ATI Med Surg Exam 3
Total Questions : 56
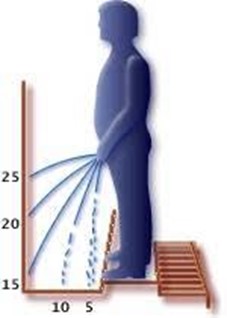
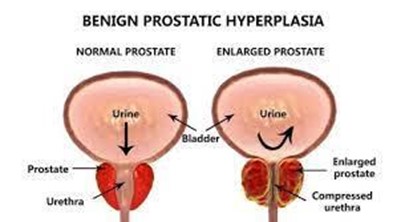
Showing 25 questions, Sign in for moreA nurse is caring for a client who has benign prostatic hyperplasia (BPH). Which of the following findings should the nurse expect?
Explanation
Choice A Reason: Painful urination is not a common finding in BPH, but it may indicate a urinary tract infection or bladder stones.
Choice B Reason: Decreased urinary stream is a common finding in BPH, as the enlarged prostate compresses the urethra and obstructs the flow of urine.
Choice C Reason: Critically elevated PSA level is not a common finding in BPH, but it may indicate prostate cancer or prostatitis.
Choice D Reason: Urge incontinence is not a common finding in BPH, but it may indicate an overactive bladder or neurogenic bladder.
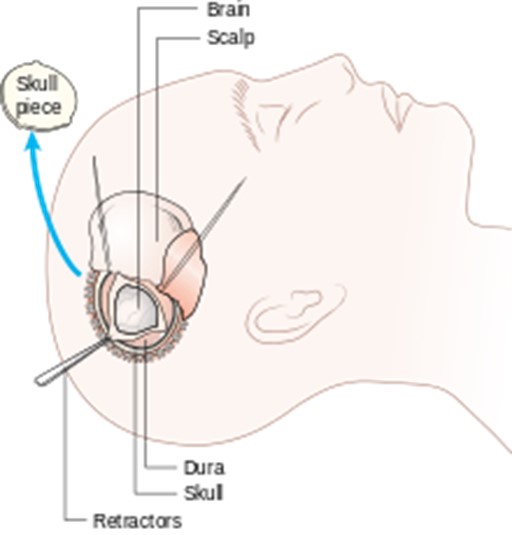
A nurse is monitoring a client for findings related to diabetes insipidus following a craniotomy. Which of the following findings should indicate a manifestation of this condition to the nurse?
Explanation
Choice A Reason: Hypertension is not a common finding in diabetes insipidus, but it may indicate increased intracranial pressure or other complications.
Choice B Reason: Fluid retention is not a common finding in diabetes insipidus, but it may indicate syndrome of inappropriate antidiuretic hormone secretion (SIADH) or heart failure.
Choice C Reason: Elevated blood glucose is not a common finding in diabetes insipidus, but it may indicate diabetes mellitus or hyperglycemia.
Choice D Reason: Increased urine output is a common finding in diabetes insipidus, as the lack of antidiuretic hormone (ADH) causes the kidneys to excrete large amounts of diluted urine.
Which of the following clinical manifestations should a nurse expect from a client with hyperthyroidism? SELECT ALL THAT APPLY
Explanation
Choice A Reason: Heat intolerance is a common finding in hyperthyroidism, as the increased metabolic rate causes the body to produce more heat and sweat.
Choice B Reason: Diarrhea is a common finding in hyperthyroidism, as the increased motility of the gastrointestinal tract causes more frequent and loose stools.
Choice C Reason: Weight loss is a common finding in hyperthyroidism, as the increased metabolism and appetite cause the body to burn more calories than it consumes.
Choice D Reason: Weight gain is not a common finding in hyperthyroidism, but it may indicate other conditions such as hypothyroidism or Cushing's syndrome.
Choice E Reason: Bradycardia is not a common finding in hyperthyroidism, but it may indicate other conditions such as heart block or beta-blocker use.
