ATI Nursing Care of Children Maternal Newborn Assessment
Total Questions : 49
Showing 25 questions, Sign in for moreA nurse is reinforcing teaching with a client who is postpartum and is taking docusate sodium to prevent constipation. Which of the following instructions should the nurse include?
Explanation
Choice A reason:
Take this medication every day for regular bowel movements. Rationale: This choice is incorrect. Docusate sodium is a stool softener used to prevent constipation, but it should not be taken daily for regular bowel movements. Overuse of stool softeners can lead to dependence and may disrupt the natural bowel function.
Choice B reason:
Take the medication with mineral oil. Rationale: This choice is incorrect. Docusate sodium should not be taken with mineral oil. When taken together, they can form a mixture that is difficult for the body to absorb, leading to potential adverse effects.
Choice C reason:
Decrease dietary fiber intake while taking this medication. Rationale: This choice is incorrect. It is not advisable to decrease dietary fiber intake while taking docusate sodium. Fiber is essential for promoting regular bowel movements and overall gastrointestinal health.
Combining the medication with a high-fiber diet can enhance its effectiveness.
Choice D reason:
 Take the medication with a full glass of water. Rationale: This choice is correct. The nurse should instruct the client to take docusate sodium with a full glass of water. The water helps to soften the stool and allows the medication to work effectively in preventing constipation.
Take the medication with a full glass of water. Rationale: This choice is correct. The nurse should instruct the client to take docusate sodium with a full glass of water. The water helps to soften the stool and allows the medication to work effectively in preventing constipation.
A nurse is caring for a 9-year-old client who is immediately postoperative. The client is nonverbal and has both cognitive and developmental delays. Which of the following pain scales should the nurse use to evaluate the client's pain?
Explanation
Choice A reason:
The FACES Scale is a visual pain scale typically used for children who can understand and verbalize their pain intensity. It consists of a series of faces with varying expressions, from smiling to crying, to help the child express their pain level. However, since the client in question is nonverbal and has cognitive and developmental delays, this scale may not be suitable as they might not be able to communicate using this tool effectively.
Choice B reason:
The Numerical Scale involves asking the patient to rate their pain on a scale of 0 to 10, with 0 being no pain and 10 being the worst pain imaginable. While this scale is commonly used for older children and adults, it may not be appropriate for a nonverbal and developmentally delayed 9-year-old client, as they may not understand or be able to use numbers effectively to express their pain.
Choice C reason:
The FLACC pain assessment scale is designed for nonverbal or preverbal individuals, including children and those with cognitive impairments. FLACC stands for Face, Legs, Activity, Cry, and Consolability. Each category is scored from 0 to 2 or 0 to 3, depending on the version used, based on specific observed behaviors. The scores are then totaled to give an overall pain assessment. This scale is particularly suitable for the current client's condition as it focuses on observable behaviors rather than verbal communication.
Choice D reason:
The Visual Analog Scale (VAS) requires the patient to mark a point along a line that represents their pain intensity, with one end indicating no pain and the other end indicating the worst pain. Although this scale is useful for older children and adults, it may not be appropriate for a 9-year-old client with cognitive and developmental delays who might not fully comprehend the concept of the scale.
A nurse is assisting with the care of a client who is receiving epidural anesthesia for pain management during labor. Which of the following actions should the nurse take?
Explanation
Choice A reason:
The nurse should not remind the client to void every 4 hours because epidural anesthesia can cause temporary loss of bladder sensation, making it difficult for the client to know when to void. Instead, the nurse should use a bladder scanner to assess for urinary retention and encourage the client to void regularly.
Choice B reason:
Encouraging the client to alternate from side to side every 2 hours is not directly related to the administration of epidural anesthesia. This action is commonly advised for clients who are on bed rest to prevent pressure ulcers and promote circulation. However, it is not specifically necessary for the client receiving epidural anesthesia for pain management during labor.
Choice C reason:
Raising the four side rails on the client's bed is not necessary in this situation. The use of side rails should be based on the client's mobility and risk assessment for falls. If the client is receiving epidural anesthesia, they may experience reduced mobility, but the decision to use side rails should be made on an individual basis, not solely based on the anesthesia.
Choice D reason:
Monitoring the client's blood pressure is a crucial action when a client is receiving epidural anesthesia. Epidural anesthesia can cause a drop in blood pressure, leading to hypotension. By regularly monitoring the client's blood pressure, the nurse can detect any significant changes and take appropriate actions to maintain hemodynamic stability.
A nurse is reinforcing teaching with a parent of a school-age child who has tonic-clonic seizures. Which of the following statements should the nurse make regarding care during a seizure?
