ATI RN CARE NURSING OF CHILDREN 2019 UPDATED 2024
Total Questions : 65
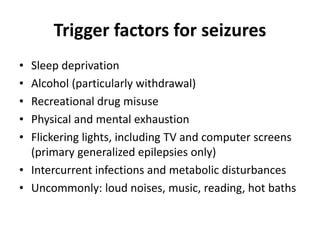
Showing 25 questions, Sign in for moreA nurse is providing teaching to the guardians of a school-age child who has a seizure disorder. Which of the following factors should the nurse include as a common trigger that increases the risk of seizures?
Explanation
Choice AReason:
Exposure to secondhand smoke is incorrect. While exposure to secondhand smoke isn't healthy for anyone, it might not be a primary trigger for seizures in most cases. However, for some individuals, exposure to certain environmental toxins or irritants might exacerbate their condition, though this varies from person to person.
Choice BReason:
Decreased temperature is incorrect. While extreme temperatures (both hot and cold) can potentially trigger seizures in some individuals, decreased temperature alone might not be a common trigger compared to other factors.
Choice C Reason:
Lack of sleep is correct. Sleep deprivation can be a significant trigger for seizures in people with epilepsy or seizure disorders. Maintaining a regular sleep schedule and ensuring adequate sleep is an important aspect of managing seizures in these individuals.
Choice D Reason:
Prolonged headache is incorrect. Headaches can sometimes be a warning sign or an aura before a seizure for some individuals, but having a headache alone might not directly trigger a seizure for most people with a seizure disorder. However, there can be a relationship between headaches and certain types of seizures in specific cases.
A nurse is preparing to initiate IV antibiotic therapy for a newly admitted 12-month-old infant. Which of the following actions should the nurse plan to take?
Explanation
Choice A Reason:
Using a 24-gauge catheter to start the IV might be too small for this age group is correct. Typically, a larger gauge (such as 22-gauge) might be more appropriate for an infant to ensure the flow rate needed for antibiotic administration.
Choice B Reason:
Changing the IV site every 3 days might not be necessary if the site is functioning well and there are no signs of complications. However, regular assessment of the site for signs of infection or infiltration is essential, and the IV site should be changed if any issues arise.
Choice C Reason:
Starting the IV in the infant's foot might be an option, but it's crucial to consider the accessibility and mobility of the foot for the infant. The hand or forearm is often preferred for IV placement in infants due to better immobilization and reduced risk of dislodgement.
Choice D Reason:
Covering the insertion site with an opaque dressing might not be necessary unless there's a specific reason for it. Generally, transparent dressings are used to allow continuous monitoring of the insertion site.

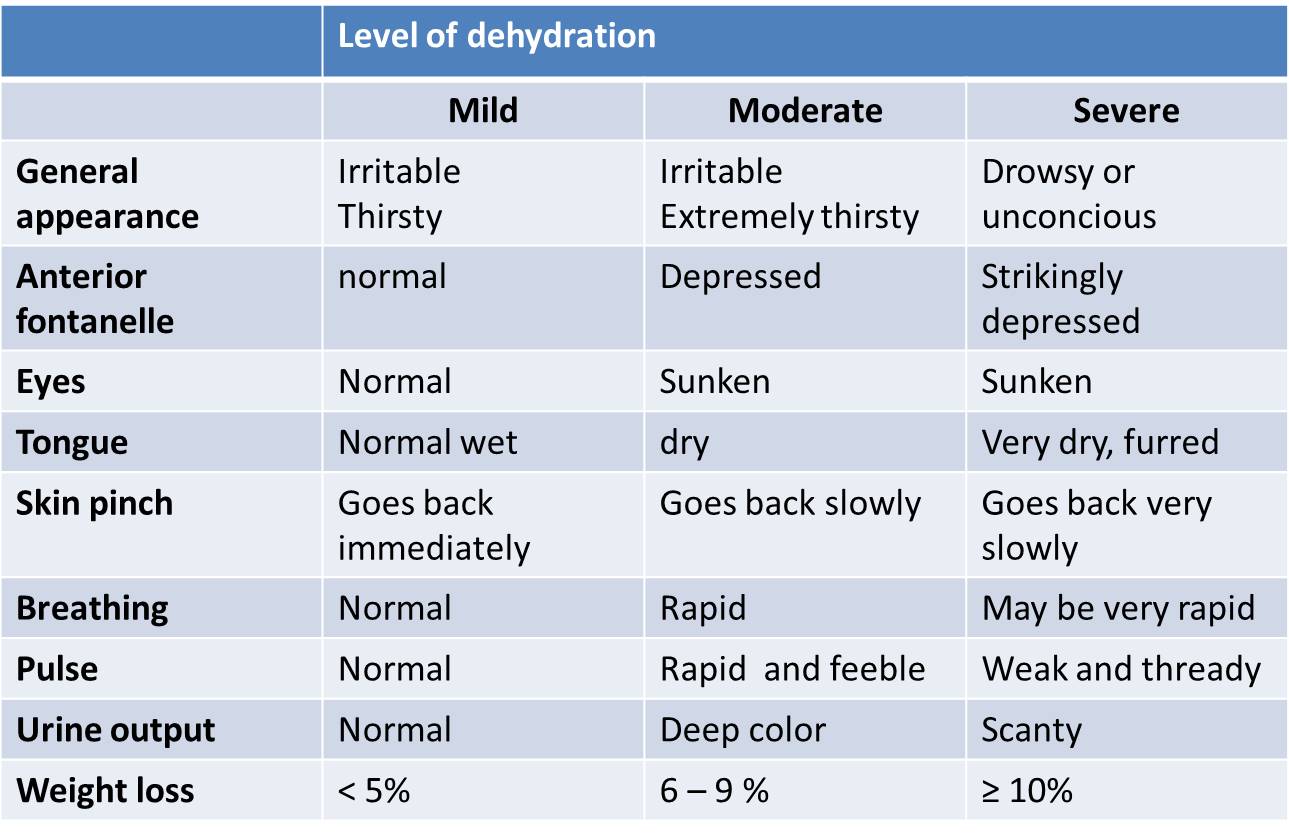
A nurse is caring for an infant who has rotavirus. Which of the following findings indicates that the infant is moderately dehydrated?
