ATI Pharmacology
Total Questions : 51
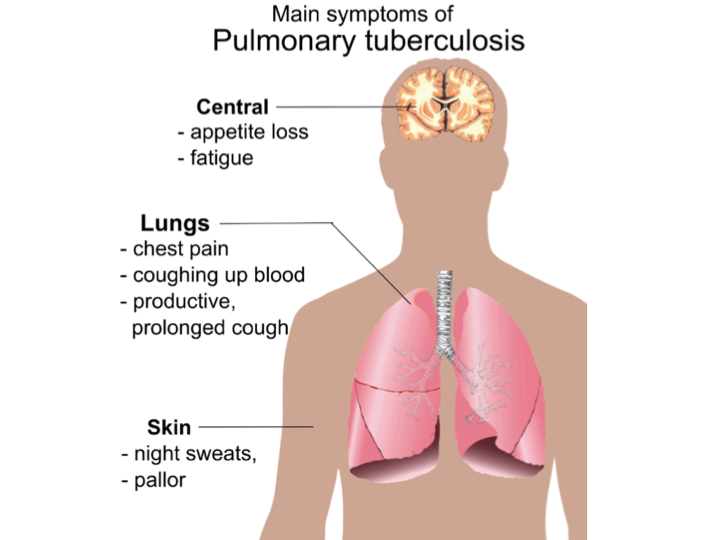
Showing 25 questions, Sign in for moreA nurse in a provider’s office is assessing a client. The nurse should identify that which of the following findings are manifestations of pulmonary tuberculosis? (Select all that apply)
Explanation
Choice A reason: This is incorrect. Weight gain is not a manifestation of pulmonary tuberculosis. In fact, weight loss is a common symptom of tuberculosis, as the infection causes the body to use more energy and reduce appetite. Weight loss can also be a result of malnutrition, dehydration, or other complications of tuberculosis.
Choice B reason: This is correct. Night sweats are a manifestation of pulmonary tuberculosis. They occur because the infection causes the body to produce more heat and sweat to fight off the bacteria. Night sweats can also be a sign of fever, which is another symptom of tuberculosis.
Choice C reason: This is correct. Low-grade fever is a manifestation of pulmonary tuberculosis. It occurs because the infection causes the body to raise its temperature to kill the bacteria. Fever can also be accompanied by chills, fatigue, or weakness.
Choice D reason: This is correct. Blood in the sputum is a manifestation of pulmonary tuberculosis. It occurs because the infection causes damage and inflammation to the lungs and the airways, which can bleed and mix with the mucus that is coughed up. Blood in the sputum can also be a sign of a serious complication, such as a ruptured blood vessel or a lung abscess.
Choice E reason: This is incorrect. Flushed cheeks are not a manifestation of pulmonary tuberculosis. They can be caused by various factors, such as embarrassment, exercise, alcohol, or hot weather. Flushed cheeks are not related to the infection or the inflammation of the lungs.
A nurse is caring for a client who had a stroke involving the right cerebral hemisphere. The nurse should monitor for which of the following findings?
Explanation
Choice A reason: A stroke involving the right cerebral hemisphere can affect the cognitive and emotional functions of the brain, such as judgment, impulse control, and emotional regulation³. This can lead to risky or inappropriate behaviors, such as acting impulsively or disregarding social norms. Therefore, the nurse should monitor the client for poor impulse control and provide appropriate interventions, such as education, cueing, feedback, and environmental modifications.
Choice B reason: A stroke involving the right cerebral hemisphere can affect the visual functions of the brain, such as depth perception, spatial orientation, and visual recognition³. However, the deficits are usually in the left visual field, not the right, because the right side of the brain controls the left side of the body and the environment. Therefore, the nurse should monitor the client for deficits in the left visual field, not the right.
Choice C reason: A stroke involving the right cerebral hemisphere can affect the abstract reasoning functions of the brain, such as understanding metaphors, humor, or sarcasm. However, the ability to discriminate words and letters is more related to the language functions of the brain, which are mainly controlled by the left cerebral hemisphere. Therefore, the nurse should monitor the client for language deficits, such as aphasia or dysarthria, if the stroke involves the left cerebral hemisphere, not the right.
Choice D reason: A stroke involving the right cerebral hemisphere can affect the motor functions of the brain, such as movement, coordination, and balance³. However, the motor retardation, which is a slowing down of physical and mental activity, is more related to the mood functions of the brain, which are mainly controlled by the frontal lobe of the brain. Therefore, the nurse should monitor the client for motor retardation if the stroke involves the frontal lobe, not the right cerebral hemisphere.
A nurse is caring for a client who has a head injury. The client states they fell off a ladder while painting approximately 2 hours ago and lost consciousness for 45 minutes according to their partner. The nurse should determine that the client is experiencing which of the following classifications of traumatic brain injury?
Explanation
This is incorrect. Moderate traumatic brain injury is defined as a head injury that results in a loss of consciousness for more than 30 minutes but less than 24 hours, a Glasgow Coma Scale (GCS) score of 9 to 12, or a posttraumatic amnesia (PTA) of more than 1 hour but less than 7 days. The client's loss of consciousness for 45 minutes meets the criterion for moderate injury, but the nurse should also consider the other factors, such as the GCS score and the PTA, which are not given in the text.
Choice B reason: This is correct. Severe traumatic brain injury is defined as a head injury that results in a loss of consciousness for more than 24 hours, a GCS score of 8 or less, or a PTA of more than 7 days. The client's loss of consciousness for 45 minutes does not meet the criterion for severe injury by itself, but it indicates a significant brain damage that may be associated with other signs of severe injury, such as coma, pupillary abnormalities, or intracranial hemorrhage. The nurse should assess the client's GCS score and PTA, as well as perform a neurological examination and order imaging studies to confirm the diagnosis of severe injury.
Choice C reason: This is incorrect. Mild traumatic brain injury, also known as concussion, is defined as a head injury that results in a loss of consciousness for less than 30 minutes, a GCS score of 13 to 15, or a PTA of less than 1 hour. The client's loss of consciousness for 45 minutes exceeds the criterion for mild injury and suggests a more serious brain damage that may require intensive care and monitoring.
Choice D reason: This is incorrect. No traumatic brain injury is defined as a head injury that does not result in any alteration of brain function or evidence of brain pathology. The client's loss of consciousness for 45 minutes clearly indicates an alteration of brain function, and implies a possible brain pathology, such as contusion, hematoma, or edema. The nurse should not dismiss the client's injury as trivial, and should provide appropriate care and evaluation.