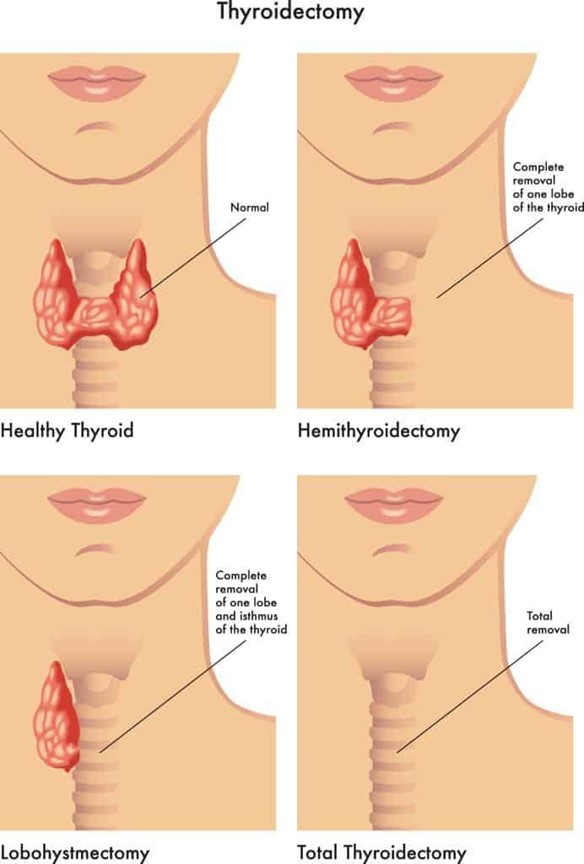
The nurse is caring for a client after a total thyroidectomy. The nurse's priority should be to:
Explanation
Choice A Reason: Encouraging the client to cough and deep breathe every two hours, with her neck in a flexed position, is not a priority for a client after a total thyroidectomy, as it may increase the risk of bleeding or damage to the surgical site.
Choice B Reason: Maintaining the client in a Fowler's position, with head neutral supported by pillows, is a priority for a client after a total thyroidectomy, as it helps to reduce swelling and edema, prevent airway obstruction, and promote venous drainage.
Choice C Reason: Maintaining the client in a supine position, with sandbags placed on either side of her head and neck, is not a priority for a client after a total thyroidectomy, as it may impair breathing and circulation, increase pressure on the surgical site, and cause neck stiffness.
Choice D Reason: Encouraging the client to turn head side to side, to promote drainage of oral secretions, is not a priority for a client after a total thyroidectomy, as it may cause pain and discomfort, disrupt the sutures or drains, and increase the risk of infection.
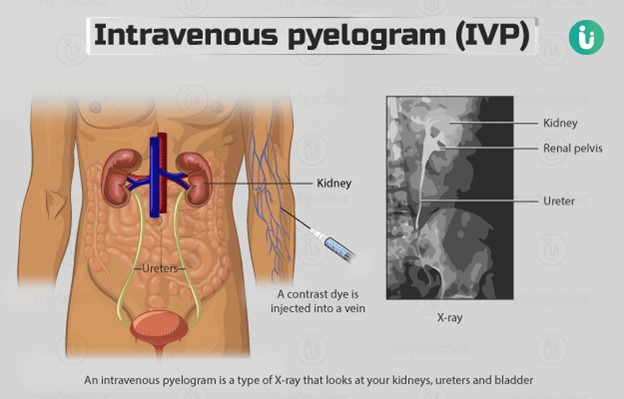
A nurse is reinforcing teaching with a client who is scheduled for an intravenous pyelogram (IVP). Which of the following statements should the nurse include in the teaching?
Explanation
Choice A Reason: The procedure will not be cancelled if the urinalysis indicates the presence of red blood cells, but it may indicate a urinary tract infection or kidney damage that needs further evaluation.
Choice B Reason: After the procedure, you will be encouraged to drink plenty of fluids, as this helps to flush out the contrast dye that was injected into your vein and prevent dehydration and kidney damage.
Choice C Reason: High frequency sound waves will not be used to identify renal system structures, but this is the principle of ultrasound imaging, which is a different diagnostic test.
Choice D Reason: You will not need to remain flat in bed for 4 hours following this procedure, but you may need to rest for a short period of time and avoid strenuous activities for the rest of the day.
