Ati nur211 mobility exam
Total Questions : 29
Showing 25 questions, Sign in for moreA nurse is observing a client admitted with a severe burn injury who is undergoing IV fluid resuscitation therapy. Which of the following findings should the nurse recognize as a sign of sufficient fluid replacement?
Explanation
Choice A Reason:
Urine output is one of the most reliable indicators of adequate fluid resuscitation in burn patients. The goal is to maintain a urine output of 0.5 to 1 mL/kg/hour in adults. This parameter is crucial because it directly reflects renal perfusion and, by extension, overall circulatory volume status. When fluid resuscitation is adequate, the kidneys receive enough blood flow to produce urine at this rate, indicating that the body's tissues are being adequately perfused. Monitoring urine output is a non-invasive and straightforward method, making it a preferred choice in clinical settings.
Choice B Reason:
Heart rate can be an indicator of fluid status, but it is less reliable than urine output. Tachycardia (an increased heart rate) can occur due to pain, anxiety, or other stressors, not just fluid deficit. While a decreasing heart rate might suggest improving fluid status, it is not a definitive indicator on its own. Other factors must be considered in conjunction with heart rate to assess fluid resuscitation adequacy.
Choice C Reason:
Blood pressure is another parameter used to assess fluid status, but it can be influenced by many factors, including the patient's baseline blood pressure, medications, and the presence of other medical conditions. While maintaining adequate blood pressure is important, it is not as sensitive or specific as urine output for assessing fluid resuscitation in burn patients. Blood pressure can remain within normal ranges even when fluid resuscitation is inadequate, especially in the early stages.
Choice D Reason:
Mental status can be affected by fluid status, but it is a late indicator of inadequate perfusion. Changes in mental status, such as confusion or decreased level of consciousness, can occur when there is significant hypoperfusion and shock. By the time mental status changes are observed, the patient may already be in a critical state. Therefore, it is not a primary indicator for assessing fluid resuscitation adequacy.
Choice E Reason:
Capillary refill time is a quick and simple test to assess peripheral perfusion. However, it is not as reliable as urine output for evaluating overall fluid status. Capillary refill can be affected by ambient temperature, lighting conditions, and the examiner's technique. While a prolonged capillary refill time can indicate poor perfusion, it is not as specific or sensitive as urine output for assessing fluid resuscitation adequacy.
A nurse is attending to a client with a closed-head injury and elevated ICP readings between 16 and 22 mm Hg. What actions should the nurse take to reduce the risk of increasing the client's ICP?
Explanation
Choice A Reason:
Elevating the client's head on two pillows can help reduce ICP by promoting venous drainage from the brain. However, it is important to ensure that the head is not elevated too high, as this can impede venous return and potentially increase ICP. The recommended elevation is typicallly 30 degrees. While this intervention is beneficial, it is not the most critical action compared to reducing environmental stimuli.
Choice B Reason:
Keeping the client well hydrated is essential for overall health, but excessive hydration can increase ICP by increasing the volume of cerebrospinal fluid and blood within the cranial vault. Fluid management must be carefully monitored to avoid exacerbating ICP. Therefore, while hydration is important, it must be balanced and not excessive.
Choice C Reason:
Decreasing the noise level in the client's room is crucial for minimizing external stimuli that can increase ICP. Noise and other environmental stressors can lead to increased agitation and stress, which in turn can elevate ICP. Creating a calm and quiet environment helps in maintaining a stable ICP and is a non-invasive, easily implementable intervention.
Choice D Reason:
Frequent suctioning of the endotracheal tube can cause transient increases in ICP due to the stimulation and potential for coughing. While suctioning is necessary to maintain airway patency, it should be performed judiciously and only when clinically indicated. Over-suctioning can lead to spikes in ICP and should be avoided.
Which types of shock and their causes should be listed? (Select all that apply.)
Explanation
Choice A Reason:
Neurogenic shock occurs due to a disruption in the autonomic nervous system, often resulting from spinal cord injuries. This disruption leads to a loss of sympathetic tone, causing widespread vasodilation and a subsequent drop in blood pressure. The hallmark of neurogenic shock is hypotension with bradycardia, which differentiates it from other types of shock that typically present with tachycardia. The loss of vascular tone results in pooling of blood in the extremities, reducing venous return to the heart and decreasing cardiac output.
Choice B Reason:
Hypovolemic shock is caused by a significant loss of blood or fluids, leading to inadequate circulating volume. This can result from trauma, surgery, gastrointestinal bleeding, or severe dehydration. The primary mechanism is a reduction in preload, which decreases stroke volume and cardiac output. Clinical signs include tachycardia, hypotension, and cool, clammy skin. Rapid fluid resuscitation is critical to restore circulating volume and improve tissue perfusion.
Choice C Reason:
Metabolic shock is not a recognized type of shock in medical literature. The term might be confused with metabolic acidosis, which can occur secondary to shock but is not a primary cause. Metabolic acidosis results from the accumulation of lactic acid due to anaerobic metabolism when tissues are inadequately perfused. Therefore, metabolic shock is not considered a valid type of shock.