A nurse is planning care for a female client who has a T4 spinal cord injury and is at risk for acquiring urinary tract infections. Which of the following actions should the nurse include in the client’s plan of care?
Explanation
Choice A reason: This is incorrect. Cleansing the perineum from back to front can increase the risk of urinary tract infections, as it can introduce bacteria from the anal area to the urethra. The nurse should instruct the client to cleanse the perineum from front to back, using a mild soap and water, and to change the pad or underwear frequently to prevent bacterial growth.
Choice B reason: This is incorrect. Obtaining a prescription for an indwelling urinary catheter can increase the risk of urinary tract infections, as it can create a direct route for bacteria to enter the bladder. Indwelling catheters should be avoided unless absolutely necessary, and should be removed as soon as possible. The nurse should explore other bladder management options for the client, such as intermittent catheterization, condom catheter, or suprapubic catheter.
Choice C reason: This is incorrect. Offering the client the bedpan every 2 hours can increase the risk of urinary tract infections, as it can cause urinary stasis and bladder distension. The nurse should assess the client's bladder function and determine the optimal frequency of bladder emptying, which may vary depending on the type and level of spinal cord injury. The nurse should also monitor the client's urine output, color, odor, and clarity, and report any signs of infection, such as fever, chills, or flank pain.
Choice D reason: This is correct. Encouraging fluid intake at and between meals can decrease the risk of urinary tract infections, as it can flush out bacteria from the urinary tract and prevent urinary stasis and bladder distension. The nurse should advise the client to drink at least 2 liters of water per day, unless contraindicated by other medical conditions. The nurse should also educate the client about the benefits of cranberry juice, which can inhibit bacterial adhesion to the bladder wall and prevent infection.
A nurse is caring for a client who has had a stroke involving the right hemisphere. Which of the following alterations in function should the nurse expect?
Explanation
Choice A reason: This is incorrect. Right hemiparesis is not a common finding in clients who had a stroke involving the right hemisphere. Hemiparesis is the weakness or partial paralysis of one side of the body. It usually affects the opposite side of the body from the side of the brain that is damaged by the stroke. Therefore, a stroke in the right hemisphere would more likely cause left hemiparesis, not right hemiparesis.
Choice B reason: This is incorrect. Aphasia is not a common finding in clients who had a stroke involving the right hemisphere. Aphasia is the loss or impairment of language functions, such as speaking, understanding, reading, or writing. It usually affects the dominant hemisphere of the brain, which is the left hemisphere for most people. Therefore, a stroke in the right hemisphere would less likely cause aphasia, unless the person is lefthanded or ambidextrous.
Choice C reason: This is correct. Inability to recognize his family members is a common finding in clients who had a stroke involving the right hemisphere. This is a type of agnosia, which is the loss or impairment of the ability to recognize objects, people, sounds, shapes, or smells. The right hemisphere of the brain is responsible for processing visual and spatial information, as well as facial recognition. A stroke in this area can damage the ability to identify familiar faces, even those of close relatives or friends.
Choice D reason: This is incorrect. Difficulty reading is not a common finding in clients who had a stroke involving the right hemisphere. Reading is a language function that involves the recognition and comprehension of written words. It usually depends on the dominant hemisphere of the brain, which is the left hemisphere for most people. Therefore, a stroke in the right hemisphere would less likely cause difficulty reading, unless the person is lefthanded or ambidextrous.
A nurse is providing discharge teaching to a client who has pulmonary tuberculosis and a new prescription for rifampin. Which of the following information should the nurse provide?
Explanation
Choice A reason: This is incorrect. It is not best to take medication with meals. Rifampin is better absorbed when taken on an empty stomach, at least 1 hour before or 2 hours after a meal. Taking rifampin with food can reduce its effectiveness and increase the risk of drug resistance. The nurse should advise the client to take the medication as directed by the doctor, and to avoid foods that can interact with rifampin, such as cheese, yogurt, or alcohol.
Choice B reason: This is incorrect. Treatment with this medication will not last for 1 month. Rifampin is usually given as part of a combination therapy for pulmonary tuberculosis, along with other drugs such as isoniazid, pyrazinamide, and ethambutol. The standard treatment regimen for drug susceptible tuberculosis consists of an intensive phase of 2 months, followed by a continuation phase of 4 or 7 months, depending on the drug regimen and the patient's response. The nurse should inform the client about the duration and the importance of completing the full course of treatment, even if the symptoms improve or the tests become negative.
Choice C reason: This is incorrect. This medication does not cause insomnia. Rifampin does not affect the sleep cycle or the quality of sleep. However, rifampin can cause other side effects, such as nausea, vomiting, diarrhea, headache, or rash. The nurse should instruct the client to report any severe or persistent side effects to the doctor, and to avoid taking over-the-counter drugs or herbal supplements without consulting the doctor, as rifampin can interact with many other medications and reduce their effectiveness.
Choice D reason: This is correct. Urine and other secretions might turn orange. Rifampin can cause a harmless discoloration of body fluids, such as urine, saliva, sweat, tears, or breast milk. The color can range from orange to red or brown, depending on the concentration of the drug and the pH of the fluid. The nurse should reassure the client that this is a normal and expected effect of rifampin, and that it does not indicate any damage to the kidneys or other organs. The nurse should also warn the client that rifampin can stain contact lenses, dentures, or clothing, and advise the client to use disposable lenses, remove dentures before taking the drug, and wear dark colored clothes.
A nurse is providing discharge teaching to a client who has asthma and new prescriptions for cromolyn and albuterol, both by nebulizer. Which of the following statements by the client indicates an understanding of the teaching?
Explanation
Choice A reason: This is incorrect. Taking the albuterol before taking the cromolyn is not necessary. Albuterol and cromolyn are both used to treat asthma, but they have different mechanisms of action. Albuterol is a bronchodilator that relaxes the muscles around the airways and opens them up, making it easier to breathe. Cromolyn is a mast cell stabilizer that prevents the release of substances that cause inflammation and allergy symptoms in the airways. Albuterol is used to relieve acute asthma attacks, while cromolyn is used to prevent chronic asthma symptoms. The nurse should advise the client to use albuterol as needed for quick relief, and to use cromolyn regularly as prescribed to prevent asthma flareups.
