Ati nsg 133 mental health exam 2
Total Questions : 38
Showing 25 questions, Sign in for moreA community health nurse is assessing an elderly client whose wife passed away 4 weeks ago. The client mentions he is not eating and says, "Why bother, why bother continuing at all?" Which of the following should the nurse recognize as a sign that further assessment is needed?
Explanation
Choice A reason:
Complicated grieving is a natural response to the loss of a loved one, characterized by intense sorrow and longing. However, the client's statement indicates a sense of hopelessness and a lack of desire to continue living, which goes beyond the typical symptoms of complicated grieving. While it is important to assess for complicated grieving, the client's expression of not wanting to go on suggests a more immediate risk.
Choice B reason:
Chronic pain can lead to depression and decreased quality of life, but the client does not mention any physical pain. The absence of such complaints makes chronic pain a less likely cause for the client's current state. It is still important to assess for any physical discomfort that the client may not be communicating.
Choice C reason:
The client's statement of questioning the purpose of continuing life is a clear indicator of suicidal ideation, which warrants immediate further assessment. The risk for suicide is often heightened following significant life events such as the loss of a spouse. The nurse must prioritize this assessment to ensure the client's safety.
Choice D reason:
Social isolation can contribute to feelings of loneliness and depression, particularly in the elderly who have lost a significant other. While social isolation is a concern and can exacerbate other mental health issues, the client's explicit questioning of life's worth points more directly to a risk for suicide.
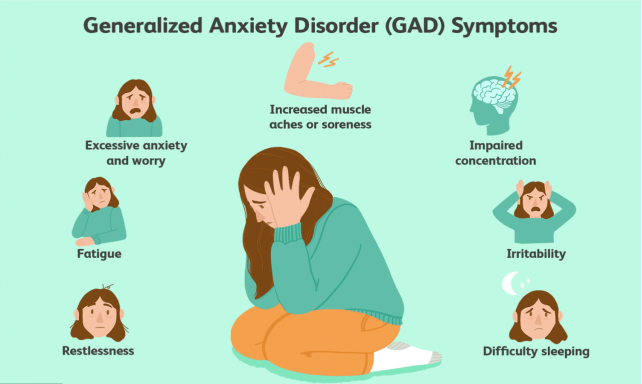
A nurse is providing education to the community about anxiety disorders. Which of the following should be included as predisposing factors for developing anxiety disorders? (Select all that apply.)
Explanation
Choice A reason:
Regular exercise is generally not considered a predisposing factor for the development of anxiety disorders. In fact, regular physical activity is often recommended as a part of the treatment plan for anxiety because it can help reduce symptoms. Exercise can improve mental health by reducing levels of the body's stress hormones, such as adrenaline and cortisol. It also stimulates the production of endorphins, chemicals in the brain that are the body's natural painkillers and mood elevators.
Choice B reason:
A family history of anxiety disorders can be a predisposing factor. Anxiety disorders can run in families, suggesting that a combination of genes and environmental stresses can produce the disorders. If a close family member has an anxiety disorder, it may increase the likelihood that an individual will develop one as well.
Choice C reason:
Regular meditation practice is typically not a predisposing factor for anxiety disorders; rather, it is often used as a coping mechanism to manage anxiety. Meditation can help reduce stress levels and improve emotional health, which may decrease the risk of developing an anxiety disorder.
Choice D reason:
Being a perfectionist can sometimes be a predisposing factor for anxiety disorders. Perfectionism is often associated with fear of failure, fear of making mistakes, and a tendency to experience high levels of stress and pressure, which can contribute to the development of anxiety disorders.
Choice E reason:
Excessive caffeine consumption can be a predisposing factor for anxiety disorders. Caffeine is a stimulant that can mimic the symptoms of anxiety, such as increased heart rate and nervousness. People who consume large amounts of caffeine may have an increased risk of developing anxiety disorders.
Choice F reason:
Chronic physical illness can be a predisposing factor for anxiety disorders. Living with a chronic illness can cause significant stress and may lead to the development of anxiety disorders. The constant worry about health, treatments, and the future can be overwhelming and may trigger or worsen anxiety symptoms.