Choice D Reason:
Anaphylactic shock is a severe, life-threatening allergic reaction that leads to widespread vasodilation, increased capillary permeability, and bronchoconstriction. Common triggers include foods, insect stings, medications, and latex. Symptoms include hypotension, swelling, difficulty breathing, and hives. Immediate administration of epinephrine is crucial to counteract the severe allergic response and stabilize the patient.
Choice E Reason:
Septic shock results from a severe infection that leads to systemic inflammation and widespread vasodilation. The infection triggers an overwhelming immune response, causing damage to blood vessels and organs. Clinical features include fever, hypotension, tachycardia, and altered mental status. Early recognition and aggressive treatment with antibiotics and fluid resuscitation are essential to improve outcomes.
Choice F Reason:
Cardiogenic shock occurs when the heart fails to pump effectively, leading to inadequate tissue perfusion. Common causes include myocardial infarction, severe heart failure, and arrhythmias. Symptoms include hypotension, tachycardia, and signs of poor perfusion such as cool extremities and altered mental status. Treatment focuses on improving cardiac output through medications, mechanical support, or revascularization procedures.
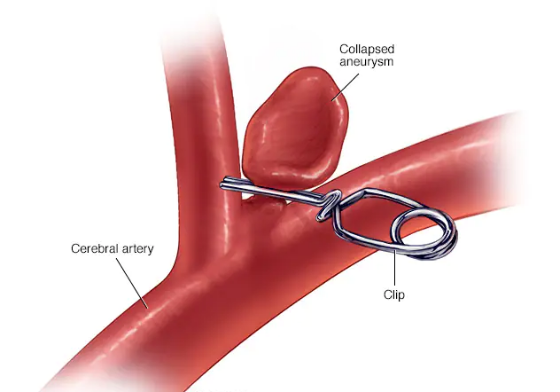
What is a possible complication of a treated aneurysm?
Explanation
Choice A Reason:
Improved blood flow to surrounding tissues is generally a desired outcome of treating an aneurysm, not a complication. When an aneurysm is successfully treated, the goal is to restore normal blood flow and prevent the aneurysm from rupturing. Improved blood flow indicates that the treatment was effective and that the risk of complications has been minimized.
Choice B Reason:
Rupture leading to severe internal bleeding is a significant potential complication of a treated aneurysm. Even after treatment, there is a risk that the aneurysm could rupture, especially if the treatment was not entirely successful or if the aneurysm was particularly large or complex. A rupture can lead to life-threatening internal bleeding and requires immediate medical attention. This is why ongoing monitoring and follow-up care are crucial for patients who have had an aneurysm treated.
Choice C Reason:
Decreased risk of blood clot formation is another desired outcome rather than a complication. Treating an aneurysm often involves measures to prevent blood clots, such as using anticoagulant medications. A successful treatment should reduce the risk of clot formation, which can otherwise lead to complications like stroke or embolism.
Choice D Reason:
Reduced risk of infection is also a desired outcome of aneurysm treatment. Infection can be a complication of any surgical procedure, including those used to treat aneurysms. However, with proper surgical techniques and post-operative care, the risk of infection can be minimized. Therefore, a reduced risk of infection is not a complication but rather an indication of successful treatment and good medical practice.
A nurse is monitoring the fluid replacement for a client with burn injuries. Which fluids should be administered in the first 24 hours after the burn?
Explanation
Choice A Reason:
0.9% sodium chloride is an isotonic crystalloid solution often used for fluid resuscitation. However, it is not the preferred choice for burn patients because it lacks the necessary electrolytes to replace those lost through burn injuries. While it can be used if Lactated Ringer's is unavailable, it does not provide the same balanced electrolyte composition.
Choice B Reason:
Lactated Ringer's is the preferred fluid for initial resuscitation in burn patients. It is an isotonic crystalloid solution that closely mimics the body's plasma, providing essential electrolytes such as sodium, potassium, calcium, and lactate. The lactate in the solution acts as a buffer, helping to correct metabolic acidosis, which is common in burn patients. The Parkland formula, widely used for calculating fluid needs in burn patients, specifically recommends Lactated Ringer's for the first 24 hours.
Choice C Reason:
Dextrose 5% in water is a hypotonic solution that provides free water and calories but lacks electrolytes. It is not suitable for initial fluid resuscitation in burn patients because it does not address the electrolyte imbalances and large fluid shifts that occur after a burn injury. Using this solution could lead to further complications such as hyponatremia.
Choice D Reason:
Dextrose 5% in 0.9% sodium chloride is a hypertonic solution that provides both glucose and electrolytes. However, it is not typically used for initial burn resuscitation because the high glucose content can lead to hyperglycemia, which is detrimental to burn patients. Additionally, the solution's osmolarity can exacerbate fluid shifts and worsen edema.
