Ati N 144 Exam 1 Fundamental Concepts for Nursing Practice
Total Questions : 34
Showing 25 questions, Sign in for moreThe nurse is caring for an older adult client who is receiving intravenous fluids at 150 mL/hr. Upon assessment, the nurse notes crackles, shortness of breath, and jugular vein distention. Based on this data, which complication of IV fluid therapy does the nurse anticipate?
Explanation
Choice A reason: Fluid volume deficit is a condition in which the body loses more fluid than it gains, resulting in dehydration, hypotension, and electrolyte imbalances. It is not a complication of IV fluid therapy, but rather a reason for initiating it.
Choice B reason: Fluid volume excess is a condition in which the body retains more fluid than it needs, resulting in edema, hypertension, and heart failure. It is a potential complication of IV fluid therapy, especially in older adults who have reduced renal function and cardiac output. The nurse's assessment findings of crackles, shortness of breath, and jugular vein distention are indicative of fluid overload and pulmonary congestion.
Choice C reason: Speed shock is a systemic reaction that occurs when a substance is administered too rapidly into the bloodstream, causing adverse effects such as chest pain, dyspnea, hypotension, and cardiac arrest. It is not a complication of IV fluid therapy, but rather a risk associated with IV medication administration.
Choice D reason: Pulmonary embolism is a blockage of one or more pulmonary arteries by a blood clot, fat, or air, causing impaired gas exchange, chest pain, dyspnea, and hemoptysis. It is not a complication of IV fluid therapy, but rather a possible outcome of venous thromboembolism, which can be prevented by using anticoagulants and mechanical devices.
What is the main goal for the RN as a teacher?
Explanation
Choice A reason: This is the correct answer because the RN as a teacher aims to promote health literacy, self-management, and shared decision-making among patients and their families. By helping people to become empowered to take care of their health, the RN can facilitate positive health outcomes and prevent complications.
Choice B reason: This is not the correct answer because the RN as a teacher does not focus on explaining what nurses do, but rather on educating patients about their health conditions, treatments, and self-care. While it is important for the patient to understand the role of the nurse, this is not the main goal of teaching.
Choice C reason: This is not the correct answer because the RN as a teacher does not limit teaching to discharge instructions. Teaching is an ongoing process that starts from admission and continues throughout the continuum of care. Discharge instructions are only one component of teaching that summarizes the key information and actions that the patient needs to follow after leaving the hospital.
Choice D reason: This is not the correct answer because the RN as a teacher does not aim to teach patients how to give themselves treatments to get them out of the hospital quicker, but rather to help them achieve optimal health and wellness. Teaching patients how to give themselves treatments is part of the skill development aspect of teaching, but it is not the main goal. The main goal is to help patients understand the rationale, benefits, and risks of their treatments, and to support them in adhering to their treatment plans.
Which of the following clients has a modifiable risk factor for osteoporosis?
Explanation
Choice A reason: William, who exercises three times a week, does not have a modifiable risk factor for osteoporosis. Exercise is actually beneficial for bone health, as it stimulates bone formation and reduces bone loss. Exercise also improves muscle strength, balance, and coordination, which can prevent falls and fractures.
Choice B reason: Samantha, who has a family history of osteoporosis, does not have a modifiable risk factor for osteoporosis. Family history is a genetic factor that cannot be changed or controlled. Having a parent or sibling with osteoporosis increases the risk of developing the condition, especially if they have had a fracture.
Choice C reason: Juanita, who smokes two packs of cigarettes a day, has a modifiable risk factor for osteoporosis. Smoking is a lifestyle factor that can be changed or controlled. Smoking increases the risk of osteoporosis by reducing the blood supply to the bones, decreasing the absorption of calcium, and lowering the levels of estrogen, which protects the bones.
Choice D reason: Tori, who is postmenopausal at age 40, does not have a modifiable risk factor for osteoporosis. Menopause is a natural process that occurs when the ovaries stop producing estrogen, which leads to bone loss and increased risk of fractures. Menopause cannot be prevented or reversed, but its effects on bone health can be managed with hormone therapy, calcium, and vitamin D supplements.
Which statement suggests that the RN understands delegation in the concept of time management?
Explanation
Choice A reason: This is the correct answer because it shows that the RN understands delegation as a way of managing time effectively. Delegation is the process of assigning tasks to other members of the health care team who are competent and qualified to perform them. By working with the LPN and nursing assistant on dividing up patient care tasks, the RN can ensure that the tasks are done safely, efficiently, and according to the scope of practice of each team member.
Choice B reason: This is not the correct answer because it shows that the RN does not understand delegation as a way of managing time effectively. Working overtime until everything is finished is not a sustainable or productive strategy, as it can lead to fatigue, burnout, and errors. The RN should prioritize the tasks that are most important and urgent, and delegate the tasks that can be done by others.
Choice C reason: This is not the correct answer because it shows that the RN does not understand delegation as a way of managing time effectively. Checking to make sure that the tasks are done correctly is part of the supervision and evaluation of delegation, but it is not the main goal of delegation. The main goal of delegation is to optimize the use of resources and skills of the health care team, and to provide quality care to the patients. The RN should trust and respect the abilities of the LPN and nursing assistant, and only intervene if there is a problem or a concern.
