ATI ns 130 Exam Psychosocial
Total Questions : 50
Showing 25 questions, Sign in for moreCommon problems in a therapeutic relationship include all of the following except
Explanation
Choice A rationale: The client is not a problem in a therapeutic relationship but is instead the focus of care and their needs and preferences be considered in their care process.
Therefore, the client should also be encouraged to participate actively in the treatment and to provide feedback on the progress and challenges.
Choice B rationale: The environment, including issues like noise, interruptions, or lack of privacy, can impact the effectiveness of therapeutic interactions.
Choice C rationale: Financial resources, for instance, lack of insurance coverage, high costs of healthcare, and limited access to quality healthcare can impair effective patient care resulting in stress and frustration for the patient.
Choice D rationale: The caregiver's own challenges, such as burnout, communication issues, and lack of knowledge, skills, and experience can impair the quality of care provided to a client thus affecting the therapeutic relationship.
Prozac 30mg PO is ordered for a client. Prozac is available in 10mg tablets. How many tablets will you administer?
Explanation
3 tablets
To calculate the number of tablets needed, divide the total prescribed dose by the strength of each tablet. In this case, 30mg / 10mg per tablet = 3 tablets.
The nurse is administering medications to a client with a diagnosis of depression. The nurse would expect to see which medication was ordered for this client.
Explanation
Choice A rationale: Crestor (Rosuvastatin) is a statin used for lowering cholesterol levels, not for treating depression.
Choice B rationale: Seroquel (Quetiapine) is an atypical antipsychotic used for various mental health conditions such as schizophrenia, bipolar disorder, and major depressive disorder. However, it is not a first-line treatment for depression.
Choice C rationale: Paxil (Paroxetine) is an antidepressant commonly used in the treatment of depression and other mood disorders. It belongs to the selective serotonin reuptake inhibitor (SSRI) class of medications.
Choice D rationale: Latuda (Lurasidone) is an atypical antipsychotic used in certain psychiatric conditions such as schizophrenia and bipolar depression but is not typically a first-line treatment for depression.

When communicating with an angry patient; the nurse must first:
Explanation
Choice A rationale: This is an important step but it comes second after actively listening to the patient. Understanding the underlying emotions allows the nurse to respond appropriately and address the patient's concerns effectively. By identifying the emotions, the nurse can establish a foundation for constructive communication and work towards resolving the source of anger.
Choice B rationale: Listening actively is an important component of effective communication and it entails paying attention to the client's verbal and non-verbal cues. This shows empathy and an interest in the patient’s concerns.
Choice C rationale: Exploring options is relevant, but it is a subsequent step in the communication process after active listening and identifying emotions.
Choice D rationale: this is inappropriate especially when dealing with an angry patient as it may sound patronizing, insincere, and dismissive.
One of the major disadvantages of benzodiazepines prescribed for anxiety is that these medications:
Explanation
Choice A rationale: Benzodiazepines typically have a relatively rapid onset of action, usually within a few minutes to hours after taking the drug hence making them effective for the management of anxiety and panic attacks.
Choice B rationale: While benzodiazepines may have side effects, serious side effects are not a major disadvantage when compared to the risk of dependency.
Choice C rationale: Benzodiazepines are a well-researched class of medications and are not considered "new to the market since they have been in use since the 1960s.
Choice D rationale: Benzodiazepines have the potential for dependency and tolerance with long-term use. They are generally recommended for short-term use due to the risk of developing a physical and psychological dependence hence the drug should only be used under the guidance of a qualified healthcare professional.

During an admission assessment, a male client states that he has been having auditory hallucinations and difficulty concentrating at work. This type of data is referred to as:
Explanation
Choice A rationale: Measured data involves quantitative information obtained through measurement and observation, not the client's self-report.
Choice B rationale: Objective data is observable and measurable, often obtained through physical examination or direct observation.
Choice C rationale: Shared data is not a commonly used term in the context of describing information provided by a client. However, it could refer to information that is communicated or exchanged between the nurse and healthcare professionals.
Choice D rationale: Subjective data refers to information provided by the client based on their own feelings, perceptions, or experiences. In this case, the client's statement about auditory hallucinations and difficulty concentrating represents subjective data.
During the night shift, several staff members are being loud at the nurses' station of an inpatient mental health unit. A nurse asks them to hold down the noise." The nurse has asked this of the staff most likely because she knows that excessive noise
Explanation
Choice A rationale: Excessive noise does impact the professional environment, but the primary concern is its potential impact on clients rather than the appearance of the mental health unit.
Choice B rationale: Excessive noise is more likely to disturb clients by causing insomnia and irritability rather than promoting relaxation.
Choice C rationale: Excessive noise in a mental health unit can disrupt the therapeutic environment and interfere with clients' thinking processes and perceptions by triggering anxiety, aggression, and anxiety. Therefore, maintaining a calm and quiet atmosphere supports mental health treatment.