Choice B reason: This is incorrect. Using both medications immediately after exercising is not recommended. Exercise can trigger asthma symptoms in some people, such as wheezing, coughing, or shortness of breath. This is called exercise induced bronchoconstriction (EIB) or exercise induced asthma (EIA). The nurse should advise the client to use albuterol 15 to 30 minutes before exercising to prevent EIB or EIA, and to avoid exercising in cold, dry, or polluted air. The nurse should also instruct the client to use cromolyn at least 15 minutes before exercising, as it takes time to work and does not provide immediate relief. The nurse should also tell the client to stop exercising and use albuterol if asthma symptoms occur during or after exercising.
Choice C reason: This is incorrect. Using cromolyn immediately if the breathing begins to feel tight is not effective. Cromolyn is not a rescue medication that can provide quick relief of asthma symptoms. It is a preventive medication that works by reducing the inflammation and sensitivity of the airways over time. The nurse should advise the client to use albuterol instead of cromolyn if the breathing begins to feel tight, as albuterol can rapidly open up the airways and ease the breathing. The nurse should also instruct the client to seek medical attention if the albuterol does not work or if the symptoms get worse.
Choice D reason: This is correct. Administering the medications 10 minutes apart is good practice. Cromolyn and albuterol can be used together to treat asthma, but they should not be mixed in the same nebulizer, as they may not be compatible and may lose their effectiveness. The nurse should instruct the client to use separate nebulizers for each medication, and to wait at least 10 minutes between each nebulization to allow the medication to reach the lungs and avoid irritation of the airways. The nurse should also teach the client how to use the nebulizer properly, and how to clean and store it after each use.

A nurse is assessing a client who is 1 day postoperative following a lobectomy and has a chest tube drainage system in place. Which of the following findings by the nurse indicates a need for intervention?
Explanation
Choice A : This is incorrect. Development of subcutaneous emphysema is not a finding that requires intervention. Subcutaneous emphysema is the presence of air under the skin, which can cause a crackling sensation when touched. It can occur after a lobectomy due to the leakage of air from the lung or the chest tube into the surrounding tissues. It is usually harmless and resolves on its own as the air is absorbed by the body. The nurse should monitor the client for signs of respiratory distress, such as dyspnea, cyanosis, or hypoxia, and report them to the doctor if they occur.
Choice B : This is incorrect. Chest tube eyelets not visible is not a finding that requires intervention. Chest tube eyelets are the small holes at the end of the chest tube that allow the drainage of air or fluid from the pleural space. They are usually not visible when the chest tube is inserted, as they are covered by the dressing or the drainage system. The nurse should check the position and patency of the chest tube by observing the drainage amount and color, and by auscultating the breath sounds over the affected lung. The nurse should also secure the chest tube with tape or sutures, and avoid pulling or kinking it.
Choice C : This is correct. Continuous bubbling in the suction control chamber is a finding that requires intervention. The suction control chamber is the part of the chest drainage system that regulates the amount of negative pressure applied to the chest tube. It is filled with sterile water to a prescribed level, and connected to a suction source. Continuous bubbling in this chamber indicates that there is an air leak in the system, which can compromise the drainage and the lung expansion. The nurse should locate and seal the source of the leak, which can be in the tubing, the connections, or the drainage system itself. The nurse should also notify the doctor if the leak persists or worsens.
Choice D: This is incorrect. The presence of tidal fluctuation in the water seal chamber is not a finding that requires intervention. The water seal chamber is the part of the chest drainage system that prevents the backflow of air or fluid into the pleural space. It is filled with sterile water to a prescribed level, and acts as a one-way valve. Tidal fluctuation is the rise and fall of the water level in this chamber with the client's breathing. It indicates that the chest tube is patent and that the lung is expanding and contracting normally. The nurse should observe the water level and report any changes, such as cessation of fluctuation, excessive fluctuation, or continuous bubbling, which can indicate problems with the chest tube or the lung.
A nurse is caring for a child who is experiencing status asthmaticus. Which of the following interventions is the priority for the nurse to take?
Explanation
Choice A reason: Administering an inhaled glucocorticoid is not the priority intervention for a child with status asthmaticus. Inhaled glucocorticoids are anti-inflammatory drugs that reduce airway inflammation and prevent asthma attacks, but they do not provide immediate relief of bronchoconstriction.
Choice B reason: Administering a short acting beta agonist (SABA) is the priority intervention for a child with status asthmaticus. SABAs are bronchodilators that relax the smooth muscles of the airways and improve airflow within minutes. They are the first line treatment for acute asthma symptoms and exacerbations.
Choice C reason: Determining the cause of the acute exacerbation is not the priority intervention for a child with status asthmaticus. While it is important to identify and avoid potential triggers of asthma, such as allergens, infections, or stress, this is not an urgent action during a severe asthma attack.
Choice D reason: Obtaining a peak flow reading is not the priority intervention for a child with status asthmaticus. Peak flow is a measure of how quickly the child can blow air out of the lungs, and it can indicate the degree of airway obstruction. However, peak flow measurement is not reliable or feasible during a severe asthma attack, and it should not delay the administration of bronchodilators.
A nurse is caring for a client who has a three-chamber closed chest tube system. Which of the following actions should the nurse take after noticing a rise in the water seal chamber with client inspiration?
Explanation
Choice A reason: Repositioning the client toward the left side is not necessary or helpful for a client who has a three-chamber closed chest tube system. The chest tube drainage system must always be placed below the drainage site and secured in an upright position to prevent it from being knocked over.
Choice B reason: Continuing to monitor the client is the appropriate action for the nurse to take after noticing a rise in the water seal chamber with client inspiration. The water in the water seal chamber should rise with inhalation and fall with exhalation (this is called tidaling), which demonstrates that the chest tube is patent. This is a normal finding and does not indicate a problem with the chest tube system or the client's condition.
Choice C reason: Clamping the chest tube near the water seal is not recommended for a client who has a three-chamber closed chest tube system. Clamping the chest tube can cause a buildup of air or fluid in the pleural space and increase the risk of complications such as tension pneumothorax or infection. Clamping the chest tube should only be done in certain situations, such as changing the drainage system, checking for an air leak, or removing the chest tube.