Choice D reason: This is not the correct answer because it shows that the RN does not understand delegation as a way of managing time effectively. Completing every nursing intervention or report by the end of the shift is not always possible or realistic, especially in a busy and dynamic health care environment. The RN should focus on the outcomes and quality of care, rather than the quantity of tasks. The RN should also communicate and collaborate with the other members of the health care team, and hand over any unfinished tasks to the next shift.
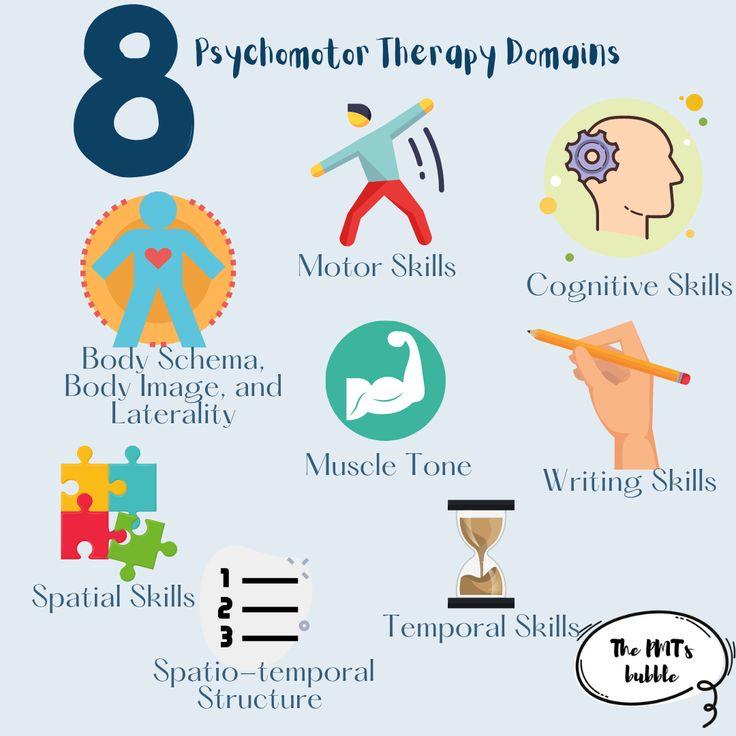
The RN asks the client to demonstrate proper use of his inhaler. This is an example of which domain of learning?
Explanation
Choice A reason: Cognitive domain of learning involves the mental processes of acquiring, storing, and applying knowledge. It includes skills such as remembering, understanding, analyzing, and evaluating. An example of cognitive learning is the RN asking the client to explain the purpose and effects of his inhaler.
Choice B reason: Affective domain of learning involves the emotional aspects of learning, such as attitudes, values, beliefs, and feelings. It includes skills such as receiving, responding, valuing, and committing. An example of affective learning is the RN asking the client how he feels about using his inhaler.
Choice C reason: Psychomotor domain of learning involves the physical aspects of learning, such as movement, coordination, and manipulation. It includes skills such as imitating, practicing, adapting, and creating. An example of psychomotor learning is the RN asking the client to demonstrate proper use of his inhaler.
Choice D reason: Kinesthetic domain of learning is not a recognized domain of learning, but rather a learning style that refers to the preference of learning by doing or experiencing. Kinesthetic learners tend to learn best by engaging in physical activities, such as hands-on tasks, simulations, and experiments.
A client presents in the emergency room with a penetrating eye injury. The object is still present in the eye. Which nursing action is priority?
Explanation
Choice A reason: This is the correct answer because stabilizing the object is the priority nursing action for a penetrating eye injury. Stabilizing the object prevents further damage to the eye structures and reduces the risk of infection and bleeding. The nurse should use a protective shield or cup to cover the eye and secure the object in place, and avoid applying any pressure or movement to the eye.
Choice B reason: This is not the correct answer because applying anesthetic drops is not the priority nursing action for a penetrating eye injury. Anesthetic drops may provide some relief from pain and discomfort, but they do not address the underlying problem of the object in the eye. Anesthetic drops should only be used under the direction of a physician, and after the object has been stabilized.
Choice C reason: This is not the correct answer because removing the object is not the priority nursing action for a penetrating eye injury. Removing the object is a surgical procedure that should only be performed by a qualified physician in a sterile environment. Attempting to remove the object by the nurse may cause more harm to the eye and increase the risk of complications.
Choice D reason: This is not the correct answer because applying eye ointment is not the priority nursing action for a penetrating eye injury. Eye ointment may interfere with the visualization and assessment of the eye, and may also contaminate the wound and cause infection. Eye ointment should only be used under the direction of a physician, and after the object has been stabilized.
A client continues to report post-surgical incision pain at a level of 9 out of 10 after pain medication is given. The next dose of pain medicine is not due for another hour. What should the critically thinking nurse do first?
Explanation
Choice A reason: This is not the correct answer because offering to notify the health care provider after morning rounds are completed is not the first action that the critically thinking nurse should take. The nurse should act promptly and advocate for the patient's pain management needs, rather than delaying the communication with the health care provider.