Explanation
Choice A reason:
The nurse should not offer the child sips of clear liquids during a seizure. During a tonic-clonic seizure, the child's swallowing reflex may be impaired, and giving liquids could lead to aspiration or choking, causing further complications.
Choice B reason:
The nurse should not restrain the child during a seizure using both arms or any other means. Restraint can potentially lead to injury for both the child and the person attempting to restrain them. It is crucial to allow the child to move freely during the seizure to prevent harm.
Choice C reason:

Placing the child's head on a pillow is the correct choice. This positioning helps to protect the child's head from injury during the seizure. The pillow provides a cushioning effect, minimizing the risk of head trauma.
Choice D reason:
The nurse should not instruct the parent to give rectal diazepam to the child at the onset of the seizure unless specifically prescribed by the child's healthcare provider. Diazepam is a medication used to manage seizures, but its administration route and timing should be determined by the child's healthcare provider. Inappropriate use of medication can be dangerous and ineffective.
A nurse is collecting data from an infant who has Hirschsprung's disease. Which of the following manifestations should the nurse expect?
Explanation
Abdominal distention. Choice A reason:
Abdominal distention is a common manifestation of Hirschsprung's disease in infants. This condition is characterized by the absence of ganglion cells in the distal segment of the colon, leading to a functional obstruction. The absence of ganglion cells causes the affected part of the colon to become narrow and unable to relax, resulting in a buildup of stool and gas, leading to abdominal distention.
Choice B reason:
Steatorrhea, which is the presence of fatty, bulky, and foul-smelling stools, is not typically associated with Hirschsprung's disease. This manifestation is more commonly seen in conditions affecting the pancreas, liver, or small intestine, where the digestion and absorption of fats are impaired.
Choice C reason:
Blood-tinged emesis (vomiting) is not a typical manifestation of Hirschsprung's disease. This symptom is more commonly associated with gastrointestinal bleeding, which can be caused by various factors such as ulcers, esophageal varices, or gastritis.
Choice D reason:
Dysphagia, which refers to difficulty swallowing, is also not a characteristic manifestation of Hirschsprung's disease. Dysphagia is more commonly seen in conditions affecting the esophagus or throat, such as esophageal strictures or neurological disorders affecting swallowing reflexes.
A nurse is collecting data from an adolescent who is postoperative and is receiving morphine for pain. Which of the following findings is the nurse's priority?
Explanation
Choice A reason:
The nurse's priority in this situation is the respiratory rate of 10/min. A respiratory rate of 10 breaths per minute is significantly low and could indicate respiratory depression, especially if the patient is receiving morphine, which is known to depress the respiratory system. This could lead to inadequate oxygenation, potential hypoxia, and other life-threatening complications.
Choice B reason:
Bladder distention may be a concern, but it is not the nurse's priority in this situation. Bladder distention can cause discomfort and urinary retention, but it is not an immediate life- threatening condition compared to potential respiratory depression.
Choice C reason:
A blood pressure of 108/64 mm Hg is within the normal range for an adolescent and may not be the nurse's priority at this time. Although it should be monitored, it does not pose an immediate threat to the patient's life.
Choice D reason:
Nausea and vomiting are common side effects of morphine administration, but they are not the nurse's priority in this situation. While they can cause distress and discomfort to the patient, they are not life-threatening conditions.
A nurse is caring for a client who is postpartum, reports an allergy to aspirin, and states that they are in pain. The nurse should identify which of the following medications as safe to administer to the client?
Explanation
Choice A reason:
Ibuprofen - Ibuprofen belongs to the nonsteroidal anti-inflammatory drugs (NSAIDs) class, which includes aspirin. Since the client reports an allergy to aspirin, there is a risk of cross- reactivity, leading to a potential allergic reaction. Therefore, Ibuprofen should be avoided.
Choice B reason:
Acetaminophen - Acetaminophen is not an NSAID, and it works differently from aspirin. It is a safe option for the client in the postpartum period to manage pain without causing a cross- reaction with their aspirin allergy. Acetaminophen primarily acts on the central nervous system to reduce pain and fever, making it suitable for the client.
Choice C reason:
Naproxen - Naproxen is also an NSAID, and like Ibuprofen, it carries the risk of cross-reactivity in someone allergic to aspirin. Therefore, Naproxen should be avoided in this client.
Choice D reason:
Celecoxib - Celecoxib is a type of NSAID known as a selective cyclooxygenase-2 (COX-2) inhibitor. Although it is a bit more selective and generally considered to have a lower risk of causing cross-reactions, it is still an NSAID and not recommended for someone with a known aspirin allergy. Hence, Celecoxib should not be administered to the client in this scenario.