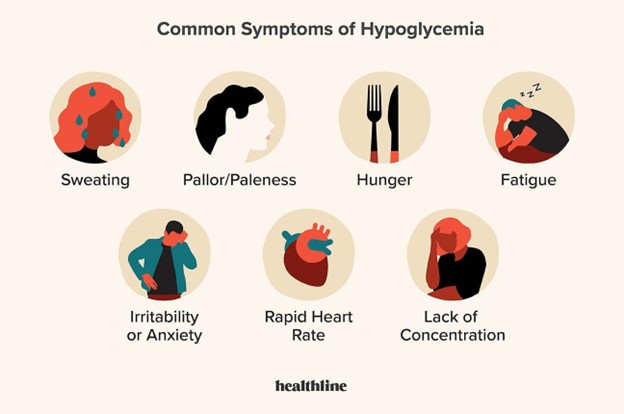
The nurse should teach a diabetic client that which symptom is indicative of hypoglycemia?
Explanation
Choice A Reason: Anorexia is not a symptom of hypoglycemia, but it may indicate a loss of appetite due to other causes such as nausea, infection, or depression.
Choice B Reason: Warm skin is not a symptom of hypoglycemia, but it may indicate a fever, inflammation, or infection.
Choice C Reason: Fruity breath is not a symptom of hypoglycemia, but it may indicate ketoacidosis, which is a serious complication of hyperglycemia.
Choice D Reason: Nervousness is a symptom of hypoglycemia, as the low blood glucose level affects the brain and causes anxiety, irritability, confusion, and tremors.
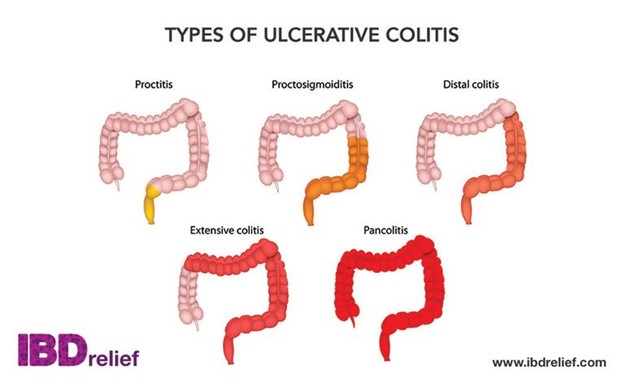
Which goal for the client's care should take priority when caring for a client admitted due to exacerbation of ulcerative colitis?
Explanation
Choice A Reason: Managing diarrhea is the priority goal for the client's care, as it helps to prevent dehydration, electrolyte imbalance, malnutrition, and infection.
Choice B Reason: Promoting rest and comfort is an important goal for the client's care, but it is not the priority, as it does not address the underlying cause of the exacerbation.
Choice C Reason: Increasing self-esteem is a long-term goal for the client's care, but it is not the priority, as it does not affect the physical condition of the client.
Choice D Reason: Promoting self-care and independence is a long-term goal for the client's care, but it is not the priority, as it does not affect the acute symptoms of the exacerbation.
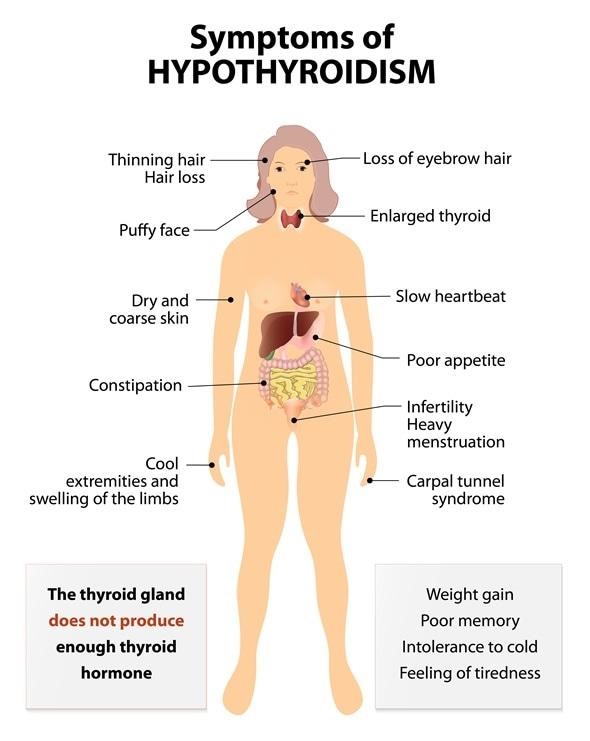
A client has been diagnosed with hypothyroidism. What information should the nurse obtain when conducting a focused assessment? Select all that apply.