Choice B reason: This is the correct answer because exploring other options for pain relief is the first action that the critically thinking nurse should take. The nurse should assess the patient's pain level, location, quality, and contributing factors, and use a multimodal approach to pain management that includes pharmacological and non-pharmacological interventions, such as ice, heat, distraction, relaxation, or massage.
Choice C reason: This is not the correct answer because discussing the surgical procedure and reason for the pain is not the first action that the critically thinking nurse should take. The nurse should focus on alleviating the patient's pain, rather than educating the patient about the surgery. The nurse can provide information and reassurance to the patient after the pain is controlled.
Choice D reason: This is not the correct answer because explaining to the patient that nothing else has been ordered is not the first action that the critically thinking nurse should take. The nurse should not dismiss the patient's pain or imply that the patient has no other options for pain relief. The nurse should collaborate with the patient and the health care provider to find the best pain management plan for the patient.
A client is 24 hours post-op after having a colon resection (part of the colon is removed and the healthy ends are sewn back together). His abdominal incision is dry and intact, but the nurse notes that bowel sounds have not returned. What condition is this client likely experiencing?
Explanation
Choice A reason: This is the correct answer because paralytic ileus is a condition in which the intestinal motility is decreased or absent, resulting in the inability to pass gas or stool. It is a common complication of abdominal surgery, as the manipulation of the bowel can cause inflammation and nerve damage. The nurse should monitor the client for signs of bowel obstruction, such as abdominal distension, nausea, vomiting, and pain.
Choice B reason: This is not the correct answer because Clostridium difficile colitis is a condition in which the normal flora of the colon is disrupted by antibiotic therapy, allowing the overgrowth of a toxin-producing bacteria that causes inflammation and diarrhea. It is not a common complication of abdominal surgery, but rather a risk associated with prolonged hospitalization and antibiotic use.
Choice C reason: This is not the correct answer because constipation is a condition in which the stool is hard, dry, and difficult to pass. It is not a common complication of abdominal surgery, but rather a side effect of opioid analgesics, which can slow down the bowel movements. The nurse should encourage the client to increase fluid and fiber intake, and use stool softeners as prescribed.
Choice D reason: This is not the correct answer because fecal impaction is a condition in which a large mass of stool is stuck in the rectum, preventing the passage of gas or stool. It is not a common complication of abdominal surgery, but rather a result of chronic constipation, dehydration, or immobility. The nurse should assess the client for signs of impaction, such as abdominal cramping, rectal pressure, and leakage of liquid stool.
A nurse is educating a client about bariatric surgery. Which of the following statements by the client indicate a need for further teaching?
Explanation
Choice A reason: This is not the correct answer because this statement by the client indicates that the client understands the dietary restrictions and guidelines that are necessary after bariatric surgery. A liquid/pureed diet and limited fluid intake are recommended to prevent complications such as nausea, vomiting, dehydration, and dumping syndrome.
Choice B reason: This is the correct answer because this statement by the client indicates that the client does not understand the importance of a thorough evaluation by the surgeon prior to the procedure. Bariatric surgery is a major surgery that involves significant risks and benefits, and requires careful consideration of the client's medical history, physical condition, psychological status, and readiness for lifestyle changes. The surgeon should assess the client's eligibility, suitability, and expectations for the surgery, and provide informed consent and education.
Choice C reason: This is not the correct answer because this statement by the client indicates that the client understands the basic principles and types of bariatric surgery. Bariatric surgery can be classified into restrictive, malabsorptive, or combined procedures, depending on how they affect the size of the stomach and the absorption of food. The most common types of bariatric surgery are gastric bypass, sleeve gastrectomy, and adjustable gastric banding.
Choice D reason: This is not the correct answer because this statement by the client indicates that the client understands the long-term implications and commitments of bariatric surgery. Bariatric surgery is not a quick fix or a magic solution for obesity, but rather a tool that helps the client achieve and maintain weight loss and improve health outcomes. The client should be aware that bariatric surgery requires lifelong changes in diet, exercise, medication, supplementation, and follow-up care.
The RN has completed an assessment on a client. What should the nurse do next?
Explanation
Choice A reason: This is not the correct answer because reassessing the patient is not the next step after completing an assessment. Reassessment is done periodically or when there is a change in the patient's condition, but not immediately after the initial assessment.
Choice B reason: This is not the correct answer because writing nursing interventions is not the next step after completing an assessment. Nursing interventions are the actions that the nurse plans and implements to achieve the desired outcomes for the patient. They are based on the nursing diagnoses, which are derived from the analysis of the assessment data.
Choice C reason: This is the correct answer because analyzing cues is the next step after completing an assessment. Analysis is the process of identifying patterns, relationships, and trends in the assessment data, and comparing them with the normal and expected findings. Analysis helps the nurse to identify the patient's problems, needs, strengths, and risks.
Choice D reason: This is not the correct answer because creating SMART goals is not the next step after completing an assessment. SMART goals are the specific, measurable, achievable, realistic, and time-bound outcomes that the nurse and the patient agree on. They are based on the nursing diagnoses, which are derived from the analysis of the assessment data.