Choice D reason: Immediately notifying the provider is not necessary for a client who has a three-chamber closed chest tube system and shows a rise in the water seal chamber with client inspiration. As mentioned above, this is a normal finding and does not indicate a problem with the chest tube system or the client's condition. The nurse should only notify the provider if there are signs of complications, such as continuous bubbling in the water seal chamber, excessive drainage, chest pain, dyspnea, or subcutaneous emphysema.
A nurse is caring for a client who has increased intracranial pressure (ICP) following a closed head injury. Which of the following actions should the nurse take?
Explanation
Choice A reason: Using log rolling to reposition the client is not advisable for a client who has increased ICP. Log rolling is a technique that involves moving the client as a unit, without flexing the spine, to prevent spinal cord injury. However, log rolling can also increase ICP by reducing venous drainage from the head and increasing cerebral blood volume. Therefore, the nurse should avoid log rolling the client unless there is a suspected spinal injury.
Choice B reason: Instructing the client to cough and breathe deep is not appropriate for a client who has increased ICP. Coughing and deep breathing can increase intrathoracic pressure, which can reduce venous return to the heart and increase ICP. Additionally, coughing and deep breathing can cause hyperventilation, which can lower the partial pressure of carbon dioxide in the blood and cause cerebral vasoconstriction. This can reduce cerebral perfusion and oxygen delivery to the brain.
Choice C reason: Placing a warming blanket on the client is not recommended for a client who has increased ICP. A warming blanket can increase the body temperature, which can increase the metabolic rate and oxygen demand of the brain. This can worsen cerebral ischemia and edema. Moreover, a warming blanket can cause vasodilation, which can increase cerebral blood volume and ICP. Therefore, the nurse should maintain a normal body temperature for the client and avoid hyperthermia.
Choice D reason: Placing the client in a supine position is the best action for the nurse to take for a client who has increased ICP. The supine position is a way of lying on a table with the back, face, and abdomen facing upwards. It is used for various surgeries and examinations, such as cranial, cardiac, abdominal, and thoracic surgery. It can also prevent respiratory, skin, and circulatory problems. The supine position can help lower ICP by facilitating venous drainage from the head and reducing cerebral blood volume [^10^]. However, the nurse should also elevate the head of the bed to 30 degrees to optimize cerebral perfusion pressure and avoid neck flexion or rotation, which can impair venous drainage.
A nurse is teaching a 12yearold child who is newly diagnosed with asthma about managing the condition to prevent asthma attacks. Which of the following statements by the child should indicate to the nurse that the teaching has been effective?
Explanation
Choice A reason: This statement indicates that the child understands the role of allergens in triggering asthma symptoms and the importance of avoiding or reducing exposure to them. Allergens such as dust mites, animal dander, mold, and pollen can cause inflammation and constriction of the airways, leading to wheezing, coughing, and shortness of breath. The nurse should teach the child how to identify and eliminate or minimize allergens in the home, school, and outdoor environments.
Choice B reason: This statement is true, but it does not indicate that the child has learned how to manage the condition to prevent asthma attacks. Missing school days is a consequence of poorly controlled asthma, not a cause or a trigger¹². The nurse should teach the child how to use a written asthma action plan, which includes daily medications, peak flow monitoring, and rescue medications, to achieve good asthma control and reduce the risk of exacerbations.
Choice C reason: This statement is false and indicates that the child has a misconception about the impact of asthma on physical activity. Physical activity is beneficial for children with asthma, as it can improve lung function, cardiovascular fitness, and quality of life. The nurse should teach the child how to prevent exercise-induced bronchoconstriction, which is a common trigger of asthma symptoms, by using a short-acting bronchodilator before exercise, warming up and cooling down, and avoiding exercise in cold or polluted air.
Choice D reason: This statement is false and indicates that the child does not recognize the signs of poor asthma control. Coughing and shortness of breath in the morning are common symptoms of nocturnal asthma, which is a sign of uncontrolled asthma and a risk factor for severe asthma attacks. The nurse should teach the child how to monitor and record asthma symptoms and peak flow readings, and how to adjust medications according to the asthma action plan.
A nurse is assessing a client who has asthma. Which of the following areas should the nurse evaluate as the most reliable indicator of central cyanosis?
Explanation
Choice A reason: The oral mucosa is the most reliable indicator of central cyanosis because it reflects the oxygen saturation of the arterial blood. Central cyanosis occurs when the arterial blood has a low oxygen saturation due to a cardiopulmonary problem. The oral mucosa is less affected by peripheral factors such as temperature, vasoconstriction, or skin pigmentation.
Choice B reason: The conjunctivae are not a reliable indicator of central cyanosis because they can be affected by other conditions such as anemia, jaundice, or eye infections. The conjunctivae are the thin membranes that cover the white part of the eye and the inner surface of the eyelids.
Choice C reason: The ear lobes are not a reliable indicator of central cyanosis because they can be affected by peripheral factors such as temperature, vasoconstriction, or skin pigmentation. The ear lobes are the fleshy lower part of the external ear.
Choice D reason: The soles of the feet are not a reliable indicator of central cyanosis because they can be affected by peripheral factors such as temperature, vasoconstriction, or skin pigmentation. The soles of the feet are the bottom part of the feet.
A nurse is assessing a client’s cranial nerves as part of a neurological examination. Which of the following actions should the nurse take to assess cranial nerve III?
Explanation
Choice A reason: Eliciting the gag reflex is not a valid way to assess cranial nerve III. The gag reflex is a protective mechanism that prevents choking or aspiration by triggering a contraction of the pharyngeal muscles when the back of the throat is stimulated. The gag reflex is mediated by cranial nerves IX and X, not III.
Choice B reason: Checking the pupillary response to light is a reliable way to assess cranial nerve III. The pupillary response to light is a reflex that causes the pupil to constrict when exposed to bright light and dilate when exposed to dim light. This reflex helps to regulate the amount of light that enters the eye and protects the retina from damage. The pupillary response to light is controlled by cranial nerve III, which innervates the sphincter pupillae muscle that constricts the pupil.
Choice C reason: Observing for facial symmetry is not a relevant way to assess cranial nerve III. Facial symmetry is the degree of similarity between the two halves of the face. Facial symmetry can be affected by various factors, such as genetics, aging, or facial nerve palsy. Facial nerve palsy is a condition that causes weakness or paralysis of the muscles that control facial expression. Facial nerve palsy is caused by damage to cranial nerve VII, not III.