Explanation
Choice A Reason: Weight gain is a common finding in hypothyroidism, as the decreased thyroid hormone level causes the metabolism to slow down and the body to store more fat.
Choice B Reason: Constipation is a common finding in hypothyroidism, as the decreased thyroid hormone level causes the gastrointestinal motility to decrease and the stools to become hard and dry.
Choice C Reason: Rapid pulse is not a common finding in hypothyroidism, but it may indicate other conditions such as hyperthyroidism or anxiety.
Choice D Reason: Decreased energy is a common finding in hypothyroidism, as the decreased thyroid hormone level causes the body to feel tired and sluggish.
Choice E Reason: Hypertension is not a common finding in hypothyroidism, but it may indicate other conditions such as renal disease or cardiovascular disease.
A client with multiple sclerosis is seen by the home health nurse and complains of severe fatigue. Which of the following is the most appropriate nursing intervention?
Explanation
Choice A Reason: Encouraging deep-breathing exercises is not the most appropriate nursing intervention, as it may not reduce fatigue and may increase respiratory effort.
Choice B Reason: Providing a relaxing warm bath is not the most appropriate nursing intervention, as it may worsen fatigue and increase the risk of heat intolerance and dehydration.
Choice C Reason: Scheduling periods of rest in between activities is the most appropriate nursing intervention, as it helps to conserve energy, prevent exhaustion, and promote recovery.
Choice D Reason: Administering multivitamins is not the most appropriate nursing intervention, as it may not improve fatigue and may cause adverse effects or interactions with other medications.
A nurse is reinforcing teaching about an endoscopy with a client who has dysphagia. Which of the following statements should the nurse include in the teaching?
Explanation
Choice A Reason: You will not remain NPO for 8 hours before the procedure, but you will be instructed to stop eating and drinking for 4 to 6 hours before the procedure.
Choice B Reason: A flexible tube is not introduced through the nose during the procedure, but through the mouth and down the esophagus.
Choice C Reason: During the procedure, a contrast dye is not administered via IV, but a sedative and an anesthetic spray are given to help you relax and numb your throat.
Choice D Reason: You will be awake while the procedure is performed, but you will not feel any pain or discomfort as the tube passes through your digestive tract.
A nurse is contributing to a teaching plan about the prevention of hepatitis A. The nurse should include which of the following activities can spread hepatitis A?
Explanation
Choice A Reason: Sharing personal hygiene items like razors is not a common way of spreading hepatitis A, but it may transmit hepatitis B or C, which are blood-borne infections.
Choice B Reason: Unprotected sexual activity is not a common way of spreading hepatitis A, but it may transmit hepatitis B or C, or other sexually transmitted infections.
Choice C Reason: Eating uncooked foods is a common way of spreading hepatitis A, as the virus can contaminate food or water that has been exposed to fecal matter from an infected person.
Choice D Reason: Getting a tattoo is not a common way of spreading hepatitis A, but it may transmit hepatitis B or C, or other blood-borne infections, if the equipment is not properly sterilized.
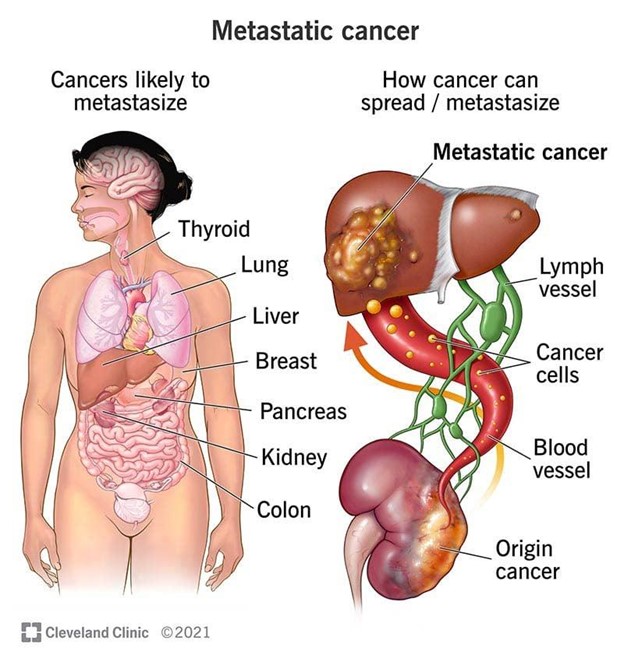
A nurse is reinforcing teaching about TNM staging with a client who has cancer. Which of the following information should the nurse include in the teaching?
