Ati pn adult medical surgical 2023 74
Total Questions : 72
Showing 25 questions, Sign in for moreA nurse is reinforcing discharge instructions for a client who experienced a cerebrovascular accident (CVA) and needs help with their activities of daily living (ADLs). What statements should the nurse offer?
Explanation
Choice A reason:
Installing grab bars in the shower is a recommended safety measure for individuals who have experienced a CVA. Grab bars provide stability and support, which can help prevent falls in the slippery environment of a shower. They are particularly useful for those who have balance issues or weakness on one side of the body, common after a stroke. The installation of grab bars is a modification that can significantly improve safety during the performance of ADLs.
Choice B reason:
While placing a towel in the shower may offer some slip resistance, it is not considered a safe or reliable method for preventing falls. Towels can move or bunch up, potentially creating a tripping hazard. Therefore, this is not the best recommendation for a client post-CVA who requires assistance with ADLs and may have balance concerns.
Choice C reason:
While hiring a home care aide can provide assistance with ADLs, it is not the only option and may not be feasible for all clients due to financial constraints or personal preferences. Additionally, the goal of post-CVA rehabilitation is often to maximize independence, and clients are encouraged to perform as many ADLs as possible with appropriate adaptations and safety measures in place.
Choice D reason:
The statement "You will not become fatigued when you use assistive devices" is misleading. While assistive devices are designed to aid in the performance of ADLs and can help reduce fatigue, they do not eliminate it entirely. Individuals post-CVA may still experience fatigue due to the extra effort required to perform tasks, even with the use of assistive devices.
A nurse is providing additional teaching about foods high in potassium to a client. Which of the following foods should the nurse suggest?
Explanation
Choice A reason:
Cabbage is a leafy green vegetable that is beneficial for overall health due to its vitamin content and fiber. However, when it comes to potassium, a cup of sliced cabbage contains approximately 151 mg, which is not particularly high. Potassium is an essential nutrient that plays a key role in cell function, including nerve transmission and muscle contraction. The recommended daily intake of potassium for adults is 2,600 to 3,400 mg. Therefore, while cabbage is healthy, it is not the best option for someone looking to significantly increase their potassium intake.
Choice B reason:
Apples are a popular fruit known for their fiber and vitamin C content. A small apple contains about 159 mg of potassium. Similar to cabbage, apples are not among the highest sources of potassium. They can be part of a balanced diet but are not the optimal choice for those who need a higher intake of this mineral.
Choice C reason:
Watermelon is a hydrating fruit with a high water content and is a good source of vitamins A and C. One cup of sliced watermelon provides roughly 170 mg of potassium. While watermelon does contribute to potassium intake, it does not contain as much potassium as other fruits and vegetables. It is best enjoyed as a refreshing snack rather than a primary source of potassium.
Choice D reason:
Potatoes are a starchy vegetable with a significant amount of potassium. A medium potato can contain up to 897 mg of potassium, making it one of the best choices for increasing potassium intake. Potatoes are versatile and can be prepared in various ways, which makes them an easy addition to many meals. Given their high potassium content, they are an excellent recommendation for someone needing to boost their intake of this mineral.
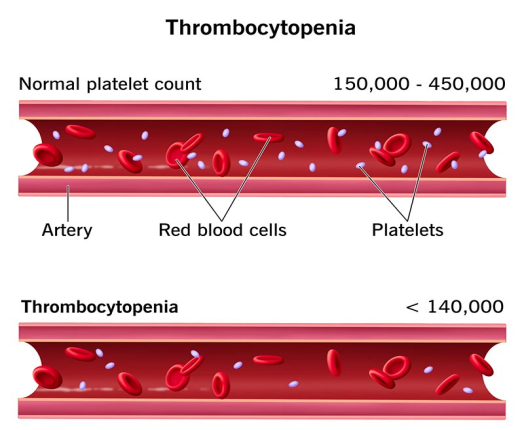
A nurse is helping to develop a care plan for a client with thrombocytopenia. Which of the following actions should the nurse incorporate into the plan?
Explanation
Choice A reason:
Checking for ecchymosis, which are large bruise-like lesions caused by bleeding under the skin, is an important part of care for patients with thrombocytopenia. Thrombocytopenia, a condition characterized by a low platelet count, can lead to increased bleeding and bruising. Ecchymosis can indicate bleeding complications, which are a risk in thrombocytopenia due to the reduced ability of the blood to clot properly.
