ATI Pediatric Exam 3 Updated 2024
Total Questions : 87
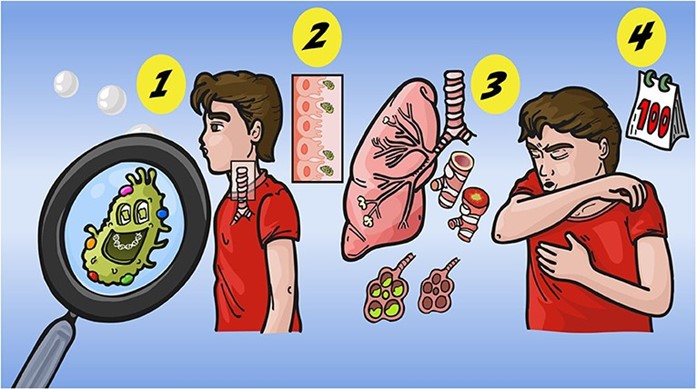
Showing 25 questions, Sign in for moreA nurse is caring for a child who has pertussis. The child's parent asks the nurse what the common name for this disease is. The nurse should respond with which of the following common names?
Explanation
Choice A reason: This choice is incorrect because mumps is not the common name for pertussis. Mumps is a viral infection that causes inflammation of the salivary glands, especially the parotid glands. It may cause symptoms such as fever, headache, and swelling of the cheeks or jaw. It can be prevented by vaccination with the measles-mumps-rubella (MMR) vaccine.
Choice B reason: This choice is correct because whooping cough is the common name for pertussis. Pertussis is a bacterial infection that causes severe coughing spells, which may be followed by a high-pitched whoop sound or vomiting. It may cause complications such as pneumonia, seizures, or brain damage, especially in infants and young children. It can be prevented by vaccination with the diphtheria-tetanus-pertussis (DTaP) vaccine.
Choice C reason: This choice is incorrect because the fifth disease is not the common name for pertussis. The fifth disease is a viral infection that causes a rash on the face, trunk, and limbs, which may resemble a slapped cheek appearance. It may cause mild symptoms such as fever, runny nose, or joint pain. It usually affects children and is self-limiting.
Choice D reason: This choice is incorrect because chickenpox is not the common name for pertussis. Chickenpox is a viral infection that causes an itchy rash with fluid-filled blisters all over the body. It may cause symptoms such as fever, headache, or loss of appetite. It can be prevented by vaccination with the varicella-zoster (VZV) vaccine.
Nursing care of a child who is immunosuppressed due to leukemia or chemotherapeutic agents should include:
(choose one best answer)
Explanation
Choice A reason: This choice is incorrect because having them share a room with a child with active mumps may expose them to infection and worsen their condition. A child who is immunosuppressed due to leukemia or chemotherapeutic agents has a weakened immune system and is more susceptible to infections from bacteria, viruses, fungi, or parasites. Therefore, they should be placed in a private room or cohorted with another immunosuppressed child.
Choice B reason: This choice is incorrect because restricting oral fluids may cause dehydration and electrolyte imbalance in the child who is immunosuppressed due to leukemia or chemotherapeutic agents. A child who is immunosuppressed due to leukemia or chemotherapeutic agents may have increased fluid losses from vomiting, diarrhea, fever, or sweating. Therefore, they should be encouraged to drink adequate fluids to maintain hydration and electrolyte balance.
Choice C reason: This choice is incorrect because strict isolation may cause psychological distress and social isolation in the child who is immunosuppressed due to leukemia or chemotherapeutic agents. A child who is immunosuppressed due to leukemia or chemotherapeutic agents may benefit from protective isolation, which involves using standard precautions and additional measures such as wearing gloves, gowns, masks, or eye protection when in contact with the child or their body fluids. However, strict isolation, which involves limiting visitors and activities, may harm the child's emotional and developmental well-being.
Choice D reason: This choice is correct because using good handwashing is essential nursing care for a child who is immunosuppressed due to leukemia or chemotherapeutic agents. Handwashing is the most effective way to prevent the transmission of microorganisms that can cause infections. The nurse should wash their hands before and after touching the child or their belongings, and teach the child and their family members to do the same. The nurse should also use alcohol-based hand rubs when water and soap are not available.
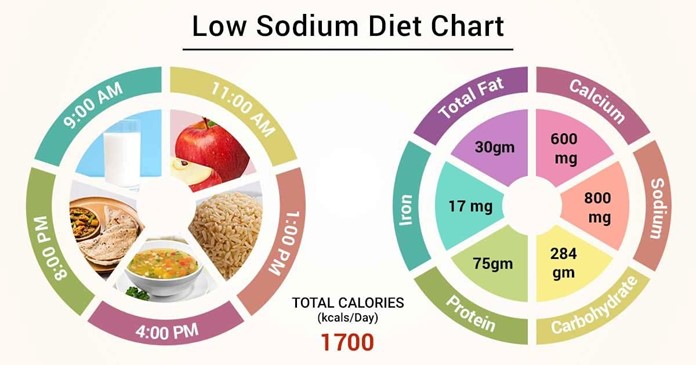
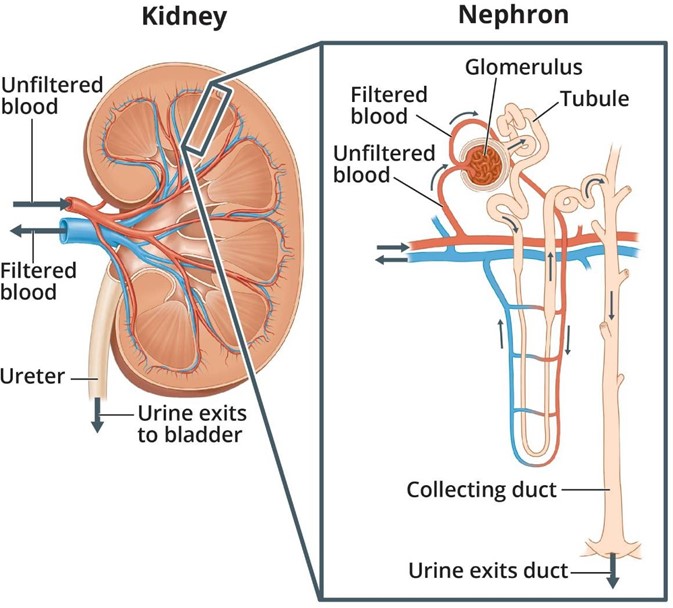
A nurse is caring for a school-age child who has acute glomerulonephritis with peripheral edema and is producing 35mL of urine per hour. The nurse should place the client on which of the following diets?
