Ati medical surgical 2 final 2024 assessment
Total Questions : 135
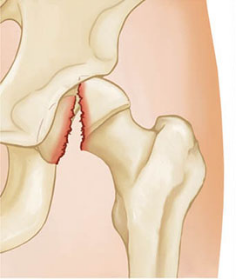
Showing 25 questions, Sign in for moreA nurse is attending to an elderly patient who sustained a femoral head fracture 24 hours prior and is currently in skin traction. The patient is experiencing shortness of breath and difficulty breathing. Which complication should the nurse suspect the patient has developed?
Explanation
Choice A reason:
Pneumothorax, a collapsed lung, can indeed cause shortness of breath and dyspnea. However, it is typically associated with a sudden onset of these symptoms following a chest injury or spontaneously in the case of a ruptured air blister. In the context of a femoral head fracture, pneumothorax is less likely unless there was additional trauma to the chest area.
Choice B reason:
Pneumonia is an infection of the lungs that leads to inflammation of the air sacs, causing them to fill with fluid or pus. Symptoms include cough with phlegm, fever, chills, and difficulty breathing. While pneumonia could cause dyspnea, it usually develops due to an infectious process rather than directly from a femoral head fracture.
Choice C reason:
Airway obstruction involves a blockage that prevents air from passing freely to the lungs. It can be caused by foreign objects, swelling due to allergic reactions, or other medical conditions. The symptoms of airway obstruction include difficulty breathing, wheezing, and potential changes in skin color. However, airway obstruction is not commonly a direct complication of a femoral head fracture.
Choice D reason:
Fat embolism syndrome is a serious condition that occurs when fat globules enter the bloodstream and lodge within the pulmonary vasculature, leading to respiratory distress. It is a known complication following long bone fractures, such as the femur, and presents with symptoms like shortness of breath, hypoxemia, and neurological manifestations. Given the recent femoral head fracture and the symptoms reported, fat embolism syndrome is the most likely diagnosis.
A nurse is organizing care for a patient undergoing chemotherapy and radiation for metastatic breast cancer who also has neutropenia. Which of the following restrictions should the nurse incorporate into the patient's care plan?
Explanation
Choice A reason:
Activities that could result in bleeding should be minimized for a client with neutropenia due to the increased risk of infection from open wounds. However, this is not the primary restriction related to neutropenia itself but rather a general precaution for patients with low platelet counts or other clotting issues.
Choice B reason:
Restricting all visitors from entering the client's room is not necessary unless the visitors are sick or have been exposed to infectious diseases. Neutropenic patients are at increased risk for infection, so visitors should be screened for illness, but complete isolation is not required.
Choice C reason:
Modifying oral fluid intake to between meals only is not a standard restriction for neutropenic patients. Adequate hydration is essential, and there are no specific neutropenia-related reasons to restrict fluids to between meals.
Choice D reason:
Fresh flowers and potted plants should be avoided in the room of a neutropenic patient. They can harbor fungi and other microorganisms that could cause infection in an immunocompromised individual. Neutropenic precautions typically include avoiding standing water and plants that may contain harmful bacteria or fungi.
A nurse is caring for a patient with fibrocystic breasts. The patient asks, "What will happen to my fibrocystic breast changes after menopause?" Which of the following responses would be appropriate for the nurse to provide?
Explanation
Choice A reason:
Telling a client that they will be at an increased risk of breast cancer due to fibrocystic breast changes would be incorrect. Fibrocystic breast changes are not directly linked to an increased risk of breast cancer. While the presence of complex fibrocystic changes may slightly elevate the risk, fibrocystic breasts themselves are a common and benign condition.
Choice B reason:
It is not accurate to say that the manifestations of fibrocystic breasts often get worse after menopause. In fact, fibrocystic changes are related to hormone levels, and most women experience relief from these symptoms after menopause when hormone levels decline.
Choice C reason:
Stating that menopause won't have any effect on the manifestations is also incorrect. Menopause typically leads to a decrease in hormone levels, which are associated with fibrocystic breast changes. Therefore, most women see an improvement in their symptoms after menopause.