Choice B reason:
Administering ibuprofen for a mild headache is not recommended for patients with thrombocytopenia. Ibuprofen is a nonsteroidal anti-inflammatory drug (NSAID) that can inhibit platelet function and increase the risk of bleeding. For patients with thrombocytopenia, it is important to avoid medications that can exacerbate bleeding risks.
Choice C reason:
Instructing a client with thrombocytopenia to shave with a disposable razor is not advisable. The use of sharp blades can lead to cuts and bleeding, which is a concern for patients with a low platelet count. Instead, electric shavers, which reduce the risk of nicks and cuts, are recommended for these patients.
Choice D reason:
Initiating protective isolation for a client with thrombocytopenia is not typically necessary unless the patient has neutropenia or is immunocompromised in addition to thrombocytopenia. Protective isolation is used to protect patients from infections when their immune system is weakened, which is not directly related to thrombocytopenia unless there are additional risk factors present.
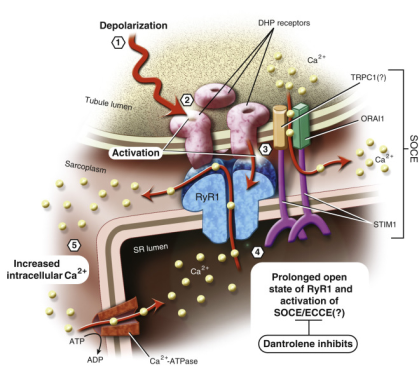
A nurse is assisting in the care of a postoperative client who has developed malignant hyperthermia. Which of the following actions should the nurse perform?
Explanation
Choice A reason:
Applying a cooling blanket is a critical intervention for a patient with malignant hyperthermia, a life-threatening condition characterized by a rapid rise in body temperature and severe muscle contractions following exposure to certain anesthetic agents. The cooling blanket helps to reduce the patient's body temperature, which can prevent further complications associated with hyperthermia.
Choice B reason:
Instilling a warm enema solution is not an appropriate action for malignant hyperthermia. This condition requires measures to reduce body temperature, not increase it. A warm enema could potentially worsen the hyperthermic state.
Choice C reason:
Administering meperidine (an opioid analgesic) intramuscularly is not recommended in the management of malignant hyperthermia. Meperidine does not play a role in the treatment of this condition and could complicate the clinical picture due to its pharmacological effects.
Choice D reason:
Ventilating the client with 50% oxygen is part of the supportive care for malignant hyperthermia, but it is not the primary intervention. The main goal is to treat the hypermetabolic state and reduce body temperature. While oxygenation is important, it should be accompanied by other specific treatments for malignant hyperthermia, such as administering dantrolene and active cooling measures.
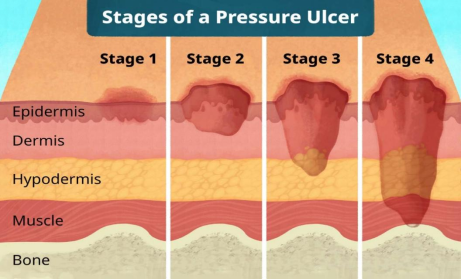
A nurse is getting ready to perform a sterile dressing change for a client with a stage III pressure ulcer. Which of the following actions should the nurse plan to carry out?
Explanation
Choice A reason:
Donning sterile gloves before removing the old dressing is not the recommended practice. The nurse should first remove the old dressing with non-sterile gloves to prevent contamination of the sterile field and then don sterile gloves to handle the new dressing.
Choice B reason:
Offering pain medication before the procedure is a crucial step in the care of a client with a pressure ulcer. Dressing changes can be painful, and preemptive pain management is essential to ensure the comfort of the client during the procedure.
Choice C reason:
Preparing sterile dressing supplies 30 minutes before the dressing change is not necessary and could potentially compromise the sterility of the supplies. Sterile supplies should be prepared immediately before the dressing change to maintain a sterile environment.
Choice D reason:
Disinfecting the wound bed with alcohol is not recommended for pressure ulcers. Alcohol can be cytotoxic and can damage the granulation tissue. Instead, a normal saline solution should be used to clean the wound bed.
A home health nurse is providing additional teaching to an older adult client about home safety precautions. Which of the following instructions should the nurse include?
Explanation
Choice A reason:
Running wires and cords under carpeting is not recommended as it poses a tripping hazard and can also lead to wear on the cords, which could cause electrical fires. It's important to keep cords and wires secured and out of walkways to prevent falls, which are a leading cause of injury among older adults.
Choice B reason:
Placing white tape on the edges of stairs is a safety measure that can help prevent falls by increasing the visibility of each step. This is particularly useful for older adults who may have vision impairments. Enhanced visibility of stair edges can significantly reduce the risk of missteps and falls.
