Ati NSG 137 Exam 3 Fall 2023
Total Questions : 48
Showing 25 questions, Sign in for moreThe nurse is providing health promotion teaching to a group of clients. The nurse should include in her teaching that which of the following population has a greater risk factor for osteoporosis?
Explanation
Choice A rationale: African Americans generally have a lower risk of osteoporosis compared to Caucasians. They tend to have higher bone mineral density, which reduces their susceptibility to osteoporosis.
Choice B rationale: Asian men may have a lower risk of osteoporosis than postmenopausal Caucasian women. However, the risk factors for osteoporosis can vary among individuals, and it's essential to consider factors such as lifestyle, genetics, and overall health.
Choice C rationale: According to research, postmenopausal caucasian women have the highest risk of osteoporosis among all population groups. This is because they tend tohave lower bone mass, lower estrogen levels, and longer life expectancy than other groups.
Choice D rationale: While American Indians may have varying risks of osteoporosis, the general risk pattern indicates that postmenopausal Caucasian women are at a higher risk. The prevalence of osteoporosis is influenced by a combination of genetic, environmental, and lifestyle factors.
A male client with possible fertility problems asks the nurse where sperm is produced. Which answer should the nurse give the client?
Explanation
Choice A rationale: The vas deferens is a duct that carries sperm from the testes to the urethra but is not the site of sperm production.
Choice B rationale: The epididymis is a structure where sperm mature and are stored but is not the primary site of sperm production.
Choice C rationale: The prostate is a gland that contributes to seminal fluid but is not involved in the production of sperm.
Choice D rationale: Sperm is produced in the testes.
An adolescent male is brought to the emergency department with complaints of excruciating pain in his left testicle. Which of the following should be the priority action by the nurse?
Explanation
Choice A rationale: Telling the adolescent that everything will be fine without a thorough assessment may delay necessary interventions.
Choice B rationale: Excruciating pain in the testicle requires immediate attention since it could be an indication of testicular torsion. The nurse should complete an assessment and notify the emergency department physician promptly.
Choice C rationale: While documentation is important, the priority is to address the immediate needs of the adolescent in severe pain.
Choice D rationale: Documenting pain assessment as n
An adolescent male is brought to the emergency department with complaints of excruciating pain in his left testicle. Which of the following should be the priority action by the nurse?
Explanation
Choice A rationale: Telling the adolescent that everything will be fine without a thorough assessment may delay necessary interventions.
Choice B rationale: Excruciating pain in the testicle requires immediate attention since it could be an indication of testicular torsion. The nurse should complete an assessment and notify the emergency department physician promptly.
Choice C rationale: While documentation is important, the priority is to address the immediate needs of the adolescent in severe pain.
Choice D rationale: Documenting pain assessment as normal is not appropriate when the client is experiencing excruciating pain.
The nurse is taking a health history from a client. The client tells the nurse that. "It feels like the room is spinning." How should the nurse document this finding?
Explanation
Choice A rationale: The sensation of the room spinning is termed vertigo. It is often caused by problems in the inner ear or the brain.
Choice B rationale: Seizure activity involves abnormal electrical activity in the brain and is not characterized by a sensation of the room spinning.
Choice C rationale: Dizziness is a more general term that may include lightheadedness or unsteadiness but does not specifically describe the sensation of the room spinning.
Choice D rationale: Syncope refers to a temporary loss of consciousness, often described as fainting, and is not indicative of a sensation of the room spinning.

The nurse is performing an assessment and finds that the client has nontarry and black stool. Which of the following subjective data should the nurse document as a normal finding consistent with nontarry black stool?
Explanation
Choice A rationale: Taking an iron supplement can lead to nontarry and black stool due to the dark color of iron.
Choice B rationale: Dry heaves are not typically associated with nontarry black stool. Choice C rationale: Eating red meat would result in reddish stool, not black. Choice D rationale: Loss of appetite is not directly related to the appearance of stool.
The nurse is performing a neurological assessment on a client with a history of Diabetes. When testing the ability to feel the vibrations of a tuning fork, the nurse notices that the client is unable to feel vibrations on the great toe or ankle bilaterally, but is able to feel vibrations on both patellae. What should the nurse suspect from these assessments?