Choice D reason:
The most appropriate response is that the manifestations usually go away after menopause. Fibrocystic breast changes are linked to hormonal fluctuations, and after menopause, when these fluctuations cease, the symptoms of fibrocystic breasts typically resolve.
A nurse is caring for a patient with a chronic wound. Which of the following factors is a systemic cause of chronic wounds?
Explanation
Choice A reason:
Venous insufficiency can contribute to the development of chronic wounds, particularly in the lower extremities. It is characterized by the inability of the veins to adequately return blood from the legs back to the heart, which can lead to pooling of blood and increased pressure in the veins. This can cause skin changes and ulcers, particularly around the ankles.
Choice B reason:
Malnutrition is indeed a systemic cause of chronic wounds. Adequate nutrition is essential for wound healing, as it provides the necessary proteins, vitamins, and minerals that play a crucial role in the repair process. Protein-energy malnutrition, deficiencies in vitamins C and D, zinc, and other nutrients can impair wound healing and lead to chronic wounds.
Choice C reason:
Infection is typically a local rather than a systemic cause of chronic wounds. While systemic infections can affect wound healing, local wound infections are more directly responsible for delayed healing and the chronicity of wounds. Bacteria can colonize the wound and impede the healing process, leading to a chronic wound.
Choice D reason:
Continued pressure, much like infection, is generally a local cause of chronic wounds. It is most commonly associated with the development of pressure ulcers in individuals who are bedridden or have limited mobility. The constant pressure on certain areas of the body can lead to tissue ischemia and necrosis, resulting in a chronic wound.
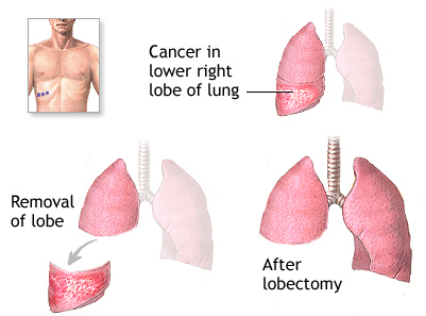
A nurse is caring for a patient with lung cancer who is scheduled for a lobectomy. The nurse should prepare the patient to anticipate which of the following after the procedure?
Explanation
Choice A reason:
While pulmonary function studies are an important part of the preoperative assessment and postoperative follow-up for lung cancer patients, they are not typically something a patient would be immediately prepared for post-lobectomy. These studies are usually scheduled for a later date to assess the impact of the surgery on lung function.
Choice B reason:
A sternal incision is not commonly associated with a lobectomy, which involves an incision in the chest wall, not the sternum. Sternal incisions are more often related to procedures that require access to the heart or the central chest area, such as open-heart surgery.
Choice C reason:
Moderate pain is expected after any major surgical procedure, including a lobectomy. However, pain management is a standard part of postoperative care, and patients are typically informed about pain control measures rather than being prepared to expect pain as a postoperative event.
Choice D reason:
The placement of a chest tube is a standard part of care following a lobectomy. The chest tube allows for drainage of fluid and air from the pleural space, ensuring proper lung expansion and preventing complications such as pneumothorax. Patients should be educated about the chest tube's purpose, care, and the sensations they may experience while the tube is in place.
A nurse is teaching a client who has chronic kidney disease about limiting foods that are high in potassium. Which of the following foods should the nurse instruct the client to avoid? (Select all that apply)
Explanation
Choice A reason:
Raisins are dried grapes and are known to have a higher concentration of nutrients, including potassium. For individuals with chronic kidney disease (CKD), consuming foods like raisins that are high in potassium can lead to hyperkalemia, a condition where potassium levels in the blood are higher than normal. This can be dangerous as it may cause heart rhythm problems.
Choice B reason:
Asparagus is considered a lower-potassium food, making it a safer choice for people with CKD. It's important for individuals with CKD to manage their potassium intake, but asparagus can be included in their diet in appropriate portions.