Choice C reason:
While having the furnace inspected regularly is important for maintaining a safe home environment, doing so every 2 years may not be sufficient. It is generally recommended to have heating systems inspected annually to ensure they are functioning properly and to prevent carbon monoxide poisoning.
Choice D reason:
Placing area rugs on wooden floors can create a tripping hazard, especially if the rugs do not have a non-slip backing. It's better to secure rugs with double-sided tape or slip-resistant backings, or to avoid them altogether in high-traffic areas to maintain a safe walking surface.
A nurse in an assisted living facility is gathering information from an older adult client who fell in their room and struck their head on the dresser. Which of the following findings should be the nurse's priority?
Explanation
Choice A reason:
While memory lapses, such as being unable to remember their adult children's names, can be concerning, they are not the immediate priority following a head injury. Memory issues may result from various factors, including the emotional shock of the fall or pre-existing cognitive conditions.
Choice B reason:
The inability to remain fully awake, or altered levels of consciousness, is a critical sign that may indicate a serious brain injury, such as a concussion or hemorrhage. This finding requires urgent attention to prevent further complications, making it the nurse's priority.
Choice C reason:
Difficulty in repeating the names of three common objects could suggest cognitive impairment or confusion, which are concerning but secondary to consciousness and alertness issues. Cognitive assessments are part of a broader neurological evaluation following a head injury.
Choice D reason:
Incorrectly answering a judgment question is part of a cognitive assessment and, while important, does not take precedence over signs that may indicate a life-threatening condition, such as changes in consciousness.
A nurse on the night shift is caring for an older adult client with dementia who is at risk for falls. Which of the following actions should the nurse take?
Explanation
Choice A reason:
Moving the overbed table away from the bed may reduce clutter and potential obstacles, which is generally a good practice in fall prevention. However, it does not directly address the immediate risk of the client falling out of bed. The overbed table, if positioned correctly, can also be used to hold personal items within easy reach of the client, reducing the need for them to stretch or reach out, which could potentially lead to a fall.
Choice B reason:
Leaving the television on in the client's room might provide a sense of comfort or distraction, but it does not contribute to fall prevention. In fact, the noise and light from the television could potentially disrupt the client's sleep pattern, leading to disorientation or restlessness, which can increase the risk of falls, especially in clients with dementia.
Choice C reason:
Applying a motion sensor mat to the client's bed is a proactive measure to prevent falls. If the client attempts to get out of bed, the sensor will trigger an alarm, alerting the nursing staff to assist the client. This intervention is particularly useful for clients with dementia who may not remember to call for assistance when getting up, thus reducing the risk of falls.
Choice D reason:
Raising all four side rails while the client is in bed may seem like a protective measure, but it can actually increase the risk of injury. Clients with dementia may become confused and attempt to climb over the rails, leading to a higher fall and potential injury. Moreover, the use of full side rails can be considered a form of restraint, which is generally discouraged in patient care unless absolutely necessary.
A nurse is helping to develop a care plan for an older adult client who has a new prescription for transdermal clonidine. Which of the following details should the nurse incorporate into the plan of care?
Explanation
Choice A reason:
Monitoring the client for weight loss is not typically associated with transdermal clonidine. Clonidine is an antihypertensive medication and does not have weight loss as a common side effect. Instead, the nurse should monitor blood pressure and heart rate, as clonidine can affect these parameters.
Choice B reason:
Diarrhea is not a common adverse effect of transdermal clonidine. The more frequent gastrointestinal side effect associated with clonidine is constipation, not diarrhea. Therefore, informing the client about diarrhea as an adverse effect would not be accurate.
Choice C reason:
Hypopigmentation under the patch is not a recognized side effect of transdermal clonidine. While skin reactions can occur, they are more likely to be irritation or contact dermatitis at the site of the patch application. Checking for hypopigmentation would not be a standard part of care for a client using a clonidine patch.
Choice D reason:
Dry mouth is a well-documented side effect of clonidine, including its transdermal form. The medication can reduce saliva production, leading to an uncomfortable dryness in the mouth. Advising the client about the possibility of increased dry mouth and ways to manage it, such as chewing sugar-free gum or sipping water, is an important part of patient education and care planning.
A nurse is providing additional teaching to a client about breast self-examinations. Which of the following client statements shows an understanding of the instruction?
Explanation
Choice A reason:
While it is true that it's common for one breast to be larger than the other, this statement does not indicate an understanding of the teaching about breast self-examinations. Breast asymmetry is a normal variation and not specifically related to the technique or timing of breast self-exams.