A nurse in a community health clinic is interviewing a couple who just lost their house in a fire. Using the priority framework of Maslow's hierarchy of needs, which category should the nurse identify for the client's situation?
Explanation
Choice A reason: This is the correct answer because safety is the second level of Maslow's hierarchy of needs, and it includes the needs for security, stability, protection, and freedom from fear and anxiety. The couple who just lost their house in a fire are likely experiencing a threat to their safety needs, as they have lost their shelter, possessions, and sense of security. The nurse should identify and address their safety needs as a priority, and help them find alternative housing, financial assistance, and emotional support.
Choice B reason: This is not the correct answer because self-actualization is the highest level of Maslow's hierarchy of needs, and it includes the needs for personal growth, fulfillment, and realization of one's potential. The couple who just lost their house in a fire are unlikely to be concerned with their self-actualization needs at this time, as they have more pressing and basic needs to meet. The nurse should focus on their lower-level needs first, before helping them achieve their higher-level needs.
Choice C reason: This is not the correct answer because esteem is the fourth level of Maslow's hierarchy of needs, and it includes the needs for self-respect, confidence, recognition, and appreciation. The couple who just lost their house in a fire may experience a loss of esteem, as they may feel ashamed, helpless, or worthless. However, their esteem needs are not the most urgent or important at this time, as they have more fundamental needs to satisfy. The nurse should support their esteem needs by showing empathy, respect, and encouragement, but not neglect their lower-level needs.
Choice D reason: This is not the correct answer because love and belonging is the third level of Maslow's hierarchy of needs, and it includes the needs for affection, intimacy, friendship, and social acceptance. The couple who just lost their house in a fire may benefit from their love and belonging needs, as they may seek comfort, support, and connection from others. However, their love and belonging needs are not the primary or essential at this time, as they have more basic and vital needs to fulfill. The nurse should facilitate their love and belonging needs by providing a caring and compassionate environment, but not overlook their lower-level needs.
The RN receives a call from the lab that a client's potassium chloride (KCl) level is 6.6 (normal range is 3.5 to 5 mEq/L). What should the nurse do first?
Explanation
Choice A reason: This is the correct answer because stopping the KCl infusion is the first and most urgent action that the nurse should take. A high level of potassium in the blood, or hyperkalemia, can cause life-threatening cardiac arrhythmias and muscle weakness. The nurse should stop the source of excess potassium, which is the KCl infusion, and monitor the client's vital signs, electrocardiogram, and symptoms.
Choice B reason: This is not the correct answer because administering oral KCl is not the first or appropriate action that the nurse should take. Oral KCl would increase the potassium level in the blood, which is already too high. The nurse should avoid giving any potassium supplements or foods that are high in potassium, such as bananas, oranges, and potatoes.
Choice C reason: This is not the correct answer because encouraging fluids for dilution is not the first or effective action that the nurse should take. Fluids alone would not lower the potassium level in the blood, but rather dilute the concentration of other electrolytes, such as sodium and calcium. The nurse should administer fluids only as prescribed by the physician, and in conjunction with other treatments, such as diuretics, insulin, or sodium bicarbonate.
Choice D reason: This is not the correct answer because calling the pharmacy is not the first or priority action that the nurse should take. Calling the pharmacy may be necessary to obtain the medications that can lower the potassium level in the blood, such as diuretics, insulin, or sodium bicarbonate. However, the nurse should first stop the KCl infusion and notify the physician, who will order the appropriate medications and dosages.
A nurse is reinforcing teaching with a young adult client who has a family history of osteoporosis. Which of the following health promotion activities should the nurse recommend?
Explanation
Choice A reason: Weight-bearing exercise, such as walking, jogging, or dancing, helps to strengthen the bones and prevent osteoporosis. It also improves muscle strength, balance, and coordination, which can reduce the risk of falls and fractures.
Choice B reason: Having a bone density scan every year is not necessary for a young adult client who has a family history of osteoporosis. A bone density scan is a test that measures the amount of calcium and other minerals in the bones. It is usually recommended for women over 65 years old, men over 70 years old, or people who have risk factors for osteoporosis, such as low body weight, smoking, or steroid use.
Choice C reason: Taking a magnesium supplement every day is not a proven way to prevent osteoporosis. Magnesium is a mineral that is involved in bone formation and metabolism, but there is not enough evidence to support its role in preventing or treating osteoporosis. A balanced diet that includes foods rich in calcium, vitamin D, and other nutrients is more effective for bone health.
Choice D reason: Drinking a cup of coffee every morning is not a good idea for a young adult client who has a family history of osteoporosis. Coffee contains caffeine, which can interfere with the absorption of calcium and increase the excretion of calcium in the urine. This can lead to lower bone density and higher risk of osteoporosis. Moderate coffee consumption (one or two cups per day) may not have a significant effect on bone health, but excessive coffee intake (more than four cups per day) should be avoided.
The nurse notes that an elderly client has a history of osteoporosis. What safety measure should the nurse prioritize for this client?