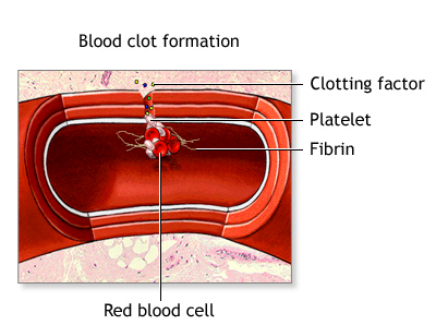
Which of the following are risk factors for disseminated intravascular coagulation (DIC)? (Select all that apply.)
Explanation
Choice A Reason:
Cancer is a significant risk factor for DIC, particularly certain types of leukemia and metastatic cancers. Cancer can trigger DIC through the release of procoagulant substances from tumor cells, leading to widespread clotting and subsequent bleeding. The hypercoagulable state associated with malignancies increases the risk of thrombotic events, which can precipitate DIC. Patients with advanced cancer are particularly susceptible due to the aggressive nature of the disease and the body's inflammatory response.
Choice B Reason:
Sepsis is one of the most common causes of DIC. Sepsis triggers a systemic inflammatory response that activates the coagulation cascade, leading to the formation of microthrombi throughout the vasculature. This widespread clotting depletes clotting factors and platelets, resulting in a paradoxical increase in bleeding risk. The severity of sepsis correlates with the likelihood of developing DIC, making early recognition and treatment of sepsis crucial.
Choice C Reason:
Trauma can lead to DIC through extensive tissue injury and the release of tissue factor into the bloodstream. Severe trauma, such as that from major accidents or surgeries, can overwhelm the body's hemostatic mechanisms, leading to uncontrolled clotting and bleeding. The inflammatory response to trauma further exacerbates the coagulation process, increasing the risk of DIC. Prompt management of traumatic injuries and monitoring for signs of DIC are essential in these patients.
Choice D Reason:
Pregnancy complications such as placental abruption, amniotic fluid embolism, and severe preeclampsia can precipitate DIC. These conditions cause significant endothelial damage and the release of procoagulant substances, triggering the coagulation cascade. The physiological changes during pregnancy, including increased blood volume and hypercoagulability, further predispose pregnant women to DIC. Early intervention and management of pregnancy-related complications are vital to prevent DIC.
Choice E Reason:
Blood transfusion reactions can lead to DIC through immune-mediated mechanisms. Incompatible blood transfusions can cause hemolysis and the release of procoagulant substances, initiating the coagulation cascade. The resulting widespread clotting and consumption of clotting factors can lead to bleeding complications. Careful matching of blood products and monitoring for transfusion reactions are critical to prevent DIC in transfusion recipients.
A nurse in the emergency department is attending to a client with extensive partial and full-thickness burns on the head. When planning the client's care, which risk should the nurse prioritize for assessment and intervention?
Explanation
Choice A Reason:
Fluid imbalance is a significant concern in burn patients due to the loss of fluids through damaged skin. This can lead to hypovolemic shock if not managed properly. However, while fluid resuscitation is crucial, it is not the immediate priority over airway management in the case of burns to the head and neck. Ensuring the airway is clear and unobstructed takes precedence because airway compromise can lead to rapid deterioration and death.
Choice B Reason:
Airway obstruction is the most critical risk in patients with extensive burns to the head and neck. Burns in these areas can cause swelling, leading to airway compromise. Inhalation injuries from smoke or hot gases can also cause airway edema and respiratory distress. Immediate assessment and intervention to secure the airway are paramount to prevent hypoxia and ensure the patient can breathe adequately. This is why airway management is the top priority in such cases.
Choice C Reason:
Infection is a major risk for burn patients due to the loss of the skin barrier, which normally protects against pathogens. Burn wounds are highly susceptible to bacterial colonization and infection, which can lead to sepsis if not properly managed. While infection control is vital, it is not the immediate priority over securing the airway in the acute phase of burn management. Once the airway is secured, infection prevention and control measures can be implemented.
A nurse is looking after a client with a traumatic brain injury. Which signs of increased intracranial pressure should the nurse monitor for?
Explanation
Choice A Reason:
Hypotension is not typically a direct manifestation of increased intracranial pressure (ICP). In fact, increased ICP often leads to hypertension as part of Cushing's triad, which includes hypertension, bradycardia, and irregular respiration. Hypotension may indicate other issues such as shock or blood loss but is not a primary indicator of increased ICP.
Choice B Reason:
Tachypnea, or rapid breathing, is not a primary sign of increased ICP. While respiratory changes can occur with increased ICP, they are more likely to present as irregular breathing patterns rather than simply an increased rate. Tachypnea might be seen in conditions like anxiety, pain, or respiratory distress but is not a hallmark of increased ICP.
Choice C Reason:
Bilateral weakness of extremities can occur with increased ICP, especially if there is significant brain swelling or herniation affecting motor pathways. However, it is not the most immediate or specific sign. Other neurological deficits can also cause bilateral weakness, so it is not solely indicative of increased ICP.
Choice D Reason:
Decreased level of consciousness is a critical and primary sign of increased ICP. As pressure within the skull rises, it can compress brain structures and impair function, leading to altered mental status ranging from confusion to coma. Monitoring the level of consciousness is essential in assessing and managing patients with potential increased ICP.