Choice B reason:
The statement that it's common for the skin on the breasts to dimple is not accurate and does not reflect an understanding of breast self-examination. Dimpling of the skin can be a sign of breast cancer, as it may indicate underlying tissue changes. It's important for individuals to report any new dimpling to their healthcare provider.
Choice C reason:
The statement "I will perform breast exams the day after my period begins" shows an understanding of the optimal timing for breast self-examinations. Performing the exam a few days after the menstrual period ends is recommended because breasts are less likely to be swollen and tender, making it easier to feel for any unusual lumps or changes.
Choice D reason:
Performing breast exams every other month does not align with the recommended frequency for breast self-examinations. It is advised that adult women of all ages perform breast self-exams at least once a month to become familiar with the normal look and feel of their breasts and to notice any changes promptly.
A nurse is caring for a client who is postoperative after a right radical mastectomy. Which of the following actions should the nurse take to prevent lymphedema?
Explanation
Choice A reason:
Using the client's left arm to obtain blood samples is the correct action to prevent lymphedema after a right radical mastectomy. Lymphedema can occur when the lymphatic drainage is disrupted, which is a risk after mastectomy involving lymph node removal. To reduce this risk, it is recommended to avoid procedures such as blood draws and blood pressure measurements on the affected side.
Choice B reason:
Obtaining blood pressure readings using the client's right arm, the side of the mastectomy, is not recommended. This action can increase the risk of lymphedema due to the pressure applied during the measurement, which can impede lymphatic flow and contribute to fluid accumulation.
Choice C reason:
Keeping both arms below the level of the client's heart is not specifically related to the prevention of lymphedema. While elevation of the affected arm can help promote lymphatic drainage and reduce swelling, there is no recommendation to keep both arms below heart level as a standard practice.
Choice D reason:
Limiting range-of-motion exercises with the affected arm is not advised as a means to prevent lymphedema. In fact, gentle range-of-motion exercises are encouraged postoperatively to prevent stiffness and improve mobility. However, these exercises should be performed carefully and gradually to avoid overexertion, which could lead to lymphedema.
A nurse is gathering information from an older adult client. Which of the following findings should alert the nurse that the client may have a bladder infection?
Explanation
Choice A reason:
A white blood cell (WBC) count of 9,000/mm³ falls within the normal range of 5,000 to 10,000/mm³ and does not necessarily indicate a bladder infection. The WBC count can be elevated in infections, but a value within the normal range, especially without other symptoms, is not a reliable indicator of a urinary tract infection (UTI).
Choice B reason:
Diminished reflexes are not typically associated with a bladder infection. They can be a sign of neurological issues or other systemic conditions. Reflex changes would more likely prompt an evaluation for neurological disorders rather than a UTI.
Choice C reason:
Changed mental status in older adults can be a sign of a bladder infection. Unlike younger individuals, older adults may not exhibit the classic symptoms of a UTI, such as pain or burning during urination. Instead, they may present with non-specific symptoms like acute confusion or altered mental status, which can be a result of the infection's systemic impact.
Choice D reason:
A temperature of 37.3°C (99.1°F) is slightly elevated but is not considered a fever and could be influenced by various factors. While it could be associated with an infection, it is not a definitive sign of a bladder infection without the presence of other symptoms.
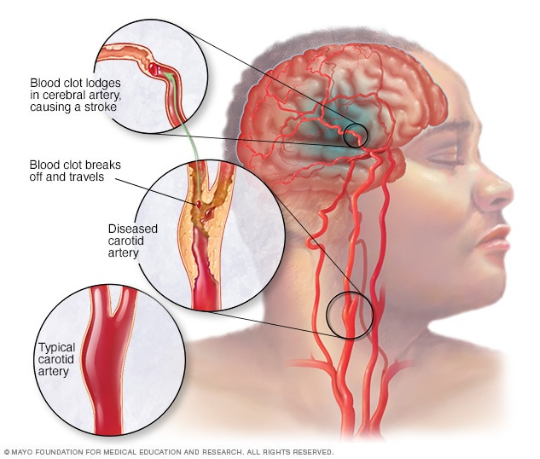
A nurse is providing additional teaching to a client with diabetes mellitus about lowering the risk of stroke. Which of the following client statements demonstrates an understanding of the teaching?