Explanation
Choice A reason: This choice is incorrect because a regular diet, no added salt may not be sufficient to prevent fluid retention and hypertension in a child who has acute glomerulonephritis. Acute glomerulonephritis is an inflammation of the glomeruli, which are the tiny blood vessels that filter blood in the kidneys. It may cause symptoms such as hematuria, proteinuria, oliguria, edema, or hypertension. Therefore, avoiding salt alone may not reduce sodium and water intake and excretion.
Choice B reason: This choice is incorrect because a low-protein, low-potassium diet may not be necessary for a child who has acute glomerulonephritis. A low-protein, low-potassium diet may be indicated for a child who has chronic kidney disease or end-stage renal disease, which can cause uremia, hyperkalemia, or metabolic acidosis. However, in acute glomerulonephritis, the kidney function usually recovers within weeks or months, and the protein and potassium levels are not significantly affected.
Choice C reason: This choice is incorrect because a low-carbohydrate, low-protein diet may not be appropriate for a child who has acute glomerulonephritis. A low-carbohydrate, low-protein diet may be used for a child who has diabetes mellitus or ketosis-prone epilepsy, which can cause hyperglycemia or ketone production. However, in acute glomerulonephritis, carbohydrate metabolism is not impaired, and the protein intake should be adequate to prevent malnutrition and promote healing.
Choice D reason: This choice is correct because a low-sodium, fluid-restricted diet is an appropriate diet for a child who has acute glomerulonephritis. A low-sodium, fluid-restricted diet helps to reduce the fluid retention and hypertension by limiting the sodium and water intake and excretion. The sodium intake should be less than 2 g per day, and the fluid intake should be equal to the urine output plus 500 mL per day.
A nurse is caring for a child who has otitis media. Which of the following assessment findings should the nurse expect?
Explanation
Choice A reason: This choice is incorrect because tugging on the affected ear lobe is not a specific sign of otitis media. Tugging on the ear lobe may indicate ear discomfort or irritation, but it may also be a normal behavior or habit in children. It does not necessarily indicate an infection or inflammation of the middle ear.
Choice B reason: This choice is incorrect because erythema and edema of the affected ear are not signs of otitis media. Erythema and edema of the ear may indicate otitis externa, which is an infection or inflammation of the external ear canal. It may cause symptoms such as itching, discharge, or hearing loss. However, in otitis media, the infection or inflammation affects the middle ear behind the eardrum, which is not visible from the outside.
Choice C reason: This choice is correct because pain when manipulating the affected ear lobe is a sign of otitis media. Pain when manipulating the ear lobe indicates that there is pressure or fluid buildup in the middle ear due to infection or inflammation. The pain may worsen when lying down or chewing. It may also cause symptoms such as fever, irritability, or reduced hearing.
Choice D reason: This choice is incorrect because clear drainage from the affected ear is not a sign of otitis media. Clear drainage from the ear may indicate cerumen impaction, which is a buildup of earwax in the ear canal. It may cause symptoms such as itching, fullness, or hearing loss. However, in otitis media, the drainage from the ear may be yellowish-green or bloody due to rupture of the eardrum from infection or inflammation.
A nurse is performing a pre-college physical assessment on an adolescent. Which of the following immunizations should the nurse anticipate administering?
Explanation
Choice A reason: This choice is incorrect because the BCG vaccine is not recommended for adolescents in the United States. The BCG vaccine is a vaccine that protects against tuberculosis (TB), a bacterial infection that affects the lungs and other organs. It may be used for children who live in countries where TB is common or who have a high risk of exposure to TB, but it is not routinely given in the United States because of the low incidence of TB and the possibility of false-positive results on TB skin tests.
Choice B reason: This choice is incorrect because the pneumococcal polysaccharide vaccine is not recommended for adolescents unless they have certain medical conditions. The pneumococcal polysaccharide vaccine is a vaccine that protects against pneumococcal disease, a bacterial infection that can cause pneumonia, meningitis, or sepsis. It may be used for adults who are 65 years or older or who have chronic diseases, immunosuppression, or cochlear implants, but it is not routinely given to adolescents who are healthy.
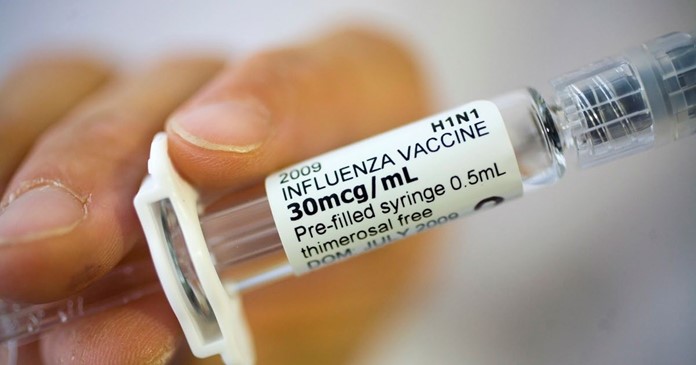
Choice C reason: This choice is incorrect because the influenza vaccine is recommended for adolescents every year, not just before college. The influenza vaccine is a vaccine that protects against influenza, a viral infection that affects the respiratory system. It may be given as an injection or a nasal spray, and it may prevent or reduce the severity of influenza and its complications. It is recommended for everyone who is 6 months or older, especially those who have a high risk of influenza-related complications.