Explanation
Choice A Reason:
Capillary refill of 1 second is within the normal range and might not specifically indicate moderate dehydration.
Choice B Reason:
Weight loss 7% is correct. In cases of moderate dehydration, a significant weight loss, typically around 6-9% of body weight, can occur due to fluid loss. This weight loss reflects the severity of dehydration in the infant.
Choice CReason:
A respiratory rate of 28/min might be slightly elevated but is not a primary indicator of moderate dehydration. Dehydration primarily affects cardiovascular and fluid balance systems rather than respiratory rate.
Choice DReason:
Bradycardia (a slow heart rate) is not typically associated with moderate dehydration. Dehydration often causes an increase in heart rate (tachycardia) as the body attempts to maintain cardiac output.
A nurse is caring for an adolescent who is 1 hr. postoperative following an appendectomy. Which of the following findings should the nurse report to the provider?
Explanation
Choice A Reason:
Muscle rigidity is correct. Muscle rigidity can indicate several concerning issues postoperatively, such as complications from anesthesia, infection, or other underlying problems. It's crucial to report this finding promptly to the provider for further evaluation and appropriate management.
Choice BReason:
Some degree of abdominal pain is expected post-appendectomy, but the severity and persistence of the pain should be assessed further.
Choice CReason:
Heart rate of 63/min is within the normal range for some adolescents and might not be an immediate concern unless there are other accompanying symptoms.
Choice D Reason:
A temperature of 36.4°C (97.5°F) falls within the normal range for body temperature and might not be a cause for immediate concern unless it's accompanied by other symptoms or if there are signs of temperature changes (like fever) over time.
A nurse is planning care for an 8-month-old infant who has heart failure. Which of the following actions should the nurse include in the plan of care?
No explanation
A nurse is planning care for an 8-month-old infant who has heart failure. Which of the following actions should the nurse include in the plan of care?
Explanation
Choice A Reason:
Placing the infant in a prone position might not be suitable for an infant with heart failure. Typically, an upright or semi-upright position can help reduce the workload on the heart by improving respiratory function and aiding in cardiac output.
Choice B Reason:
Repeating a digoxin dosage if the infant vomits within 1 hour of administration isn't recommended without consulting a healthcare provider. If vomiting occurs within this time frame, giving another dose might result in overdosing.
Choice C Reason:
Administering cool, humidified oxygen via nasal cannula can be beneficial for an infant with heart failure, as it helps in providing supplemental oxygen and maintaining adequate oxygenation levels.
Choice D Reason:
Providing less frequent, higher volume feedings might not be appropriate for an infant with heart failure. These infants often require smaller, more frequent feedings to prevent overloading the digestive system and to manage fluid intake.
A nurse is caring for a preschooler who is postoperative following a tonsillectomy. The child is now ready to resume oral intake. Which of the following dietary choices should the nurse offer the child?
Explanation
Choice AReason:
Chocolate milk is incorrect. Similar to ice cream, chocolate milk is dairy-based and may have a thicker consistency, potentially causing discomfort or irritation to the throat.
Choice B Reason:
Sugar-free cherry gelatin is correct. Sugar-free gelatin is often recommended post-tonsillectomy as it is cool, soothing, and easy to swallow. It helps in providing hydration and doesn't pose a risk of causing irritation to the surgical site. Additionally, it's important to avoid dairy products and acidic or rough-textured foods that could potentially irritate the throat or disrupt the healing process.