A nurse is caring for a client who is at 12 weeks of gestation and is prescribed a high-protein diet. Which of the following foods should the nurse recommend as containing the highest amount of protein?
Explanation
Choice A reason:
One cup of oatmeal - Oatmeal is a nutritious food, but it does not contain as high a protein content as some other options. While it offers some protein, it is not the best choice for a high-protein diet during pregnancy. Oatmeal is primarily known for its fiber content and complex carbohydrates, which provide sustained energy.
Choice B reason:
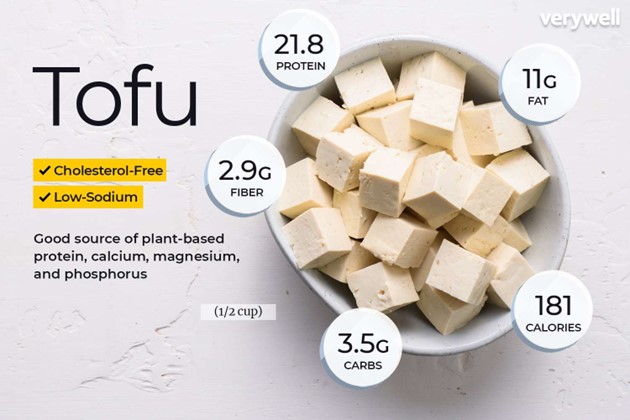 One cup of tofu - Tofu is an excellent source of protein and is a suitable choice for a high- protein diet during pregnancy. Tofu is made from soybeans and is rich in plant-based proteins, making it an ideal option for individuals following a vegetarian or vegan diet as well. Additionally, tofu contains essential amino acids, iron, calcium, and other nutrients beneficial for both the mother and the developing fetus.
One cup of tofu - Tofu is an excellent source of protein and is a suitable choice for a high- protein diet during pregnancy. Tofu is made from soybeans and is rich in plant-based proteins, making it an ideal option for individuals following a vegetarian or vegan diet as well. Additionally, tofu contains essential amino acids, iron, calcium, and other nutrients beneficial for both the mother and the developing fetus.
Choice C reason:
One cup of brown rice - While brown rice is a healthy whole grain and provides some protein, it does not have as high a protein content as tofu. Brown rice is a good source of complex carbohydrates, fiber, vitamins, and minerals, but it may not meet the high protein requirements of a pregnant woman's diet.
Choice D reason:
One cup of kale - Kale is a nutritious leafy green vegetable, but it does not offer a significant amount of protein compared to tofu. It is rich in vitamins, minerals, and antioxidants, making it a valuable addition to a balanced diet. However, for a high-protein diet during pregnancy, other options like tofu are more suitable.
A nurse is caring for an adolescent who states an intention to self-harm. Which of the following actions should the nurse take first?
Explanation
The nurse should maintain continuous observation of the adolescent.
Choice A reason:
The first and most crucial action when a patient expresses an intention to self-harm is to ensure their safety. By maintaining continuous observation, the nurse can closely monitor the adolescent's behavior and intervene promptly if any signs of self-harm emerge. This action helps prevent immediate harm and allows for timely interventions.
Choice B reason:
Applying wrist restraints to the adolescent (Choice B) would not be appropriate in this situation. Restraints are typically used as a last resort for patients who pose a danger to themselves or others and only when less restrictive measures have failed. In the case of self- harm, using restraints can increase the patient's distress and potentially worsen the situation.
Choice C reason:
Collecting data about the adolescent's mental status (Choice C) is an essential step in understanding their overall condition, but it should not be the first action taken. While gathering data is important for a comprehensive assessment, immediate safety concerns must take precedence.
Choice D reason:
Obtaining consent from the adolescent's guardian for the application of restraints (Choice D) is not the first priority when the patient expresses an intention to self-harm. The focus should be on ensuring the patient's immediate safety, and consent for restraints may be necessary only if other interventions prove inadequate.
A nurse is collecting data from a 4-year-old child during a well-child visit. Which of the following findings should the nurse expect?
Explanation
Birth weight has doubled.
Choice A reason:
The nurse should not expect a positive Babinski sign in a 4-year-old child during a well-child visit. The Babinski sign is a reflex seen in infants up to about 1 year of age and disappears as the nervous system matures. Its presence in a 4-year-old would be abnormal and may indicate neurological issues.
Choice B reason:
The nurse should not expect birth height to double in a 4-year-old child during a well-child visit. While children do experience significant growth in their early years, it is unlikely that birth height will have doubled by the age of 4. Doubling of birth height would be an atypical finding.
Choice C reason:
The correct choice. The nurse should expect that the child's birth weight has doubled during a well-child visit. From birth to age 4, children typically experience substantial weight gain, and doubling of birth weight is a common milestone in healthy development.