Choice C reason:
Bananas are well-known for being rich in potassium. For someone with CKD, eating bananas can contribute to an excessive intake of potassium, which their kidneys may not be able to eliminate efficiently, potentially leading to hyperkalemia.
Choice D reason:
Tomatoes, including tomato products like sauces, juices, and purees, are high in potassium. Therefore, they should be limited or avoided in the diet of a person with CKD to prevent complications associated with high potassium levels.
Choice E reason:
Green beans are considered to be a lower-potassium vegetable. They can be included in a kidney-friendly diet, provided they are consumed in moderation and balanced with other dietary needs.
A nurse is caring for a 68-kg (150-lb) patient with dehydration. Which of the following signs indicates that the treatment is effective?
Explanation
Choice A reason:
Lightheadedness is generally not an indication of effective treatment for dehydration. It is often a symptom of dehydration itself, as it can result from decreased blood volume and reduced blood flow to the brain. Effective rehydration should alleviate symptoms like lightheadedness, not present as an indication of it.
Choice B reason:
Decreased pulse pressure may indicate a drop in the volume of blood circulating through the body, which is not a sign of effective rehydration. Pulse pressure is the difference between systolic and diastolic blood pressure readings, and a narrow pulse pressure can be a sign of hypovolemia, or low blood volume, often due to dehydration.
Choice C reason:
Urine output of 75 mL in 1 hr can be considered within the normal range of urine output for an adult, which is typically about 0.5 to 1 mL/kg/hr⁵. This indicates that the kidneys are functioning and the body is excreting waste, suggesting effective rehydration.
Choice D reason:
A urine specific gravity of 1.038 is higher than the normal range of 1.005 to 1.030[^10^]. This indicates concentrated urine, which is commonly seen in dehydration as the body attempts to conserve water. Therefore, this is not an indication of effective treatment for dehydration.
A nurse is caring for a patient who is 1 day postoperative after a left radical mastectomy. Which of the following behaviors should prompt the nurse to consider that the patient may be struggling to adjust to the loss of her breast?
Explanation
Choice A reason:
Asking questions about the information on her postoperative care pamphlet is a positive behavior indicating that the client is proactive in understanding her care and recovery process. It shows engagement and a desire to comply with medical advice, which is beneficial for recovery.
Choice B reason:
Refusing to look at the dressing or surgical incision may indicate psychological distress and difficulty in accepting the physical changes following a mastectomy. This behavior can be a sign of avoidance and a potential struggle with body image and the emotional impact of breast loss. It's important for healthcare providers to recognize this as a call for psychological support and possible referral to counseling services.
Choice C reason:
Performing arm exercises once or twice a day is typically recommended as part of the postoperative care after a mastectomy to prevent stiffness and improve mobility. This behavior suggests that the client is following postoperative instructions and actively participating in her recovery.
Choice D reason:
Asking for pain medication every 3 hours is not necessarily an indication of difficulty adjusting to the loss of a breast. Postoperative pain management is crucial, and regular requests for pain relief are common and appropriate during the initial recovery period. However, if the client seems to be using pain medication to cope with emotional distress rather than physical pain, it may warrant further assessment.
A nurse is educating a group of teenage patients on using condoms to prevent sexually transmitted infections (STIs). Which of the following statements should the nurse include in the instruction?
Explanation
Choice A reason:
The statement about using a natural membrane condom rather than a polyurethane condom is incorrect. Natural membrane condoms, such as those made from lambskin, have small pores that can allow viruses to pass through. Therefore, they are not recommended for the prevention of STIs. Polyurethane condoms, on the other hand, do not have these pores and are considered effective in preventing STIs, including HIV.
Choice B reason:
Female condoms, also known as internal condoms, are effective in preventing the transmission of sexually transmitted viruses, including HIV. They act as a barrier to prevent the exchange of bodily fluids during sexual activity, thereby reducing the risk of STI transmission. It's important to include this information in the teaching as it empowers individuals with an additional option for protection.