A nurse is assessing a client who has been brought to the emergency room with burn injuries. Which of the following findings should the nurse recognize as indicative of a deep partial-thickness burn?
Explanation
Choice A Reason:
Deep partial-thickness burns, also known as second-degree burns, typically present with a pink or red color and blisters. These burns extend into the deeper layers of the dermis but do not affect the full thickness of the skin. The presence of blisters indicates that the burn has penetrated the epidermis and reached the dermis, causing fluid accumulation between these layers.
Choice B Reason:
The burned area being yellow in color with severe edema is more indicative of a full-thickness burn or a severe infection. Full-thickness burns (third-degree burns) often appear white, brown, or black and are characterized by a leathery texture. Severe edema can occur with any burn but is not specific to deep partial-thickness burns.
Choice C Reason:
A burned area that is red in color with eschar present suggests a full-thickness burn. Eschar is a hard, leathery crust that forms over a full-thickness burn as the skin dies and coagulates. This type of burn destroys both the epidermis and dermis, and the presence of eschar indicates a more severe injury than a deep partial-thickness burn.
Choice D Reason:
A burned area that is black in color and pain is absent is characteristic of a full-thickness burn. In these burns, the nerve endings are destroyed, leading to a lack of pain sensation. The black color indicates necrosis of the skin and underlying tissues, which is not seen in deep partial-thickness burns.
A nurse is attending to a client who was brought to the emergency department (ED) by EMS after losing consciousness from diving into a lake. The client was intubated by paramedics in the field. A CT scan of the head and neck showed a spinal cord injury at the C3-4 level. What should be the nurse's priority action?
Explanation
Choice A Reason:
Maintaining the cervical collar in place is crucial for a client with a spinal cord injury at the level of C3-4. This action prevents further damage to the spinal cord by immobilizing the neck and maintaining proper alignment. Any movement could exacerbate the injury, potentially leading to more severe neurological deficits or even paralysis.
Choice B Reason:
Asking the client if they remember any events around the time of the injury is not the priority in this situation. While obtaining a history is important, it should not take precedence over stabilizing the spinal cord to prevent further injury. The primary focus should be on ensuring the client's safety and preventing additional harm.
Choice C Reason:
Explaining to the client that they will never be able to walk again is inappropriate and premature. The prognosis for spinal cord injuries can vary widely, and it is essential to provide accurate information based on a thorough assessment and consultation with specialists. Additionally, delivering such news requires sensitivity and should be done in a supportive manner.
Choice D Reason:
Notifying the client's parents that they are in the ED is important for family communication and support. However, it is not the immediate priority. The primary focus should be on stabilizing the client's condition and preventing further injury. Once the client is stabilized, the nurse can then inform the family.
Which stage of shock is defined by low blood pressure and insufficient tissue perfusion?
Explanation
Choice A Reason:
The irreversible stage of shock, also known as the terminal stage, is characterized by severe organ damage and failure. At this point, the body's compensatory mechanisms have failed, and recovery is unlikely. Decreased blood pressure and inadequate tissue perfusion are present, but they are more pronounced in the progressive stage.
Choice B Reason:
The refractory stage is often used interchangeably with the irreversible stage. It signifies a point where shock has progressed to such an extent that treatment is no longer effective. The body's organs have sustained irreversible damage, and despite medical intervention, the patient is unlikely to survive.
Choice C Reason:
The progressive stage of shock is characterized by a significant drop in blood pressure and inadequate tissue perfusion. During this stage, the body's compensatory mechanisms begin to fail, leading to worsening hypoperfusion and cellular damage. This stage is critical as it marks the transition from reversible to potentially irreversible damage if not promptly treated.
Choice D Reason:
The compensatory stage, also known as the non-progressive stage, involves the body's initial response to shock. During this stage, mechanisms such as increased heart rate and vasoconstriction work to maintain blood pressure and perfusion to vital organs. Blood pressure may still be within normal limits, and tissue perfusion is maintained, albeit at a reduced level.
What is an important teaching point to cover when educating a client about disseminated intravascular coagulation (DIC)?
Explanation
Choice A Reason:
Consuming a diet high in vitamin K to promote clotting is not typically recommended for patients with DIC. While vitamin K is essential for clotting, DIC involves both excessive clotting and bleeding. Increasing vitamin K intake could exacerbate clotting issues without addressing the underlying imbalance.
Choice B Reason:
Stopping all medications to prevent interactions with clotting factors is not advisable. Patients with DIC often require medications to manage their condition, including anticoagulants and treatments for the underlying cause. Discontinuing all medications could lead to uncontrolled symptoms and complications.
Choice C Reason:
Engaging in physical activity to promote blood flow is generally beneficial for overall health, but in the context of DIC, it must be approached with caution. Physical activity can increase the risk of injury and bleeding, which is a significant concern for patients with DIC. Therefore, any exercise regimen should be carefully monitored and tailored to the patient's condition.