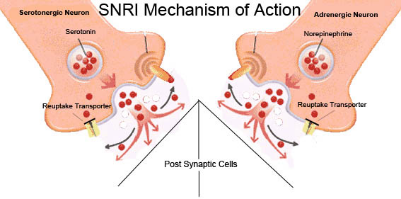
Serotonin-norepinephrine reuptake inhibitors (SNRIs), like Duloxetine, are prescribed for generalized anxiety disorder. Which of the following factors increases the risk of a client developing serotonin syndrome?
Explanation
Choice A reason:
Missing a dose of medication that increases serotonin levels does not typically increase the risk of serotonin syndrome. In fact, missing a dose may lead to lower levels of serotonin in the body, which is contrary to the condition of serotonin syndrome that arises from an excess of serotonin.
Choice B reason:
Taking MAOI medication alone does not inherently increase the risk of serotonin syndrome. However, combining MAOIs with other medications that affect serotonin levels can significantly increase the risk. It is crucial to avoid taking MAOIs and other serotonergic drugs concurrently without medical supervision.
Choice C reason:
Taking SNRIs as directed by a healthcare provider generally does not increase the risk of serotonin syndrome. These medications are designed to be taken regularly to manage conditions like anxiety and depression. However, any changes in dosage or frequency should be done under medical guidance to avoid any adverse effects.
Choice D reason:
Combining medications that increase serotonin levels is the primary risk factor for developing serotonin syndrome. This can occur when a patient takes multiple serotonergic drugs, such as combining an SNRI with an SSRI, certain pain medications, or even some over-the-counter drugs and supplements that increase serotonin levels. This combination can lead to an excessive accumulation of serotonin in the body, triggering the symptoms of serotonin syndrome.
A nurse is providing education to the community about anxiety disorders. Which of the following should be included as predisposing factors for developing anxiety disorders? (Select all that apply.)
Explanation
Choice A reason:
While it is beneficial for clients to be involved in their care planning, this is not the immediate priority. Active participation in care planning is a goal that can be pursued once the client's safety and stability are ensured.
Choice B reason:
Identifying positive qualities about oneself is an important step in improving self-esteem and promoting recovery in clients with major depressive disorder. However, this is not the most immediate priority when compared to ensuring the client's safety¹.
Choice C reason:
Exhibiting expected grieving behaviors is a natural and necessary process for healing after the loss of a loved one. However, the priority in the acute phase of care, especially when a client is at risk for self-harm, is to ensure safety.
Choice D reason:
The priority nursing goal for a client with major depressive disorder, especially following a significant loss, is to ensure safety. Making a contract to avoid self-harm is a critical intervention that addresses the risk of suicide, which is heightened in individuals with major depressive disorder and recent significant loss. This contract is a verbal or written agreement between the client and the healthcare provider that the client will not harm themselves and will seek help if they have thoughts of self-harm.
The nurse is evaluating the effectiveness of teaching for a client diagnosed with depression who has been prescribed bupropion (Wellbutrin). Which of the following statements by the client indicates that the teaching was successful?
Explanation
Choice A reason:
This statement is accurate and reflects effective teaching. Bupropion, like many antidepressants, can take several weeks to reach its full therapeutic effect. Informing patients about this delay is important to set realistic expectations and to encourage adherence to the medication regimen.
Choice B reason:
This statement is not entirely accurate. While moderate alcohol consumption may be permissible for some patients taking bupropion, it is generally advised to avoid or limit alcohol intake due to the risk of seizures and other side effects. Alcohol can also worsen depression symptoms and interact with the medication.
Choice C reason:
This statement is incorrect. Bupropion does not typically cause bradycardia (slow heartbeat). Instead, it can cause tachycardia (fast heartbeat) as a side effect. Patients should be informed about the potential cardiovascular effects of bupropion, including an increased heart rate.
Choice D reason:
This statement is incorrect. Increased salivation and drooling are not common side effects of bupropion. The medication is more commonly associated with dry mouth. Effective teaching would include informing the patient about the more likely side effects, such as dry mouth, insomnia, and headaches.