Choice CReason:
Lime-flavored ice pop is incorrect. Citrus flavors, like lime, can be acidic and may cause irritation to the surgical site, leading to discomfort or pain during consumption.
Choice D Reason:
Vanilla ice cream is incorrect. While ice cream might seem soothing, it's dairy-based and can coat the throat, potentially causing discomfort or mucus production, which may not be ideal for the healing process.
A nurse is planning care for an adolescent who has sickle cell anemia. Which of the following immunizations should the nurse include in the plan?
Explanation
Choice AReason:
Measles, mumps, and rubella (MMR) vaccine is important for general immunity, but it might not be specifically emphasized for an adolescent with sickle cell anemia unless they have missed these vaccinations previously.
Choice BReason:
Respiratory syncytial virus (RSV) vaccine is often recommended for infants at high risk for severe RSV infection but may not be a primary concern for an adolescent with sickle cell anemia.
Choice CReason:
Pneumococcal conjugate (PCV13) would be an important immunization to include in the plan for an adolescent with sickle cell anemia. Sickle cell disease increases the risk of infections, particularly with encapsulated bacteria like Streptococcus pneumoniae, which the PCV13 vaccine covers. This immunization helps prevent pneumonia, meningitis, and other invasive pneumococcal diseases.
Choice DReason:
Rotavirus vaccine is typically administered in infancy and might not be relevant for an adolescent population.
A charge nurse is planning care for an infant who has failure to thrive. Which of the following actions should the nurse include in the plan of care?
Explanation
Choice A Reason:
Keeping the infant in a visually stimulating environment might not directly address the nutritional or developmental needs of an infant with failure to thrive. While visual stimulation is essential for infant development, it's not the primary intervention for this condition.
Choice B Reason:
Assigning consistent nursing staff to care for the infant can provide stability and continuity, which can positively impact the infant's emotional well-being. However, this alone might not address the underlying issues related to failure to thrive.
Choice C Reason:
Giving the infant fruit juice between feedings might not be the best approach. Fruit juice can fill an infant's stomach without providing the necessary nutrients, potentially further reducing the intake of essential formula or breast milk.
Choice D Reason:
Using half-strength formula when feeding the infant isn't recommended without specific guidance from a healthcare provider. Diluting formula can compromise the infant's nutritional intake, potentially exacerbating the issue of failure to thrive.
A nurse is teaching the parent of a school-age child about bicycle safety. Which of the following instructions should the nurse include in the teaching?
Explanation
Choice A Reason:
"Your child should ride the bicycle against the flow of traffic." This instruction is incorrect. Children should ride their bicycles in the same direction as traffic flow to reduce the risk of accidents.
Choice B Reason:
While it's a good practice for pedestrians to walk through intersections, it's not specifically tied to bicycle safety. When riding a bicycle through intersections, children should slow down, look both ways, and yield to pedestrians and vehicles as appropriate.
Choice C Reason:
"Your child should keep the bicycle at least 3 feet from the curb while riding in the street." This instruction is a good guideline. Riding a safe distance away from the curb can help avoid obstacles and allow for better maneuverability.
Choice D Reason:
"Your child's feet should be 3 to 6 inches off the ground when seated on the bicycle." This instruction isn't related to safety but rather to the appropriate seat height adjustment for comfortable and efficient cycling. It might not be a primary safety concern.
A nurse is providing discharge teaching to the parents of an infant who is at risk for sudden infant death syndrome (SIDS). Which of the following statements by the parents indicates an understanding of the teaching?
Explanation
Choice A Reason:
Moving the baby's stuffed animal to the corner of the crib might not address the risk factors for SIDS, and loose bedding or soft objects in the sleep environment can increase the risk.
Choice B Reason:
Having the baby sleep next to the parent in bed might increase the risk of accidental suffocation or entrapment, which are factors associated with an increased risk of SIDS.
Choice C Reason:
Placing the baby on their side to sleep for naps is not recommended because the safest sleep position for infants is on their back. Side sleeping can also increase the risk of the baby rolling onto their stomach, which is a higher risk position for SIDS.
Choice D Reason:
"I will dress my baby in lightweight clothing to sleep." Is correct. Sudden Infant Death Syndrome (SIDS) risk reduction strategies include dressing infants in lightweight clothing to prevent overheating, which is considered a risk factor for SIDS. Ensuring the baby is not excessively bundled up or overheated during sleep can help reduce the risk.
A nurse in a PACU is caring for a school-age child immediately following a tonsillectomy. Which of the following actions should the nurse take?
Explanation
Choice A Reason:
Instructing the child to drink fluids through a straw should be avoided immediately after a tonsillectomy. The sucking motion required when using a straw can potentially disrupt the healing process and dislodge the blood clot at the surgical site, leading to bleeding. Therefore, this action is not recommended.
Choice B Reason:
Offering the child ice cream when alert might not be the best choice immediately after a tonsillectomy. Cold foods like ice cream can potentially irritate the surgical site and may not be advised during the immediate postoperative period when throat pain and the risk of bleeding are concerns.