Choice D reason: Testing visual acuity is not a sufficient way to assess cranial nerve III. Visual acuity is the ability to see fine details and distinguish objects at a distance. Visual acuity depends on various factors, such as the clarity of the lens and cornea, the shape of the eyeball, and the function of the retina. Visual acuity is mainly affected by cranial nerve II, which carries visual information from the retina to the brain. Cranial nerve III does not directly influence visual acuity, but it does innervate some of the muscles that move the eye and enable binocular vision.
A nurse is caring for a client who has an endotracheal tube and is receiving mechanical ventilation. Which of the following actions should the nurse take to reduce the risk of ventilator associated pneumonia?
Explanation
Choice A reason: Positioning the head of the client’s bed in the flat position is not a good way to reduce the risk of ventilator associated pneumonia. This position can increase the risk of aspiration of oral secretions or gastric contents into the lungs, which can cause infection. The nurse should elevate the head of the bed to 30 to 45 degrees to prevent aspiration and promote drainage of secretions.
Choice B reason: Brushing the client’s teeth with a suction toothbrush every 12 hr is an effective way to reduce the risk of ventilator associated pneumonia. Oral hygiene can reduce the number of bacteria in the mouth and prevent the formation of dental plaque, which can harbor pathogens that can cause pneumonia. The nurse should use a suction toothbrush to remove debris and secretions from the mouth and prevent them from entering the lungs.
Choice C reason: Providing humidity by maintaining moisture within the ventilator tubing is not a helpful way to reduce the risk of ventilator associated pneumonia. Humidity can increase the growth of bacteria and fungi in the ventilator circuit, which can contaminate the air delivered to the lungs. The nurse should change the ventilator tubing and filters regularly and use sterile water to fill the humidifier.
Choice D reason: Turning the client every 4 hr is not a sufficient way to reduce the risk of ventilator associated pneumonia. Turning can help prevent pressure ulcers and improve blood circulation, but it does not prevent the accumulation of secretions in the lungs, which can cause infection. The nurse should use chest physiotherapy, suctioning, and coughing techniques to mobilize and clear secretions from the airways.
A nurse is caring for a client who has had a hemorrhagic stroke following a ruptured cerebral aneurysm. Which of the following manifestations should the nurse expect?
Explanation
Choice A reason: A history of neurologic deficits lasting less than 1 hr is not a typical manifestation of a hemorrhagic stroke. This could be a sign of a transient ischemic attack (TIA), which is a temporary blockage of blood flow to the brain that causes stroke like symptoms. A TIA is different from a hemorrhagic stroke, which is caused by bleeding in the brain due to a ruptured blood vessel.
Choice B reason: Manifestations preceded by a severe headache is a common manifestation of a hemorrhagic stroke. A ruptured cerebral aneurysm can cause sudden and intense pain in the head, often described as the worst headache of one's life. This is due to the increased pressure and irritation of the brain tissue and nerves by the blood leaking from the aneurysm.
Choice C reason: A gradual onset of several hours is not a usual manifestation of a hemorrhagic stroke. A hemorrhagic stroke is a medical emergency that requires immediate treatment, as the bleeding can cause rapid damage to the brain and increase the risk of death or disability. The symptoms of a hemorrhagic stroke usually develop suddenly and worsen quickly.
Choice D reason: Maintaining consciousness is not a likely manifestation of a hemorrhagic stroke. A hemorrhagic stroke can cause loss of consciousness, confusion, drowsiness, or coma due to the reduced blood flow and oxygen to the brain. The level of consciousness can also be affected by the location and extent of the bleeding, as well as the presence of complications such as hydrocephalus or vasospasm.
A nurse is evaluating teaching on a client who has a new prescription for montelukast to treat asthma. Which of the following statements by the client indicates an understanding of the teaching?
Explanation
Choice A reason: Taking this medication when getting an asthma attack is not a correct way to use montelukast. Montelukast is a leukotriene modifier that helps to reduce inflammation and prevent asthma attacks and exercise induced bronchoconstriction. It is taken once a day in oral form and may cause side effects such as stomach pain, diarrhea, or mood changes. It is not a fast acting rescue medicine for asthma attacks and needs to be taken daily.
Choice B reason: Rinsing the mouth after taking this medication is not necessary or helpful for montelukast. Rinsing the mouth is usually recommended for inhaled corticosteroids, which can cause oral thrush, a fungal infection in the mouth. Montelukast is not an inhaled corticosteroid and does not cause oral thrush.
Choice C reason: Taking this medication once a day in the evening is the correct way to use montelukast. Montelukast works best when taken in the evening, as it can improve the symptoms of asthma and allergic rhinitis that occur at night or early in the morning. Taking it at the same time every day can also help to maintain a steady level of the drug in the body and prevent missed doses.
Choice D reason: Using a spacer device when inhaling this medication is not applicable or useful for montelukast. A spacer device is a tube that attaches to an inhaler and helps to deliver the medication more effectively to the lungs. Montelukast is not an inhaler, but a tablet or a granule that is swallowed.
A nurse in a provider’s office is assessing an older adult client whose son reports that the client has been sick with a respiratory illness for the past 6 days. Which of the following assessment findings is a manifestation of pneumonia in the older adult client?
Explanation
Choice A reason: Narrowed pulse pressure is not a specific manifestation of pneumonia in the older adult client. Pulse pressure is the difference between the systolic and diastolic blood pressure readings. A normal pulse pressure is about 40 mm Hg, and a narrowed pulse pressure is less than 25 mm Hg. A narrowed pulse pressure can indicate various conditions, such as heart failure, shock, or aortic stenosis, but it is not a sign of pneumonia.
Choice B reason: Night sweats are not a common manifestation of pneumonia in the older adult client. Night sweats are episodes of excessive sweating during sleep that can soak the bedding or clothing. Night sweats can have many causes, such as menopause, infections, medications, or cancer, but they are not typically associated with pneumonia.
Choice C reason: Bradycardia is not a usual manifestation of pneumonia in the older adult client. Bradycardia is a slow heart rate, defined as less than 60 beats per minute. Bradycardia can be normal in some people, such as athletes or those who are very fit, or it can be a sign of a problem with the heart's electrical system. Pneumonia does not cause bradycardia, but it can cause tachycardia, which is a fast heart rate, due to the increased oxygen demand and inflammation.