A nurse is attending to a client with generalized anxiety disorder who is having a panic attack. What should be the nurse's primary action for this client?
Explanation
Choice A reason:
Escorting the client to the common area is not the priority action. While being around others can sometimes be comforting, during a panic attack, the client may feel overwhelmed and exposed, which could exacerbate the situation.
Choice B reason:
Contacting security for possible restraints should be a last resort and is not the priority action. Restraints can increase anxiety and fear, potentially escalating the panic attack. The use of restraints is only considered when the client is at risk of harming themselves or others and all other interventions have failed.
Choice C reason:
Staying with the client is the priority action. During a panic attack, the client needs reassurance and a sense of safety. The nurse's presence can provide comfort. The nurse should remain calm, use a quiet voice, and avoid making any sudden movements. Implementing relaxation techniques and promoting a calming environment are also beneficial.
Choice D reason:
Staying away from the client is not the priority action. Leaving the client alone can increase feelings of isolation and fear. The nurse should provide continuous observation and support during the panic attack.
A nurse is looking after a client with a depressive disorder who is experiencing alcohol withdrawal and has recently lost their job. What should be the primary nursing intervention?
Explanation
Choice A reason:
Referring the client to a mental health care provider is an important step, but it may not be the immediate priority. The referral process can be initiated once the client's immediate safety and acute needs are addressed.
Choice B reason:
Determining the presence and degree of suicidal risk is the priority nursing intervention. Clients with depressive disorders, especially those experiencing significant life stressors such as job loss and undergoing alcohol withdrawal, are at a higher risk for suicide. It is crucial to assess their risk and take appropriate measures to ensure their safety.
Choice C reason:
Identifying support groups is a valuable part of long-term treatment and recovery, but it is not the immediate priority. Support groups can provide ongoing assistance and a sense of community once the client is stable and ready to engage in long-term recovery.
Choice D reason:
Assisting the client to identify the negative effects of chemical dependency is an important aspect of treatment, but it is not the immediate priority. This intervention is part of the client's long-term recovery and education process.
A nurse is giving discharge instructions to a client with bipolar disorder who will be leaving with a lithium prescription. The nurse should inform the client about which of the following factors that could increase the risk of lithium toxicity?
Explanation
Choice A reason:
Eating foods high in tyramine is not a risk factor for lithium toxicity. Tyramine is associated with dietary restrictions in patients taking monoamine oxidase inhibitors, not lithium.
Choice B reason:
Engaging in activities that cause excessive sweating, such as running 4 miles outdoors every afternoon, can lead to dehydration. Dehydration is a significant risk factor for lithium toxicity because it can increase lithium levels in the blood, potentially leading to toxicity.
Choice C reason:
Drinking 2 liters of liquids daily is generally recommended for hydration and is not a risk factor for lithium toxicity. Adequate hydration can help prevent lithium toxicity by ensuring that lithium is properly excreted through the kidneys.
Choice D reason:
Eating 2 to 3 grams of sodium-containing foods daily is within normal dietary intake ranges and is not a risk factor for lithium toxicity. Maintaining a consistent sodium intake is important when taking lithium, as low sodium levels can lead to increased lithium retention and potential toxicity.
A nurse is attending to a client who was engaged in severe combat and witnessed war casualties. The nurse should suspect posttraumatic stress disorder (PTSD) if the client makes which of the following statements?
Explanation
Choice A reason:
This statement reflects hypervigilance and a persistent sense of threat, which are symptoms associated with PTSD. Individuals with PTSD may feel constantly on edge as if danger is always imminent, leading to behaviors such as checking rooms repeatedly.
Choice B reason:
While this statement indicates a traumatic experience, it does not directly suggest symptoms of PTSD. PTSD is characterized by specific symptoms such as intrusive thoughts, flashbacks, and avoidance behaviors related to the traumatic event.
Choice C reason:
This statement may be indicative of a distressing combat experience but does not directly align with the symptoms of PTSD. It does not reflect the re-experiencing, avoidance, or arousal symptoms typically seen in PTSD.
Choice D reason:
This statement is a clear example of re-experiencing symptoms, which is a core feature of PTSD. Nightmares about the traumatic event and intrusive, distressing memories are common in individuals with PTSD. The vivid and distressing nature of such dreams can significantly impact an individual's well-being.