Choice C Reason:
Placing the child in a side-lying position might not be specifically indicated unless directed by the healthcare provider for a specific reason. The child should be placed in a comfortable position that supports airway patency and monitoring but not necessarily in a side-lying position routinely.
Choice D Reason:
Encouraging the child to deep breath and cough is generally a good practice to prevent respiratory complications post-anesthesia. However, immediate post-tonsillectomy, the focus might be more on airway patency and monitoring for signs of bleeding or adverse reactions rather than deep breathing and coughing.
A nurse in a PACU is caring for a school-age child immediately following a tonsillectomy. Which of the following actions should the nurse take?
Explanation
Choice A Reason:
Instructing the child to drink fluids through a straw should be avoided immediately after a tonsillectomy. The sucking motion required when using a straw can potentially disrupt the healing process and dislodge the blood clot at the surgical site, leading to bleeding. Therefore, this action is not recommended.
Choice B Reason:
Offering the child ice cream when alert might not be the best choice immediately after a tonsillectomy. Cold foods like ice cream can potentially irritate the surgical site and may not be advised during the immediate postoperative period when throat pain and the risk of bleeding are concerns.
Choice C Reason:
Placing the child in a side-lying position might not be specifically indicated unless directed by the healthcare provider for a specific reason. The child should be placed in a comfortable position that supports airway patency and monitoring but not necessarily in a side-lying position routinely.
Choice D Reason:
Encouraging the child to deep breath and cough is generally a good practice to prevent respiratory complications post-anesthesia. However, immediate post-tonsillectomy, the focus might be more on airway patency and monitoring for signs of bleeding or adverse reactions rather than deep breathing and coughing.
A nurse in the emergency department is caring for an adolescent who is requesting testing for STIs. Which of the following actions is appropriate for the nurse to take?
Explanation
Choice A Reason:
Obtain written consent from the client is correct. In many jurisdictions, adolescents have the legal right to consent to STI testing and treatment without parental involvement or notification. Healthcare providers must adhere to confidentiality and privacy laws regarding adolescent health, particularly concerning sensitive issues like STI testing and treatment.
Choice B Reason:
Contact the client's parents to obtain phone consent is incorrect. Contacting the client's parents for consent might breach the adolescent's privacy and confidentiality, particularly in cases where they have the legal right to seek STI testing without parental involvement. In many jurisdictions, adolescents have the right to confidential healthcare services related to sexual health.
Choice C Reason:
Postpone the testing until the client's parents are present is incorrect. Delaying the testing until the client's parents are present could potentially compromise the adolescent's health. Confidentiality and timely access to healthcare services are critical, especially in cases concerning sexual health where prompt testing and treatment might be necessary.
Choice D Reason:
Request verbal consent from the social worker. Obtaining consent through a social worker might not follow proper healthcare protocols. Written consent from the adolescent themselves, if legally permissible, is typically required for such medical procedures, ensuring proper documentation and legal compliance.
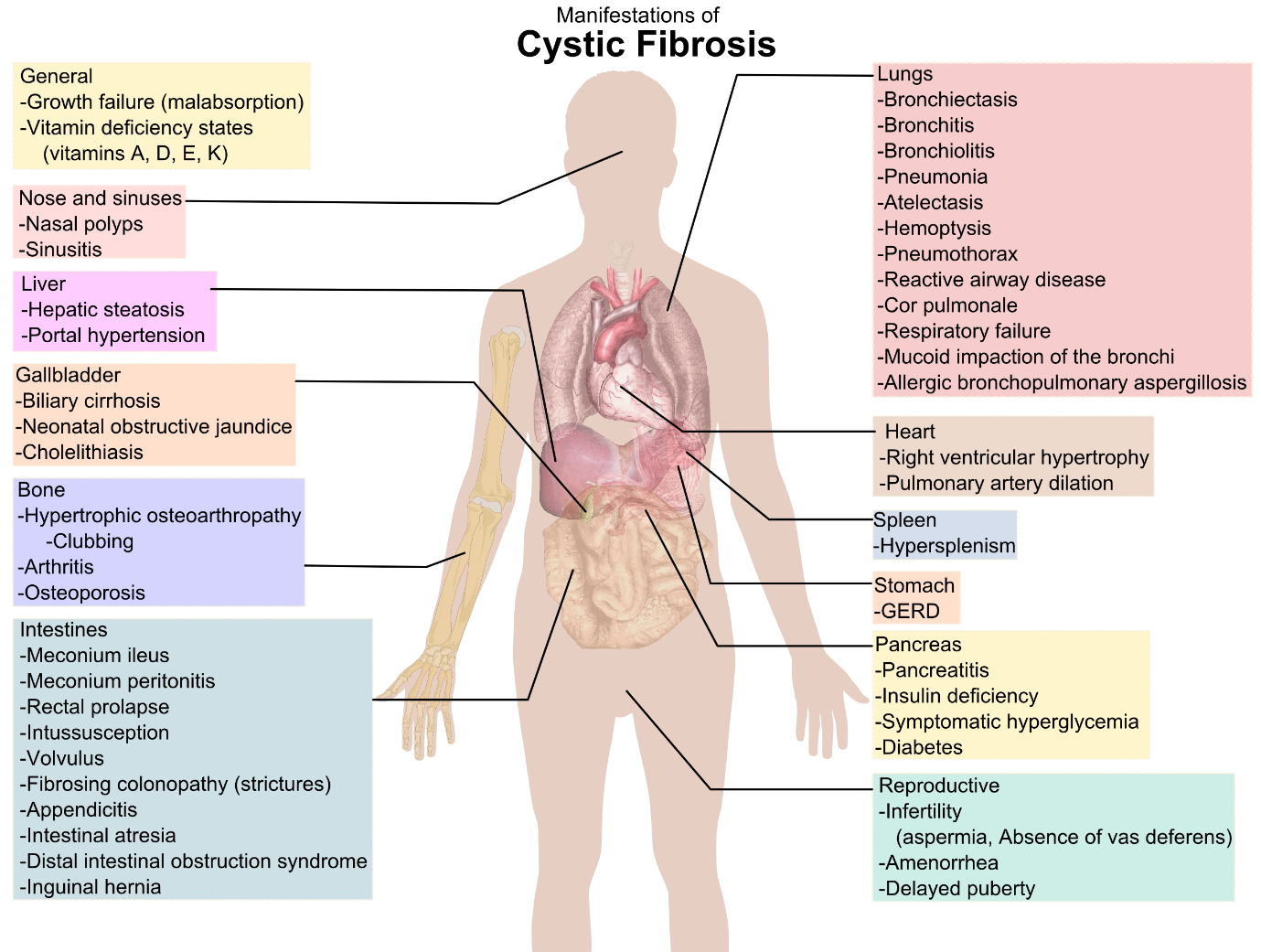
A nurse is assessing a toddler who has cystic fibrosis. Which of the following findings should the nurse expect?
Explanation
Choice A Reason:
Steatorrhea is correct. Cystic fibrosis (CF) can lead to issues with digestion and absorption of nutrients due to problems with pancreatic enzymes. Steatorrhea, which is the passage of foul-smelling, fatty stools, is a common symptom in individuals with CF due to pancreatic insufficiency. It occurs because the body cannot properly digest and absorb fats, resulting in their presence in the stool.
Choice B Reason:
Weight gain is incorrect. Typically, children with CF might have difficulty gaining weight due to malabsorption issues, despite having a good appetite.
Choice C Reason:
Rhinorrhea is incorrect. While respiratory symptoms like chronic cough and recurrent infections are common in CF due to thick mucus production, rhinorrhea (runny nose) might not be a prominent feature directly associated with CF.
Choice D Reason:
Visible peristalsis is incorrect. This refers to the visible movement of the intestines through the abdomen, which is not typically associated with CF. CF primarily affects the respiratory and digestive systems, and visible peristalsis is not a common finding specifically related to CF.
A nurse is assessing a 5-month-old infant. Which of the following findings should the nurse report to the provider?
Explanation
Choice A Reason:
Exhibits head lag when pulled to a sitting position is correct. At 5 months old, infants typically show improvement in head control, and head lag (where the infant's head falls back when pulled to a sitting position) should be diminishing. Persistent head lag might indicate potential developmental concerns or issues with muscle tone that warrant further evaluation by the healthcare provider.
Choice B Reason:
Unable to hold a bottle is incorrect. At 5 months old, some infants might not have developed the ability to hold a bottle independently yet. This skill can vary among infants and might not be a significant concern at this stage.
Choice C Reason:
Unable to roll from back to abdomen is incorrect. Rolling from back to abdomen might not be fully developed in all infants at 5 months old. It's a milestone that some infants achieve later within the 5 to 6-month range, so it might not be an immediate concern unless it persists significantly beyond that range.
Choice D Reason:
Absent grasp reflex is incorrect. By 5 months old, the typical infant's grasp reflex usually starts to diminish as voluntary grasping begins to develop. However, the absence of the grasp reflex might not be an immediate concern unless it's accompanied by other signs of developmental delay or regression.
A nurse is caring for a 10-month-old child who was brought to the emergency department by his parents following a head injury. Which of the following actions should the nurse take first?
Explanation
Choice A Reason:
Assess respiratory status is correct. Ensuring the child's respiratory status is the first priority in any emergency situation. A head injury might result in an altered level of consciousness, which can compromise the child's ability to maintain a patent airway or adequate breathing. Assessing respiratory status involves observing breathing patterns, chest movements, and ensuring airway patency to ensure the child is adequately oxygenated.