Choice D rationale: There is no indication that excessive client noise is encouraged by the staff. However, the main concern is the impact of the staff noise on clients.
The nurse who is caring for a client begins to have very protective feelings toward the client that are interfering with the therapeutic relationship between the nurse, the client, and the client's family. This is an example of a problem that is encountered in some therapeutic relationships and is known as:
Explanation
Choice A rationale: Transference involves the client projecting feelings or attitudes onto the healthcare provider and can affect the therapeutic relationship.
Choice B rationale: Environmental problems are external issues arising from the individual’s physical and social setting such as interruptions and noise and can affect the therapeutic environment, not the nurse's emotional responses.
Choice C rationale: Resistance refers to the situation where the client consciously or unconsciously opposes or is reluctant to engage in therapeutic interventions and hinders treatment progress and outcomes.
Choice D rationale: Countertransference occurs when the healthcare provider projects their feelings and emotions, experiences, or unresolved issues onto the client. The nurse's overprotective feelings interfere with the objectivity and effectiveness of the therapeutic relationship.
During the mental status assessment, the nurse hands the client a piece of paper that reads "Please raise your left hand." If the client follows the command, the nurse has just assessed which ability of the client
Explanation
Choice A rationale: Abstract thinking involves the ability to think conceptually and comprehend concrete concepts such as proverbs.
Choice B rationale: Memory assesses the client’s ability to recall previously experienced or learned information and is not directly assessed by the client's ability to follow a written command.
Choice C rationale: General knowledge refers to the ability of a client to answer questions on common topics and facts and is not assessed by the client's response to a written command.
Choice D rationale: The ability to follow a written command, such as "Please raise your left hand," assesses the client's ability to read and understand written instructions.
Upon entrance into a mental health care system, clients are thoroughly assessed, and this is followed by the development of a mental health treatment plan. Which of the following are the purposes of the treatment plan? (Select all that apply.)
Explanation
Choice A rationale: the mental health treatment is designed to monitor and assess an individual’s progress and response to treatment over time by outlining measurable and realistic targets that are evaluated periodically.
Choice B rationale: the treatment plan can be used by healthcare providers as a guide while providing care to their clients by issuing a clear rationale behind the interventions chosen.
Choice C rationale: the treatment plan is a document outlining the objectives, interventions, and expected outcomes in the management of clients thus it serves as a communication tool amongst various healthcare providers across all the cadres involved in multi-disciplinary patient care.
Choice D rationale: the treatment plan evaluates the effectiveness of the interventions provided to a client by providing a comparison between the actual results and the expected outcomes thus guiding on the need for any necessary adjustments to be made when needed.
Choice E rationale: the treatment plan is not primarily responsible for ensuring that a client adheres to their treatment but instead it empowers and supports them during their recovery process. Therefore, the client’s needs and preferences should always be considered while developing the treatment plan which should be flexible to the changing needs of clients.
A client in the mental health unit has a history of Asthma. Which axis would the nurse document this information?
Explanation
Choice A rationale: Axis 3 is used in the documentation of conditions, for instance, asthma, hypertension, and diabetes mellitus among others which are known to have effects on an individual’s mental health.
Choice B rationale: Axis 2 is used in the documentation of conditions affecting a client’s functioning such as personality disorders and mental retardation.
Choice C rationale: Axis 4 is used in the documentation of environmental and psychosocial issues contributing to a patient’s stress such as financial and family stressors.
Choice D rationale: Axis 1 is used to document clinical disorders that are the primary focus of management such as schizophrenia, major depressive disorder, and bipolar disorder among others.
What is the therapeutic range of Lithium (Eskalith)?
Explanation
Choice A rationale: The therapeutic range of lithium is generally considered to be 0.6-1.5 mEq/L. However, some patients may require higher or lower levels depending on their individual response to the medication and their clinical condition. Lithium has a narrow therapeutic range hence the blood level of the drug should be closely monitored to minimize the risk of toxicity and sub-therapeutic effects.
Choice B rationale: 0.1-0.5 is too low hence the drug will provide sub-optimal effects thus providing inadequate mood stabilization.
Choice C rationale: 0.2-0.5 is too low hence the drug will provide sub-optimal effects thus providing inadequate mood stabilization.
Choice D rationale: 0.4-1.6 the lower limit is too low and may result in sub-therapeutic effects while the upper limit is too high and increases the risk of lithium toxicity which can manifest as nausea, vomiting, tremors, seizures, and death in severe cases.
Which medication side effect is irreversible if not caught early:
Explanation
Choice A rationale: Akathisia refers to restlessness and agitation and is a common side effect of antipsychotic medications. This condition can be reversed by reducing the dose of antipsychotic medication taken by the client.