A nurse is conducting an admission assessment for a client who is undergoing treatment after a situational crisis. Which of the following assessments should the nurse prioritize?
Explanation
Choice A reason:
Identifying the client's support systems is an important aspect of the assessment, as support systems can play a crucial role in the client's recovery. However, it is not the highest priority during the initial assessment. Support systems can provide emotional, social, and sometimes financial assistance, which can be beneficial in managing a situational crisis.
Choice B reason:
Identifying the client's coping skills is also important because it helps the nurse understand how the client typically deals with stress and crises. Coping skills are mechanisms that individuals use to manage stressful situations and can include problem-solving, seeking support, and using relaxation techniques. However, this is not the highest priority during the initial assessment.
Choice C reason:
Asking the client to identify the cause of the crisis can provide valuable information about the client's perspective and insight into the situation. Understanding the cause can help in planning appropriate interventions. However, this is not the highest priority during the initial assessment, especially if the client is not in a stable condition to discuss the crisis.
Choice D reason:
Determining if the client has psychotic thinking, is the highest priority. Psychotic thinking can include delusions, hallucinations, and disorganized thoughts, which may indicate a severe mental health condition that requires immediate attention. It is essential to assess for psychotic symptoms to ensure the safety of the client and others, as well as to determine the need for urgent psychiatric intervention.
A client displays symptoms that align with factitious disorder. Which of the following hypotheses should the nurse give priority to in the client's care? (Select all that apply)
Explanation
Choice A reason:
This hypothesis aligns with the typical motivations seen in factitious disorder, where individuals intentionally produce or exaggerate symptoms of illness in themselves to receive attention, sympathy, and care from medical personnel¹. The nurse should prioritize understanding this behavior to manage the client's care effectively and to avoid unnecessary medical interventions.
Choice B reason:
Similar to choice A, individuals with factitious disorder may induce injury or illness to fulfill a psychological need for attention and validation. Recognizing this motivation is crucial for the nurse to provide appropriate psychological support and to prevent further self-harm.
Choice C reason:
While misdiagnosis or medical error can occur, this is not typically a hypothesis that should be prioritized in the care of a client with factitious disorder. The disorder involves intentional actions by the client, not errors by healthcare providers.
Choice D reason:
Seeking financial gain is more characteristic of malingering than factitious disorder. In factitious disorder, the primary motivation is psychological gratification from playing the patient role, rather than external incentives like financial gain.
Choice E reason:
Factitious disorder involves the intentional production of symptoms without an underlying medical condition. Therefore, this hypothesis would not be a priority in the care of a client with factitious disorder, as the symptoms are not related to a genuine medical condition but are self-induced.

A nurse is getting ready to educate a client about a lithium prescription for managing bipolar disorder. Which of the following statements should the nurse include in the instruction?
Explanation
Choice A reason:
This statement is incorrect. Nausea, vomiting, and diarrhea can be side effects of lithium and are concerns while on this medication. It is important for clients to report these symptoms to their healthcare provider, as they can be signs of lithium toxicity.
Choice B reason:
This statement is correct. Maintaining adequate sodium intake is important while taking lithium. Sodium levels can affect lithium levels in the body, and sudden changes in sodium intake can lead to lithium toxicity or decreased effectiveness of the medication.
Choice C reason:
This statement is incorrect. Lithium does not necessarily need to be taken on an empty stomach. It can be taken with or without food, although taking it with food may help reduce stomach upset.
Choice D reason:
This statement is correct. Regular monitoring of blood levels is essential during the first month of lithium therapy to ensure that lithium levels are within the therapeutic range and to avoid toxicity. The frequency of monitoring may change based on the results and as treatment continues.
A nurse is conducting a community education course on the physical complications of substance use disorder. Which of the following points should the nurse mention as a health risk associated with heroin use?
Explanation
Choice A reason:
Respiratory depression/arrest is a well-documented risk associated with heroin use. Heroin is an opioid that can significantly depress the central nervous system, leading to slowed or stopped breathing. This can result in hypoxia, a condition where not enough oxygen reaches the brain, which can be fatal.