Choice D Reason:
Avoiding activities that may cause injury or bleeding is crucial for patients with DIC. Due to the risk of spontaneous bleeding and the potential for minor injuries to lead to significant blood loss, patients must take precautions to minimize these risks. This includes avoiding contact sports, using soft-bristled toothbrushes, and being cautious with sharp objects.
Which of the following factors has a direct impact on stroke volume?
Explanation
Choice A Reason:
Blood pressure itself does not directly affect stroke volume. However, it can influence afterload, which in turn affects stroke volume. Blood pressure is the force exerted by circulating blood on the walls of blood vessels, and while it is related to cardiac function, it is not a direct determinant of stroke volume.
Choice B Reason:
Preload directly affects stroke volume. Preload refers to the degree of stretch of the cardiac muscle fibers at the end of diastole, just before contraction. It is influenced by the volume of blood returning to the heart (venous return). According to the Frank-Starling law, an increase in preload leads to an increase in stroke volume due to the enhanced force of contraction.
Choice C Reason:
Afterload also directly affects stroke volume. Afterload is the resistance the ventricles must overcome to eject blood during systole. It is influenced by factors such as arterial blood pressure and vascular resistance. An increase in afterload can decrease stroke volume because the heart has to work harder to pump blood against the higher resistance.
Choice D Reason:
Heart rate does not directly affect stroke volume. Instead, heart rate and stroke volume together determine cardiac output (CO = HR × SV). While heart rate can influence the overall amount of blood pumped by the heart per minute, it does not directly change the volume of blood ejected with each beat.
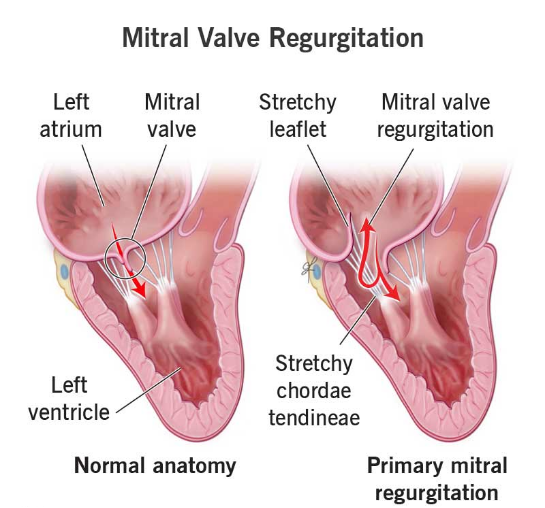
James, the ICU nurse, is assessing a client with mitral valve insufficiency. What findings should the nurse anticipate?
Explanation
Choice A Reason:
Neck vein distention is a common finding in patients with mitral valve insufficiency. This condition leads to increased pressure in the left atrium, which can back up into the pulmonary veins and subsequently the right side of the heart, causing jugular venous distention.
Choice B Reason:
Splenomegaly is not typically associated with mitral valve insufficiency. It is more commonly seen in conditions like liver disease, hematologic disorders, and infections. Mitral valve insufficiency primarily affects the heart and lungs rather than the spleen.
Choice C Reason:
Petechiae are small, red or purple spots caused by bleeding into the skin. They are not a common finding in mitral valve insufficiency. Petechiae are more often associated with conditions that affect platelet function or coagulation, such as thrombocytopenia or vasculitis.
Choice D Reason:
An S4 heart sound, also known as an atrial gallop, can be heard in patients with mitral valve insufficiency. This sound occurs due to the atria contracting forcefully to overcome a stiff or hypertrophic ventricle, which is often a result of chronic pressure overload from the regurgitant flow.
What is the function of a hemodynamic monitoring system?
Explanation
Choice A Reason:
Monitoring the client's respiratory status and oxygen saturation is important but not the primary purpose of a hemodynamic monitoring system. Hemodynamic monitoring focuses on the cardiovascular system, including parameters like cardiac output, stroke volume, and systemic vascular resistance.
Choice B Reason:
Evaluating the client's renal function and electrolyte balance is crucial in overall patient care but is not the main focus of hemodynamic monitoring. Hemodynamic monitoring systems are designed to assess cardiovascular function rather than renal function.
Choice C Reason:
Monitoring the client's neurological status and intracranial pressure is essential in certain clinical situations, such as traumatic brain injury. However, this is not the primary purpose of hemodynamic monitoring, which is centered on cardiovascular assessment.
Choice D Reason:
The primary purpose of a hemodynamic monitoring system is to measure and assess the client's cardiovascular status and function. This includes monitoring parameters such as blood pressure, cardiac output, and tissue perfusion to ensure adequate organ perfusion and guide treatment decisions.
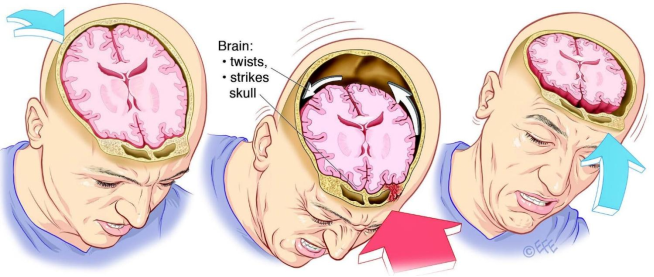
A nurse in the emergency department is looking after a client with a contusion from a motor-vehicle accident. Which of the following findings would be expected in this situation?