Choice D reason: This choice is correct because the meningococcal polysaccharide vaccine is recommended for adolescents before college. The meningococcal polysaccharide vaccine is a vaccine that protects against meningococcal disease, a bacterial infection that can cause meningitis, septicemia, or death. It may be given as a single dose or a booster dose, and it may prevent outbreaks of meningococcal disease in crowded settings such as dormitories or military barracks. It is recommended for adolescents who are 11 to 12 years old, with a booster dose at 16 years old, or for those who are entering college and have not been previously vaccinated.
A nurse is providing nutritional teaching to the mother of a preschooler and is recommending food options to provide 1 oz of grains. Which of the following foods should the nurse recommend?
Explanation
Choice A reason: This choice is incorrect because 1 cup of cooked rice provides more than 1 oz of grains. According to the U.S. Department of Agriculture (USDA), one-ounce equivalent of grains equals one slice of bread, one cup of ready-to-eat cereal, or half a cup of cooked rice, pasta, or cereal. Therefore, 1 cup of cooked rice provides about 2 oz of grains.
Choice B reason: This choice is incorrect because 1/2 slice of white bread provides less than 1 oz of grains. As explained above, one-ounce equivalent of grains equals one slice of bread, so 1/2 slice of white bread provides only 0.5 oz of grains.
Choice C reason: This choice is correct because 1 cup of ready-to-eat cereal flakes provides exactly 1 oz of grains. As explained above, the one-ounce equivalent of grains equals one cup of ready-to-eat cereal, so 1 cup of ready-to-eat cereal flakes provides 1 oz of grains.
Choice D reason: This choice is incorrect because 1/2 white flour tortilla provides less than 1 oz of grains. According to the USDA, one-ounce equivalent of grains equals one small tortilla (6 inches in diameter), so 1/2 white flour tortilla provides only about 0.4 oz of grains.
A nurse is planning care for an infant who has spina bifida and is to undergo surgical closure of the myelomeningocele sac. Which of the following interventions should the nurse include in the plan of care?
Explanation
Choice A reason: This choice is correct because providing a latex-free environment is an essential intervention for an infant who has spina bifida and is to undergo surgical closure of the myelomeningocele sac. Spina bifida is a congenital defect in which the spinal cord and its coverings do not close properly, resulting in a protrusion of the meninges (meningocele) or the meninges and spinal cord (myelomeningocele). Children who have spina bifida are at a high risk of developing a latex allergy, which can cause severe reactions such as anaphylaxis or death. Therefore, avoiding exposure to latex products such as gloves, catheters, balloons, or bandages is crucial to prevent complications.
Choice B reason: This choice is incorrect because initiating contact precautions is not necessary for an infant who has spina bifida and is to undergo surgical closure of the myelomeningocele sac. Contact precautions are infection control measures that prevent the transmission of microorganisms that can be spread by direct or indirect contact with the client or their environment. They may be indicated for clients who have multidrug-resistant organisms, clostridium difficile, or scabies, but they are not required for clients who have spina bifida unless they have a concurrent infection.
Choice C reason: This choice is incorrect because limiting visitors to immediate family members is not indicated for an infant who has spina bifida and is to undergo surgical closure of the myelomeningocele sac. Limiting visitors may be indicated for clients who have immunosuppression, isolation, or terminal illness, but it may not be beneficial for clients who have spina bifida. Allowing visitors may provide emotional and social support for the client and their family, as long as they follow standard precautions and do not pose any risk of infection or injury.
Choice D reason: This choice is incorrect because maintaining the infant in the supine position is not an appropriate intervention for an infant who has spina bifida and is to undergo surgical closure of the myelomeningocele sac.
Maintaining the infant in the supine position may cause pressure or trauma to the sac, which can lead to rupture, infection, or nerve damage. Therefore, positioning the infant in a prone or side-lying position with the hips flexed and knees abducted can help to protect the sac and prevent complications.
A nurse is providing teaching to an adolescent who has type 1 diabetes mellitus. Which of the following should the nurse include in the teaching?
Explanation
Choice A reason: This choice is incorrect because taking glyburide with breakfast is not recommended for an adolescent who has type 1 diabetes mellitus. Glyburide is an oral hypoglycemic medication that lowers blood glucose levels by stimulating insulin secretion from the pancreas. It may be used for clients who have type 2 diabetes mellitus, but it does not work for clients who have type 1 diabetes mellitus or DKA.
Choice B reason: This choice is correct because obtaining an influenza vaccine annually is recommended for an adolescent who has type 1 diabetes mellitus. The influenza vaccine is a vaccine that protects against influenza, a viral infection that affects the respiratory system. It may prevent or reduce the severity of influenza and its complications, such as pneumonia or sepsis. It is recommended for everyone who is 6 months or older, especially those who have chronic conditions such as diabetes mellitus that increase their risk of influenza-related complications.
Choice C reason: This choice is incorrect because administering glucagon for hyperglycemia is not indicated for an adolescent who has type 1 diabetes mellitus. Glucagon is a hormone that raises blood glucose levels by stimulating glycogen breakdown in the liver. It may be used for clients who have hypoglycemia, which is a condition in which blood glucose levels are lower than normal (less than 70 mg/dL). It may cause symptoms such as sweating, trembling, confusion, or loss of consciousness. However, in type 1 diabetes mellitus, hyperglycemia (high blood glucose levels) rather than hypoglycemia is more likely to occur due to insulin deficiency or resistance.