Choice D reason: Confusion is a frequent manifestation of pneumonia in the older adult client. Confusion is a state of impaired awareness, orientation, memory, or judgment. Confusion can occur in older adults with pneumonia due to several factors, such as hypoxia, dehydration, electrolyte imbalance, fever, or infection. Confusion can also increase the risk of complications, such as aspiration, falls, or delirium. Therefore, the nurse should monitor the mental status of the older adult client with pneumonia and report any changes to the provider..
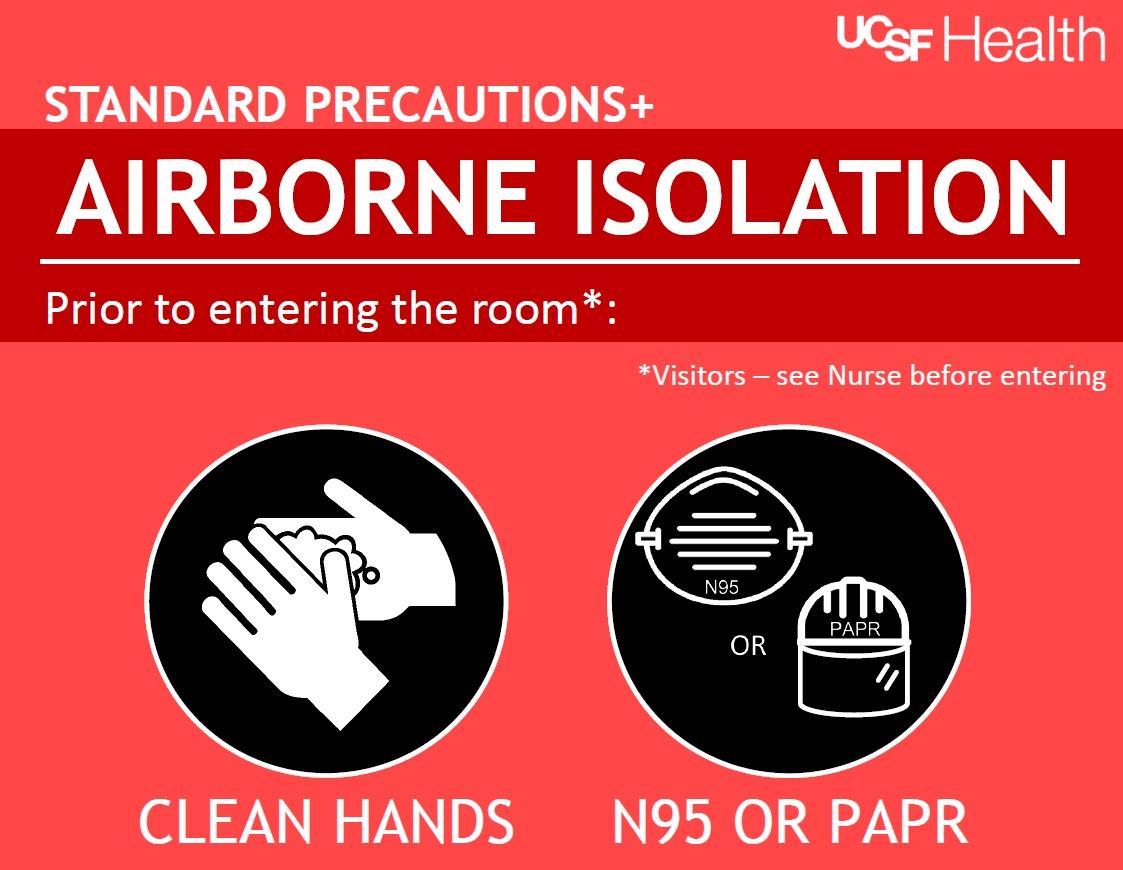
A nurse is admitting a client who has tuberculosis and a productive cough. Which of the following types of isolation precautions should the nurse initiate for the client?
Explanation
Choice A reason: Droplet precautions are not appropriate for a client who has tuberculosis and a productive cough. Droplet precautions are used to prevent the transmission of infectious agents that are spread by large respiratory droplets, such as influenza, pertussis, or meningitis. Droplet precautions require the use of a surgical mask, eye protection, and gloves when in close contact with the client.
Choice B reason: Protective precautions are not applicable for a client who has tuberculosis and a productive cough. Protective precautions are used to protect immunocompromised clients from exposure to pathogens, such as those undergoing chemotherapy, organ transplantation, or stem cell transplantation. Protective precautions require the use of a HEPA filter, a positive pressure room, and a mask for the client when leaving the room.
Choice C reason: Contact precautions are not sufficient for a client who has tuberculosis and a productive cough. Contact precautions are used to prevent the transmission of infectious agents that are spread by direct or indirect contact with the client or the client's environment, such as Clostridioides difficile, MRSA, or VRE. Contact precautions require the use of gloves and gowns when entering the room and the dedicated use of noncritical patientcare equipment.
Choice D reason: Airborne precautions are the correct type of isolation precautions for a client who has tuberculosis and a productive cough. Airborne precautions are used to prevent the transmission of infectious agents that are spread by small respiratory droplets that can remain suspended in the air, such as tuberculosis, measles, or chickenpox. Airborne precautions require the use of a respirator, such as an N95 mask, a negative pressure room, and a mask for the client when leaving the room.
A nurse is assessing a client who has a traumatic head injury to determine motor function response. Which of the following client responses to painful stimulus is expected?
Explanation
Choice A reason: Flexing the upper and extending the lower extremities in response to the painful stimulus is not an expected response for a client who has a traumatic head injury. This is a sign of decorticate posturing, which indicates damage to the cerebral hemispheres or the internal capsule. Decorticate posturing is a type of abnormal flexion that involves the abduction of the arms, internal rotation of the shoulders, flexion of the wrists, and extension of the legs.
Choice B reason: Pushing the painful stimulus away is not an expected response for a client who has a traumatic head injury. This is a sign of normal motor function, which indicates that the client can localize and withdraw from the painful stimulus. This is the highest level of motor response on the Glasgow Coma Scale (GCS), which is a neurological scoring system used to assess conscious level after head injury.
Choice C reason: Extending the body toward the painful stimulus is an expected response for a client who has a traumatic head injury. This is a sign of decerebrate posturing, which indicates damage to the brainstem or midbrain. Decerebrate posturing is a type of abnormal extension that involves the abduction of the arms, external rotation of the shoulders, extension of the wrists, and extension of the legs.