Explanation
Choice A rationale: Hyperalgesia refers to increased sensitivity to pain and is not evident in this scenario.
Choice B rationale: Inability to feel vibrations in the great toe or ankle bilaterally suggests peripheral neuropathy, which is a common complication of diabetes affecting the peripheral nerves.
Choice C rationale: Hyperparalysis is not a recognized term in the context of this assessment.
Choice D rationale: Lesion of the sensory cortex would likely have more widespread sensory deficits and wouldn't selectively affect the great toe and ankle.
A client reports pain in the left wrist after falling while playing basketball. After assessing the wrist, which of the following assessment finding would make the nurse suspect a fracture?
Explanation
Choice A rationale: Dull throbbing pain that increases with rest is less suggestive of a fracture.
Choice B rationale: A dull ache may be present with various conditions and is not specific to a fracture.
Choice C rationale: Sharp pain that increases with movement is indicative of a possible fracture, as movement can cause the fractured ends of the bone to rub against each other.
Choice D rationale: Deep pain in the wrist is nonspecific and may not be strongly indicative of a fracture.
The nurse has completed a peripheral vascular assessment on a client. Which of the following would the nurse document as expected findings?
Explanation
Choice A rationale: A normal capillary refill time is less than 3 seconds, which indicates adequate blood flow and oxygenation.
Choice B rationale: Radial pulses 2+ with regular rate and rhythm bilaterally are expected findings in a peripheral vascular assessment, indicating normal blood flow to the extremities.
Choice C rationale: Pale and cool feet may indicate decreased blood flow and are not expected findings.
Choice D rationale: Ankle edema may indicate venous insufficiency or other circulatory issues, and it is not an expected finding in a healthy peripheral vascular assessment.
A nurse is assessing a client's cranial nerves. Which of the following methods should the nurse use to assess cranial nerve V?
Explanation
Choice A rationale: Listening to the client's speech is not related to the assessment of cranial nerve V.
Choice B rationale: Reading a Snellen chart is related to visual acuity and involves cranial nerve II, not cranial nerve V.
Choice C rationale: Identifying scented aromas is related to olfaction, which involves cranial nerve I, not cranial nerve V.
Choice D rationale: Cranial nerve V, the trigeminal nerve, is responsible for sensory input from the face and motor function such as biting and chewing. Asking the client to clench his teeth assesses the motor function of the trigeminal nerve.
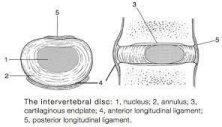
The nurse teaches a client that there are shock absorbers in the back to cushion the spine and to help it move. The client understands that which of the following is another name for shock absorbers:
Explanation
Choice A rationale: The vertebral column refers to the entire structure of the spine.
Choice B rationale: Intervertebral disks are the structures between the vertebrae that act as shock absorbers, providing cushioning and flexibility to the spine.
Choice C rationale: The vertebral foramen is an opening in each vertebra through which the spinal cord passes.
Choice D rationale: Nucleus pulposus is the soft, gel-like substance in the center of an intervertebral disk.
During an abdominal assessment, the nurse is unable to hear bowel sounds in a client's abdomen. How long should the nurse listen before reporting absent bowel sounds?
Explanation
Choice A rationale: One minute is not sufficient to determine the absence of bowel sounds, especially in all quadrants.
Choice B rationale: Ten minutes in each quadrant is excessive and not a standard practice.
Choice C rationale: The nurse should listen for at least 1 minute in each quadrant before concluding that bowel sounds are absent, as they may be very faint or irregular.
Choice D rationale: Five minutes in each quadrant is excessive and not a standard practice.
A 60-year-old man has been told that he has benign prostatic hypertrophy (BPH). He expresses that his friend just died from prostate cancer and that he is concerned about dying from cancer. Which of the following is an appropriate response by the nurse?
Explanation
Choice A rationale: Stating that it would be very unusual for a man his age to have prostate cancer may not be accurate, as prostate cancer can occur in older individuals.
Choice B rationale: Discussing chemotherapy implies a cancer treatment plan, which may not be applicable to BPH.