Choice D reason: This choice is incorrect because injecting insulin in the deltoid muscle is not an optimal method for an adolescent who has type 1 diabetes mellitus. Insulin is a hormone that lowers blood glucose levels by facilitating glucose uptake into the cells. It may be administered by injection or infusion, and it may vary in onset, peak, and duration of action. The preferred sites for insulin injection are the abdomen, the thighs, the buttocks, or the upper arms, as they have more subcutaneous fat and less muscle tissue. Injecting insulin into the deltoid muscle may cause faster absorption and shorter duration of action, which can affect blood glucose control and increase the risk of hypoglycemia.
A nurse is assessing a child who is in a sickle cell crisis. Which of the following findings should the nurse expect?
Explanation
Choice A reason: This choice is incorrect because bradycardia is not a common finding in a child who is in a sickle cell crisis. Bradycardia is a condition in which the heart rate is slower than normal (less than 60 beats per minute). It may be caused by various factors such as hypothermia, hypothyroidism, or medication side effects, but it does not indicate a sickle cell crisis.
Choice B reason: This choice is incorrect because constipation is not a common finding in a child who is in a sickle cell crisis. Constipation is a condition in which the bowel movements are infrequent, hard, or difficult to pass. It may be caused by various factors such as dehydration, a low-fiber diet, or lack of physical activity, but it does not indicate a sickle cell crisis.
Choice C reason: This choice is correct because pain is a common finding in a child who is in a sickle cell crisis. Sickle cell crisis is a condition in which the red blood cells become sickle-shaped and clump together, blocking the blood flow and oxygen delivery to the organs and tissues. It may cause severe pain in the chest, abdomen, joints, or bones, as well as symptoms such as pallor, jaundice, fatigue, or shortness of breath.
Choice D reason: This choice is incorrect because high fever is not a specific finding in a child who is in a sickle cell crisis. High fever may indicate infection, inflammation, or dehydration, but it does not indicate sickle cell crisis. However, the infection can trigger or worsen the sickle cell crisis, so it should be treated promptly with antibiotics and fluids.
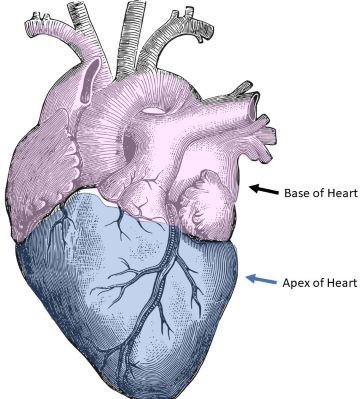
A nurse is preparing to measure an infant's vital signs. The nurse should use which of the following sites to assess a heart rate?
Explanation
Choice A reason: This choice is incorrect because the radial artery is not an ideal site to assess the heart rate in an infant. The radial artery is located on the thumb side of the wrist, and it can be palpated by placing two fingers over it. It may be used for adults or older children who have a strong pulse, but it may be difficult to locate or feel in an infant who has a small or weak pulse.
Choice B reason: This choice is incorrect because the carotid artery is not an ideal site to assess the heart rate in an infant. The carotid artery is located on either side of the neck, and it can be palpated by placing two fingers over it. It may be used for adults or older children who have a cardiac arrest or shock, but it may be risky to use in an infant who has a fragile neck or airway.
Choice C reason: This choice is incorrect because the brachial artery is not an ideal site to assess the heart rate in an infant. The brachial artery is located on the inner side of the upper arm, and it can be palpated by placing two fingers over it. It may be used for infants or young children who have a blood pressure measurement, but it may be uncomfortable or inaccurate to use for a heart rate assessment.
Choice D reason: This choice is correct because the apex of the heart is an ideal site to assess the heart rate in an infant. The apex of the heart is located at the fifth intercostal space on the left midclavicular line, and it can be auscultated by placing a stethoscope over it. It may be used for infants or young children who have a regular and strong heartbeat, and it may provide the most accurate measurement of the heart rate.
A nurse is assessing a toddler at a well-child visit. At what point in the physical examination should the nurse examine the child's tympanic membrane? (The child will likely view this as invasive and traumatic)
Explanation
Choice A reason: This choice is correct because examining the child's tympanic membrane at the end of the physical examination is the best strategy to avoid upsetting or frightening the child. The tympanic membrane is the thin membrane that separates the outer ear from the middle ear, and it can be examined by using an otoscope, which is a device that has a light and a magnifying lens. Examining the tympanic membrane may be uncomfortable or painful for the child, especially if they have an ear infection or inflammation. Therefore, performing this procedure at the end of the examination can help to minimize the child's distress and resistance.
Choice B reason: This choice is incorrect because examining the child's tympanic membrane before auscultating the chest and abdomen is not a good strategy to avoid upsetting or frightening the child. Auscultating the chest and abdomen is a procedure that involves listening to the sounds of the heart, lungs, and bowel by using a stethoscope, which is a device that has a chest piece and earpieces. Auscultating the chest and abdomen may be soothing or relaxing for the child, as it does not cause any discomfort or pain. Therefore, performing this procedure before examining the tympanic membrane can help to calm and distract the child.
Choice C reason: This choice is incorrect because examining the child's tympanic membrane at the beginning of the physical examination is not a good strategy to avoid upsetting or frightening the child. Examining the tympanic membrane at the beginning of the examination may cause anxiety or fear in the child, which can affect their cooperation and trust for the rest of the examination. Therefore, performing this procedure at the beginning of the examination can increase the child's distress and resistance.