Explanation
Choice A Reason:
Narrowing pulse pressure is not typically associated with contusions from a motor-vehicle crash. It is more commonly seen in conditions like cardiac tamponade or severe blood loss. While it can indicate a serious condition, it is not a direct result of a contusion.
Choice B Reason:
Drainage of clear fluid from the ears, known as otorrhea, can indicate a basilar skull fracture rather than a simple contusion. This finding suggests cerebrospinal fluid leakage, which is a serious complication requiring immediate medical attention.
Choice C Reason:
Periods of unconsciousness and/or confusion are expected findings in clients with contusions, especially if the brain is involved. These symptoms indicate a concussion or more severe brain injury, which can result from the impact of a motor-vehicle crash.
Choice D Reason:
Extensive bruising in the mastoid area, known as Battle's sign, is indicative of a basilar skull fracture rather than a contusion. This type of bruising appears behind the ear and is a sign of a more severe head injury.
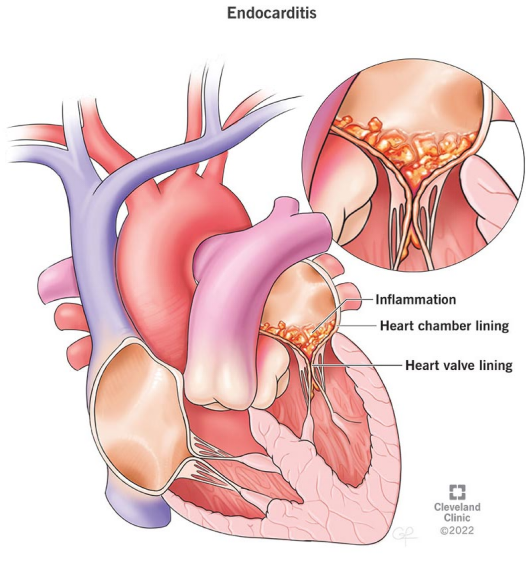
Which of the following is a complex symptom of infective endocarditis?
Explanation
Choice A Reason:
Reduced blood pressure is not a specific complication of infective endocarditis. While hypotension can occur in severe cases due to septic shock, it is not a hallmark of the disease. Infective endocarditis primarily affects the heart valves and can lead to embolic events, heart failure, and other complications.
Choice B Reason:
Osler's nodes are a classic sign of infective endocarditis. These are painful, red or purple, raised lesions found on the hands and feet. They are caused by immune complex deposition and are indicative of the systemic nature of the infection. Their presence can help in the clinical diagnosis of infective endocarditis.
Choice C Reason:
Clear lung sounds are not a complication of infective endocarditis. In fact, clear lung sounds would generally indicate that there is no pulmonary involvement or congestion. Complications of infective endocarditis are more likely to involve the heart, kidneys, and other organs through embolic events.
Choice D Reason:
Increased appetite is not associated with infective endocarditis. Patients with this condition often experience symptoms such as fever, fatigue, and weight loss due to the chronic infection. Increased appetite would be an unusual finding and not related to the disease process.
A nurse is caring for a client with a halo fixation device. Which of the following actions should be part of the care plan?
Explanation
Choice A Reason:
Monitoring the client for an elevated temperature is crucial because it can indicate an infection at the pin sites or other complications. Infections are a common risk with halo fixation devices due to the invasive nature of the pins.
Choice B Reason:
Ensuring the halo jacket is snug against the client's skin is incorrect. The halo jacket should fit properly but not be too tight, as this can cause skin breakdown and discomfort. There should be enough space to insert a flat hand between the vest and the skin.
Choice C Reason:
Providing range of motion to the client's neck is not appropriate for a client with a halo fixation device. The purpose of the halo is to immobilize the neck to allow for proper healing of cervical injuries. Any movement could jeopardize the stability of the injury.
Choice D Reason:
Removing the vest daily to inspect the client's skin integrity is incorrect. The halo vest should not be removed frequently as it is meant to provide continuous immobilization. Skin integrity can be monitored by checking the areas around the vest without removing it.
A nurse is caring for a client with paraplegia resulting from a spinal cord injury. After a week on the unit, the nurse observes that the client is becoming withdrawn and increasingly resistant to rehabilitation efforts by the staff. What action should the nurse take?
Explanation
Choice A Reason:
Allowing the client to control the timing and frequency of the therapy might seem beneficial, but it can lead to inconsistent participation and lack of progress. Structured therapy sessions are essential for rehabilitation, and while some flexibility is important, a completely client-controlled schedule may not provide the necessary consistency.
Choice B Reason:
Limiting visiting hours until the client begins to participate in therapy is not an effective approach. Social support from family and friends is crucial for the emotional well-being of the client and can actually motivate them to engage more in their rehabilitation efforts. Restricting visits could lead to increased feelings of isolation and resistance.