Choice D reason: Showing no reaction to the painful stimulus is not an expected response for a client who has a traumatic head injury. This is a sign of flaccid paralysis, which indicates damage to the spinal cord or peripheral nerves. Flaccid paralysis is a type of complete loss of muscle tone and reflexes that involves the absence of any voluntary or involuntary movements.
A nurse is caring for a client who had a stroke involving the left cerebral hemisphere. The nurse should monitor for which of the following findings?
Explanation
Choice A reason: Impaired sense of humor is not a common finding for a client who had a stroke involving the left cerebral hemisphere. Impaired sense of humor is more likely to occur after a stroke involving the right cerebral hemisphere, which is responsible for processing humor, irony, and sarcasm.
Choice B reason: Poor judgment is not a typical finding for a client who had a stroke involving the left cerebral hemisphere. Poor judgment is more likely to occur after a stroke involving the frontal lobe, which is involved in executive functions, such as planning, reasoning, and decision making.
Choice C reason: Intellectual impairment is a possible finding for a client who had a stroke involving the left cerebral hemisphere. The left cerebral hemisphere is dominant for language and analytical thinking in most people. A stroke affecting this hemisphere can impair the ability to speak, read, write, calculate, and comprehend information.
Choice D reason: Loss of depth perception is not a frequent finding for a client who had a stroke involving the left cerebral hemisphere. Loss of depth perception is more likely to occur after a stroke involving the occipital lobe, which is involved in visual processing, or the parietal lobe, which is involved in spatial awareness.
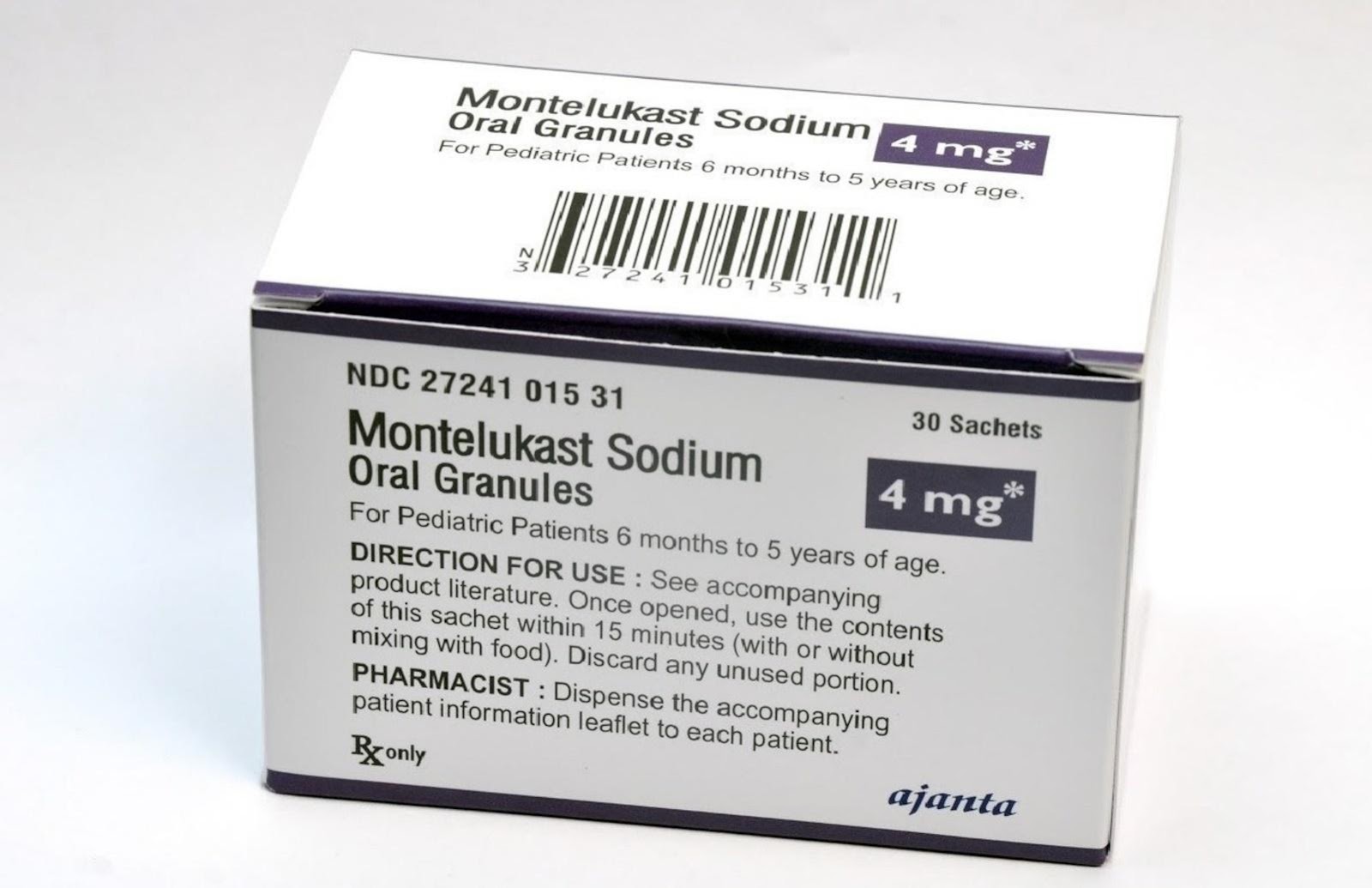
A nurse is caring for a child who has asthma and a prescription for montelukast granules. Which of the following instructions should the nurse provide the client’s parent on administering the medication?
Explanation
Choice A reason: Administering the medication 2 hr before exercise is a correct instruction for the parent of a child who has asthma and a prescription for montelukast granules. Montelukast is a leukotriene modifier that helps to prevent asthma attacks and exercise induced bronchoconstriction. It is taken once a day in oral form and may cause side effects such as stomach pain, diarrhea, or mood changes. For children who have exercise induced asthma, an additional dose of montelukast may be taken 2 hr before exercise.
Choice B reason: Giving the medication at the onset of wheezing is not a correct instruction for the parent of a child who has asthma and a prescription for montelukast granules. Montelukast is not a fast acting rescue medicine for asthma attacks and needs to be taken daily. It does not work quickly enough to relieve the symptoms of an acute asthma attack, such as wheezing, coughing, or shortness of breath. For an asthma attack, the child should use a short acting beta agonist inhaler, such as albuterol, as prescribed by the provider.