Explanation
Choice A reason:
Having a total cholesterol level below 200 mg/dL is actually considered desirable and does not increase the risk for a stroke. It is when the cholesterol level is high that the risk for atherosclerosis (plaque buildup in arteries) and consequently, stroke, increases. The American Heart Association recommends that total cholesterol levels should be less than 200 mg/dL to reduce the risk of heart disease and stroke.
Choice B reason:
Glucocorticoids are not typically prescribed to decrease the risk of stroke in patients with diabetes mellitus. In fact, glucocorticoids can increase blood glucose levels and potentially worsen diabetes control, which could indirectly increase the risk of stroke. Stroke prevention in diabetes focuses on controlling blood glucose, blood pressure, and cholesterol levels, as well as lifestyle modifications such as diet and exercise.
Choice C reason:
Losing excess weight is a recognized strategy for reducing the risk of stroke, especially in individuals with diabetes mellitus. Excess weight can contribute to high blood pressure, increased cholesterol levels, and poor blood glucose control, all of which are risk factors for stroke. Weight loss can improve these parameters and thus reduce the risk.
Choice D reason:
An HbA1c level of 6 percent or less is typically a goal in diabetes management to indicate good blood glucose control and does not increase the risk for a stroke. On the contrary, maintaining an HbA1c level within the target range helps reduce the risk of diabetes-related complications, including stroke.
A nurse is helping to develop a care plan for a client who has an infectious wound with foul-smelling drainage. Which of the following actions should the nurse incorporate into the plan of care?
Explanation
Choice A reason:
Discarding soiled wound care supplies in a trash receptacle outside the client's room is a necessary action to prevent the spread of infection within the healthcare facility. It is important to ensure that these materials are disposed of properly to maintain a clean environment and reduce the risk of contaminating other areas.
Choice B reason:
Instructing visitors to perform hand hygiene is crucial in preventing the spread of infection. However, the CDC recommends washing hands for at least 20 seconds to effectively remove germs, not just 5 seconds. Proper hand hygiene practices are essential in a healthcare setting, especially when dealing with infectious wounds.
Choice C reason:
Administering antibiotic therapy before culturing the client's wound is not the recommended practice. Culturing should be done prior to the administration of antibiotics to accurately identify the causative organisms and determine the most effective antibiotic treatment.
Choice D reason:
Placing the client in a private room with a private bathroom is the most appropriate action listed. It helps to isolate the client and prevent the spread of infection to other patients. This measure is in line with infection control protocols and provides a controlled environment for the client's care.
A nurse is providing additional teaching to the partner of a client who is under contact precautions for methicillin-resistant Staphylococcus aureus (MRSA). Which of the following statements by the client's partner demonstrates an understanding of the teaching?
Explanation
Choice A reason:
Reusing gloves, even if they appear unsoiled, is not recommended in healthcare settings. This practice can lead to cross-contamination and compromise both healthcare worker and patient safety. Gloves are designed to be disposable and should be discarded after each use to prevent the spread of pathogens like MRSA.
Choice B reason:
Wearing a gown during patient care activities that might involve contact with the patient or their immediate environment is a standard precautionary measure. This is especially important when dealing with MRSA, which can be transmitted through direct contact. The gown acts as a barrier and helps prevent the spread of infection.
Choice C reason:
Patients with MRSA should have limited movement outside their room to prevent the spread of MRSA to other areas and individuals. While wearing a mask may provide some protection, it does not eliminate the risk of transmission through contact with surfaces or other people.
Choice D reason:
Hand hygiene is crucial in preventing the spread of infections, including MRSA. Washing hands immediately after leaving the room of a patient with MRSA is an essential practice; however, it does not indicate an understanding of all necessary precautions within the room itself.
A nurse on the oncology unit is assessing a client's response after administering a dose of aprepitant. Which of the following therapeutic effects should the nurse anticipate?
Explanation
Choice A Reason:
Decreased dysrhythmias are not a therapeutic effect associated with aprepitant. Aprepitant is a neurokinin-1 (NK1) receptor antagonist used primarily to prevent chemotherapy-induced nausea and vomiting (CINV). It does not have a direct effect on cardiac rhythms.
Choice B Reason:
Absence of dizziness is not a specific therapeutic effect of aprepitant. While preventing dizziness can be a secondary benefit of controlling nausea and vomiting, aprepitant's primary function is not to treat dizziness but to block the action of substance P/neurokinin 1 (NK1) in the brain, which can cause vomiting.
Choice C Reason:
Decreased incisional pain is not a therapeutic effect of aprepitant. Aprepitant does not have analgesic properties and is not indicated for pain management. Its role is in the prevention of nausea and vomiting through its action as an NK1 receptor antagonist.