Choice C reason:
Condoms are designed for single use only. Using a condom more than once greatly increases the risk of condom failure, which can lead to the transmission of STIs or unintended pregnancy. It is crucial to emphasize the importance of using a new condom for each act of sexual intercourse.
Choice D reason:
Oil-based lubricants should not be used with latex condoms as they can weaken the material, leading to condom breakage. Instead, water-based or silicone-based lubricants are recommended as they do not damage the condom and can help prevent breakage.
A nurse is caring for a patient who complains of low back pain and requests specific exercise recommendations. Which of the following activities should the nurse recommend?
Explanation
Choice A reason:
Tennis may not be the best recommendation for someone with low back pain. The sport requires quick lateral movements, sudden stops, and starts, as well as repetitive twisting motions that can exacerbate back pain. While it provides good general exercise, the high-impact nature of tennis and the strain it puts on the back could potentially worsen the client's condition.
Choice B reason:
Canoeing involves repetitive rowing actions that can strain the lower back, especially if the individual does not use proper form. The seated position in a canoe may also put additional pressure on the lower back. Therefore, it might not be the most suitable activity for someone experiencing low back pain.
Choice C reason:
Rowing, similar to canoeing, can place stress on the lower back due to the repetitive motion and the need for strong engagement of the core muscles. If not performed with proper technique, rowing could lead to increased back pain and is not typically recommended for those with existing low back issues.
Choice D reason:
Swimming is often recommended for individuals with low back pain because it is a low-impact exercise that does not put additional stress on the spine. The buoyancy of the water supports the body, reducing the load on the back while allowing for a full range of motion. Swimming can help strengthen the back muscles and improve flexibility, making it a suitable activity for managing low back pain.
A nurse is reviewing the medical records of patients on a hospital floor. Which patient would the nurse anticipate is at the highest risk for hyperthyroidism
Explanation
Choice A reason:
While metabolic syndrome is associated with several health issues, it is not a direct risk factor for hyperthyroidism. Metabolic syndrome typically includes conditions like insulin resistance, hypertension, and dyslipidemia, which are more closely related to diabetes and cardiovascular diseases rather than thyroid function.
Choice B reason:
An iodine deficiency is commonly associated with hypothyroidism, not hyperthyroidism. Iodine is essential for the production of thyroid hormones, and a lack of it can lead to decreased hormone production and an underactive thyroid.
Choice C reason:
Graves' disease is the most common cause of hyperthyroidism. It is an autoimmune disorder where the immune system mistakenly attacks the thyroid gland, causing it to produce too much thyroid hormone. A 35-year-old male with Graves' disease would indeed be at high risk for hyperthyroidism.
Choice D reason:
While a family history of autoimmune disorders can increase the risk of developing autoimmune-related hyperthyroidism, it is not as direct a risk factor as having Graves' disease itself. Autoimmune disorders can have a genetic component, but having a family history does not guarantee the development of hyperthyroidism.
A nurse is caring for a patient with an unrepaired midshaft femur fracture. Which of the following techniques should the nurse use when assessing the patient's neurovascular status?
Explanation
Choice A reason:
Measuring the circumference of the thigh can be part of the assessment for swelling or edema, which may indicate compartment syndrome or other issues. However, it is not a direct measure of neurovascular status, which focuses on blood flow and nerve function.
Choice B reason:
Palpating the femoral pulse is important for assessing blood flow to the leg, but for a midshaft femur fracture, more distal pulses such as the popliteal, dorsalis pedis, or posterior tibial pulses would be more indicative of the neurovascular status of the affected limb.
Choice C reason:
Monitoring the client's calf for edema is a useful technique for identifying signs of swelling that could suggest complications like deep vein thrombosis or compartment syndrome. However, it does not provide a complete picture of neurovascular integrity, which also includes sensory and motor function assessment.
Choice D reason:
Instructing the client to wiggle his toes is a direct assessment of motor function, which is a key component of neurovascular status. This action, along with checking for sensation and capillary refill, helps to determine if there is any impairment in nerve function or blood supply to the affected area.
A nurse is evaluating a patient with a left lower arm fracture. Which of the following signs suggests impaired venous return in the affected arm?