Choice D reason:
The nurse should not expect the presence of permanent teeth in a 4-year-old child during a well-child visit. Permanent teeth typically begin to emerge around 6 years of age and continue to erupt over the following years. The appearance of permanent teeth at age 4 would be premature and unusual.
A nurse is caring for an infant who has pertussis. Which of the following precautions should the nurse implement?
Explanation
Choice A reason:
Airborne precautions are implemented for diseases that spread through small airborne particles, such as tuberculosis or measles. These diseases can remain suspended in the air for extended periods and be inhaled by others. Pertussis, also known as whooping cough, is primarily spread through respiratory droplets when an infected person coughs or sneezes, making airborne precautions unnecessary.
Choice B reason:
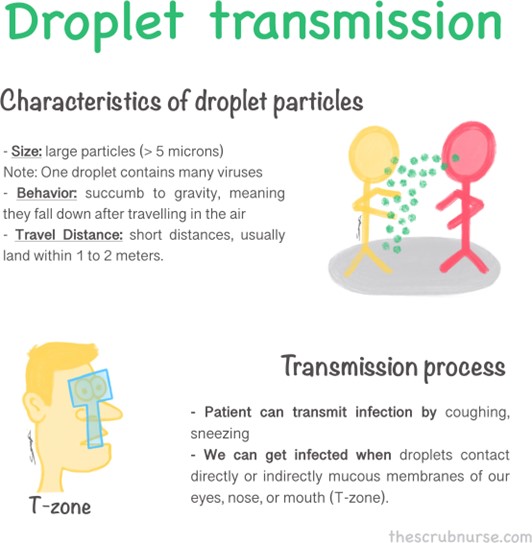
Droplet precautions are appropriate for illnesses that spread through respiratory droplets produced when an infected person talks, coughs, or sneezes. Pertussis falls into this category as it is transmitted mainly through respiratory droplets. By implementing droplet precautions, the nurse will minimize the risk of transmission to others, including healthcare workers and other patients.
Choice C reason:
Standard precautions are the baseline infection prevention practices used for all patients to prevent the spread of infections in healthcare settings. While important, they may not be sufficient to control the transmission of pertussis, as it requires additional measures like droplet precautions due to its specific mode of transmission.
Choice D reason:
Neutropenic precautions are used for patients with compromised immune systems, particularly those with low white blood cell counts (neutropenia). The purpose is to protect these vulnerable individuals from exposure to infectious agents. However, pertussis precautions are different and do not fall under the neutropenic category.
A nurse is reinforcing teaching with the parent of a school-age child who has ADHD and a new prescription for a methylphenidate transdermal patch. Which of the following statements by the parent indicates an understanding of the teaching?
Explanation
"I will reinforce the patch edges with clear tape if they don't lie flat.".
Choice A reason:
Placing a heat pack on the patch to improve adhesion is not recommended. Heat can potentially increase the absorption of the medication and lead to adverse effects. Applying additional heat to the patch can be dangerous and may cause an overdose or other complications.
Choice B reason:
Placing the patch on the back side of the child's arm is not the correct application site for a methylphenidate transdermal patch. The appropriate site for application is typically the hip or the top of the buttocks. The back of the arm may not provide proper absorption and can result in suboptimal medication delivery.
Choice C reason:
This statement indicates an understanding of the teaching. Reinforcing the patch edges with clear tape if they don't lie flat is a recommended step to ensure proper adhesion of the patch. If the edges of the patch lift or don't stick properly, using clear tape can help keep the patch securely in place, ensuring continuous and consistent drug delivery.
Choice D reason:
Leaving the patch in place for no more than 9 hours is incorrect. The duration of wear for a methylphenidate transdermal patch varies depending on the specific brand and formulation. Typically, these patches are designed for 9 to 12 hours of wear, and leaving them on for a shorter duration may result in inadequate symptom control.
A nurse is collecting data from a 6-month-old infant. Which of the following findings should the nurse expect?
Explanation
Choice C reason: The infant makes babbling sounds. At 6 months of age, it is typical for infants to engage in babbling sounds. Babbling is a significant milestone in language development during infancy. It involves the repetition of consonant-vowel combinations (e.g., "ba-ba,”. "ma-ma") and is an essential precursor to later language skills, such as forming words and sentences. The nurse should expect the 6-month-old infant to be making these babbling sounds as part of their normal development.
Choice A reason:
The infant has a pincer grasp. A pincer grasp is the ability to pick up small objects using the thumb and index finger. This fine motor skill typically develops around 9 to 12 months of age. At 6 months old, infants have not yet acquired the pincer grasp. Therefore, the nurse should not expect the 6-month-old infant to demonstrate this skill during the assessment.