Choice C reason: Administering the granules mixed with 20 oz of water is not a correct instruction for the parent of a child who has asthma and a prescription for montelukast granules. Montelukast granules come in a sachet with 4 mg of granules inside (one dose). They can be placed directly on the child's tongue or mixed with a spoonful of cold or room temperature soft food, such as applesauce, mashed carrots, rice, or ice cream. They can also be mixed with 1 teaspoonful (5 mL) of cold or room temperature baby formula or breast milk. They should not be mixed with any other liquid drink other than baby formula or breast milk. The mixture should be taken within 15 minutes after opening the packet.
Choice D reason: Giving the medication in the morning daily is not a correct instruction for the parent of a child who has asthma and a prescription for montelukast granules. Montelukast works best when taken in the evening, as it can improve the symptoms of asthma and allergic rhinitis that occur at night or early in the morning. Taking it at the same time every day can also help to maintain a steady level of the drug in the body and prevent missed doses.
A nurse in a clinic sees a client who has an acute asthma exacerbation. Which of the following medications should reduce the symptoms?
Explanation
Choice A reason: Budesonide via dry powder inhaler is not a suitable medication for an acute asthma exacerbation. Budesonide is an inhaled corticosteroid that helps to reduce inflammation and prevent asthma attacks. It is taken daily as a maintenance therapy and does not work quickly enough to relieve the symptoms of an acute asthma exacerbation.
Choice B reason: Cromolyn via metered dose inhaler is not an effective medication for an acute asthma exacerbation. Cromolyn is a mast cell stabilizer that helps to prevent the release of inflammatory mediators that cause asthma symptoms. It is taken daily as a preventive therapy and does not work quickly enough to relieve the symptoms of an acute asthma exacerbation.
Choice C reason: Albuterol via jet nebulizer is a recommended medication for an acute asthma exacerbation. Albuterol is a short acting beta 2 agonist that helps to relax the smooth muscles of the airways and improve breathing. It is taken as needed as a rescue therapy and works quickly to relieve the symptoms of an acute asthma exacerbation.
Choice D reason: Montelukast orally is not a preferred medication for an acute asthma exacerbation. Montelukast is a leukotriene modifier that helps to reduce inflammation and prevent asthma attacks and exercise induced bronchoconstriction. It is taken once a day as an adjunctive therapy and does not work quickly enough to relieve the symptoms of an acute asthma exacerbation.
nurse is caring for a client who has an acute respiratory failure (ARF). The nurse should monitor the client for which of the following manifestations of this condition? (Select all that apply.)
Explanation
Choice A reason: Hypotension is not a common manifestation of ARF. Hypotension is a low blood pressure, defined as less than 90/60 mm Hg. Hypotension can have many causes, such as dehydration, blood loss, heart problems, or medications. ARF does not directly cause hypotension, but it can lead to complications such as shock or organ failure, which can lower the blood pressure.
Choice B reason: Decreased level of consciousness is a frequent manifestation of ARF. Decreased level of consciousness is a state of impaired awareness, orientation, memory, or judgment. Decreased level of consciousness can occur in ARF due to several factors, such as hypoxia, hypercapnia, acidosis, or infection. The nurse should monitor the mental status of the client with ARF and report any changes to the provider.
Choice C reason: Severe dyspnea is a common manifestation of ARF. Dyspnea is a subjective sensation of difficulty breathing or shortness of breath. Severe dyspnea can occur in ARF due to the reduced oxygen delivery or increased carbon dioxide retention in the blood. The nurse should assess the respiratory rate, rhythm, depth, and effort of the client with ARF and provide oxygen therapy as prescribed.
Choice D reason: Headache is not a typical manifestation of ARF. Headache is a pain or discomfort in the head, scalp, or neck. Headache can have many causes, such as stress, dehydration, sinusitis, or migraine. ARF does not directly cause headache, but it can cause increased intracranial pressure or cerebral edema, which can trigger headache.
Choice E reason: Nausea is not a usual manifestation of ARF. Nausea is a feeling of sickness or discomfort in the stomach that can lead to vomiting. Nausea can have many causes, such as food poisoning, motion sickness, pregnancy, or medications. ARF does not directly cause nausea, but it can cause gastrointestinal bleeding or hepatic encephalopathy, which can induce nausea.
A nurse is caring for a client who has right sided acoustic neuroma resulting in impairment of cranial nerves IX and X. Which of the following actions should the nurse take?
Explanation
Choice A reason: Placing suction equipment at the client’s bedside is a necessary action for the nurse to take for a client who has right sided acoustic neuroma resulting in impairment of cranial nerves IX and X. Acoustic neuroma is a noncancerous tumor that develops on the vestibulocochlear nerve, which is responsible for hearing and balance. It can also affect the adjacent cranial nerves, such as the glossopharyngeal (CN IX) and the vagus (CN X) nerves, which are involved in swallowing and gagging. A client with acoustic neuroma may have difficulty swallowing and clearing secretions, which can increase the risk of aspiration and respiratory infections. The nurse should have suction equipment ready to remove any excess saliva or mucus from the client’s mouth or throat.
Choice B reason: Avoiding the use of warm water to wash the client’s face is not a relevant action for the nurse to take for a client who has right sided acoustic neuroma resulting in impairment of cranial nerves IX and X. The temperature of the water does not affect the function of these nerves or the tumor. The nurse should use gentle and appropriate hygiene measures to clean the client’s face and prevent skin breakdown.
Choice C reason: Providing range of motion exercises to the client’s neck and shoulders is not a priority action for the nurse to take for a client who has right sided acoustic neuroma resulting in impairment of cranial nerves IX and X. Range of motion exercises can help to maintain joint mobility and prevent stiffness, but they are not directly related to the cranial nerve impairment or the tumor. The nurse should consult with a physical therapist to determine the best exercise regimen for the client.
Choice D reason: Applying an eye patch to the client’s right eye is not a helpful action for the nurse to take for a client who has right sided acoustic neuroma resulting in impairment of cranial nerves IX and X. An eye patch is used to protect the eye from injury or infection, or to treat conditions such as strabismus or amblyopia. An eye patch does not affect the function of the cranial nerves IX and X or the tumor. The nurse should monitor the client’s eye movements and vision, as acoustic neuroma can also affect the facial (CN VII) and oculomotor (CN III) nerves, which are involved in blinking and eye movement.
Sign Up or Login to view all the 51 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