Explanation
Choice A reason: Fall prevention is the most important safety measure for an elderly client with osteoporosis, as falls can result in fractures and other complications. The nurse should assess the client's risk factors for falls, such as impaired vision, balance, or mobility, and implement interventions to reduce them, such as providing adequate lighting, removing clutter, and using assistive devices.
Choice B reason: Pressure injury prevention is also important for an elderly client, but not as crucial as fall prevention for a client with osteoporosis. Pressure injuries are caused by prolonged pressure on the skin, especially over bony prominences. The nurse should reposition the client frequently, use pressure-relieving devices, and monitor the skin for signs of breakdown.
Choice C reason: Cognitive impairment prevention is not a specific safety measure for an elderly client with osteoporosis, although it may affect the client's ability to follow instructions and adhere to treatment. Cognitive impairment may be caused by various factors, such as dementia, delirium, or medication side effects. The nurse should assess the client's mental status, provide orientation and stimulation, and manage any underlying causes.
Choice D reason: Functional decline prevention is not a specific safety measure for an elderly client with osteoporosis, although it may affect the client's quality of life and independence. Functional decline may be caused by various factors, such as pain, weakness, or depression. The nurse should encourage the client to participate in physical and occupational therapy, promote self-care activities, and provide emotional support.
A nurse administers an antihypertensive medication to a patient at the scheduled time of 0900. The nursing assistant then reports to the nurse that the patient's blood pressure was low when it was taken at 0830. The patient begins to complain of feeling dizzy and light-headed. The blood pressure is re-checked and it has dropped even lower. The nurse first made an error in what phase of the nursing process?
Explanation
Choice A reason: Assessment is the first and most important phase of the nursing process, as it involves collecting and analyzing data about the patient's health status, needs, and preferences. The nurse should have assessed the patient's blood pressure before administering the antihypertensive medication, as it could have been contraindicated or required a dosage adjustment. By failing to do so, the nurse put the patient at risk of hypotension and its complications.
Choice B reason: Planning is the second phase of the nursing process, in which the nurse sets goals and outcomes for the patient's care and selects appropriate interventions. The nurse did not make an error in this phase, as the administration of the antihypertensive medication was part of the plan of care for the patient with hypertension.
Choice C reason: Diagnosis is the third phase of the nursing process, in which the nurse identifies the patient's actual or potential health problems based on the assessment data. The nurse did not make an error in this phase, as the diagnosis of hypertension was accurate and supported by the patient's history and vital signs.
Choice D reason: Evaluation is the fourth and final phase of the nursing process, in which the nurse measures the patient's progress and outcomes and modifies the plan of care as needed. The nurse did not make an error in this phase, as the re-checking of the blood pressure and the recognition of the patient's symptoms were part of the evaluation process. However, the nurse should have also notified the provider and implemented interventions to treat the hypotension.
A nurse is talking with a client who has osteoporosis and needs to increase her vitamin D intake as part of her treatment plan. Which of the following recommendations should the nurse reinforce with the client to help ensure an adequate intake of vitamin D?
Explanation
Choice A reason: Vitamin D is a fat-soluble vitamin that helps the body absorb calcium and phosphorus, which are essential for bone health. The main source of vitamin D is exposure to sunlight, which triggers the skin to produce it. The nurse should advise the client to spend at least 15 minutes outdoors every day, preferably in the morning or evening, when the sun is not too strong. The client should also wear sunscreen and protective clothing to prevent sunburn and skin damage.
Choice B reason: Reducing the amount of cereal in the diet is not a good recommendation for increasing vitamin D intake. Cereal is often fortified with vitamin D and other nutrients, such as iron and folic acid. The nurse should encourage the client to choose cereals that are high in vitamin D and low in sugar and fat. The client should also consume other foods that are rich in vitamin D, such as fatty fish, egg yolks, cheese, and mushrooms.
Choice C reason: Increasing intake of dietary calcium is important for preventing and treating osteoporosis, but it does not directly affect vitamin D intake. Calcium is a mineral that helps build and maintain strong bones and teeth. The nurse should recommend the client to consume foods that are high in calcium, such as dairy products, leafy greens, nuts, and tofu. The client should also take a calcium supplement if needed, as prescribed by the provider.
Choice D reason: Adding a regular exercise routine is beneficial for improving overall health and well-being, but it does not directly influence vitamin D intake. Exercise helps strengthen the muscles and bones, prevent falls and fractures, and reduce the risk of chronic diseases. The nurse should suggest the client to engage in moderate physical activity for at least 30 minutes a day, three times a week. The client should choose exercises that are appropriate for their age and fitness level, such as walking, swimming, or yoga.
Identify which client could be considered to be in a state of wellness?
Explanation
Choice A reason: A teacher who notices a mole change but doesn't have time to see a dermatologist is not in a state of wellness. A mole change could indicate skin cancer, which is a serious health problem that requires prompt medical attention. Ignoring or delaying the diagnosis and treatment of skin cancer could compromise the teacher's physical and emotional well-being.
Choice B reason: A fitness trainer who is struggling to cope with the death of her mother is not in a state of wellness. The death of a loved one is a major life stressor that can affect the fitness trainer's mental and emotional health. Grieving is a normal and healthy process, but it can also interfere with the fitness trainer's daily functioning and quality of life. The fitness trainer may need professional help or support from family and friends to cope with the loss.
