reason:
The viability of the fetus at 38 weeks of gestation is typically not the primary concern when heavy, red vaginal bleeding occurs without contractions. Fetal movements reported by the mother are a good sign of fetal well-being. However, the ultrasound in this scenario is more likely to be used to rule out placental issues that could cause bleeding, rather than to assess fetal viability.
Choice b reason:
The biparietal diameter (BPD) is a measurement taken during an ultrasound to assess fetal growth and development. While BPD is an important parameter, it is not typically the focus of an urgent ultrasound in the context of heavy vaginal bleeding late in pregnancy. The BPD is more relevant to growth assessments rather than acute bleeding episodes.
Choice c reason:
Locating the placenta is crucial in the case of heavy, red vaginal bleeding at 38 weeks of gestation. The bleeding could be indicative of placental abruption or placenta previa, both of which are serious conditions that require immediate medical attention. An ultrasound can quickly determine the location of the placenta and assess for these conditions.
Choice d reason:
Assessing fetal lung maturity is not typically the priority in an emergency situation involving heavy vaginal bleeding. While lung maturity is an important consideration for the timing of delivery, especially in preterm labor, the immediate concern in this scenario would be to identify the source of bleeding and ensure the safety of both the mother and fetus.
A nurse is caring for a client who is exploring different contraception options. Which of the following methods should the nurse identify as the most reliable?
Explanation
Choice a reason:
A male condom is a barrier method of contraception that is typically easy to use and accessible. It has the added benefit of providing protection against sexually transmitted infections (STIs). However, its effectiveness can be compromised by improper use or breakage. With typical use, male condoms are about 85% effective.
Choice b reason:
A diaphragm with spermicide is another barrier method that can be used to prevent pregnancy. The diaphragm covers the cervix and the spermicide kills or immobilizes sperm. The effectiveness of a diaphragm with spermicide is generally lower than some other methods, with typical use effectiveness around 88%.
Choice c reason:
An intrauterine device (IUD) is a small device inserted into the uterus by a healthcare provider. IUDs come in two types: hormonal and copper. Both types are highly effective, with over 99% effectiveness. They are long-acting, reversible, and do not require daily attention, which contributes to their reliability.
Choice d reason:
An oral contraceptive, also known as the birth control pill, is a popular method of contraception that requires the user to take a pill at the same time every day. The effectiveness of the pill can be high, but because it relies on user adherence, its typical use effectiveness is around 91%.
A nurse is assessing a client who is 3 days postpartum and breastfeeding. The nurse observes that the fundus is three fingerbreadths below the umbilicus, lochia rubra is moderate, and the breasts are firm and warm to the touch. Which of the following interpretations should the nurse make based on these findings?
Explanation
Choice a reason:
Mastitis is an infection of the breast tissue that results in pain, swelling, warmth, and redness. The symptoms of mastitis typically include breast tenderness, redness on the skin, breast pain, and sometimes fever and malaise. While the client's breasts are described as hard and warm, which could be associated with mastitis, the absence of other key symptoms such as fever or flu-like symptoms suggests that mastitis may not be the issue here.
Choice b reason:
Three days postpartum, it is normal for the fundus to be below the umbilicus and for lochia rubra to be present. The hardness and warmth of the breasts could be due to milk coming in, which is also a normal postpartum change. Without additional symptoms of concern, such as fever, severe pain, or signs of infection, it is reasonable to conclude that no additional interventions are required at this time.
Choice c reason:
Removing a nursing bra can provide comfort, especially if it is too tight and contributing to breast engorgement or clogged ducts. However, there is no indication that the client's nursing bra is causing an issue. Nursing bras are designed to support the breasts during breastfeeding and typically do not need to be removed unless they are causing specific problems.
Choice d reason:
Applying a heating pad can help with milk let-down and relieve discomfort from engorgement or clogged ducts. However, since the client is not exhibiting signs of mastitis or severe engorgement, and the warmth of the breasts may be due to normal postpartum changes, the application of a heating pad is not necessarily indicated at this time.
A nurse is caring for a newborn who is small for gestational age (SGA). Which of the following findings is commonly linked to this condition?
Explanation
Choice a reason:
Moist skin is not typically associated with SGA newborns. Newborns, in general, may have moist skin shortly after birth due to the amniotic fluid and vernix caseosa, but this is not a distinguishing characteristic of SGA infants.
Choice b reason:
A gray umbilical cord is not a finding specifically associated with SGA. The color of the umbilical cord at birth can vary, and a gray color may indicate that the cord is drying, which is a normal process after clamping and cutting the cord.
Choice c reason:
Wide skull sutures are associated with SGA infants. SGA can be a result of intrauterine growth restriction (IUGR), which can lead to underdevelopment of the skull bones, resulting in wider-than-normal sutures. This is because the skull may not have grown to its expected size due to the growth restriction experienced by the infant.