Choice D Reason:
Absence of nausea is the expected therapeutic effect of aprepitant. Aprepitant works by inhibiting the substance P/neurokinin 1 (NK1) receptor, which plays a significant role in the emetic process. By blocking this receptor, aprepitant augments the antiemetic activity of other agents like 5-HT3 receptor antagonists and corticosteroids to prevent acute and delayed phases of CINV.
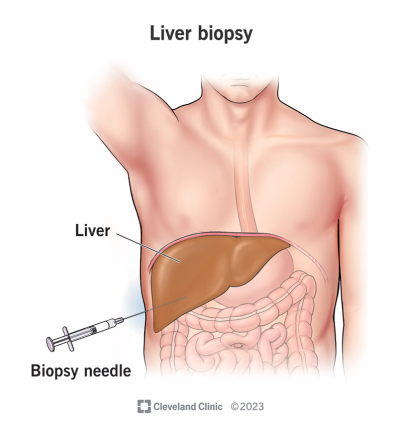
A nurse is examining the lab data of a client who is scheduled for a liver biopsy. Which of the following values should the nurse report to the provider?
Explanation
Choice A Reason:
The ammonia level of 55 mcg/dL falls within the normal range of 10 to 80 mcg/dL. Ammonia is a byproduct of protein metabolism and is converted to urea by the liver before being excreted by the kidneys. Elevated levels can indicate liver dysfunction, but in this case, the value does not warrant concern.
Choice B Reason:
A bilirubin level of 1.0 mg/dL is at the upper limit of the normal range, which is 0.3 to 1.0 mg/dL. Bilirubin is produced during the normal breakdown of red blood cells and is processed by the liver. While this value is at the higher end, it is not abnormal and does not require reporting to the provider unless there are symptoms of jaundice or other clinical signs of liver disease.
Choice C Reason:
The platelet count of 60,000/mm³ is significantly below the normal range of 150,000 to 450,000/mm³. Platelets are crucial for blood clotting, and a low count, known as thrombocytopenia, can increase the risk of bleeding, especially concerning in the context of an invasive procedure like a liver biopsy. This value should be reported to the provider as it may necessitate a change in the biopsy plan or require intervention to address the low platelet count.
Choice D Reason:
An AST level of 34 units/L is at the upper boundary of the normal range. AST is an enzyme found in high amounts in the liver, heart, and muscles, and it is released into the bloodstream when any of these tissues are damaged. While this value is at the upper limit, it is not elevated and typically would not need to be reported unless there are other indicators of liver injury or the patient is symptomatic.
A nurse is helping to develop a care plan for a client with viral meningitis. Which of the following interventions should the nurse suggest?
Explanation
Choice A Reason:
Initiating contact precautions for a client with viral meningitis is not typically necessary. Viral meningitis is less contagious than bacterial meningitis and is usually spread through fecal contamination or respiratory secretions. Standard precautions are generally sufficient unless there is a specific outbreak or the patient has enterovirus meningitis.
Choice B Reason:
Monitoring the client's temperature every 6 hours is important for detecting fever, which can be a sign of worsening infection or an adverse reaction to medication. However, this is a standard nursing intervention for many conditions and not specific to the care of a client with viral meningitis.
Choice C Reason:
Measuring the client's intake and output every 8 hours is a standard practice for monitoring fluid balance, especially in clients who may be at risk of cerebral edema or dehydration. While important, it is not the most specific intervention for viral meningitis care.
Choice D Reason:
Dimming the lighting in the client's room is a specific intervention for viral meningitis care. Clients with meningitis often experience photophobia, or sensitivity to light, which can exacerbate headaches and other discomforts. Providing a dimly lit or dark room can help alleviate this symptom and is a recommended practice.
A nurse is gathering admission history data from a client in a semi-private room. Which of the following information is the nurse's priority to address?
Explanation
Choice A Reason:
Nocturia, or frequent urination during the night, can be a symptom of various conditions, including urinary tract infections, diabetes, or high fluid intake before bed. While it can affect the client's sleep and quality of life, it is not typically considered an immediate priority unless it is indicative of a more serious underlying condition.
Choice B Reason:
A history of generalized anxiety disorder is important to consider for a client's overall mental health and well-being. It may affect how the client copes with hospitalization and can influence the plan of care. However, it is not usually an immediate priority upon admission unless the client is currently experiencing severe anxiety or panic attacks.
Choice C Reason:
Recent exposure to tuberculosis (TB) is a critical piece of information that must be addressed promptly. TB is a highly contagious bacterial infection that can spread quickly in a semi-private room or hospital setting. The nurse must report this to the healthcare provider and infection control team to initiate appropriate isolation precautions and testing.