Choice C reason: A hospice client who is comfortable and at peace with dying is in a state of wellness. Wellness is not only the absence of disease, but also the presence of positive health behaviors and attitudes. A hospice client who is comfortable and at peace with dying has accepted the reality of their condition and has made peace with themselves and others. The hospice client may also receive palliative care, which aims to relieve pain and suffering and improve the quality of life for terminally ill patients and their families.
Choice D reason: A type 1 diabetic who gives himself extra insulin so he can eat cookies is not in a state of wellness. A type 1 diabetic who gives himself extra insulin so he can eat cookies is engaging in unhealthy and risky behavior that could harm his physical health. Extra insulin could cause hypoglycemia, which is a condition where the blood sugar level drops too low and can lead to seizures, coma, or death. Eating cookies could also increase the blood sugar level and contribute to complications such as nerve damage, kidney damage, or cardiovascular disease. A type 1 diabetic who wants to eat cookies should follow a balanced diet and monitor his blood sugar level regularly.
A client has chronic back pain from a work-related injury that occurred 5 years ago. Which patient goal meets the SMART criteria?
Explanation
Choice A reason: The client will be able to return to work is not a SMART goal. SMART stands for Specific, Measurable, Achievable, Relevant, and Time-bound. This goal is not specific, as it does not state what kind of work the client will do, or how the client's back pain will affect their work performance. It is also not measurable, as it does not state how the client's work ability will be assessed. It may not be achievable, as the client's work-related injury may prevent them from returning to their previous occupation. It may not be relevant, as the client may have other priorities or preferences than work. It is also not time-bound, as it does not state when the client will return to work.
Choice B reason: The client will verbalize diminished pain at the conclusion of physical therapy is not a SMART goal. This goal is not specific, as it does not state how much pain the client will experience, or what level of pain is acceptable for the client. It is also not measurable, as it relies on the client's subjective report of pain, which may vary depending on the client's mood, expectations, or coping skills. It may not be achievable, as the client's chronic back pain may not be fully resolved by physical therapy. It may not be relevant, as the client may have other outcomes or indicators of improvement than pain. It is also not time-bound, as it does not state how long the physical therapy will last, or when the client will verbalize their pain level.
Choice C reason: The client will be able to perform self-care is not a SMART goal. This goal is not specific, as it does not state what aspects of self-care the client will perform, or how the client's back pain will affect their self-care abilities. It is also not measurable, as it does not state how the client's self-care performance will be evaluated. It may not be achievable, as the client's chronic back pain may limit their range of motion, strength, or endurance for self-care tasks. It may not be relevant, as the client may have other goals or needs than self-care. It is also not time-bound, as it does not state when the client will achieve this goal.
Choice D reason: The client will engage in desired activities without the pain level increasing above a pain scale level of 3 out of 10 within one month is a SMART goal. This goal is specific, as it states what activities the client wants to do, and how the client's pain level will be monitored. It is measurable, as it uses a numeric pain scale that can be easily recorded and compared. It is achievable, as it sets a realistic and attainable pain threshold that allows the client to enjoy their activities. It is relevant, as it reflects the client's personal interests and values, and enhances their quality of life. It is time-bound, as it states a clear and reasonable deadline for achieving this goal.
A patient at a long-term care facility makes the following statements regarding management of his constipation. Which statement would require follow-up teaching by the nurse?
Explanation
Choice A reason: I try to walk in the hallway each day with assistance is a correct statement. Walking is a form of physical activity that can stimulate bowel movements and prevent constipation. Walking also has other benefits such as improving circulation, muscle strength, and mood. The patient should be encouraged to walk as much as possible with assistance to prevent falls and injuries.
Choice B reason: I need to increase fiber in my diet and drink more water is a correct statement. Fiber is a type of carbohydrate that is not digested by the body and helps to form soft and bulky stools. Fiber can be found in foods such as fruits, vegetables, whole grains, nuts, and seeds. Water is essential for hydration and helps to soften the stools and ease their passage. The patient should be advised to consume at least 25 grams of fiber and 8 glasses of water per day to prevent constipation.
Choice C reason: I take my laxative every morning and an enema every night is an incorrect statement that requires follow-up teaching by the nurse. Laxatives and enemas are medications that are used to treat constipation by stimulating or lubricating the bowel. However, they should not be used routinely or excessively, as they can cause side effects such as dehydration, electrolyte imbalance, abdominal cramps, diarrhea, or dependence. The patient should be instructed to use laxatives and enemas only as prescribed by the doctor and for a short period of time. The patient should also be informed of the potential risks and complications of overusing laxatives and enemas.
Choice D reason: The pain medication I take tends to make my constipation worse is a correct statement. Pain medications, especially opioids, can slow down the movement of the bowel and cause constipation. This is a common and expected side effect of pain medications. The patient should be educated on how to manage constipation caused by pain medications, such as increasing fiber and water intake, exercising regularly, and using stool softeners or laxatives as needed. The patient should also be reassured that constipation does not mean that the pain medication is not working or that they are addicted to it.