Choice C Reason:
Establishing a plan of care with the client that sets attainable goals is the most effective approach. Involving the client in their care plan fosters a sense of ownership and motivation. Setting realistic and achievable goals helps the client see progress, which can boost their confidence and willingness to participate in therapy.
Choice D Reason:
Informing the client that privileges are related to participation in therapy can be perceived as punitive and may not be effective in motivating the client. It is important to use positive reinforcement and encouragement rather than threats or restrictions to foster cooperation and engagement in the rehabilitation process.
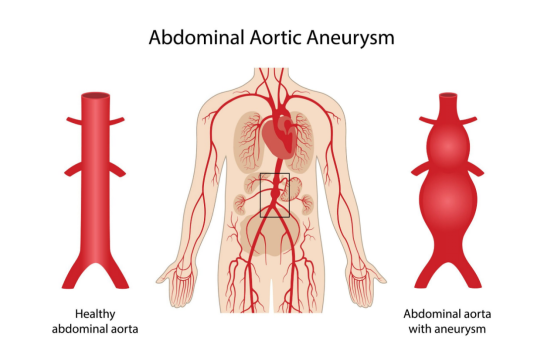
The nurse is caring for a client with an abdominal aortic aneurysm (AAA). Which vital sign should be prioritized for monitoring?
Explanation
Choice A Reason:
Core temperature is important to monitor in many clinical situations, but it is not the primary concern for a client with an abdominal aortic aneurysm. While fever can indicate infection, which is a potential complication, it is not directly related to the immediate risks associated with AAA.
Choice B Reason:
Blood pressure is the most critical vital sign to monitor in a client with an abdominal aortic aneurysm. Elevated blood pressure can increase the risk of aneurysm rupture, which is a life-threatening emergency. Maintaining blood pressure within a safe range is essential to prevent complications and ensure the stability of the aneurysm.
Choice C Reason:
Pulse rate is also important to monitor, but it is not as directly indicative of the risk of aneurysm rupture as blood pressure. While changes in pulse rate can signal cardiovascular stress or other issues, blood pressure provides more direct information about the forces acting on the aneurysm.
Choice D Reason:
Respiratory rate is a vital sign that can indicate respiratory distress or other systemic issues, but it is not the primary concern in the context of an abdominal aortic aneurysm. Blood pressure remains the most critical parameter to monitor to prevent rupture and manage the condition effectively.
What is the normal measurement range for cardiac output in adults?
Explanation
Choice A Reason:
The range of 0.5-1 L/min is significantly lower than the normal cardiac output for adults. Such low values could indicate severe heart failure or other critical conditions where the heart is unable to pump sufficient blood to meet the body's needs.
Choice B Reason:
A cardiac output of 10-12 L/min is higher than the normal range for adults at rest. This level of cardiac output might be seen during intense physical activity or in conditions like hyperthyroidism, where the heart pumps more blood to meet increased metabolic demands.
Choice C Reason:
The normal range for cardiac output in adults is typically between 4-6 L/min. This range represents the volume of blood the heart pumps per minute at rest, ensuring adequate perfusion of tissues and organs. Cardiac output can vary based on factors such as age, body size, and physical activity.
Choice D Reason:
A cardiac output of 15-20 L/min is extremely high and would generally be seen only during extreme physical exertion or in pathological conditions. Such high values are not typical for resting adults and indicate a state of increased cardiac demand.
A nurse is assessing a client with a basal skull fracture and observes a thin stream of clear fluid coming from the client's right nostril. What should the nurse's initial action be?
Explanation
Choice A Reason:
Suctioning the nose is not the first action to take. Suctioning can increase intracranial pressure and potentially cause further injury. It is important to first determine the nature of the drainage before taking any invasive actions.
Choice B Reason:
Notifying the physician is important, but it should be done after confirming the nature of the drainage. Testing the fluid for glucose can help determine if it is cerebrospinal fluid (CSF), which would indicate a serious complication requiring immediate medical attention.
Choice C Reason:
Testing the drainage for glucose is the correct first action. CSF contains glucose, so a positive test would confirm that the clear fluid is CSF. This is a critical step in diagnosing a CSF leak, which can occur with basal skull fractures and requires prompt intervention to prevent infection and other complications.
Choice D Reason:
Asking the client to blow their nose is contraindicated. Blowing the nose can increase intracranial pressure and exacerbate a CSF leak. It is important to avoid any actions that could worsen the condition until the nature of the drainage is confirmed.
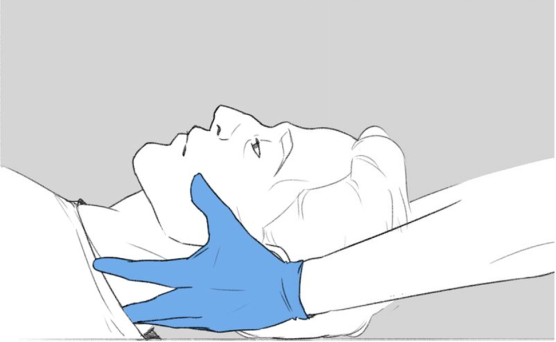
The nurse is attending to a client who was brought to the emergency department after a head-on collision. The client is unresponsive, has respirations of 22/min, and a bleeding forehead laceration. What is the priority nursing action in this situation?