Choice D reason: This choice is incorrect because examining the child's tympanic membrane before examining the
head and neck is not a good strategy to avoid upsetting or frightening the child. Examining the head and neck is a procedure that involves inspecting and palpating the scalp, hair, face, eyes, ears, nose, mouth, throat, lymph nodes, and thyroid gland. Examining the head and neck may be easy or pleasant for the child, as it does not cause any discomfort or pain. Therefore, performing this procedure before examining the tympanic membrane can help to establish rapport and confidence with the child.
A nurse is caring for a 10-month-old infant who is in a cast for developmental dysplasia of the hip (DDH). Which of the following strategies should the nurse implement to promote the infant's growth and development?
Explanation
Choice A reason: This choice is incorrect because tying colorful latex balloons to the side of
the crib may pose a risk of choking or suffocation for the infant who is in a cast for DDH. Latex balloons are made of rubber that can break easily and form small pieces that can block the airway or lungs if swallowed or inhaled by
the infant. Therefore, avoiding latex products such as balloons, gloves, or bandages is important to prevent accidents or injuries.
Choice B reason: This choice is incorrect because following the doctor's instructions regarding activities and treatment plans is not a specific strategy to promote the infant's growth and development. Following
the doctor's instructions regarding activities and treatment plans is a general responsibility of the nurse that applies to any client who has any condition or procedure. It may help to ensure the safety and effectiveness of the care, but it does not address the developmental needs of the infant who is in a cast for DDH.
Choice C reason: This choice is correct because providing a small electronic toy is a specific strategy to promote
the infant's growth and development. Providing a small electronic toy can help stimulate the infant's senses, cognition, and motor skills by offering visual, auditory, or tactile feedback. It may also help to reduce boredom, frustration, or depression by providing entertainment, diversion, or comfort. Therefore, providing a small electronic toy can help to enhance the developmental outcomes of the infant who is in a cast for DDH.
Choice D reason: This choice is incorrect because changing the infant's diaper as soon as soiling occurs is not a specific strategy to promote the infant's growth and development. Changing the infant's diaper as soon as soiling occurs is a general hygiene measure that applies to any infant who wears a diaper. It may help to prevent skin irritation, infection, or odor by keeping the diaper area clean and dry, but it does not address the developmental needs of the infant who is in a cast for DDH.
A nurse in an emergency department is caring for an adolescent following a suicide attempt. After reviewing the client's history, the nurse should determine that which of the following is the priority risk factor for suicide completion.
Explanation
Choice A reason: This choice is incorrect because the loss of a parent is not the priority risk factor for suicide completion. Loss of a parent is a stressful life event that may cause grief, depression, or anxiety in an adolescent, but it does not necessarily increase the risk of suicide completion. However, the loss of a parent may be associated with other risk factors such as low self-esteem, poor coping skills, or social isolation, which can contribute to suicidal ideation or behavior.
Choice B reason: This choice is incorrect because a history of substance abuse is not the priority risk factor for suicide completion. History of substance abuse is a behavioral problem that may impair the judgment, mood, or impulse control of an adolescent, but it does not necessarily increase the risk of suicide completion. However, a history of substance abuse may be associated with other risk factors such as mental illness, family conflict, or legal trouble, which can contribute to suicidal ideation or behavior.
Choice C reason: This choice is correct because a previous suicide attempt is the priority risk factor for suicide completion. Previous suicide attempt is a clear indicator of suicidal intent and capability, and it increases the likelihood of future attempts and completion. According to the American Foundation for Suicide Prevention (AFSP), about 40% of people who die by suicide have a history of previous attempts. Therefore, assessing and addressing previous suicide attempts is essential to prevent further harm and save lives.
Choice D reason: This choice is incorrect because active psychiatric disorder is not the priority risk factor for suicide completion. Active psychiatric disorder is a mental health condition that may affect the thoughts, feelings, or behaviors of an adolescent, but it does not necessarily increase the risk of suicide completion. However, active psychiatric disorder may be associated with other risk factors such as hopelessness, helplessness, or isolation, which can contribute to suicidal ideation or behavior.
A nurse is providing teaching about iron deficiency anemia to the parents of an infant. Which of the following should the nurse recommend as a method of preventing iron deficiency anemia?
Explanation
Choice A reason: This choice is incorrect because limiting intake of high-protein foods is not a method of preventing iron deficiency anemia. High-protein foods are foods that contain a large amount of protein, such as meat, poultry, fish, eggs, dairy products, beans, nuts, or seeds. Protein is a nutrient that helps to build and repair body tissues and support immune function. It may also provide iron, which is a mineral that helps to produce hemoglobin, the protein that carries oxygen in red blood cells. Therefore, limiting intake of high-protein foods may reduce iron intake and increase the risk of iron deficiency anemia.
Choice B reason: This choice is correct because mom should continue prenatal vitamins if breastfeeding or formula with an iron supplement is a method of preventing iron deficiency anemia. Prenatal vitamins are supplements that contain various vitamins and minerals that are essential for pregnant or lactating women and their babies. They may include iron, which helps to prevent maternal and infant anemia. Formula with an iron supplement is a type of infant formula that contains added iron to meet the nutritional needs of infants who are not breastfed or partially breastfed. Therefore, mom should continue prenatal vitamins if breastfeeding or formula with an iron supplement can help to provide adequate iron intake and prevent iron deficiency anemia.
Choice C reason: This choice is incorrect because administering fat-soluble vitamins daily is not a method of preventing iron deficiency anemia. Fat-soluble vitamins are vitamins that dissolve in fat and can be stored in the body, such as vitamins A, D, E, and K. They have various functions such as maintaining vision, bone health, skin health, and blood clotting. They do not have a direct role in preventing iron deficiency anemia.
Choice D reason: This choice is incorrect because including fluoridated water in the toddler's diet is not a method of preventing iron deficiency anemia. Fluoridated water is water that contains fluoride, which is a substance that helps to prevent tooth decay and cavities. It does not have a direct role in preventing iron deficiency anemia.