The RN is using clinical judgment to determine which patient she needs to see first. What is one primary reason for prioritizing care?
Explanation
Choice A reason: Nurses can accomplish more if they perform the easiest or fastest interventions is not a primary reason for prioritizing care. This statement implies that nurses should focus on the quantity rather than the quality of care. However, nurses should prioritize care based on the urgency and complexity of the patient's needs, not on the ease or speed of the interventions. Performing the easiest or fastest interventions may not address the most important or critical issues that the patient faces.
Choice B reason: Nurses should always perform interventions related to client preference early in the shift is not a primary reason for prioritizing care. This statement implies that nurses should base their care on the patient's wishes rather than the patient's condition. However, nurses should prioritize care based on the severity and acuity of the patient's problems, not on the patient's preference. Performing interventions related to client preference early in the shift may not be feasible or appropriate if the patient has more urgent or emergent needs that require immediate attention.
Choice C reason: Nurses need to plan how to accomplish all activities within one shift is not a primary reason for prioritizing care. This statement implies that nurses should focus on the completion rather than the quality of care. However, nurses should prioritize care based on the significance and impact of the patient's outcomes, not on the completion of the activities. Accomplishing all activities within one shift may not be possible or necessary if the patient's situation changes or if some activities can be delegated or postponed.
Choice D reason: Nurses have a limited amount of time to perform nursing interventions during a shift is a primary reason for prioritizing care. This statement acknowledges that nurses face time constraints and competing demands in their work environment. Therefore, nurses should prioritize care based on the best use of their time and resources to meet the patient's needs. Having a limited amount of time to perform nursing interventions during a shift requires nurses to make clinical judgments and decisions that optimize the patient's health and safety.
A person is experiencing stress because they are worried about passing their driver's license test tomorrow. This is an example of what type of stress?
Explanation
Choice A reason: Environmental stress is not the correct answer. Environmental stress is caused by external factors that are beyond the person's control, such as noise, pollution, weather, or natural disasters. These factors can affect the person's physical and mental health, but they are not related to the person's specific situation or event.
Choice B reason: Situational stress is the correct answer. Situational stress is caused by a particular situation or event that the person faces, such as a test, a job interview, a conflict, or a loss. These situations or events can create pressure, uncertainty, or anxiety for the person, and they may require the person to adapt or cope with the change or challenge.
Choice C reason: Daily Hassle stress is not the correct answer. Daily Hassle stress is caused by the minor annoyances or frustrations that the person encounters in their everyday life, such as traffic, deadlines, bills, or household chores. These hassles can accumulate and affect the person's mood, health, or well-being, but they are not related to the person's specific situation or event.
Choice D reason: Episodic stress is not the correct answer. Episodic stress is caused by frequent or chronic exposure to stressful situations or events, such as work overload, financial problems, or family issues. These situations or events can create a constant state of worry, agitation, or distress for the person, and they may affect the person's physical and mental health. Episodic stress is not a type of stress, but rather a result of experiencing too much stress over a long period of time.
A person is experiencing stress because they are worried about passing their driver's license test tomorrow. This is an example of what type of stress?
Explanation
Choice A reason: Environmental stress is not the correct answer. Environmental stress is caused by external factors that are beyond the person's control, such as noise, pollution, weather, or natural disasters. These factors can affect the person's physical and mental health, but they are not related to the person's specific situation or event.
Choice B reason: Situational stress is the correct answer. Situational stress is caused by a particular situation or event that the person faces, such as a test, a job interview, a conflict, or a loss. These situations or events can create pressure, uncertainty, or anxiety for the person, and they may require the person to adapt or cope with the change or challenge.
Choice C reason: Daily Hassle stress is not the correct answer. Daily Hassle stress is caused by the minor annoyances or frustrations that the person encounters in their everyday life, such as traffic, deadlines, bills, or household chores. These hassles can accumulate and affect the person's mood, health, or well-being, but they are not related to the person's specific situation or event.
Choice D reason: Episodic stress is not the correct answer. Episodic stress is caused by frequent or chronic exposure to stressful situations or events, such as work overload, financial problems, or family issues. These situations or events can create a constant state of worry, agitation, or distress for the person, and they may affect the person's physical and mental health. Episodic stress is not a type of stress, but rather a result of experiencing too much stress over a long period of time.
Which intervention is an example of the RN working in a health promotion role through primary prevention?
Explanation
Choice A reason: Administering a vaccine to a well child is an example of the RN working in a health promotion role through primary prevention. Primary prevention is the level of prevention that aims to prevent disease or injury before it occurs. It involves reducing exposure to risk factors and enhancing protective factors. Vaccination is a primary prevention strategy that protects the child from contracting or spreading infectious diseases, such as measles, polio, or tetanus.
Choice B reason: Obtaining a blood glucose level on a client with hypoglycemia (low blood sugar) is not an example of the RN working in a health promotion role through primary prevention. This is an example of the RN working in a disease management role through tertiary prevention. Tertiary prevention is the level of prevention that aims to reduce the complications and disability associated with chronic or irreversible diseases or injuries. It involves providing treatment, rehabilitation, and support services. Obtaining a blood glucose level on a client with hypoglycemia is a tertiary prevention strategy that monitors the client's condition and prevents further deterioration or complications, such as coma or seizures.