Choice D reason:
The infant crawls on their hands and knees. Crawling is a gross motor skill that usually emerges between 7 to 10 months of age. While some infants may start crawling earlier or later, it is not a skill that is typically present in a 6-month-old. Therefore, the nurse should not anticipate the 6-month-old infant to be crawling on their hands and knees during the assessment.
Choice B reason:
The infant drops objects with the expectation of someone picking them up. This behavior, known as "object permanence,”. is a cognitive milestone that develops around 8 to 12 months of age. At 6 months old, infants have not yet fully developed this concept. They might drop objects as part of their exploratory behavior, but they do not yet understand the expectation of someone picking them up. Therefore, the nurse should not expect the 6- month-old infant to exhibit this specific behavior during the assessment.
A nurse in a provider's office is planning to administer immunizations to an 11-year-old child who is up to date with current recommendations. Which of the following immunizations should the nurse plan to administer?
Explanation
Choice A reason:
Hepatitis B (Hep B) The rationale for not choosing Hepatitis B is that the child is already up to date with current recommendations. If the child has received all the necessary doses of Hepatitis B vaccine according to the immunization schedule, administering an additional dose unnecessarily is not recommended. It's crucial to adhere to the recommended immunization guidelines to avoid over-vaccination.
Choice B reason:
Measles, mumps, rubella (MMR) The rationale for not choosing Measles, mumps, rubella (MMR) is the same as for choice A. If the child has already received the required doses of the MMR vaccine, giving extra doses is not necessary and may not provide any additional benefit.
Choice C reason:
Tetanus, diphtheria, and pertussis (Tdap) - Correct Answer The reason for choosing Tdap is that it is a booster dose of the vaccine, and it's usually recommended around the age of 11 years. Tdap protects against tetanus, diphtheria, and pertussis (whooping cough).
Administering this vaccine at the appropriate age helps ensure continued protection against these diseases.
Choice D reason:
Pneumococcal (PCV) The rationale for not choosing Pneumococcal (PCV) is that this vaccine is typically given in infancy and early childhood as part of the routine immunization schedule.
Since the child is 11 years old and up to date with current recommendations, they are unlikely to require another dose of PCV at this stage.
A nurse is preparing to administer an intermittent enteral feeding to a child who has an NG tube in place. Which of the following actions should the nurse take first?
Explanation
Choice A reason:
The nurse should prioritize Choice B over Choice A as it is essential to first confirm the correct placement of the NG tube before proceeding with any other actions. If the tube is not correctly positioned, administering the enteral feeding can lead to potential complications, such as aspiration, which can be life-threatening. Therefore, it is crucial to ensure the NG tube's proper placement before moving forward with the feeding
Choice B reason:
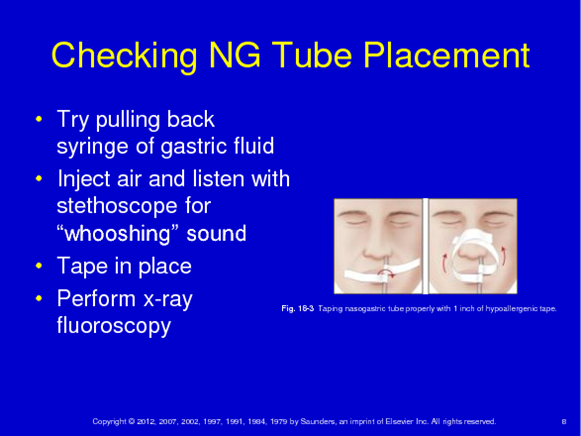
This option takes precedence as verifying the NG tube's position is a fundamental step in the enteral feeding process. The nurse must use appropriate methods, such as X-ray or pH testing, to confirm that the tube is in the stomach and not in the respiratory tract or elsewhere. This verification ensures the safety and effectiveness of the feeding procedure and prevents potential harm to the child.
Choice C reason:
While checking the gastric residual volume (GRV) is an important step in some cases, it should be done after confirming the NG tube's proper placement (Choice B). GRV provides information about the amount of feeding left in the stomach and helps in assessing tolerance to the feeding. However, if the NG tube is misplaced, determining GRV becomes irrelevant as the feeding would not be going to the intended location.
Choice D reason:
Flushing the child's NG tube with sterile water is an appropriate step during the enteral feeding process but should be done after verifying the tube's position (Choice B). Flushing ensures that the tube is patent and free from any obstructions, allowing the feeding to pass through smoothly. However, again, if the NG tube is incorrectly positioned, flushing it would not address the underlying issue.