Explanation
Choice A Reason: N0 does not indicate presence of regional lymph node involvement, but absence of it. N1 to N3 indicate increasing degrees of regional lymph node involvement.
Choice B Reason: TIS does not indicate that a tumor has been resolved, but that it is in situ, meaning that it is confined to the original site and has not invaded deeper tissues.
Choice C Reason: T4 does not indicate a tumor at its smallest size, but at its largest size. T1 to T4 indicate increasing sizes or extents of the primary tumor.
Choice D Reason: M1 indicates tumor metastasis to a single site, meaning that the cancer has spread to another organ or distant lymph node. M0 indicates no distant metastasis.
What should the nurse do first when a client with a head injury begins to have clear drainage from the nose?
Explanation
Choice A Reason: Compressing the nares is not the first action that the nurse should take, as it may increase intracranial pressure and worsen the head injury.
Choice B Reason: Administering decongestant for postnasal drip is not the first action that the nurse should take, as it may mask the signs of cerebrospinal fluid (CSF) leakage and delay diagnosis and treatment.
Choice C Reason: Tilting the head back is not the first action that the nurse should take, as it may cause aspiration of CSF or blood and increase the risk of infection.
Choice D Reason: Collecting the drainage is the first action that the nurse should take, as it helps to identify if the drainage is CSF or nasal secretions, and to monitor the amount and characteristics of the drainage.
A nurse is reinforcing teaching about TNM staging with a client who has cancer. Which of the following information should the nurse include in the teaching?
Explanation
Choice A Reason: N0 does not indicate presence of regional lymph node involvement, but absence of it. N1 to N3 indicate increasing degrees of regional lymph node involvement.
Choice B Reason: TIS does not indicate that a tumor has been resolved, but that it is in situ, meaning that it is confined to the original site and has not invaded deeper tissues.
Choice C Reason: T4 does not indicate a tumor at its smallest size, but at its largest size. T1 to T4 indicate increasing sizes or extents of the primary tumor.
Choice D Reason: M1 indicates tumor metastasis to a single site, meaning that the cancer has spread to another organ or distant lymph node. M0 indicates no distant metastasis.
A client diagnosed with esophageal varices has a Sengstaken-Blakemore tube. What is the most important safety intervention for this client?
Explanation
Choice A Reason: Keeping scissors at the bedside is the most important safety intervention for this client, as it allows for quick removal of the tube in case of airway obstruction or bleeding.
Choice B Reason: Providing good mouth care is an important intervention for this client, but it is not the most important, as it helps to prevent oral infections and discomfort.
Choice C Reason: Deflating the balloon on a regular basis is not an appropriate intervention for this client, as it may cause bleeding or displacement of the tube.
Choice D Reason: Monitoring IV fluid intake is an important intervention for this client, but it is not the most important, as it helps to prevent fluid overload or dehydration.
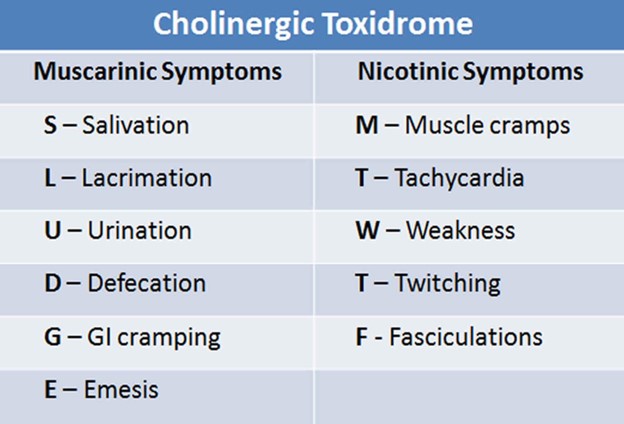
A nurse is caring for a client with myasthenia gravis who is exhibiting signs of cholinergic crisis. Which medication does the nurse ensure is available to treat this crisis?