Choice C reason: Educating a patient on wound care is not an example of the RN working in a health promotion role through primary prevention. This is an example of the RN working in a disease management role through secondary prevention. Secondary prevention is the level of prevention that aims to detect and treat diseases or injuries early, before they become more serious or chronic. It involves screening, diagnosis, and intervention. Educating a patient on wound care is a secondary prevention strategy that helps the patient to prevent infection, promote healing, and avoid complications, such as scarring or gangrene.
Choice D reason: Administering a nebulizer treatment to a client with asthma is not an example of the RN working in a health promotion role through primary prevention. This is an example of the RN working in a disease management role through tertiary prevention. Tertiary prevention is the level of prevention that aims to reduce the complications and disability associated with chronic or irreversible diseases or injuries. It involves providing treatment, rehabilitation, and support services. Administering a nebulizer treatment to a client with asthma is a tertiary prevention strategy that helps the client to relieve symptoms, improve lung function, and prevent exacerbations, such as asthma attacks.
Physiological response to fear and anxiety includes which of the following?
Explanation
Choice A reason: Tachycardia is a physiological response to fear and anxiety. Tachycardia is a condition where the heart rate is faster than normal, usually above 100 beats per minute. Fear and anxiety can trigger the release of stress hormones, such as adrenaline and cortisol, that stimulate the sympathetic nervous system. This causes the heart to beat faster and stronger, increasing the blood flow and oxygen delivery to the muscles and organs. This prepares the body for the fight-or-flight response, which is a survival mechanism that helps the person to cope with a perceived threat or danger.
Choice B reason: Bronchial constriction is not a physiological response to fear and anxiety. Bronchial constriction is a condition where the airways in the lungs become narrow and inflamed, reducing the airflow and causing difficulty breathing. Bronchial constriction can be caused by various factors, such as asthma, allergies, infections, or irritants. Fear and anxiety can worsen the symptoms of bronchial constriction, but they are not the primary cause of it.
Choice C reason: Bradypnea is not a physiological response to fear and anxiety. Bradypnea is a condition where the breathing rate is slower than normal, usually below 12 breaths per minute. Bradypnea can be caused by various factors, such as brain injury, drug overdose, sleep apnea, or metabolic disorders. Fear and anxiety can increase the breathing rate, not decrease it, as the body needs more oxygen to cope with the stress.
Choice D reason: Pupillary constriction is not a physiological response to fear and anxiety. Pupillary constriction is a condition where the pupils in the eyes become smaller and less responsive to light. Pupillary constriction can be caused by various factors, such as eye injury, medication, aging, or neurological disorders. Fear and anxiety can cause pupillary dilation, not constriction, as the pupils widen to allow more light and improve the vision. This helps the person to see better and react faster to the situation.
A nurse on a medical-surgical unit knows that for clients with a BMI greater than or equal to 30, it is important to:
Explanation
Choice A reason: Utilize supine positioning to maximize chest expansion is not an important intervention for clients with a BMI greater than or equal to 30. Supine positioning is when the client lies flat on their back. This position can actually impair chest expansion and breathing for clients with a high BMI, as the weight of the abdomen and chest can compress the lungs and diaphragm. A semi-Fowler's position, where the head of the bed is elevated at 30 to 45 degrees, is preferred for these clients, as it reduces the pressure on the chest and improves ventilation.
Choice B reason: Use an appropriately sized blood pressure cuff is an important intervention for clients with a BMI greater than or equal to 30. A blood pressure cuff that is too small or too tight can cause inaccurate readings and increase the risk of injury to the client. A blood pressure cuff that is too large or too loose can also cause inaccurate readings and compromise the quality of care. A blood pressure cuff that fits the client's arm circumference and width is essential for obtaining accurate and reliable measurements and preventing complications.
Choice C reason: Consult a nutritionist because the client is malnourished/underweight is not an important intervention for clients with a BMI greater than or equal to 30. A BMI greater than or equal to 30 indicates that the client is obese, not malnourished or underweight. Obesity is a condition where the client has excess body fat that can affect their health and well-being. Malnutrition is a condition where the client has inadequate or imbalanced intake of nutrients that can affect their growth and development. Underweight is a condition where the client has a low body weight that can affect their immunity and energy. A nutritionist can help clients with any of these conditions, but the statement is incorrect for clients with a high BMI.
Choice D reason: Place the client on fall precautions because of increased risk for falls due to frail bones is not an important intervention for clients with a BMI greater than or equal to 30. Frail bones are not a common consequence of obesity, but rather of osteoporosis, a condition where the bones become weak and brittle. Obesity can actually increase the bone density and strength, as the bones have to support more weight. However, obesity can increase the risk for falls due to other factors, such as impaired mobility, balance, or coordination. Fall precautions are important for any client who is at risk for falls, but the statement is inaccurate for clients with a high BMI.
Sign Up or Login to view all the 34 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