A nurse is reviewing laboratory reports for four antepartum clients. Which of the following laboratory results should the nurse report to the provider?
Explanation
Choice D reason: The nurse should report the laboratory result of 2+ proteinuria (Choice D) to the healthcare provider. Proteinuria is the presence of excess protein in the urine, which can indicate a potential kidney problem or a complication related to pregnancy, such as preeclampsia. Preeclampsia is a serious condition characterized by high blood pressure and damage to organs like the liver and kidneys. Therefore, this result needs immediate attention to assess the client's condition properly and take appropriate actions to ensure the safety and well-being of both the mother and the baby.
Choice A reason:
The 2-hour postprandial glucose level of 105 mg/dL (Choice A) is within the normal range. During pregnancy, glucose levels are carefully monitored to check for gestational diabetes. In this case, the result falls within the acceptable range, indicating that the client's glucose levels are stable, and gestational diabetes is not a concern at this time.
Choice B reason:
A negative group B streptococcus (GBS) B-hemolytic result (Choice B) is actually a positive finding. It means that the client does not have an active infection with group B streptococcus, which is essential information for the management of labor and delivery. Therefore, there is no need to report this result to the provider as it indicates a favorable condition.
Choice C reason:
The hemoglobin (Hgb) level of 13 g/dL (Choice C) is within the normal range for a non- pregnant adult female. During pregnancy, blood volume increases, and hemoglobin levels can naturally decrease. However, the provided value is still within the acceptable range, indicating that the client's blood oxygen-carrying capacity is adequate and there is no immediate concern.
A nurse is contributing to the plan of care for a newborn who has hyperbilirubinemia and requires phototherapy. Which of the following interventions should the nurse include?
Explanation
Swaddle the newborn during the treatment. Choice A reason:
Apply lotion to the newborn's skin twice per day. Rationale: The nurse should not apply lotion to the newborn's skin during phototherapy. Phototherapy involves exposing the baby's skin to light to treat hyperbilirubinemia. Applying lotion may interfere with the effectiveness of the treatment or cause adverse reactions.
Choice B reason:
Check the newborn's blood glucose every 2 hours. Rationale: While monitoring the newborn's blood glucose is an essential part of neonatal care, it is not directly related to phototherapy or the treatment of hyperbilirubinemia. Glucose monitoring is typically done to assess for hypoglycemia or other metabolic disturbances.
Choice C reason:
Swaddle the newborn during the treatment. Rationale: Swaddling the newborn during phototherapy can help keep the baby calm and prevent unnecessary movement. Reducing
movement is important as it allows the phototherapy lights to be positioned effectively and consistently over the baby's skin, maximizing the treatment's benefits.
Choice D reason:
Remove the newborn's eye mask during feedings. Rationale: The newborn's eye mask should not be removed during feedings. The eye mask is specifically designed to protect the baby's eyes from the phototherapy lights, which can be harmful to the eyes. The mask should remain in place throughout the treatment, even during feedings.
A nurse is contributing to the plan of care for a client 48 hr following cesarean birth. Which of the following nonpharmacologic interventions should the nurse include to reduce pain from intestinal gas?
Explanation
Choice A reason:
The nurse should provide the client with a carbonated beverage as a nonpharmacologic intervention to reduce pain from intestinal gas. Carbonated beverages, like soda or sparkling water, can help alleviate gas by promoting burping, which releases trapped gas from the digestive system. The effervescence of the carbonated drink can help relieve the discomfort caused by accumulated gas, offering relief to the client.
Choice B reason:
Encouraging the client to lie on their right side is not an effective nonpharmacologic intervention for reducing pain from intestinal gas. Although positioning can sometimes aid in relieving discomfort, lying on the right side does not specifically target the reduction of gas. Therefore, it is not the most appropriate choice in this scenario.
Choice C reason:
Encouraging the client to ambulate is a beneficial nonpharmacologic intervention for various post-operative conditions. However, when it comes to reducing pain from intestinal gas, it may not be as effective as other options. While movement can aid in gas passage through the digestive system, it might not be the most immediate or direct solution for alleviating the client's discomfort.
Choice D reason:
Providing the client with straws for beverages does not directly address the issue of intestinal gas. It is an unrelated intervention and may not provide any significant relief for the client's discomfort.
A nurse on a pediatric unit is assisting with the admission of a toddler who has pneumonia. The nurse should identify that which of the following findings is an expected behavior of hospitalization?
Explanation
Choice A reason:
Experiences separation anxiety - This is a common behavior seen in toddlers during hospitalization. Being away from their parents or caregivers and being in an unfamiliar environment can lead to feelings of anxiety and distress. Separation anxiety is a natural response for young children who rely on their primary caregivers for comfort and security.