Explanation
Choice A reason:
Ecchymosis, or bruising, of the surrounding skin is a common finding associated with fractures due to the trauma to blood vessels in the area. While it can indicate bleeding or injury, ecchymosis itself does not specifically indicate impaired venous return.
Choice B reason:
Acute pain is a typical symptom following a fracture and results from the injury to the bone and surrounding tissues. Pain is an expected finding and does not directly suggest an issue with venous return.
Choice C reason:
A bounding distal pulse may actually suggest increased arterial flow or could be a sign of other conditions such as high blood pressure or fever. It does not indicate impaired venous return, which is typically characterized by a lack of pulse or a very weak pulse.
Choice D reason:
Increasing edema, or swelling, in the affected arm is a sign of impaired venous return. When veins are unable to effectively return blood to the heart, fluid can accumulate in the tissues, leading to edema. In the context of a fracture, this could be due to compression or damage to the veins, which can impede blood flow and result in swelling.
A nurse is educating a patient who is preparing for a below-the-knee amputation. Which of the following statements is accurate concerning the postoperative placement of a prosthesis?
Explanation
Choice A reason:
The statement that the prosthesis will be adjustable depending on what shoe you are wearing is not accurate. Prostheses are custom-made to fit the individual and are not typically adjustable to different shoe types. The fit and alignment of the prosthesis are crucial for comfort and function, and these are not dependent on the footwear.
Choice B reason:
It is true that clients will need to do special exercises in advance of getting their prosthesis. These exercises are designed to strengthen the remaining limb and prepare the body for the use of a prosthesis. They are an essential part of rehabilitation and help ensure the best possible outcome for the client.
Choice C reason:
Clients are not fitted for their prosthesis at the time of surgery. Fitting for a prosthesis typically occurs after the residual limb has sufficiently healed, which can take several weeks. The fitting process involves careful measurement and customization to ensure the prosthesis will be comfortable and functional.
Choice D reason:
While a special dressing is applied postoperatively, its primary purpose is not to cushion the prosthesis. Initially, dressings are used to protect the surgical site, control swelling, and promote healing. The prosthesis is fitted after the residual limb has healed, and at that time, different types of socket liners may be used for cushioning.
A nurse is reviewing the BUN and creatinine levels of an older adult patient with chronic kidney disease. The nurse should anticipate which of the following findings?
Explanation
Choice A reason:
A BUN level of 8 mg/dL and a creatinine level of 0.7 mg/dL are within normal ranges for a healthy individual without kidney disease. In chronic kidney disease (CKD), we would expect these values to be elevated due to the kidneys' reduced ability to filter waste products from the blood.
Choice B reason:
A BUN level of 45 mg/dL and a creatinine level of 8 mg/dL are significantly higher than the normal range, which is consistent with impaired kidney function seen in CKD. These elevated levels indicate that the kidneys are not effectively filtering urea and creatinine from the blood, leading to their accumulation.
Choice C reason:
A BUN level of 23 mg/dL and a creatinine level of 1.0 mg/dL could be seen in the early stages of CKD. While the creatinine level is within the normal range, the BUN level is slightly elevated, which may suggest a decline in kidney function.
Choice D reason:
A BUN level of 10 mg/dL and a creatinine level of 0.3 mg/dL are both below the normal range. This is an unlikely finding for a patient with CKD, as kidney impairment typically leads to increased levels of these substances in the blood.
A nurse is caring for a patient whose throat culture tested positive for group A streptococcus 24 hours after a rapid strep test (RST) was negative. What should be the nurse's priority action?
Explanation
Choice A reason:
While gargling with warm saline can provide symptomatic relief for a sore throat, it does not address the underlying bacterial infection. Therefore, it is not the priority action once a diagnosis of group A streptococcus has been confirmed.
Choice B reason:
Identifying close contacts is important for public health tracking and potentially preventing the spread of the infection. However, the immediate priority for the client is the initiation of treatment to address the infection.