Explanation
Choice A Reason: Atropine sulfate is the medication that the nurse should ensure is available to treat cholinergic crisis, as it blocks the effects of acetylcholine and reverses the symptoms of excessive parasympathetic stimulation.
Choice B Reason: Pyridostigmine bromide (Mestinon) is not the medication that the nurse should ensure is available to treat cholinergic crisis, but it is used to treat myasthenia gravis by increasing acetylcholine levels and improving muscle strength.
Choice C Reason: Protamine sulfate is not the medication that the nurse should ensure is available to treat cholinergic crisis, but it is used to reverse the effects of heparin and prevent bleeding.
Choice D Reason: Acetylcysteine (Mucomyst) is not the medication that the nurse should ensure is available to treat cholinergic crisis, but it is used to treat acetaminophen overdose and prevent liver damage.
What should the nurse do first when a client with a head injury begins to have clear drainage from the nose?
Explanation
Choice A Reason: Compressing the nares is not the first action that the nurse should take, as it may increase intracranial pressure and worsen the head injury.
Choice B Reason: Administering decongestant for postnasal drip is not the first action that the nurse should take, as it may mask the signs of cerebrospinal fluid (CSF) leakage and delay diagnosis and treatment.
Choice C Reason: Tilting the head back is not the first action that the nurse should take, as it may cause aspiration of CSF or blood and increase the risk of infection.
Choice D Reason: Collecting the drainage is the first action that the nurse should take, as it helps to identify if the drainage is CSF or nasal secretions, and to monitor the amount and characteristics of the drainage.
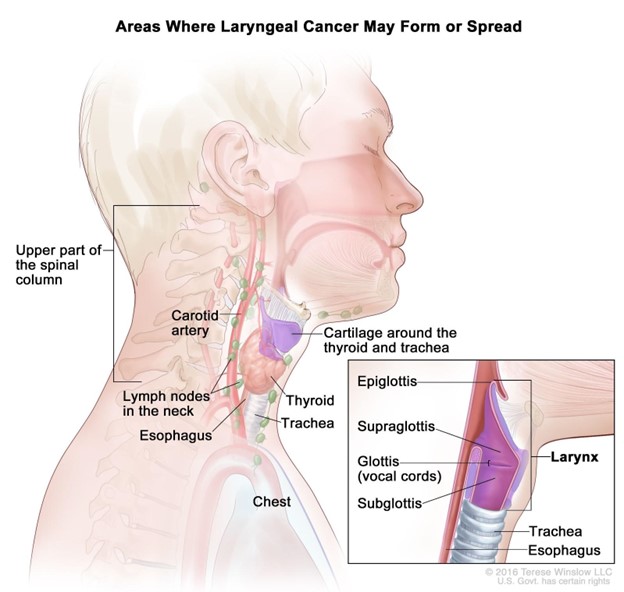
A nurse is collecting data from a client diagnosed with laryngeal cancer who is postoperative following a laryngectomy. Which of the following is a clinical manifestation of a hemorrhage?
Explanation
Choice A Reason: Increased pain is not a specific sign of hemorrhage, but it may indicate inflammation, infection, or nerve damage.
Choice B Reason: Continuous swallowing is a sign of hemorrhage, as it indicates that blood is accumulating in the throat or esophagus and stimulating the swallowing reflex.
Choice C Reason: Poor fluid intake is not a sign of hemorrhage, but it may indicate difficulty swallowing, nausea, or dehydration.
Choice D Reason: Drooling is not a sign of hemorrhage, but it may indicate impaired oral control, salivary gland damage, or infection.
A nurse reinforces instructions to a client with hypothyroidism about the dosage, method of administration, and side effects of levothyroxine sodium. Which statement by the client indicates an understanding of the nurse's instructions?
Explanation
Choice A Reason: If I feel nervous or have tremors, I should not only take half the dose, but I should contact my healthcare provider, as these may indicate signs of overdose or hyperthyroidism.
Choice B Reason: I cannot expect diarrhea, insomnia, and excessive sweating, but these are possible side effects of overdose or hyperthyroidism.
Choice C Reason: I need to call my healthcare provider if my heart rate becomes fast, as this may indicate a serious adverse reaction or overdose of levothyroxine sodium.