Choice d reason:
A protruded abdomen is not typically associated with SGA infants. In fact, SGA infants may have a scaphoid or sunken abdomen due to reduced subcutaneous fat and muscle mass. A protruded abdomen in a newborn could be a sign of other conditions such as organomegaly or gastrointestinal issues.
A nurse is caring for a client with preeclampsia who is receiving magnesium sulfate treatment. The client's respiratory rate is 10 breaths per minute, and deep-tendon reflexes are absent. Which of the following actions should the nurse take?
Explanation
Choice a reason:
Placing the client in the Trendelenburg position, which involves lying on the back with the feet higher than the head, is not indicated for the symptoms presented. This position is typically used to treat hypotension or improve venous return to the heart, not for respiratory depression or absent deep-tendon reflexes, which are signs of magnesium sulfate toxicity.
Choice b reason:
Assessing maternal blood glucose is important in the overall care of a preeclamptic patient, especially if there is a concern for gestational diabetes. However, it is not the immediate action required when a patient exhibits signs of magnesium sulfate toxicity, such as a respiratory rate of 10/min and absent deep-tendon reflexes.
Choice c reason:
Discontinuing the medication infusion is the correct action. A respiratory rate of 10/min and absent deep-tendon reflexes are signs of magnesium sulfate toxicity. Immediate cessation of the drug is necessary to prevent further complications, such as respiratory depression or cardiac arrest. After stopping the infusion, the nurse should monitor the patient closely and prepare to administer calcium gluconate, the antidote for magnesium sulfate toxicity, if ordered by the physician.
Choice d reason:
Preparing for an emergency cesarean birth may be necessary if the fetus is in distress or if there are other obstetric indications. However, the information provided does not indicate fetal distress or an immediate need for delivery. The priority is addressing the signs of magnesium sulfate toxicity in the mother.
A nurse is caring for a client who is 1 hour postpartum and notices a large amount of lochia rubra along with several small clots on the client's perineal pad. The fundus is midline and firm at the level of the umbilicus. Which of the following actions should the nurse take?
Explanation
Choice a reason:
Encouraging the client to empty her bladder is an appropriate action because a full bladder can displace the uterus and prevent it from contracting effectively, which can lead to increased bleeding. By emptying the bladder, the uterus can contract more efficiently and reduce the amount of lochia.
Choice b reason:
Increasing the frequency of fundal massage is not necessary in this case because the fundus is already firm and at the level of the umbilicus, which indicates that the uterus is contracting well. Fundal massage is typically used when the uterus is boggy or not well-contracted.
Choice c reason:
Notifying the client's provider may not be immediately necessary if the fundus is firm and there are no other signs of complications. The presence of lochia rubra and small clots can be normal within the first few hours postpartum. However, if the bleeding increases or other symptoms arise, the provider should be notified.
Choice d reason:
Documenting the findings and continuing to monitor the client is an ongoing part of postpartum care. However, the priority action in this scenario is to address the potential cause of increased bleeding, which is likely a full bladder. Therefore, while documentation and monitoring are important, they are secondary to ensuring the bladder is emptied.
A nurse is reinforcing education with a client on how to reduce the risk of perineal infection after a vaginal delivery. Which of the following points should the nurse include in the teaching? (Select all that apply.)
Explanation
Choice a reason:
Washing the perineal area using a squeeze bottle of warm water after each voiding is a recommended practice to reduce the risk of infection. This method gently cleanses without causing irritation and ensures that any bacteria are washed away, which is particularly important after a vaginal delivery when the perineal tissue may be more susceptible to infection.
Choice b reason:
Applying ice packs to the perineal area several times daily can help reduce swelling and provide pain relief, but it is not directly related to reducing the risk of infection. Ice packs should be used as part of pain management and swelling reduction rather than for hygiene purposes.
Choice c reason:
Blotting the perineal area dry after cleansing is important to maintain the integrity of the skin and prevent moisture buildup, which can create an environment conducive to bacterial growth. Patting the area dry gently can help prevent irritation and reduce the risk of infection.
Choice d reason:
Cleaning the perineal area from front to back is a critical practice to prevent the spread of bacteria from the anal area to the vagina and urethra, which can cause urinary tract infections. This technique is especially important postpartum when the perineal area is healing.
Choice e reason:
Performing hand hygiene before and after voiding is a fundamental practice to prevent the introduction of pathogens to the perineal area and reduce the risk of infection. Proper handwashing can significantly decrease the likelihood of perineal infections by ensuring that the hands are clean when they come into contact with sensitive areas.
Sign Up or Login to view all the 89 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