Choice B reason:
Acute pancreatitis is not typically associated directly with heroin use. While substance use can lead to various health complications, acute pancreatitis is more commonly associated with alcohol abuse rather than opioids like heroin.
Choice C reason:
Nasal septum perforation is a potential risk for individuals who snort heroin. The repeated irritation and damage to the mucosal tissues in the nose can lead to a perforation of the nasal septum, the tissue that separates the nasal passages.
Choice D reason:
Permanent short-term memory loss is not a commonly reported direct effect of heroin use. While chronic use of heroin can lead to cognitive deficits and deterioration of white matter in the brain, which affects decision-making and behavior regulation, it does not specifically cause permanent short-term memory loss.

A nurse is looking after a client three days after admission for depression treatment. The client leaves their current activity, approaches the nurse, and says, "There's no reason to go on living. I just want to end it all." What action should the nurse take?
Explanation
Choice A reason:
When a client expresses thoughts of wanting to end their life, it is crucial for the nurse to immediately assess the risk of suicide. Asking the client if they have a plan to commit suicide is a direct approach to gauge the immediacy and seriousness of the risk. This information is vital for determining the next steps in care, which may include close supervision, safety precautions, and urgent psychiatric evaluation.
Choice B reason:
While ensuring the client is comfortable is important, allowing the client to rest without further assessment or intervention may not be safe if the client is at immediate risk of self-harm. The priority is to assess and secure the client's safety.
Choice C reason:
It is inappropriate and potentially dangerous to dismiss the client's statement as manipulation. All expressions of suicidal ideation should be taken seriously, and the nurse should provide a supportive response that addresses the client's emotional state and safety concerns.
Choice D reason:
Notifying the client's family can be part of a broader safety plan, but it should not replace immediate assessment and intervention by the healthcare team. Family members may provide support, but they are not a substitute for professional care and suicide risk assessment.
A nurse is attending to a client after an OxyContin overdose. Which medication does the nurse expect to be prescribed to reverse the effects of the opioids?
Explanation
Choice A reason: Aspirin is not used to reverse the effects of opioids. It is an anti-inflammatory drug that can reduce pain and fever, but it does not have the capability to counteract opioid effects.
Choice B reason: Acetaminophen, also known as Tylenol, is a pain reliever and a fever reducer. It does not have the properties to reverse opioid overdoses and is not an antidote for opioids.
Choice C reason: Naloxone is the correct medication to reverse the effects of opioids. It is an opioid antagonist that can quickly restore normal breathing in a person if their breathing has slowed or stopped because of an opioid overdose. Naloxone binds to opioid receptors and can reverse and block the effects of other opioids.
Choice D reason: Ibuprofen is a nonsteroidal anti-inflammatory drug (NSAID) used to treat pain, fever, and inflammation. Like aspirin and acetaminophen, it does not reverse the effects of an opioid overdose.
In conclusion, naloxone is the medication that is used to reverse the effects of opioids in the case of an overdose. It is a critical drug in emergency situations involving opioids and can save lives by reversing life-threatening respiratory depression caused by opioid overdose. Healthcare providers should be prepared to administer naloxone and provide appropriate follow-up care after its use.
The nurse is looking after a client with a history of alcohol use disorder who is showing withdrawal symptoms. What should be the nurse's primary action?
Explanation
Choice A reason:
Supporting the client's attempt to rebuild damaged interpersonal relationships is an important long-term goal in the recovery process. However, it is not the immediate priority when a client is experiencing acute withdrawal symptoms, which can be life-threatening.
Choice B reason:
Educating the client about the effects of alcohol dependence and the need for rehabilitation is crucial for long-term recovery and preventing relapse. Nevertheless, during acute withdrawal, the priority is to manage the physical and psychological symptoms safely.
Choice C reason:
Teaching the client alternative strategies for managing anxiety is a valuable part of therapy and helps in long-term coping. However, during acute withdrawal, the client may not be able to learn or apply these strategies effectively due to the severity of their symptoms.