Choice C reason:
Taking antipyretics can help manage fever and provide comfort to the client. While managing symptoms is important, it is secondary to initiating antibiotic therapy, which addresses the cause of the symptoms.
Choice D reason:
The priority action is to notify the client to return to the clinic for initiation of antibiotic therapy. Group A streptococcus is a bacterial infection that requires antibiotics for treatment. Prompt initiation of antibiotics is crucial to prevent complications and promote recovery.
A nurse is educating a patient on skin cancer prevention. Which of the following patient statements suggests that further teaching is necessary?
Explanation
Choice A reason:
The statement about eating a high fiber diet reducing the risk for developing skin cancer is misleading. While a high fiber diet has many health benefits, there is no direct evidence that it significantly reduces the risk of skin cancer. Skin cancer prevention primarily focuses on protecting the skin from excessive sun exposure and avoiding ultraviolet (UV) light sources.
Choice B reason:
Avoiding the use of tanning booths is correct advice. Tanning booths emit UV radiation, which can increase the risk of skin cancer, including melanoma, the deadliest form of skin cancer. The use of tanning beds is strongly discouraged by health professionals.
Choice C reason:
Using sunscreen even on cloudy days is also correct. UV rays can penetrate through clouds, and sun protection is necessary regardless of the weather to reduce the risk of skin cancer. Sunscreen should be applied to all exposed skin and reapplied regularly, especially after swimming or sweating.
Choice D reason:
Checking the skin monthly for any changes is an important part of skin cancer prevention. Early detection of changes in moles or new skin growths can lead to early diagnosis and treatment, which is crucial for a better prognosis. This practice should be encouraged as part of routine self-care.
A nurse is reviewing the lab results of a patient after a hemodialysis treatment. The nurse should expect a decrease in which of the following lab values?
Explanation
Choice A reason:
Hemodialysis does not typically result in a significant decrease in RBC count. While there can be a minimal loss of red blood cells during the process, it is not the primary focus of the treatment. The main purpose of hemodialysis is to remove waste products and excess fluid from the blood when the kidneys are not functioning properly.
Choice B reason:
Calcium levels may vary during hemodialysis, and the treatment can be adjusted to prevent significant changes in calcium levels. Hemodialysis can remove some calcium from the blood, but it is usually not the most affected value, and calcium can be added to the dialysate solution if necessary.
Choice C reason:
Potassium is one of the primary electrolytes removed during hemodialysis. High levels of potassium, which can be life-threatening, are commonly seen in clients with renal failure. Hemodialysis effectively reduces high potassium levels, which is crucial for preventing complications such as cardiac arrhythmias.
Choice D reason:
Protein levels are not directly targeted by hemodialysis, and significant protein loss is not a usual outcome of the treatment. The dialysis membrane is designed to allow smaller molecules like urea and potassium to pass through while retaining larger molecules like proteins.
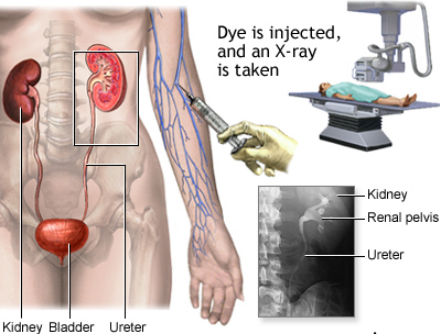
A nurse is preparing to educate a patient who is scheduled for an intravenous pyelogram (IVP). Which of the following statements should the nurse include in the teaching?
Explanation
Choice A reason:
Resuming a regular diet immediately after the test may not always be recommended. Depending on the individual's condition and the specific instructions from the healthcare provider, there may be dietary restrictions before or after the procedure.
Choice B reason:
Encouraging fluid intake after the procedure is important because it helps to flush out the contrast dye used during the IVP. Adequate hydration can aid in the elimination of the dye and reduce the risk of kidney damage, especially in individuals with pre-existing kidney conditions.
Choice C reason:
This statement is incorrect. An IVP does not use high-frequency sound waves; it involves taking X-ray images of the urinary tract after a contrast dye is injected into a vein. The dye outlines the kidneys, ureters, and bladder on the X-ray images.