Choice C rationale: Describing the swelling in the prostate as temporary and going away may not be accurate for BPH, as it is a chronic condition.
Choice D rationale: The nurse provides accurate information by explaining that benign prostatic hypertrophy (BPH) is caused by hormonal changes and is not cancerous.
During an assessment of the cranial nerves (CNS), the nurse finds the following asymmetry when the client smiles or frowns, uneven lifting of the eyebrows, and escape of air when the nurse presses against the right puffed cheek. The nurse recognized that these findings indicate dysfunction of which cranial nerve(s)?
Explanation
Choice A rationale: CN X (vagus nerve) and CN VII (facial nerve) are separate cranial nerves, and the described findings are more indicative of dysfunction in the motor component of CN VII.
Choice B rationale: CN XI (accessory nerve) is primarily involved in motor function related to the sternocleidomastoid and trapezius muscles. It is not likely to cause the described facial asymmetry.
Choice C rationale: CN IV (trochlear nerve) is responsible for eye movement and would not be directly related to the described facial findings.
Choice D rationale: The described findings, such as asymmetry when smiling or frowning, uneven lifting of the eyebrows, and escape of air when pressing against a puffed cheek, indicate dysfunction of the motor component of cranial nerve VII (facial nerve).
A client tells the nurse about being very unsteady and has difficulty in maintaining balance. The nurses recognizes that which area of the brain is involved and requires further assessment?
Explanation
Choice A rationale: The brainstem is involved in basic life functions such as breathing, heart rate, and consciousness.
Choice B rationale: The cerebellum is primarily responsible for coordination, balance, and muscle tone. Unsteadiness and difficulty maintaining balance often indicate issues with the cerebellum and warrant further assessment.
Choice C rationale: The extrapyramidal tract is associated with motor function and does not play a primary role in balance and coordination.
Choice D rationale: The thalamus is involved in relaying sensory information but is not the primary center for balance and coordination.
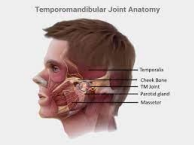
The nurse is performing a physical assessment on the client's mandible and temporal bone. The nurse recognizes that the articulation of the mandible and the temporal bone is called?
Explanation
Choice A rationale: The condyle of the mandible is the rounded process that fits into the TMJ.
Choice B rationale: The zygomatic arch is a bony structure formed by the zygomatic bone and the temporal bone.
Choice C rationale: The articulation of the mandible and the temporal bone is called the temporomandibular joint (TMJ).
Choice D rationale: The intervertebral foramen is an opening between vertebrae through which nerves exit the spinal cord.
A client comes to the clinic and reports having weakness in the left arm and leg for the past week. The nurse should perform which type of neurological exam?
Explanation
Choice A rationale: The Glasgow Coma Scale is used to assess the level of consciousness, not specific weakness in the extremities.
Choice B rationale: A complete neurological examination is appropriate to assess the client's weakness in the left arm and leg. This examination includes evaluating motor function, sensory function, coordination, reflexes, and cranial nerve function.
Choice C rationale: A muscular examination may focus on specific muscle groups but may not provide a comprehensive assessment of neurological function.
Choice D rationale: A neurologic recheck examination is not a standardized term and may not cover all aspects of a complete neurological assessment.
The nurse is assessing a female client who reports painful menstruation. Which of the following should the nurse document in the client's record about painful menstruation?
Explanation
Choice A rationale: Painful menstruation is referred to as dysmenorrhea.
Choice B rationale: Dysuria is painful or difficult urination and is not related to menstruation.
Choice C rationale: Hematuria is the presence of blood in the urine and is not related to menstruation.
Choice D rationale: Dyschezia is difficulty or pain during bowel movements and is not related to menstruation.
The nurse is assessing a client who reports cessation of menses. The nurse should document the cessation of menses in the client's record as:
Explanation
Choice A rationale: Salpingitis is inflammation of the fallopian tubes.
Choice B rationale: Adnexa refers to the accessory structures of the uterus, including the ovaries and fallopian tubes.
Choice C rationale: Menarche is the onset of menstruation, not the cessation. Choice D rationale: Cessation of menses is referred to as menopause.