A nurse is admitting a child who has leukemia. Which of the following clients should the nurse place in the same room with this child?
Explanation
Choice A reason: This choice is correct because a child who has nephrotic syndrome is the most appropriate roommate for a child who has leukemia. Nephrotic syndrome is a kidney disorder that causes proteinuria, edema, hypoalbuminemia, and hyperlipidemia. It does not pose any risk of infection or injury to the child who has leukemia, and it does not require any isolation or special precautions. Therefore, placing these two children in the same room can help to conserve resources and promote socialization.
Choice B reason: This choice is incorrect because a child recovering from a ruptured appendix is not an appropriate roommate for a child who has leukemia. A ruptured appendix is a medical emergency that occurs when the appendix becomes inflamed and bursts, releasing bacteria and pus into the abdominal cavity. It may cause peritonitis, sepsis, or abscess formation, and it requires surgery and antibiotics. It may pose a risk of infection to a child who has leukemia, who has a weakened immune system due to chemotherapy or bone marrow suppression. Therefore, placing these two children in the same room can increase the chance of cross-contamination and complications.
Choice C reason: This choice is incorrect because a child who has rheumatic fever is not an appropriate roommate for a child who has leukemia. Rheumatic fever is an inflammatory disease that occurs as a complication of streptococcal infection, such as strep throat or scarlet fever. It may affect the heart, joints, skin, or nervous system, and it requires anti-inflammatory and antibiotic medications. It may pose a risk of infection to the child who has leukemia, who has a compromised immune system due to cancer or treatment. Therefore, placing these two children in the same room can increase the likelihood of transmission and infection.
Choice D reason: This choice is incorrect because a child who has cystic fibrosis is not an appropriate roommate for a child who has leukemia. Cystic fibrosis is a genetic disorder that affects the mucus glands of the lungs, pancreas, liver, intestines, and reproductive organs. It causes thick and sticky mucus to build up in the organs, leading to chronic lung infections, pancreatic insufficiency, malnutrition, and infertility. It requires respiratory therapy, enzyme supplements, nutritional support, and antibiotics. It may pose a risk of infection to the child who has leukemia, who has a reduced ability to fight germs due to malignancy or therapy. Therefore, placing these two children in the same room can increase the possibility of exposure and infection.
A nurse is reviewing data for four children. Which of the following children should the nurse assess first?
Explanation
Choice A reason: This choice is incorrect because a 1-year-old toddler who has roseola and a temperature of 39° C (102.2° F) is not the most urgent case to assess. Roseola is a viral infection that causes a rash on the trunk and limbs, followed by a high fever that lasts for several days. It usually affects infants and young children and is self-limiting.
The fever can be managed by giving antipyretics such as acetaminophen or ibuprofen, and by providing fluids and comfort measures. The fever does not indicate any serious complication or threat to life.
Choice B reason: This choice is incorrect because a 4-year-old child who has asthma and an O2 sat of 97% is not the most urgent case to assess. Asthma is a chronic respiratory condition that causes inflammation and narrowing of the airways, leading to wheezing, coughing, chest tightness, or shortness of breath. It may be triggered by allergens, irritants, exercise, or infections. The O2 sat is a measure of oxygen saturation in the blood, which indicates how well oxygen is delivered to the tissues. A normal O2 sat range is 95% to 100%, so an O2 sat of 97% indicates that the child has adequate oxygenation and is not in respiratory distress.
Choice C reason: This choice is correct because a 10-year-old child who has sickle cell anemia and reports severe chest pain is the most urgent case to assess. Sickle cell anemia is a genetic disorder that causes the red blood cells to become sickle-shaped and clump together, blocking the blood flow and oxygen delivery to the organs and tissues. It may cause severe pain in the chest, abdomen, joints, or bones, as well as symptoms such as pallor, jaundice, fatigue, or shortness of breath. Severe chest pain may indicate acute chest syndrome, which is a life-threatening complication of sickle cell anemia that involves infection or infarction of the lungs. It may cause fever, cough, hypoxia, or respiratory failure. Therefore, assessing and treating this child is a priority to prevent further damage and death.
Choice D reason: This choice is incorrect because a 7-year-old child who has diabetes insipidus and a urine specific gravity of 1.016 is not the most urgent case to assess. Diabetes insipidus is a rare disorder that affects the balance of fluids in the body. It causes the kidneys to produce large amounts of dilute urine, leading to polyuria, polydipsia, dehydration, or electrolyte imbalance. It may be caused by a deficiency of antidiuretic hormone (ADH) or a resistance to its action. The urine specific gravity is a measure of urine concentration, which indicates how well the kidneys are functioning. A normal urine specific gravity range is 1.005 to 1.030, so a urine specific gravity of 1.016 indicates that the child has normal urine concentration and is not dehydrated.
A nurse is planning care for a 4-year-old child who requires airborne precautions. Which of the following activities should the nurse plan for the child?
Explanation
Choice A reason: This choice is incorrect because constructing a model airplane is not an appropriate activity for a 4- year-old child who requires airborne precautions. Airborne precautions are infection control measures that prevent the transmission of microorganisms that can be spread by small droplets that remain suspended in the air, such as tuberculosis, measles, or chickenpox. They involve placing the child in a negative-pressure room with a HEPA filter, wearing a respirator mask, and limiting movement outside the room. Constructing a model airplane may involve small parts that can be choking hazards, sharp edges that can cause injury or glue that can cause irritation or allergy. Therefore, this activity may not be safe or suitable for the child.
Choice B reason: This choice is incorrect because pulling a wagon with toys in the hallway is not an appropriate activity for a 4-year-old child who requires airborne precautions. As explained above, airborne precautions involve limiting movement outside the room to prevent exposure and transmission of microorganisms. Pulling a wagon with toys in the hallway may violate these precautions and increase the risk of infection for the child and others.