Choice D reason:
Preparing to administer Ativan as ordered is the priority action. Ativan (lorazepam) is a benzodiazepine commonly used to treat alcohol withdrawal symptoms. It helps to prevent seizures, reduce agitation, and manage other withdrawal symptoms. During the acute phase of alcohol withdrawal, maintaining physiological stability and ensuring the client's safety are the primary concerns.
A nurse on a mental health unit is attending to a client with generalized anxiety disorder who received an upsetting phone call and is now pacing the corridors. What action should the nurse take?
Explanation
Choice A reason:
Walking with the client at a gradually slower pace is a therapeutic technique that can help reduce anxiety. It allows the nurse to provide a calming presence and support while also helping to decrease the client's physical agitation in a controlled manner. This approach is non-confrontational and can be very effective in managing acute anxiety symptoms.
Choice B reason:
Having a staff member escort the client to her room might seem like a reasonable option, but it could be perceived as punitive or isolating, especially if the client is not posing a risk to themselves or others. It may also escalate the client's anxiety by making them feel confined or punished.
Choice C reason:
Instructing the client to sit down and stop pacing is not advisable as it may come across as dismissive of the client's distress. It could also increase the client's anxiety by making them feel that their coping mechanism (pacing) is not acceptable, which could lead to increased agitation or resistance.
Choice D reason:
Allowing the client to pace alone until physically tired is not the best option as it does not provide any direct support or intervention from the nurse. While pacing may be a self-soothing behavior, it does not address the underlying anxiety and could potentially lead to physical exhaustion without any emotional relief.
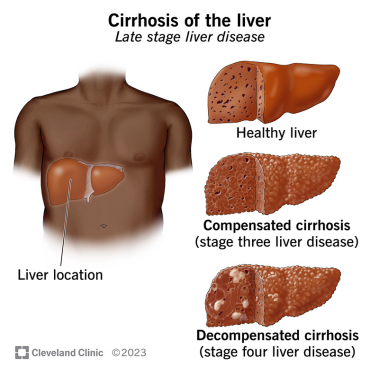
A nurse is conducting a community education course on the physical complications of substance use disorder. Which of the following should the nurse identify as the main cause of liver cirrhosis?
Explanation
Choice A reason:
Caffeine is not typically associated with liver cirrhosis. While excessive consumption of caffeine can have various health implications, it is not considered a direct cause of liver cirrhosis. The liver metabolizes caffeine without significant damage or scarring to the liver tissue.
Choice B reason:
Alcohol is the primary cause of liver cirrhosis in many cases. Chronic alcohol abuse leads to liver damage and subsequent scarring, known as cirrhosis. The liver's function is to process and filter toxins, including alcohol. Excessive and prolonged alcohol consumption overwhelms the liver's ability to process it, leading to inflammation, damage, and eventually scarring of the liver tissue.
Choice C reason:
Inhalants are substances that produce chemical vapors that can be inhaled to induce a psychoactive, or mind-altering, effect. While they can cause a range of acute and chronic health issues, including damage to the heart, kidneys, lungs, and brain, they are not commonly associated with liver cirrhosis. Liver cirrhosis is not a typical consequence of inhalant use.
Choice D reason:
Cocaine use can lead to various health problems, including cardiovascular and neurological issues, but it is not commonly identified as a primary cause of liver cirrhosis. Cocaine metabolites can be toxic to the liver; however, the direct causation of cirrhosis from cocaine alone is less established compared to alcohol-related liver disease.
A nurse is admitting a patient with a history of alcohol use disorder to the medical unit. Which of the following potential long-term physiological effects on the patient's body should the nurse be aware of? (Select all that apply)
Explanation
Choice A reason:
Cirrhosis is a severe scarring of the liver and poor liver function seen at the terminal stages of chronic liver disease. It is one of the primary long-term effects of alcohol use disorder, as the liver is the main organ responsible for metabolizing alcohol. Chronic alcohol consumption can lead to inflammation, liver cell death, and eventually cirrhosis, which significantly impairs the liver's ability to function properly.
Choice B reason:
Heightened awareness is not typically a long-term physiological effect of alcohol use disorder. In fact, chronic alcohol use is more likely to dull cognitive functions and reduce awareness due to its depressive effects on the central nervous system.