Choice D Reason:
While periodic migraine headaches can significantly impact a client's comfort and ability to participate in care, they are not typically a priority for immediate action upon admission unless the client is currently experiencing a migraine.
A nurse is caring for a client with dysphagia after a stroke. When assisting the client during mealtime, which of the following actions should the nurse plan to implement?
Explanation
Choice A reason:
Providing oral care before meals is crucial for a client with dysphagia after a stroke. Oral care can help clear the mouth of bacteria and food debris, reducing the risk of aspiration and improving the client's ability to taste and swallow food. According to the American Stroke Association, maintaining good oral hygiene is part of managing dysphagia to prevent complications like pneumonia.
Choice B reason:
Instructing the client to tilt their head back to facilitate swallowing is not recommended for individuals with dysphagia following a stroke. This position can increase the risk of aspiration, as it may allow food or liquid to enter the airway. Instead, the client should be encouraged to maintain an upright position, and in some cases, to tuck the chin slightly to protect the airway during swallowing.
Choice C reason:
Encouraging the use of a straw is generally not advised for clients with dysphagia. Using a straw can increase the speed at which liquid enters the mouth, which can be difficult to control and may lead to aspiration. The American Speech-Language-Hearing Association suggests that taking small sips and bites and avoiding straws can help manage dysphagia more safely.
Choice D reason:
Scheduling physical therapy directly before meals is not ideal for clients with dysphagia. Physical therapy can be fatiguing, and fatigue may worsen the client's ability to control the muscles needed for safe swallowing. It's better to schedule therapy sessions at a time when the client is well-rested and alert, ensuring they have the energy and focus required for safe eating practice
A nurse is providing additional teaching to a client who was admitted due to a COPD exacerbation. Which of the following information should the nurse include in the teaching?
Explanation
Choice A reason:
Increasing oxygen to 5 liters per minute if experiencing shortness of breath is not a standard recommendation for all COPD patients. Oxygen therapy must be tailored to each individual's needs, and excessive oxygen can be harmful, leading to CO2 retention and respiratory depression. The goal is to maintain oxygen saturation at 88-92%.
Choice B reason:
Discontinuing prednisone abruptly can lead to adrenal insufficiency, as the body needs time to resume natural cortisol production. Prednisone should be tapered off under medical supervision, especially for COPD patients who may be on long-term corticosteroids for their condition.
Choice C reason:
Decreasing caloric intake is not generally advised for COPD patients without considering their nutritional status. COPD patients often require more calories due to the increased effort of breathing and the body's higher energy demands during respiratory distress.
Choice D reason:
Consuming small, frequent meals is beneficial for COPD patients. It can help avoid the discomfort of fullness, which can impede the diaphragm's movement and make breathing more difficult. Smaller meals can also ensure better nutrient absorption and maintain energy levels throughout the day.
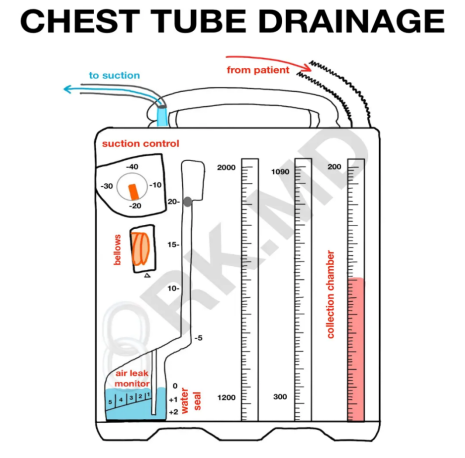
A nurse is helping care for a client with a closed-chest tube drainage system. Which of the following actions should the nurse perform?
Explanation
Choice A reason:
Pinning the tubing to the client's bed sheets is not recommended as it can cause tension on the tube, potentially leading to dislodgement or damage to the tube. The tubing should be secured in a manner that allows some mobility without causing undue stress on the chest tube insertion site.
Choice B reason:
Replacing the unit when the drainage chamber is full is essential to maintain the functionality of the closed-chest tube drainage system. A full drainage chamber can prevent further collection of fluid or air, compromising the system's ability to maintain negative pressure in the pleural space, which is necessary for lung re-expansion.
Choice C reason:
Clamping the tube for 30 minutes every 6 hours is not a standard practice and could be dangerous. Clamping a chest tube without a physician's order or not in preparation for removal can lead to tension pneumothorax, especially if the patient has ongoing air leaks.