Choice B Reason:
Examining the scalp for lacerations is incorrect. While assessing for any lacerations or external signs of head trauma is essential, it's not the primary immediate concern. The focus should be on ensuring the child's respiratory status and stabilizing their condition first.
Choice C Reason:
Checking pupil reactions is incorrect. Assessing pupil reactions is crucial in evaluating neurological function after a head injury. However, assessing respiratory status takes precedence as it is the most critical and immediate concern in any emergency situation.
Choice D Reason:
Inspecting for fluid leaking from the ears is incorrect. Fluid leaking from the ears might indicate a serious head injury, potentially involving the skull base. While this is an important assessment, it doesn't take priority over assessing the child's respiratory status, which is crucial for immediate intervention to ensure adequate oxygenation.
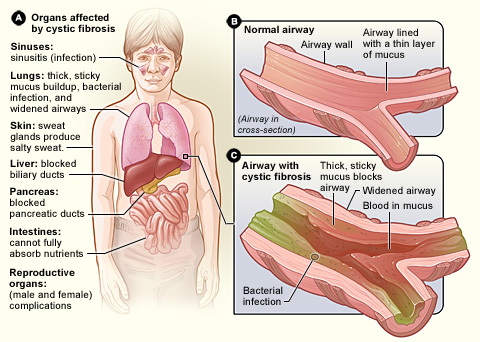
A nurse is providing teaching to the parents of an infant who is to undergo pilocarpine iontophoresis testing for cystic fibrosis. Which of the following statements should the nurse include in the teaching?
Explanation
Choice A Reason:
Inserting an IV is not typically required for this specific test. The test involves applying a substance (pilocarpine) to the skin to stimulate sweat production in a localized area for sweat collection.
Choice B Reason:
Measuring protein in the urine over a 24-hour period is unrelated to the pilocarpine iontophoresis test for cystic fibrosis. Protein measurement in urine over a 24-hour period is a different diagnostic test used for various conditions, but not for cystic fibrosis diagnosis.
Choice C Reason:
Fasting for 8 hours prior to the test is not necessary for the pilocarpine iontophoresis test. There's no requirement for fasting before this particular test.
Choice D Reason:
"The test will measure the amount of chloride in your baby's sweat." Is correct. Pilocarpine iontophoresis testing is a diagnostic test used to measure the concentration of chloride in a person's sweat. Elevated chloride levels in sweat are a hallmark of cystic fibrosis, so this test helps in the diagnosis of the condition.
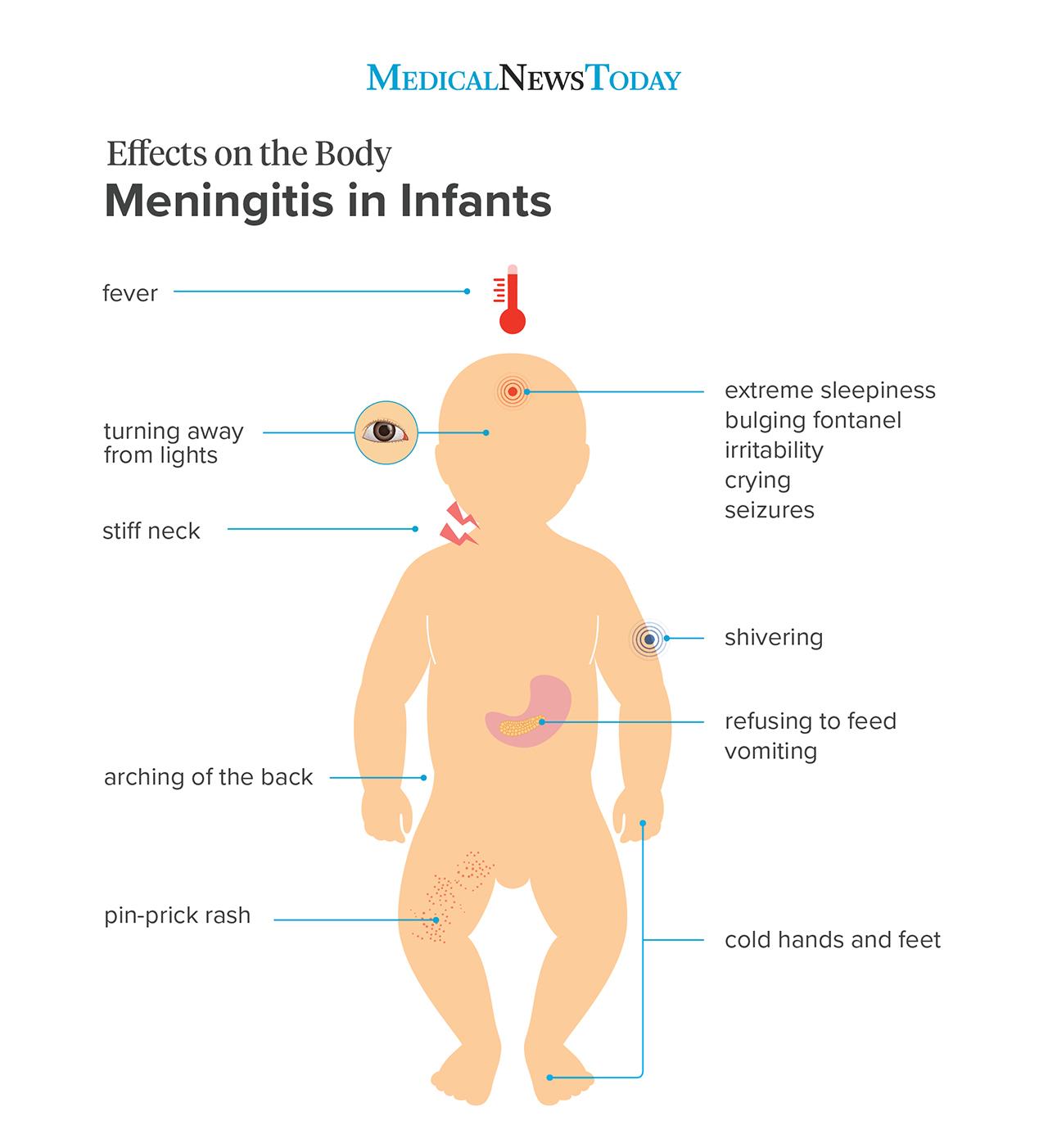
A nurse is planning care for a 6-month-old infant who has bacterial meningitis. Which of the following interventions should the nurse include in the plan of care?
Explanation
Choice A Reason:
Pad the side rails of the crib is correct. This intervention aims to ensure the infant's safety by preventing injury or entrapment in the crib. It's relevant to prevent accidental harm, especially if the infant is experiencing seizures or increased muscle tone due to meningitis.
Choice B Reason:
Keep the television on in the room to provide background noise is incorrect. Background noise might be distracting and uncomfortable for an infant with bacterial meningitis, especially if they're experiencing sensitivity to light and sound due to their condition. A quiet, calm environment is generally more conducive to their recovery.
Choice C Reason:
Place the infant in a semiprivate room is incorrect. Providing a quieter environment with fewer disturbances can be beneficial for an infant with bacterial meningitis. This measure promotes rest and minimizes exposure to potential infections from other patients.
Choice D Reason:
Provide frequent range of motion to the neck and shoulders is incorrect. In cases of bacterial meningitis, particularly when inflammation occurs in the meninges (the protective membranes covering the brain and spinal cord), excessive movement or manipulation of the head and neck might be painful and could exacerbate symptoms.
A nurse is reviewing the laboratory results of a preschooler who has gastroenteritis and notes the client's potassium level is 3.2 mEq/L. Which of the following assessment findings should the nurse expect?
Explanation
Choice A reason:
Oliguria is incorrect. Low potassium levels (hypokalemia) may lead to decreased kidney function and reduced urine output (oliguria) in severe cases. However, at this potassium level, oliguria might not be the immediate or most prominent finding.
Choice B Reason:
Hyperactive bowel sounds are incorrect. Gastroenteritis typically presents with increased bowel sounds due to gastrointestinal irritation or inflammation. Potassium levels might not directly influence bowel sounds, so hyperactive bowel sounds might not be specifically related to the potassium level.
Choice C Reason:
Hyporeflexia is correct. Hypokalemia, indicated by a low potassium level, can affect nerve conduction and muscular function, potentially leading to hyporeflexia (reduced reflexes) as one of its manifestations. This can be a relevant finding associated with low potassium levels.
Choice D Reason:
Hypertension is incorrect. Hypokalemia is more commonly associated with hypotension (low blood pressure) rather than hypertension (high blood pressure). Therefore, hypertension is less likely to be an expected finding related to low potassium levels.
A nurse is providing teaching to the parents of a 2-month-old infant who has developmental dysplasia of the hip and has a prescription for a Pavlik harness. Which of the following statements by the parents indicates an understanding of the teaching?
Explanation
Choice A Reason:
"We will apply lotion to the skin under the straps." Applying lotion under the straps might create moisture, interfere with the harness's function, or cause skin irritation. It's generally recommended to avoid lotions or creams under the straps.
Choice B Reason:
"We should expect our baby to wear this harness for 2 weeks." The duration for wearing a Pavlik harness can vary significantly depending on the severity of the hip dysplasia and the infant's response to treatment. The duration is determined by the healthcare provider's assessment and may extend beyond 2 weeks.
Choice C Reason:
"We will place the diaper under the straps." Placing the diaper under the straps helps prevent skin irritation and chafing caused by the straps rubbing against the skin. It ensures that the skin remains protected and reduces the risk of skin breakdown or discomfort for the infant.