Choice C reason:
Gastritis, an inflammation of the stomach lining, is another potential long-term effect of alcohol use disorder. Alcohol can irritate and erode the gastric mucosa, leading to gastritis, which may present with symptoms such as abdominal pain, nausea, and vomiting.
Choice D reason:
Brain damage is a serious long-term effect of alcohol use disorder. Alcohol can cause changes in the brain, leading to problems with cognition, memory, and motor skills. Chronic exposure to alcohol can result in brain shrinkage and the development of conditions like Wernicke-Korsakoff syndrome.
Choice E reason:
Esophageal varices are enlarged veins in the esophagus that can occur as a result of portal hypertension, often due to cirrhosis of the liver caused by alcohol use disorder. They are a significant risk because they can rupture and lead to life-threatening bleeding.
A client dies by suicide in an acute mental health facility. What is the priority follow-up intervention for the staff on the unit after this incident?
Explanation
Choice A reason:
While giving the family an opportunity to talk about their feelings is important, it is not the immediate priority for staff intervention following the incident. The family's needs are crucial, but the question specifically asks about the staff's follow-up actions.
Choice B reason:
Investigating and identifying cues in the client's behavior that might have indicated contemplation of suicide is a critical step in understanding and preventing future incidents. However, this is more of a retrospective action and not the immediate priority for staff intervention after such an event.
Choice C reason:
Providing professional counseling for staff members is the priority intervention. Staff members may experience a range of emotions, including grief, guilt, and trauma, following a client's suicide. Professional counseling can support staff in processing these feelings and prevent potential long-term psychological effects.
Choice D reason:
Changing policies for staff observation of clients who are suicidal may be necessary, but it is not the immediate priority following the incident. Policy review and changes are part of a longer-term strategy to improve care and prevent future incidents.
A nurse on a crisis hotline is talking to a client who says, "I just ingested an entire bottle of amitriptyline." What response should the nurse provide?
Explanation
Choice A Reason:
In a situation where a client has ingested a potentially lethal amount of medication, immediate medical intervention is crucial. Amitriptyline is a tricyclic antidepressant, and overdose can lead to life-threatening conditions such as cardiac arrhythmias, severe hypotension, and seizures. The nurse's priority is to ensure the safety of the client by sending an ambulance. This response also acknowledges the client's cry for help and initiates prompt action.
Choice B Reason:
While it's important to recognize the emotional state of the client, this response does not address the immediate medical emergency. The client's safety is the priority, and while their feelings are valid, this choice does not facilitate the urgent care needed.
Choice C Reason:
Asking if the client was trying to commit suicide can come across as judgmental and may close off communication. It's essential to maintain an open line of communication and focus on getting medical help rather than determining intent at this critical moment.
Choice D Reason:
Knowing the quantity of medication ingested can be useful information for medical professionals; however, it is not the most immediate concern in a crisis situation. The first response should be to ensure that medical help is on its way.
A nurse is attending to a client admitted with a suspected stimulant overdose. What should be the nurse's first priority in their care?
Explanation
Choice A Reason:
Administering activated charcoal can be a treatment option in some overdose cases, particularly when the substance ingested is known to be adsorbed by charcoal. However, its effectiveness varies depending on the substance and the timing of administration post-ingestion. In the case of a stimulant overdose, activated charcoal is not the first-line treatment, especially when the specific stimulant and time of ingestion are unknown.
Choice B Reason:
Obtaining a urine sample for drug testing is important for confirming the type of stimulant ingested and can guide further treatment. However, this is not the immediate priority in an acute overdose situation where the patient's life may be at risk.
Choice C Reason:
Initiating seizure precautions is important in the management of stimulant overdose due to the risk of seizures. However, this is a precautionary measure and not the first action to take. The initial focus should be on assessing and stabilizing the patient's vital functions.
Choice D Reason:
Monitoring vital signs is the most critical initial step in managing a suspected stimulant overdose. Stimulants can cause severe hypertension, tachycardia, hyperthermia, and arrhythmias. Frequent monitoring allows for the early detection of life-threatening conditions and the initiation of appropriate interventions to stabilize the patient's condition.