Choice B reason:
Fears a loss of control - Toddlers may feel overwhelmed and fearful when they find themselves in a hospital setting. The loss of control over their daily routines and environment can be frightening for them. They may be unable to understand the reasons behind medical procedures or interventions, further increasing their anxiety.
Choice C reason:
Feels hospitalization is punishment - While some children might have difficulty understanding the reasons for hospitalization, it is less common for them to perceive it as punishment.
Children at this age often lack the cognitive capacity to associate their illness with punishment.
Choice D reason:
Develops body image disturbance - Body image disturbance is not a typical behavior observed in toddlers during hospitalization. This issue is more common in older children or adolescents who may experience changes in their appearance due to medical conditions or treatments.
A nurse is reinforcing teaching with an adolescent who has type 1 diabetes mellitus. Which of the following statements by the adolescent indicates an understanding of the teaching?
Explanation
Choice A reason:
The statement "I will discard insulin bottles 60 days after opening”. is incorrect. Insulin bottles typically have a shorter shelf life after opening, usually around 28 days. Discarding them after 60 days could lead to using ineffective insulin, which can be harmful to the individual's blood sugar control.
Choice B reason:
This statement is correct and indicates an understanding of diabetes management. Exercise can lower blood sugar levels, and taking an extra 10 units of insulin before exercising helps prevent hypoglycemia (low blood sugar) during physical activity.
Choice C reason:
The statement "If I feel dizzy, I will drink 4 ounces of orange juice”. is incorrect. While orange juice contains sugar and can raise blood sugar levels, it is not the best choice for treating dizziness. In case of dizziness, the individual should check their blood sugar levels first and treat it accordingly, following their healthcare provider's instructions.
Choice D reason:
The statement "A hemoglobin A1c of 9 percent is a good goal”. is incorrect. Hemoglobin A1c reflects average blood sugar levels over the past 2-3 months. An A1c of 9 percent is relatively high and suggests poor diabetes management. The target A1c goal for most people with diabetes is typically below 7 percent, as recommended by the American Diabetes Association.
A nurse is reinforcing teaching with a client who is postpartum and plans to breastfeed their newborn. Which of the following statements by the client indicates an understanding of the teaching?
Explanation
Choice A reason:
The client stating, "I should add 500 calories per day to my diet,” is not an accurate understanding of breastfeeding. While it is true that breastfeeding mothers require additional calories to support lactation, the specific amount of calories needed varies depending on individual factors and should be discussed with a healthcare professional. Simply adding 500 calories per day may not be appropriate for every woman and could lead to excessive weight gain.
Choice B reason:
This choice indicates an understanding of proper breast hygiene during breastfeeding. Using antibacterial soap and warm water to wash the breasts helps to prevent infection and maintain good breast health, reducing the risk of complications for both the mother and the baby.
Choice C reason:
The statement, "Breastfeeding is a reliable method of birth control,” is incorrect. While breastfeeding can provide some natural contraceptive effects, it is not a foolproof method of birth control. This concept is known as the lactational amenorrhea method (LAM), and specific criteria must be met for it to be considered a reliable form of contraception. Relying solely on breastfeeding as birth control can lead to an unintended pregnancy.
Choice D reason:
The statement, "If my nipples become cracked and red, I will apply hydrocortisone cream,” is not advisable. While hydrocortisone cream may provide temporary relief from irritation, it is not recommended for breastfeeding mothers. Ingestion of the cream by the baby can be harmful. Instead, the client should seek guidance from a healthcare professional to address and resolve any breastfeeding-related nipple issues.
A nurse in an antepartum clinic is reinforcing teaching with a pregnant client about breastfeeding. Which of the following statements by the client indicates an understanding of the teaching?
Explanation
"I should start trying to breastfeed within an hour of having my baby.” Choice A reason:
The client's statement indicates an understanding of the teaching because initiating breastfeeding within the first hour after birth is crucial for successful breastfeeding. This early initiation allows the baby to receive colostrum, which is rich in nutrients and antibodies, supporting the baby's immune system and providing essential nutrition during the initial stages of life. Additionally, early breastfeeding helps establish a strong bond between the mother and the baby while promoting the baby's suckling reflex.
Choice B reason:
The statement in Choice B is incorrect. Formula feeding between breastfeedings is not recommended in the early stages of breastfeeding, especially if the baby loses 5 percent of their birth weight. Newborns often lose some weight initially, which is normal, and it can be regained through effective breastfeeding. Supplementing with formula may interfere with establishing a good milk supply and the baby's ability to latch properly.