Choice B rationale: Tardive dyskinesia refers to the involuntary movement of body parts such as the limbs, face, jaw, and tongue and is a common side effect of long-term use of first-generation antipsychotic medications which work by blocking dopamine receptors. This condition is irreversible, especially when not detected early.
Choice C rationale: Dystonia which refers to muscle spasms affecting the jaw, eyes, and limbs can be reversed by the use of anticholinergic medications or botulin toxin.
Choice D: Akinesia refers to the absence of movement and can be managed by adjusting the dosage of the antipsychotic medications being taken by the patient.

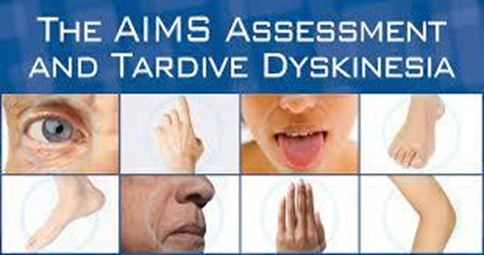
Which assessment tool is used to monitor clients for Tardive Dyskinesia?
Explanation
Choice A rationale: The AIMS Scale refers to the Abnormal Involuntary Movement Scale and is used in the assessment of patients for the presence of involuntary movements across body regions. The score ranges from zero which denotes the absence of dyskinesia and four which stands for severe, maximal amplitude and persistence of the abnormal movements during the examination period. It is also used to monitor clients with tardive dyskinesia.
Choice B rationale: the Hamilton scale is a multiple-item questionnaire used in the assessment of clients for depression and provides a guide for patient recovery evaluation.
Choice C rationale: the Braden Scale is used in the assessment of clients for the risk of pressure ulcers.
Choice D rationale: the Morse Scale is a Fall Risk Assessment tool used in assessing the probability of a client sustaining a fall.
Haldol 2mg IM stat has been ordered for the agitated client. Haldol is available in 5mg/ml. How many mls will you administer?
Explanation
To answer the above question we will use the formula:
Dose (ml)= ordered dose (mg)/ Concentration (mg/ml)
= 2mg/5mg/ml
= 0.4 ml
While the nurse is talking with a female client, the client becomes silent for several seconds. Which is the nurse's best response?
Explanation
Choice A rationale: this may imply that the client is not cooperating and may make them feel guilty thus discouraging any further communication which may be useful in generating a treatment plan for the patient.
Choice B rationale: assuming that the client has completed her conversation is incorrect since it is an opportunity to explore the client’s feelings and thoughts that may be missed.
Choice C rationale: this is not the best action since it may interrupt the client’s natural process of reflection and expression while pressuring him/her to respond to the questions asked.
Choice D rationale: remaining silent and being attentive to the client’s nonverbal communication shows respect for the client’s pace and readiness to speak.
Furthermore, it demonstrates the nurse’s presence and their support.
A client is on Clozaril (Clozapine). The nurse is aware that frequent blood work is essential during the first 6 months of treatment to monitor for the presence of what?
Explanation
Choice A rationale: Clozapine is an antipsychotic medication associated with agranulocytosis which is a condition where the bone marrow does not provide enough white blood cells. This increases an individual’s risk of infections. Therefore, frequent blood tests should be performed on an individual taking this medication to monitor the WBC count and stop the medication if need be.
Choice B rationale: clozapine is not associated with a low hemoglobin level. Anemia may be caused by conditions such as iron deficiency, chronic conditions such as chronic kidney disease, and vitamin B12 deficiency.
Choice C rationale: An increase in white blood cell count is not a side effect of clozapine but can be caused by infections. Clozapine causes low white blood cell count.
Choice D rationale: blood in urine is not a side effect of clozapine but can be caused by the use of medications such as cyclophosphamide.
In the Working phase of the nurse-client relationship, the client and nurse work toward the goals that are agreed upon. (True or False)
Explanation
The working phase of the nurse-client relationship entails the implementation of interventions and evaluation of outcomes while modifying the plan of care with need. The nurse supports and educates the client while helping them to cope with their situation. This process requires constant communication, trust, and collaboration between the nurse and the client.
A client has been taking an antipsychotic medication for several years. It is of vital importance for the nurse to observe the client for tardive dyskinesia. Signs and symptoms of tardive dyskinesia include:
Explanation
Choice A rationale: absence of physical and mental movement refers to catatonia that can occur in severe depression or schizophrenia.
Choice B rationale: akinesia refers to the absence of voluntary movement and can be seen in individuals with Parkinson’s disease or as a side effect of some antipsychotic medications.
Choice C rationale: these are signs and symptoms of tardive dyskinesia which is a serious side effect of antipsychotic therapy resulting from the damage of nerve cells controlling movement and is irreversible especially when detected late.
Choice D rationale: this refers to dystonia which is a condition characterized by abnormal muscle tone resulting in painful muscle spasms and abnormal postures. This is a side effect of some antipsychotic medications.