Explanation
Choice A Reason:
Establishing IV access and starting fluid replacement is important for maintaining hemodynamic stability, especially if there is significant blood loss. However, it is not the immediate priority in this scenario. Ensuring the neck is stabilized takes precedence to prevent potential spinal cord injury.
Choice B Reason:
Inserting a nasogastric tube is not a priority in the acute management of a trauma patient with a head injury. This procedure can be deferred until the patient's airway and cervical spine are secured and other life-threatening conditions are addressed.
Choice C Reason:
Keeping the neck stabilized is the priority action. In a trauma patient with a head injury, there is a high risk of cervical spine injury. Stabilizing the neck prevents further damage to the spinal cord, which could result in paralysis or other severe complications.
Choice D Reason:
Monitoring pulse and blood pressure frequently is essential for assessing the patient's hemodynamic status. However, it is not the immediate priority over stabilizing the cervical spine. Once the neck is stabilized, continuous monitoring of vital signs should follow.
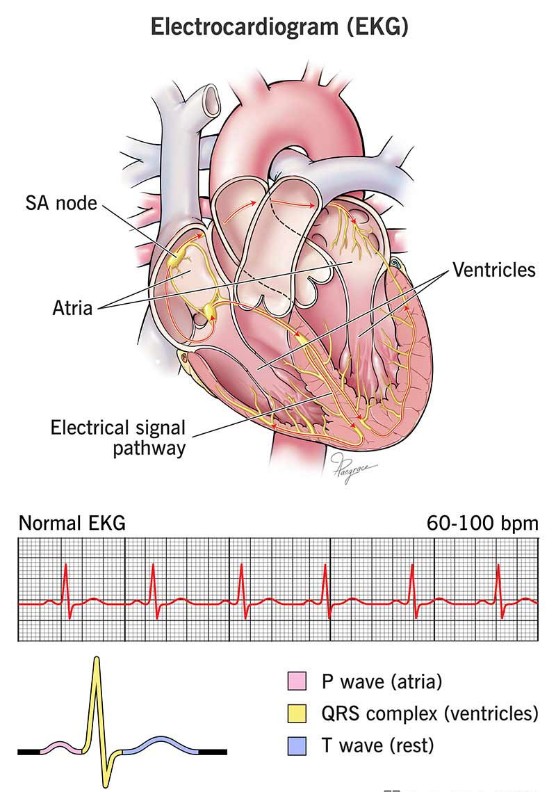
Which diagnostic test is frequently utilized to assess heart failure?
Explanation
Choice A Reason:
Pulmonary function tests are used to assess lung function and diagnose respiratory conditions such as asthma, chronic obstructive pulmonary disease (COPD), and other lung disorders. While heart failure can affect lung function, pulmonary function tests are not specifically used to diagnose heart failure.
Choice B Reason:
An electrocardiogram (ECG) is a common diagnostic test used to assess heart failure. It records the electrical activity of the heart and can detect abnormalities in heart rhythm, heart size, and the presence of ischemia or infarction. ECGs are crucial in diagnosing and monitoring heart conditions, including heart failure.
Choice C Reason:
Urinalysis is a test that examines the content of urine and is used to diagnose and monitor kidney function, urinary tract infections, and other metabolic conditions. It is not specifically used to diagnose heart failure, although kidney function can be affected by heart failure.
Choice D Reason:
A complete blood count (CBC) measures the levels of different blood cells, including red blood cells, white blood cells, and platelets. While a CBC can provide valuable information about a patient's overall health and detect conditions like anemia or infection, it is not specifically used to diagnose heart failure.
A nurse is caring for a client with burns on the face, ears, and eyelids. Which of the following findings should the nurse prioritize reporting to the provider?
Explanation
Choice A Reason:
Difficulty swallowing is a critical finding in a client with burns to the face, ears, and eyelids. This symptom can indicate airway edema or obstruction, which is a life-threatening condition. Burns in these areas can cause significant swelling, leading to compromised airways. Immediate intervention is required to secure the airway and prevent respiratory failure.
Choice B Reason:
Pain of 6 on a scale of 0 to 10 is important to manage for patient comfort and to prevent complications related to pain, such as increased heart rate and blood pressure. However, it is not the immediate priority over potential airway compromise. Pain management can be addressed once the airway is secured.
Choice C Reason:
A heart rate of 122/min indicates tachycardia, which can be a response to pain, stress, or hypovolemia. While it is important to monitor and manage, it is not as immediately life-threatening as airway obstruction. Tachycardia can be addressed after ensuring the airway is clear.
Choice D Reason:
Urinary output of 25 mL/hr is below the normal range (typically 30-50 mL/hr) and can indicate dehydration or renal impairment. While this is a concerning finding, it is not the immediate priority compared to securing the airway. Fluid resuscitation and renal function can be managed once the airway is stabilized.
Sign Up or Login to view all the 29 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