Choice D reason:
The presence of red blood cells in the urinalysis does not typically result in the cancellation of an IVP. However, certain conditions, such as an allergy to the contrast dye or severe kidney impairment, may contraindicate the use of an IVP.
A nurse is instructing a patient with fibromyalgia on self-care strategies for managing the condition. Which of the following information should the nurse provide?
Explanation
Choice A reason:
Advising to avoid exercise during flare-ups of fibromyalgia can be beneficial. During flare-ups, symptoms such as muscle pain and fatigue are heightened, and rest may be necessary. However, gentle exercises like stretching or water aerobics might still be recommended to maintain muscle flexibility and strength.
Choice B reason:
Establishing a regular sleep pattern is crucial for managing fibromyalgia. Sleep disturbances are common in fibromyalgia, and poor sleep can exacerbate pain and fatigue. Good sleep hygiene, including a consistent sleep schedule and a comfortable sleep environment, can help improve sleep quality and overall symptom management.
Choice C reason:
While regular exercise is important in managing fibromyalgia, jogging or running may not be suitable for all individuals, especially during periods between flare-ups. Low-impact exercises are generally recommended to reduce stress on the joints and muscles.
Choice D reason:
There is no specific recommendation to increase calcium intake as a self-care strategy for fibromyalgia. While maintaining a balanced diet is important, there is no direct link between calcium intake and fibromyalgia symptom management.
A nurse is evaluating a patient after applying a leg cast for a fracture. If the cast is too tight, which of the following symptoms should the nurse expect to notice first?
Explanation
Choice A reason:
The inability to move toes can be an early sign that a cast is too tight. This symptom may indicate that the cast is impinging on nerves or blood vessels, leading to decreased motor function. It is essential to address this immediately to prevent further complications such as permanent damage or compartment syndrome.
Choice B reason:
Edema, or swelling of the toes, can occur if a cast is too tight, but it may not be the first sign observed. Swelling is a response to increased pressure in the tissues and can develop over time as fluid accumulates. While it is a concern, it often follows other symptoms such as changes in sensation or movement.
Choice C reason:
Pallor of the toes, indicating reduced blood flow, can be a sign of a cast that is too tight. However, pallor may not be as immediately noticeable as the inability to move toes or changes in sensation. It is still a critical sign that requires prompt evaluation and possible adjustment of the cast.
Choice D reason:
A change in the temperature of the toes, such as them becoming cooler to the touch, can suggest impaired blood flow due to a tight cast. This sign, along with pallor, may develop after other symptoms such as numbness or motor impairment.
A nurse is caring for a patient with multiple long bone fractures resulting from a motor vehicle crash that occurred 24 hours ago. The patient reports shortness of breath and chest pain. The nurse should further assess the patient for which of the following potential complications?
Explanation
Choice A reason:
Venous thromboembolism (VTE) is a condition where blood clots form in the deep veins, usually in the legs. While VTE is a risk following trauma and immobilization, the acute onset of shortness of breath and chest pain is less typical for VTE, which more commonly presents with leg pain and swelling.
Choice B reason:
Hypovolemic shock occurs due to significant blood or fluid loss, leading to decreased blood volume and inadequate circulation. While it can result from a motor-vehicle crash, the client's symptoms of shortness of breath and chest pain are not the most indicative of hypovolemic shock, which typically presents with rapid pulse, low blood pressure, and cold, clammy skin.
Choice C reason:
Compartment syndrome is a surgical emergency where increased pressure within the muscle compartments impairs circulation and nerve function. It presents with severe pain, swelling, and sometimes paralysis of the affected limb, but it does not typically cause shortness of breath or chest pain.
Choice D reason:
Fat embolism syndrome (FES) is a serious complication that can occur after long bone fractures. Fat globules may enter the bloodstream and travel to the lungs, leading to respiratory distress, which can manifest as shortness of breath and chest pain. FES can also cause neurological symptoms and a petechial rash. Given the client's symptoms and recent trauma, FES is a likely complication and requires immediate assessment and intervention.