Therefore, this activity may not be allowed or advisable for the child.
Choice C reason: This choice is correct because putting a large-piece puzzle together is an appropriate activity for a 4-year-old child who requires airborne precautions. Putting a large-piece puzzle together can help to stimulate the child's cognitive, visual, and fine motor skills by requiring them to match shapes, colors, and patterns. It can also help to reduce boredom, frustration, or anxiety by providing entertainment, diversion, or achievement. Therefore, this activity may be beneficial and enjoyable for the child.
Choice D reason: This choice is incorrect because watching a video game in the playroom is not an appropriate activity for a 4-year-old child who requires airborne precautions. As explained above, airborne precautions involve limiting movement outside the room to prevent exposure and transmission of microorganisms. Watching a video game in the playroom may violate these precautions and increase the risk of infection for the child and others.
Therefore, this activity may not be permitted or recommended for the child.
A nurse is providing discharge instructions to a parent and his school-age child who has juvenile idiopathic arthritis. Which of the following instructions should the nurse include?
Explanation
Choice A reason: This choice is incorrect because applying cool compresses for 20 min every hour is not an effective instruction for a parent and his school-age child who has juvenile idiopathic arthritis. Juvenile idiopathic arthritis is an autoimmune disorder that causes inflammation and stiffness of the joints, resulting in pain, swelling, reduced range of motion, or deformity. Applying cool compresses may help to reduce inflammation and pain in acute episodes, but it may also cause vasoconstriction and impair blood flow to the joints. Therefore, applying warm compresses or taking warm baths may be more beneficial and comfortable for the child.
Choice B reason: This choice is correct because encouraging the child to take a 45-minute nap daily is an effective instruction for a parent and his school-age child who has juvenile idiopathic arthritis. Encouraging the child to take a 45-minute nap daily can help promote rest and relaxation, which are essential for healing and recovery. It can also help to reduce fatigue, stress, or depression, which are common complications of chronic illness. Therefore, encouraging the child to take a 45-minute nap daily can help to improve the physical and mental well-being of the child.
Choice C reason: This choice is incorrect because allowing the child to stay at home on days when her joints are painful is not an effective instruction for a parent and his school-age child who has juvenile idiopathic arthritis.
Allowing the child to stay at home on days when her joints are painful may reinforce the idea that pain limits her activities and abilities, which can affect her self-esteem and socialization. It may also cause muscle atrophy,
joint contractures, or deformities due to lack of movement. Therefore, encouraging the child to attend school and participate in regular physical therapy and exercise can help to maintain her joint function, mobility, and quality of life.
Choice D reason: This choice is incorrect because administering prednisone on an alternate-day schedule is not an effective instruction for a parent and his school-age child who has juvenile idiopathic arthritis. Prednisone is a corticosteroid medication that suppresses the immune system and reduces inflammation and pain in the joints. It may be used for short-term or long-term treatment of juvenile idiopathic arthritis, but it can cause serious side effects such as weight gain, growth retardation, osteoporosis, or infection. Therefore, administering prednisone on an alternate-day schedule may not provide adequate or consistent relief for the child, and it may increase the risk of complications.
A nurse is caring for a child who has tinea pedis. The child's parent asks the nurse what this infection is commonly called. The nurse should respond with which of the following common names?
Explanation
Choice A: Shingles is a viral infection that causes a painful rash, usually on one side of the body. It is caused by the same virus that causes chickenpox. Shingles is not related to tinea pedis, which is a fungal infection.
Choice B: Valley fever is a fungal infection that affects the lungs and can cause flu-like symptoms, such as fever, cough, and chest pain. It is caused by inhaling spores from a fungus that grows in dry soil. Valley fever is not related to tinea pedis, which affects the skin of the feet.
Choice C: Athlete's foot is a common name for tinea pedis, which is a fungal infection that affects the skin between the toes and on the soles of the feet. It can cause itching, burning, scaling, and cracking of the skin. Athlete's foot is contagious and can be spread by direct contact or by sharing shoes, socks, or towels.
Choice D: Fever blister is another name for a cold sore, which is a small blister that forms on or near the lips. It is caused by a type of herpes virus that can be transmitted by kissing or sharing utensils. Fever blister is not related to tinea pedis, which is a fungal infection.
A nurse is teaching a parent of a child who has hemophilia how to control a minor bleeding episode. Which of the following statements by the parent indicates a need for further teaching?
Explanation
Choice A: Applying heat to a bleeding site can increase blood flow and worsen the bleeding. This statement indicates a need for further teaching, as the parent should avoid applying heat and use cold compresses instead.
Choice B: Having the child rest can reduce physical activity and prevent further injury or bleeding. This statement indicates that the parent understands the teaching, as resting is one of the recommended actions for controlling a minor bleeding episode.
Choice C: Compressing the site can apply pressure and stop the bleeding. This statement indicates that the parent understands the teaching, as compressing is one of the recommended actions for controlling a minor bleeding episode.
Choice D: Elevating the affected part can reduce blood pressure and slow down the bleeding. This statement indicates that the parent understands the teaching, as elevating is one of the recommended actions for controlling a minor bleeding episode.
A nurse is providing teaching about lice to the parents of a school-age child at a well-child visit. Which of the following information should the nurse include in the teaching?
Explanation
Choice A: Lice cannot survive for more than 48 hours away from the host. This statement is false and should not be included in the teaching, as it can cause unnecessary anxiety or confusion.
Choice B: Washing your child's hair daily will not prevent lice, as lice do not depend on hair cleanliness or hygiene.
This statement is false and should not be included in the teaching, as it can create a false sense of security or stigma.