Choice D Reason:
"We should adjust the straps daily." Adjusting the straps of the Pavlik harness daily is an essential part of care to ensure proper positioning and support for the infant's hips. Correct adjustment maintains the harness's effectiveness in keeping the hips in the appropriate position for optimal treatment of developmental dysplasia.

A nurse is reviewing the medical record of a 15-month-old child who is scheduled to receive the measles, mumps, and rubella (MMR) vaccine. Which of the following findings should the nurse identify as a contraindication for receiving this vaccine?
Explanation
Choice A Reason:
Allergy to neomycin is correct. Neomycin is an antibiotic, and individuals with a known severe allergic reaction to neomycin should avoid vaccines that contain this component. The MMR vaccine, along with some other vaccines, may contain trace amounts of neomycin, and individuals with a severe allergy to neomycin might be at risk for an allergic reaction if they receive a vaccine containing this substance.
Choice BReason:
Temperature of 37.2° C (99° F) is incorrect. A low-grade fever (slight elevation in temperature) is not a contraindication for the MMR vaccine unless the fever is part of a more severe illness or if the child has a high fever or is significantly unwell.
Choice CReason:
Family history of seizures is incorrect. A family history of seizures generally does not contraindicate the MMR vaccine. However, certain specific medical conditions or individual situations related to seizures might be considered by the healthcare provider.
Choice D Reason:
Upper respiratory infection 2 days ago is incorrect. Having had a mild upper respiratory infection in the recent past, especially if the child has recovered and is feeling well without any fever, is generally not a contraindication for the MMR vaccine. However, if the child is currently acutely ill or has a fever, the vaccine might be postponed until they are feeling better.
A nurse is discussing coping mechanisms with a parent of a 3-month-old infant. Which of the following therapeutic questions should the nurse ask the parent?
Explanation
Choice A Reason:
"Are you willing to take new parenting classes?" This question is about the parent's willingness to seek additional education rather than exploring their current coping methods.
Choice B Reason:
"What do you do when your infant is fussy?" is correct. This question invites the parent to share their strategies for managing their infant's fussiness, allowing the nurse to gain insight into the parent's coping mechanisms and caregiving approaches. It acknowledges the challenges of dealing with a fussy infant while providing an opportunity for the parent to discuss their techniques for soothing or calming the baby.
Choice C Reason:
"Is it overwhelming when your infant is having a bad day?" While this question acknowledges the potential stress the parent may experience, it might not directly invite discussion about coping mechanisms or strategies.
Choice D Reason:
"Does parenting because you stress?" This question directly addresses stress but might not encourage the parent to discuss specific coping mechanisms or strategies they use when faced with challenging situations.
A nurse is performing a cranial nerve assessment on a school-age child. Which of the following findings indicates proper functioning of the child's trigeminal nerve?
Explanation
Choice A Reason:
The child exhibits a gag reflex when stimulated with a tongue blade. The gag reflex involves the glossopharyngeal nerve (cranial nerve IX) and vagus nerve (cranial nerve X), not the trigeminal nerve.
Choice B Reason:
The child has symmetrical jaw strength when biting down is correct. This finding indicates proper functioning of the child's trigeminal nerve. Symmetrical jaw strength when biting down suggests that both sides of the jaw muscles, which are innervated by the trigeminal nerve, are functioning equally and appropriately.
Choice C Reason:
The child maintains balance when standing with eyes closed is incorrect. This assessment involves the vestibular system and coordination, which are primarily associated with the vestibulocochlear nerve (cranial nerve VIII), not the trigeminal nerve.
Choice D Reason:
The child correctly identifies specific scents is incorrect. The olfactory nerve (cranial nerve I) is responsible for the sense of smell, not the trigeminal nerve.

A nurse is evaluating a 4-year-old child who has cystic fibrosis and has been receiving chest physiotherapy treatments. The nurse should identify which of the following findings as an indication that the therapy has been effective?
Explanation
Choice A Reason:
Increased expectoration is correct. Increased expectoration (coughing up and clearing mucus) could indicate improved airway clearance, which is a primary goal of chest physiotherapy in cystic fibrosis. Effective therapy would facilitate the removal of mucus from the airways, making it easier for the child to clear secretions.
Choice B Reason:
Reduced pain is incorrect. While reducing pain is important for overall comfort, chest physiotherapy's primary goal in cystic fibrosis is to improve airway clearance and lung function. Pain reduction might not be the primary indicator of the therapy's effectiveness in this context.
Choice C Reason:
Increased heart rate is incorrect. An increased heart rate might not directly indicate the effectiveness of chest physiotherapy for cystic fibrosis. The focus is primarily on improving respiratory function and airway clearance rather than affecting heart rate.
Choice D Reason:
Increased urine output is incorrect. Increased urine output is not typically a direct indicator of the effectiveness of chest physiotherapy in cystic fibrosis. Chest physiotherapy aims to improve respiratory function rather than affecting urine output.
Sign Up or Login to view all the 65 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