A nurse is monitoring a patient who is postoperative after a thyroidectomy. Which of the following information should the nurse recognize as the priority to monitor?
Explanation
Choice A reason:
Monitoring temperature is important postoperatively as it can indicate infection or inflammation. However, it is not the immediate priority following a thyroidectomy. The primary concern post-thyroidectomy is ensuring the airway is not compromised due to swelling or bleeding.
Choice B reason:
Monitoring urination is part of postoperative care to ensure kidney function and that the body is adequately eliminating fluids. While important, it is not the priority in the immediate postoperative period following a thyroidectomy.
Choice C reason:
Pain control is essential for patient comfort and recovery. However, while managing pain is a significant aspect of postoperative care, it is not the most critical priority following a thyroidectomy. The nurse must first ensure that the airway is clear.
Choice D reason:
Airway patency is the priority for monitoring a client post-thyroidectomy. Due to the proximity of the surgery to the trachea, there is a risk of swelling, hematoma, or other complications that could lead to airway obstruction. Ensuring the client has a patent airway is crucial to prevent respiratory distress or compromise.
A nurse is educating a patient with erectile dysfunction who has been prescribed nitroglycerin about dietary supplements. Which of the following statements is the most crucial for the nurse to include in the teaching?
Explanation
Choice A reason:
While it is true that many dietary supplements have not been tested and approved by the government, this is not the most critical information for a client taking nitroglycerin. The primary concern with dietary supplements is their potential interaction with other medications.
Choice B reason:
This is the most important statement for the nurse to include. Dietary supplements, especially those containing L-arginine or other compounds that affect blood flow, can have serious interactions with nitrates like nitroglycerin, potentially leading to dangerously low blood pressure.
Choice C reason:
The effectiveness of dietary supplements for erectile dysfunction varies, and there is indeed a lack of evidence for many of these products. However, the immediate concern for a client taking nitroglycerin is the risk of interaction, not the general effectiveness of supplements.
Choice D reason:
The cost and insurance coverage of dietary supplements can be a concern for clients, but it is not as critical as understanding the potential risks associated with their use alongside prescribed medications like nitroglycerin.
A nurse is reviewing the arterial blood gas values of a patient with chronic kidney disease. Which of the following sets of values should the nurse anticipate?
Explanation
Choice A reason:
This choice suggests a pH of 7.50, which is indicative of alkalosis, and not typically expected in a client with chronic kidney disease (CKD). CKD often leads to metabolic acidosis due to the accumulation of acids in the body as the kidneys fail to excrete them. The HCO₃⁻ level of 20 mEq/L is slightly lower than the normal range (22-26 mEq/L), and the PaCO₂ of 32 mm Hg is within the normal range (35-45 mm Hg), but these values do not align with the expected acidosis associated with CKD.
Choice B reason:
This set of values is consistent with metabolic acidosis, which is commonly seen in clients with CKD. A pH of 7.25 indicates acidemia, and an HCO₃⁻ level of 19 mEq/L is below the normal range, suggesting a primary metabolic acidosis. The PaCO₂ of 30 mm Hg is at the lower end of the normal range, which may indicate a compensatory respiratory response to the metabolic acidosis.
Choice C reason:
A pH of 7.30, while on the lower side, is not as acidic as one would expect in a client with CKD. The HCO₃⁻ level of 26 mEq/L is within the normal range, and a PaCO₂ of 50 mm Hg suggests respiratory acidosis, which is not the primary disorder in CKD.
Choice D reason:
This choice indicates a pH of 7.55, which is too alkaline and not characteristic of CKD, where metabolic acidosis is the expected finding. An HCO₃⁻ level of 30 mEq/L is higher than the normal range, suggesting metabolic alkalosis. The PaCO₂ of 31 mm Hg is slightly below the normal range, possibly indicating a compensatory response, but it does not align with the metabolic acidosis typically seen in CKD.
Sign Up or Login to view all the 135 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