Choice C: Lice cannot jump or fly from one child to another, as they only crawl. This statement is false and should not be included in the teaching, as it can cause unnecessary fear or panic.
Choice D: Encouraging your child to avoid sharing hats with other children can prevent lice, as lice can be transmitted by direct contact or by sharing personal items. This statement is true and should be included in the teaching, as it can help prevent lice infestation or spread.
A nurse is providing teaching about lice to the parents of a school-age child at a well-child visit. Which of the the following information should the nurse include in the teaching?
Explanation
Choice A: Lice cannot survive for more than 48 hours away from the host. This statement is false and should not be included in the teaching, as it can cause unnecessary anxiety or confusion.
Choice B: Washing your child's hair daily will not prevent lice, as lice do not depend on hair cleanliness or hygiene. This statement is false and should not be included in the teaching, as it can create a false sense of security or stigma.
Choice C: Lice cannot jump or fly from one child to another, as they only crawl. This statement is false and should not be included in the teaching, as it can cause unnecessary fear or panic.
Choice D: Encouraging your child to avoid sharing hats with other children can prevent lice, as lice can be transmitted by direct contact or by sharing personal items. This statement is true and should be included in the teaching, as it can help prevent lice infestation or spread.
A nurse is caring for a child who has a suspected diagnosis of bacterial meningitis. Which of the following actions is the nurse's priority?
Explanation
Choice A: Reducing environmental stimuli can help decrease the discomfort and agitation of a child who has meningitis, as they may experience headache, photophobia, and neck stiffness. However, this action is not the priority, as it does not address the cause of the infection or prevent complications.
Choice B: Documenting intake and output can help monitor the fluid balance and hydration status of a child who has meningitis, as they may have fever, vomiting, and decreased oral intake. However, this action is not the priority, as it does not address the cause of the infection or prevent complications.
Choice C: Administering antibiotics when available can help treat the bacterial infection that causes meningitis and prevent serious complications such as brain damage, hearing loss, or death. This action is the priority, as it can save the child's life and improve their outcome.
Choice D: Maintaining seizure precautions can help protect the child from injury and provide safety measures in case of a seizure, as meningitis can cause increased intracranial pressure and seizures. However, this action is not the priority, as it does not address the cause of the infection or prevent complications.
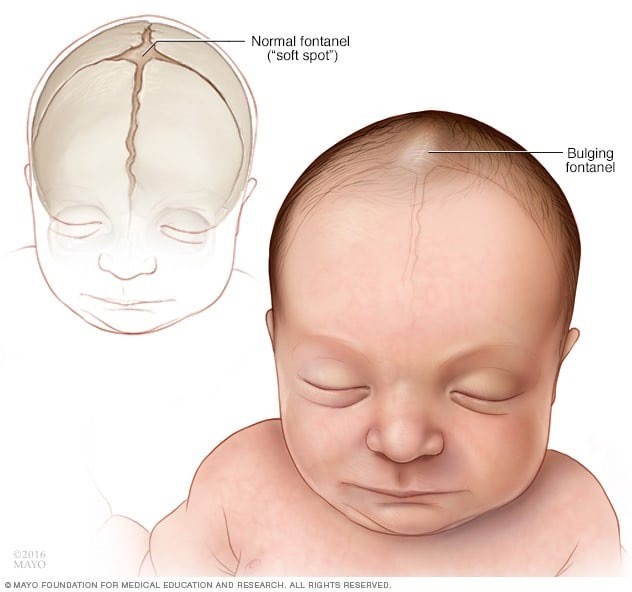
A nurse is assessing an 11-month-old infant. Which of the following manifestations is associated with a CNS infection?
Explanation
Choice A: Oliguria is a condition of reduced urine output, which can indicate dehydration, kidney failure, or urinary tract obstruction. It is not associated with a CNS infection, which affects the brain and spinal cord.
Choice B: A negative Brudzinski sign is a normal finding that indicates no meningeal irritation. It is elicited by flexing the neck of a supine patient and observing no involuntary flexion of the hips and knees. A positive Brudzinski sign, on the other hand, is a sign of meningitis, which is a type of CNS infection.
Choice C: A bulging fontanel is an abnormal finding that indicates increased intracranial pressure, which can be caused by a CNS infection, such as meningitis or encephalitis. A fontanel is a soft spot on the skull of an infant that allows for brain growth and development.
Choice D: Jaundice is a condition of yellowing of the skin and eyes, which can indicate liver disease, hemolytic anemia, or neonatal hyperbilirubinemia. It is not associated with a CNS infection, which affects the brain and spinal cord.
Which of the following best describes a neuroblastoma?
Explanation
Choice A: Urinary incontinence is a condition of involuntary loss of urine control, which can be caused by various factors, such as nerve damage, bladder dysfunction, or medication side effects. It is not always caused by neuroblastoma, which is a type of cancer that arises from immature nerve cells.
Choice B: Blood-fed is not a term that describes a neuroblastoma. Neuroblastoma is a type of cancer that arises from immature nerve cells, which can form tumors in various parts of the body, such as the adrenal glands, abdomen, chest, or spine.
Choice C: Tiny is not a term that describes a neuroblastoma. Neuroblastoma can vary in size and shape depending on the location and stage of the tumor. Some neuroblastomas can be very large and cause compression of nearby organs or structures.
Choice D: Unfortunately, much of the time, by the time a diagnosis has been made, metastasis has already occurred. This statement describes a neuroblastoma accurately. Neuroblastoma is a type of cancer that arises from immature nerve cells, which can spread rapidly to other parts of the body, such as the bones, liver, lymph nodes, or skin.
Metastasis is the process of cancer cells breaking away from the original tumor and forming new tumors elsewhere. Neuroblastoma often has no specific symptoms until it has metastasized, making it difficult to diagnose early and treat effectively.
Sign Up or Login to view all the 87 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