In communicating with the psychiatric patient, which nurse responses could block effective communication with a client? (Select all that apply)
Explanation
Choice A rationale: this response is dismissive of the patient’s feelings and concerns and does not acknowledge the patient’s reality and perspective. It implies that the patient is overreacting and may make the client feel judged and ignored.
Choice B rationale: this response is intrusive and prescriptive since the patient’s reasons and preferences are not considered. it assumes that the patient has a husband and that they have a good relationship together which may not be the case.
Choice C rationale: this response is accusatory and confrontational while implying that the patient’s behavior was wrong and unacceptable. Furthermore, it focuses on the past rather than the present or the future which is relevant in this case. It also makes the patient feel guilty and ashamed which may impair their ability to open up hence ineffective care.
Choice D rationale: This response is empathic and validating. It reflects the patient's feelings and shows understanding and compassion. It does not judge or minimize the patient's emotions, and it invites the patient to share more if they wish. This response could make the patient feel heard, supported, and respected.
Choice E rationale: this response encourages the patient to open up and express their thoughts and feelings. This makes the patient feel valued and empowered thus allowing them to share their feelings at their own pace.
During the mental status examination, the nurse observes that the client rapidly changes from one idea to another related thought. Which disordered thinking process is the client displaying?
Explanation
Choice A rationale: this is a type of delusion involving the misinterpretation of random events as having personal significance or reference.
Choice B rationale: flight of ideas refers to a disordered thinking process involving rapid shifts from one topic to another. The client’s speech is often incoherent and difficult to follow.
Choice C rationale: this is a type of memory distortion involving the fabrication of stories or details to fill the gaps in an individual’s memory. Usually occurs in conditions such as dementia, substance abuse, and brain damage.
Choice D rationale: this refers to the repetition of the same word, phrase, or action over and over without being able to stop or switch to something else. Occurs in conditions such as schizophrenia, brain injury, or a stroke.

The nurse is talking with the client in an activity room where others are present. The client becomes tearful when talking about his children at home. What is the nurse's best action?
Explanation
Choice A rationale: This is inappropriate since it does not address the client’s feelings about his/her children and may make the client feel that their feelings are not important and have been disregarded.
Choice B rationale: this is inappropriate since the client’s family issues will be exposed if they talk about them in a room full of other patients hence this will potentially increase his distress.
Choice C rationale: taking the client to a private room respects their right to privacy and dignity. Furthermore, it is a form of empathy and would encourage the client to open up with ease to the nurse.
Choice D rationale: asking the client why he is crying sounds judgmental and accusatory hence this may prevent the client from opening up to the nurse concerning his children.
The nurse should monitor which vital signs in the client who is taking Clozaril (Clozapine).
Explanation
Choice A rationale: Clozapine has no effect on a patient’s blood pressure levels. However, blood pressure monitoring for all patients is crucial but the temperature is more relevant for a patient on clozapine.
Choice B rationale: Clozapine has no effect on an individual’s respiratory rate hence in this case it is not the priority vital sign to monitor.
Choice C rationale: Clozapine use does not cause pain. Furthermore, pain is not a vital sign.
Choice D rationale: One of the side effects of clozapine is agranulocytosis hence this predisposes the patient to infections which may manifest with fever. Therefore, it is important to monitor the patient’s temperature while on treatment.
Which is an accepted criterion for inpatient admission to a mental health facility?
Explanation
Choice A rationale: this is incorrect since it is not sufficient by itself to warrant an inpatient admission hence the client can be managed as an outpatient.
Choice B rationale: this is one of the criteria for inpatient admission to a mental health facility since with the inability to cope with life stressors or control his behaviors the patient is at risk of harming either themselves or others. Moreover, this criterion reflects the principle of beneficence, meaning that the best is being done for the client's well-being and safety.
Choice C rationale: this is incorrect since depression is not sufficient by itself to warrant an inpatient admission hence the client can be managed as an outpatient.
Choice D rationale: this is incorrect since it is not sufficient by itself to warrant an inpatient admission hence the client can be managed as an outpatient.
A male inpatient client who is experiencing depression has no interest in eating. He skips meals frequently and has been losing weight. What is the best nursing action in this situation?
Explanation
Choice A rationale: this is correct since it provides the patient with an opportunity to eat his meals freely whenever they are ready to eat without feeling pressured or threatened.
Choice B rationale: the patient already knows about the benefits of good nutrition but still lacks the motivation to eat owed of his depression hence this may not be very helpful in this situation.
Choice C rationale: this may make the patient feel manipulated and guilty for not eating hence may not be helpful in addressing the underlying situation.
Choice D rationale: this may worsen the patient’s depression and lower their self-esteem since they will receive punishment for their condition rather than being offered the necessary help.
Sign Up or Login to view all the 50 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