Choice D reason:
Monitoring for at least 150 mL of drainage every hour is not a specific action that should be taken. The amount of drainage should be monitored, but there is no standard amount that applies to all patients. Excessive drainage should be reported, as it may indicate hemorrhage or other complications.
A nurse is providing additional teaching to a client with a grade 2 ankle sprain. Which of the following client statements indicates an understanding of the instruction?
Explanation
Choice A reason:
Bearing full weight on an affected ankle with a grade 2 sprain is not advisable. A grade 2 sprain involves partial tearing of the ligament, which requires support and limited movement to heal properly. Bearing full weight too soon can aggravate the injury and delay healing.
Choice B reason:
Wrapping the affected ankle with an elastic bandage is a recommended action for a grade 2 ankle sprain. The compression from the bandage can help reduce swelling and provide support to the injured area, aiding in the healing process. It’s important to wrap the bandage correctly to ensure it’s effective without being too tight, which could impede circulation.
Choice C reason:
Dangling the affected ankle from the edge of the bed is not typically advised immediately following a grade 2 sprain. While gentle movement and exercises are part of the rehabilitation process, they should be done in a controlled manner to avoid further injury. Initially, rest and immobilization are more important to allow the ligaments to heal.
Choice D reason:
Applying heat to a newly sprained ankle is not recommended. Heat can increase circulation and lead to more swelling in the initial injury phase. Instead, ice is usually suggested to reduce swelling and numb the pain. Heat may be used in later stages of healing to promote blood flow and flexibility once the swelling has decreased.
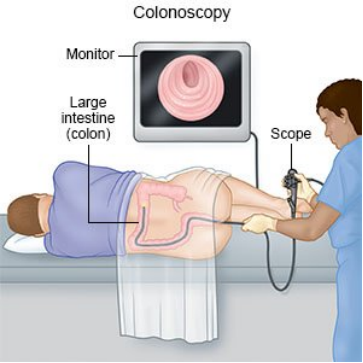
A nurse is providing additional teaching to a client who is scheduled for a colonoscopy the following week. Which of the following instructions should the nurse include?
Explanation
Choice A reason:
Expecting the provider to schedule another procedure to remove any polyps is not a standard pre-procedure instruction. While it's true that polyps may be found and removed during a colonoscopy, the expectation of a separate procedure is not part of the standard preparation instructions. The focus should be on preparing the bowel for clear visualization during the colonoscopy.
Choice B reason:
Advising the client not to eat or drink anything except water for 12 hours before the procedure is partially correct. However, the preparation typically involves more than just fasting; it includes consuming a clear liquid diet and taking a bowel-cleaning laxative as directed by the healthcare provider.
Choice C reason:
Administering enemas 2 days before the procedure is not a typical instruction for colonoscopy preparation. While enemas may be used in some cases, the standard preparation involves a bowel-cleaning laxative to ensure the colon is clear of any stool.
Choice D reason:
Restricting the diet to clear liquids for 1 to 3 days before the procedure is a key part of the preparation for a colonoscopy. This helps to ensure that the bowel is clear so that the physician can have an unobstructed view of the colon during the examination. Clear liquids include water, broth, and other transparent liquids that do not contain solid particles.
A nurse is helping to develop a care plan for a client with thrombocytopenia. Which of the following actions should the nurse include in the plan?
Explanation
Choice A reason:
Checking the client for ecchymosis is an important part of care for patients with thrombocytopenia. Ecchymosis, or bruising, can be a sign of bleeding under the skin and may indicate a drop in platelet count. Since normal platelet counts range from 150,000 to 450,000 platelets per microliter of blood, and thrombocytopenia involves counts lower than this, monitoring for signs of bleeding is crucial.
Choice B reason:
Administering ibuprofen for a mild headache is not recommended for clients with thrombocytopenia. Ibuprofen is a nonsteroidal anti-inflammatory drug (NSAID) that can inhibit platelet function and increase bleeding risk. Instead, acetaminophen may be used for pain relief as it has less effect on platelet function.
Choice C reason:
Instructing the client to shave with a disposable razor is not advisable. Shaving can cause cuts or nicks, which can lead to bleeding. For clients with thrombocytopenia, using an electric razor is safer because it reduces the risk of skin lacerations.
Choice D reason:
Initiating protective isolation for the client with thrombocytopenia is not typically necessary unless the client has an additional condition that warrants it, such as an immunocompromised state. Thrombocytopenia itself does not require isolation; instead, precautions to prevent bleeding are the priority.
Sign Up or Login to view all the 72 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