Choice C reason:
This statement in Choice C is incorrect. During breastfeeding sessions, it's essential for the baby to nurse on one breast fully before switching to the other breast. Allowing the baby to nurse for at least 10-15 minutes on each breast ensures they receive the hindmilk, which is higher in fat and essential for the baby's growth and development.
Choice D reason:
The statement in Choice D is incorrect. Offering a pacifier right after breastfeeding might interfere with the baby's feeding cues and lead to decreased breastfeeding frequency.
Newborns may suck for non-nutritive reasons, and offering a pacifier too soon can hinder proper breastfeeding establishment, as they may satisfy their sucking needs with the pacifier rather than nursing at the breast.
A nurse is evaluating the parenting styles of a group of parents of school-age children. Which of the following statements by a parent indicates the use of a permissive parenting style?
Explanation
"We allow our children the freedom to decide their own behavior.”
Choice A reason:
This statement does not indicate a permissive parenting style. In fact, it suggests an authoritative or authoritarian style, where the parents make decisions for their children without considering their input. The parents' imposition of their decisions on their children's time indicates a more controlling approach.
Choice B reason:
This statement also does not reflect a permissive parenting style. Instead, it represents an authoritative or authoritarian style, where the parents expect obedience and compliance without allowing room for questions or autonomy. This approach tends to be more structured and directive.
Choice C reason:
This statement demonstrates the use of a permissive parenting style. In permissive parenting, parents tend to be lenient and allow their children considerable freedom in decision-making and behavior. By giving their children the freedom to decide their own behavior, the parents are adopting a permissive approach, which can sometimes lead to indulgence and lack of necessary boundaries.
Choice D reason:
This statement does not indicate a permissive parenting style either. Instead, it suggests an authoritative or democratic style, where the parents explain the reasoning behind the rules they set. This approach encourages understanding and cooperation but is different from permissiveness.
A nurse is discussing growth and development milestones with the parents of a 3-year-old preschooler. Which of the following statements by a parent indicates to the nurse that the preschooler is meeting the expected benchmarks of other preschoolers in this age group?
Explanation
Choice A reason:
If the parent states, "My child uses scissors to cut out the outline of an object,” this indicates fine motor skills development. While this is a positive milestone, it is not specific to the expected benchmarks of other preschoolers in this age group. The ability to cut out shapes with scissors varies widely among preschoolers.
Choice B reason:
"My child can copy triangle shapes onto paper.” This statement shows that the child can demonstrate some level of visual-motor coordination and fine motor skills. Copying shapes like triangles is a common milestone for many preschoolers at the age of 3 and is considered an expected benchmark.
Choice C reason:
If the parent says, "My child can ride a tricycle,” this indicates gross motor skills development. Riding a tricycle is also a milestone achieved by many preschoolers, but it may not be as specific to the expected benchmarks of this age group as choice B, which focuses on fine motor skills and visual-motor coordination.
Choice D reason:
If the parent mentions, "My child can throw a ball overhead,” this also points to gross motor skills development. While throwing a ball overhead is an impressive skill for a 3-year-old, it may not be as common or consistent among all preschoolers in this age group as the ability to copy triangle shapes onto paper (choice B).
A nurse is reinforcing teaching with an adolescent about subdermal progesterone contraception devices. Which of the following statements by the client indicates an understanding of the teaching?
Explanation
"I should call my provider if I notice thick white discharge in my underwear.”
Choice A reason:
The client stating, "I will need to have this device replaced every 3 years,” is incorrect. Subdermal progesterone contraception devices, such as Nexplanon, can typically last for up to 3 years, not needing replacement within that time frame. The rationale behind this is that these devices release a steady amount of progesterone to prevent pregnancy, and they are designed to be effective for the specified duration.
Choice B reason:
The statement, "This device will protect me from STIs,” in Choice B is incorrect. Subdermal progesterone contraception devices do not provide protection against sexually transmitted infections (STIs). Their primary function is to prevent pregnancy by inhibiting ovulation, thickening cervical mucus, and altering the uterine lining, but they do not offer any defense against STIs. It is essential for the client to understand that barrier methods, such as condoms, are necessary for STI protection.
Choice C reason:
The correct answer, "I should call my provider if I notice thick white discharge in my underwear,” is an accurate statement. Thick white discharge could be indicative of a vaginal infection, such as yeast infection, which might require medical attention. It is crucial for the client to report any changes in vaginal discharge to their healthcare provider for proper evaluation and treatment.
Choice D reason:
The statement in Choice D, "I need to decrease the amount of milk I drink while I have this device,” is incorrect. There is no association between subdermal progesterone contraception devices and milk consumption. The device does not interfere with dairy intake or affect its metabolism. This information is unrelated to the proper use or management of the contraception device.
Sign Up or Login to view all the 49 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