The nurse suspects that a client has carpal tunnel syndrome and prepares to conduct the Phalen test. What instructions should the nurse give the client to perform the Phalen test?
Explanation
Choice A rationale: Plantarflexion of the foot is not part of the Phalen test. Choice B rationale: Dorsiflexion of the foot is not part of the Phalen test.
Choice C rationale: To perform the Phalen test, the client should hold both hands back to back while flexing the wrists 90 degrees for 60 seconds. This test helps assess for symptoms of carpal tunnel syndrome.
Choice D rationale: Hyperextension of the wrists with the palmar surface of both hands touching is not the correct position for the Phalen test.

The nurse is performing a scrotal assessment on a male client. Which of the following findings of the scrotum should the nurse recognize as abnormal?
Explanation
Choice A rationale: Asymmetry with one side hanging lower than the other is a normal variation in scrotal anatomy.
Choice B rationale: Marked tenderness on palpation of the scrotum is abnormal and may indicate inflammation or infection.
Choice C rationale: Easy sliding of scrotal contents when palpated is a normal finding.
Choice D rationale: Small, firm, nontender, yellowish nodules may represent sebaceous cysts or Fordyce spots, which are typically benign and not a cause for concern.
The nurse tests the function of Cranial Nerve XI while performing a physical examination on a client. Which statement best describes the response the nurse should expect if Cranial Nerve XI is intact?
Explanation
Choice A rationale: Sticking out the tongue without tremors or deviation is related to Cranial Nerve XII (hypoglossal nerve), not Cranial Nerve XI.
Choice B rationale: Following an object with the eyes without nystagmus or strabismus is more related to visual tracking and coordination, not Cranial Nerve XI.
Choice C rationale: Hearing ability is primarily associated with Cranial Nerve VIII (vestibulocochlear nerve), not Cranial Nerve XI.
Choice D rationale: Cranial Nerve XI, also known as the accessory nerve, is responsible for the movement of the head and shoulders against resistance. If intact, the client should be able to perform this action with equal strength on both sides.
A nurse is assessing a client's cranial nerves as part of a neurological examination. Which of the following actions should the nurse take to assess cranial nerve III?
Explanation
Choice A rationale: Observing for facial symmetry is more relevant to Cranial Nerve VII (facial nerve).
Choice B rationale: Cranial nerve III (oculomotor nerve) is responsible for pupillary constriction. The nurse should check the pupillary response to light to assess the function of this cranial nerve.
Choice C rationale: Testing visual acuity is not specific to Cranial Nerve III but is more associated with Cranial Nerve II (optic nerve).
Choice D rationale: Eliciting the gag reflex is related to Cranial Nerve IX (glossopharyngeal nerve) and X (vagus nerve), not Cranial Nerve III.
During a community screening event for bone density, an elderly client asked the nurse why she is an inch shorter in height. Which of the following responses by the nurse is correct?
Explanation
Choice A rationale: Loss of subcutaneous fat is not a primary factor contributing to decreased height with aging.
Choice B rationale: The flexibility of the spine may contribute to posture but is not the primary reason for a significant decrease in height.
Choice C rationale: With aging, the cartilage between the bones in the spine gets worn down, leading to decreased height. This is due to degenerative changes in the intervertebral disks.
Choice D rationale: Thickening of intervertebral disks is not typically associated with aging and decreased height. Degeneration and thinning of the disks are more common factors.
The nurse is completing a neurological assessment on a client who suffered from a motor vehicle accident (MVA). Which of the following findings should the nurse report to the practitioner immediately?
Explanation
Choice A rationale: The ability to swallow pureed foods is not an immediate concern and does not indicate a life-threatening condition.
Choice B rationale: Mild headache, while noteworthy, may not require immediate attention unless it is accompanied by other concerning symptoms.
Choice C rationale: Weakness is a general symptom that should be further assessed for severity and associated symptoms before determining the urgency of intervention. The GCS score of 5 takes precedence in this context.
Choice D rationale: A Glasgow Coma Scale (GCS) of 5 indicates severe impairment of consciousness and requires immediate attention. A lower GCS score reflects a deeper level of coma.
Sign Up or Login to view all the 48 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