A nurse is attending to a client who has been using Xanax (alprazolam) for anxiety. What should the nurse expect?
Explanation
Choice A reason:
Decreasing the dose of Xanax (alprazolam) is often necessary when a client shows signs of dependency or when there are concerns about potential side effects, such as uncontrolled hypertension. Xanax is a fast-acting benzodiazepine, which can be highly addictive, especially when taken in doses of 4 mg/day for longer than 12 weeks. It is essential to monitor the client's blood pressure and adjust the medication accordingly to avoid exacerbating hypertension.
Choice B reason:
Increasing the dose may temporarily control symptoms of anxiety, but it also increases the risk of dependency and other side effects. Given the client's uncontrolled hypertension, increasing the dose could lead to further complications.
Choice C reason:
This statement is incorrect. Xanax does cause dependency, and it is one of the most addictive benzodiazepine medications on the market today. Dependency can develop quickly, even in users who follow a prescribed dosing schedule.
Choice D reason:
While Ativan (Lorazepam) is also used to treat anxiety, adding it to the client's medication regimen without careful consideration could increase the risk of dependency and adverse effects. Both Xanax and Ativan are benzodiazepines, and their combined use should be monitored closely by a healthcare professional.
A nurse is looking after a client who is depressed and unwilling to join group therapy or carry out daily activities. What statement should the nurse make to the client?
Explanation
Choice A reason:
This choice represents an authoritative approach, which may not be effective with a depressed client who is refusing therapy and ADLs. It does not offer support or understanding of the client's condition and may exacerbate feelings of helplessness or resistance to care.
Choice B reason:
While this statement offers a degree of autonomy to the client, it lacks the active encouragement and assistance that might be necessary to motivate a client who is depressed. It does not address the importance of participating in therapy or ADLs for the client's recovery.
Choice C reason:
This is the most therapeutic choice as it offers both support and a gentle nudge towards participation. It acknowledges the client's current state and provides a clear, immediate, and supportive next step. This approach can help reduce the client's feelings of being overwhelmed and can foster a sense of collaboration between the nurse and the client.
Choice D reason:
This statement, although factual, may come across as confrontational and could potentially discourage the client further. It does not provide the supportive framework that is crucial for engaging a client who is struggling with depression.
A nurse is reinforcing teaching about alcohol tolerance with a newly admitted client. Which statement made by the client shows that the teaching was effective?
Explanation
Choice A reason:
The statement "Alcohol tolerance causes me to have an increased effect when taking opiates" is incorrect. Alcohol tolerance refers to the body's diminished response to the effects of alcohol due to prolonged exposure. It does not directly affect the body's response to other substances like opiates. However, it's important to note that mixing alcohol with opiates can be dangerous and is generally advised against due to the risk of respiratory depression and other adverse effects.
Choice B reason:
The statement "I will develop a decreased physical response to alcohol" is correct and indicates effective teaching. As a person develops alcohol tolerance, their body requires more alcohol to achieve the same effects that were previously attained with less alcohol. This is due to physiological adaptations within the body, particularly in the liver and central nervous system, which become more efficient at metabolizing alcohol and less responsive to its effects.
Choice C reason:
The statement "Alcohol tolerance is a medical emergency and can develop as a result of withdrawal" is incorrect. Alcohol tolerance itself is not a medical emergency; rather, it is a physiological adaptation to regular alcohol consumption. Withdrawal, on the other hand, can be a medical emergency if severe symptoms such as seizures or delirium tremens occur. Tolerance and withdrawal are related but distinct phenomena; tolerance can lead to dependence, which, when alcohol use is stopped, can result in withdrawal symptoms.
Choice D reason:
The statement "Alcohol tolerance produces physical changes when I haven't recently ingested alcohol" is misleading. Alcohol tolerance does not produce physical changes in the absence of alcohol. Instead, tolerance is characterized by a reduced response to alcohol when it is consumed. Physical changes, such as withdrawal symptoms, may occur when a person who has developed tolerance stops consuming alcohol, but these are not due to tolerance itself.
Sign Up or Login to view all the 38 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