Choice D Reason: I should not take the medication in the evening, but in the morning on an empty stomach at least 30 minutes before breakfast, as this ensures better absorption and prevents insomnia.
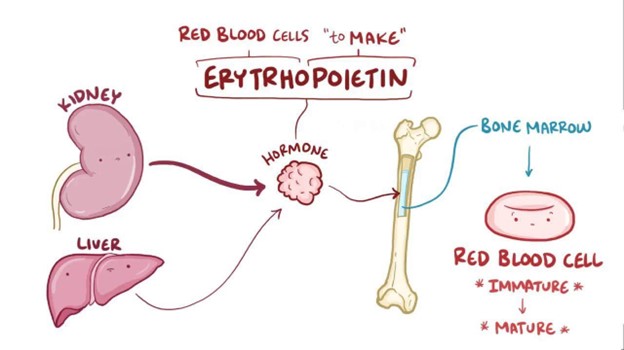
A client with chronic renal failure asks the nurse the effects of losing erythropoietin. Which of the following statements best explains the loss of this hormone?
Explanation
Choice A Reason: Loss of erythropoietin will not result in diminished immunologic function, but it may affect the production of some white blood cells and antibodies.
Choice B Reason: Loss of erythropoietin will not result in hypertension, but it may cause hypotension due to reduced blood volume and viscosity.
Choice C Reason: Loss of erythropoietin will not result in elevated lipid levels in the bloodstream, but it may be associated with dyslipidemia due to other factors such as malnutrition, inflammation, or medication use.
Choice D Reason: Loss of erythropoietin will result in anemia, as erythropoietin is a hormone that stimulates the bone marrow to produce red blood cells.
The nurse is completing a health assessment of a client suspected of hyperthyroidism. Which of the following clinical manifestations should the nurse expect?
Explanation
Choice A Reason: Cold skin is not a common finding in hyperthyroidism, but it may indicate hypothyroidism or other conditions such as hypothermia or shock.
Choice B Reason: Weight gain is not a common finding in hyperthyroidism, but it may indicate hypothyroidism or other conditions such as Cushing's syndrome or edema.
Choice C Reason: Tachycardia is a common finding in hyperthyroidism, as the increased thyroid hormone level causes the heart rate and cardiac output to increase.
Choice D Reason: Anorexia is not a common finding in hyperthyroidism, but it may indicate other conditions such as depression, infection, or cancer.
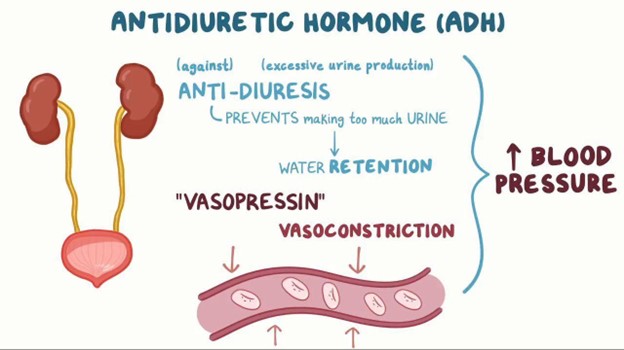
A nurse is reviewing data for a client who has a head injury. Which of the following findings should indicate to the nurse that the client might have diabetes insipidus?
Explanation
Choice A Reason: Urine output 800 mL/hr is a sign of diabetes insipidus, as it indicates that the kidneys are producing large amounts of diluted urine due to the lack of antidiuretic hormone (ADH) or its action.
Choice B Reason: Blood glucose 198 mg/dL is not a sign of diabetes insipidus, but it may indicate diabetes mellitus or hyperglycemia.
Choice C Reason: Serum sodium 145 mEq/L is not a sign of diabetes insipidus, but it is within the normal range (135-145 mEq/L).
Choice D Reason: Urine specific gravity 1.028 is not a sign of diabetes insipidus, but it indicates concentrated urine due to dehydration or other causes.
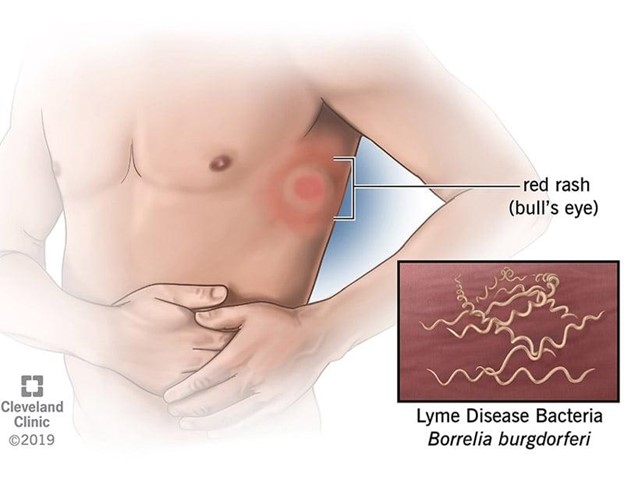
A nurse is collecting data from a client who was bitten by a tick one week ago. Which of the following client manifestations should the nurse identify as an indication of the development of Lyme disease?
Explanation
Choice A Reason: Swollen, painful joints are not a sign of Lyme disease in the early stage, but they may occur in the late stage, which can take months or years to develop.
Choice B Reason: An expanding circular rash, also known as erythema migrans, is a sign of Lyme disease in the early stage, which usually appears within 3 to 30 days after the tick bite. The rash may have a bull's-eye appearance and can spread up to 12 inches in diameter.
Choice C Reason: Decreased level of consciousness is not a sign of Lyme disease, but it may indicate other serious conditions such as meningitis, encephalitis, or stroke.
Choice D Reason: Necrosis at the site of the bite is not a sign of Lyme disease, but it may indicate a brown recluse spider bite, which can cause tissue damage and ulceration.
A nurse is assisting with data collection of a client with suspected cholecystitis. Which finding does the nurse expect to note if cholecystitis is present?
Explanation
Choice A Reason: Murphy sign is a finding that indicates cholecystitis, which is inflammation of the gallbladder. It is elicited by palpating the right upper quadrant of the abdomen and asking the client to take a deep breath. The client will experience pain and stop breathing in if cholecystitis is present.
Choice B Reason: McBurney sign is a finding that indicates appendicitis, which is inflammation of the appendix. It is elicited by palpating the right lower quadrant of the abdomen at a point one-third of the distance from the anterior superior iliac spine to the umbilicus. The client will experience pain and tenderness if appendicitis is present.
Choice C Reason: Cullen's sign is a finding that indicates intra-abdominal bleeding, which can be caused by various conditions such as ruptured ectopic pregnancy, pancreatitis, or trauma. It is characterized by bruising around the umbilicus due to blood accumulation under the skin.
Choice D Reason: Homan sign is a finding that indicates deep vein thrombosis (DVT), which is a blood clot in a deep vein, usually in the leg. It is elicited by dorsiflexing the foot and squeezing the calf muscle. The client will experience pain and resistance if DVT is present.
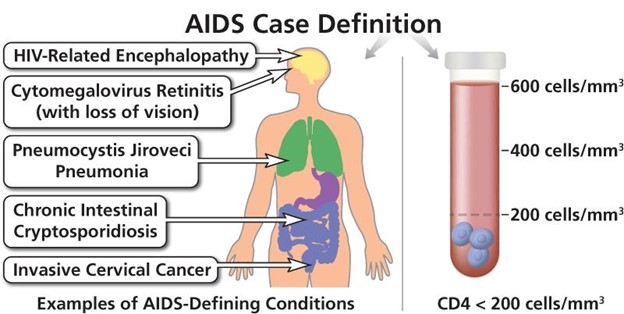
The nurse is participating in a care planning conference for a patient with acquired immunodeficiency syndrome (AIDS). What is the nurse's highest priority in providing care to this client?
Explanation
Choice A Reason: Instituting measures to prevent infection is the highest priority in providing care to this client, as AIDS impairs the immune system and makes the client susceptible to opportunistic infections that can be life-threatening.
Choice B Reason: Providing emotional support is an important aspect of providing care to this client, but it is not the highest priority, as it does not address the physical needs of the client.
Choice C Reason: Identifying risk factors related to contracting AIDS is not relevant for providing care to this client, as it does not help to improve the current condition or prevent complications.
Choice D Reason: Discussing the cause of AIDS is not essential for providing care to this client, as it does not affect the treatment or prognosis of the disease.
Sign Up or Login to view all the 56 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
