ATI RN FUNDAMENTALS 2019 Updated 2024
Total Questions : 48
Showing 25 questions, Sign in for moreA nurse is mixing a short-acting insulin and an intermediate-acting insulin in the same syringe for a client who has diabetes mellitus. Which following actions should the nurse take first?
Explanation
The correct order of actions for mixing short-acting and intermediate-acting insulin in the same syringe is as follows:
- Inject air into the intermediate-acting insulin vial.
- Inject air into the short-acting insulin vial.
- Draw the short-acting insulin into the syringe.
- Draw the intermediate-acting insulin into the syringe.
The reason for this order is to prevent contamination of the vials. By injecting air into each vial first, you create equalized pressure, making it easier to withdraw the insulin. Drawing the short-acting insulin before the intermediate-acting insulin helps prevent contamination of the short-acting insulin vial with the intermediate-acting insulin.
A nurse is caring for a client who is scheduled for surgery. While the nurse is witnessing the client's signature, the client states, "I trust my doctor, but I don't understand what is meant by resecting my intestines." Which of the following actions should the nurse take?
Explanation
It is important for the nurse to ensure that the client has a clear understanding of the procedure they are about to undergo. The nurse should use clear and simple language to explain the purpose and process of the surgery, as well as any potential risks or benefits. This will help address the client's concerns and ensure they are fully informed before giving their consent.
While it may be necessary to involve the provider if there are specific questions or concerns beyond the nurse's scope of practice, providing information and addressing the client's immediate concerns is the first step.
Providing brochures about the procedure can also be helpful, but it should be accompanied by a verbal explanation to ensure understanding.
Completing an incident report is not warranted in this situation unless there is an actual incident or error in the process of obtaining informed consent.
A nurse is caring for a client who refuses to follow the provider's prescription for strict bed rest. The nurse overhears an assistive personnel (AP) tell the client, "If you do not remain in bed, I will place you in restraints." The nurse should identify that the AP is committing which of the following torts?
Explanation
False imprisonment occurs when a person intentionally restricts another person's freedom of movement without lawful justification. By threatening to place the client in restraints if they do not comply with bed rest, the AP is unlawfully restraining the client's freedom. This action is a violation of the client's rights and is considered a form of false imprisonment.
Assault refers to the threat or apprehension of harmful or offensive contact, while battery involves the actual intentional harmful or offensive contact.
Defamation of character refers to making false statements that harm a person's reputation.
A nurse is providing teaching for a client who is scheduled for an allogeneic stem cell transplant. Which of the following information should the nurse include?
Explanation
“You will be in a negative-airflow room to keep the air cleaner." This is important because individuals undergoing stem cell transplants are at increased risk of infections, and being in a negative-airflow room helps reduce the risk of airborne contaminants.
"You will need to wear a mask when outside of your room." This is necessary to protect the client from exposure to potential pathogens in the hospital environment, as their immune system may be compromised during the transplant process.
"Your visitors will need to wear protective gowns." This is important to ensure that visitors do not bring in any infections or pathogens that could potentially harm the client. Protective gowns help reduce the risk of transmission.
However, the statement "You will be placed in a semi-private room" is not accurate. Patients undergoing stem cell transplants are usually placed in private rooms to minimize the risk of infections and to provide a controlled environment.
A nurse is caring for a client who has restraints to each extremity. Which of the following assessments should the nurse perform first?
Explanation
The nurse should assess the pulses in the extremities to ensure that circulation is not compromised by the restraints.
Once the nurse has confirmed that the peripheral pulses are intact, they should assess the client's skin integrity. Prolonged or improperly applied restraints can cause pressure injuries or skin breakdown, so it is important to check for any signs of skin damage.
After assessing peripheral pulses and skin integrity, the nurse should evaluate the client's comfort level. The nurse should address any discomfort or pain caused by the restraints and ensure that the client's physical and emotional needs are met.
While elimination needs are important, they may not pose an immediate threat to the client's safety compared to compromised circulation or skin integrity. Once the more urgent assessments have been completed, the nurse should address the client's elimination needs.
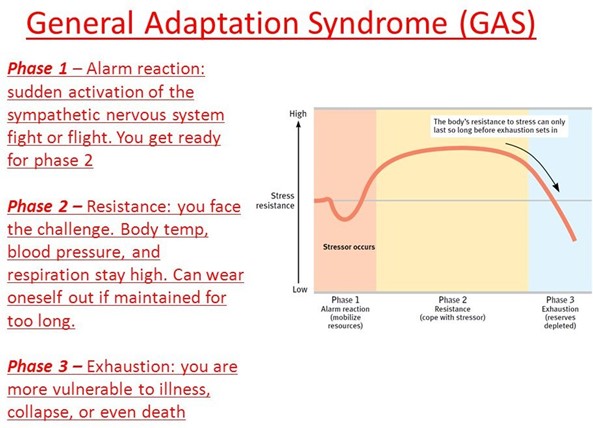
A nurse is discussing the stages of general adaptation syndrome with a newly licensed nurse. The nurse should identify that which of the following manifestations occurs during the alarm reaction stage?
Explanation
During the alarm reaction stage of the general adaptation syndrome (GAS), the body's initial response to stress occurs. This stage is characterized by the activation of the body's
fight-or-flight response. The nurse should identify that the manifestation that occurs during the alarm reaction stage is dilated pupils.
The alarm reaction stage is the body's immediate response to a stressor, where it mobilizes its resources to cope with the perceived threat. During this stage, the sympathetic nervous system is activated, resulting in various physiological changes to prepare the body for action. Dilated pupils are one of the responses caused by the sympathetic nervous system activation. This physiological change enhances visual acuity and allows for better peripheral vision, which can be beneficial in assessing the environment for potential threats.
A nurse is teaching a client how to self-administer daily low-dose heparin injections. Which of the following factors is most likely to increase the client's motivation to learn?
Explanation
Motivation is influenced by various factors, including the client's perception of the benefits or rewards they will receive by engaging in a particular behavior. When the client believes that their needs will be met through education, they are more likely to be motivated to learn and actively participate in the teaching process.
Seeking family approval, while a positive influence, may not be the strongest motivator for learning in this context. While family approval can be a source of motivation, it may not be the primary driving factor for an individual's willingness to learn a specific skill.
The nurse explaining the need for education is important for providing rationale and understanding, but it may not directly increase the client's motivation unless it is tied to the client's own needs and expectations.
The nurse's empathy is a valuable quality that can create a supportive and trusting environment for the client. While empathy can foster a positive nurse-client relationship and enhance the client's overall experience, it may not directly increase the client's motivation to learn unless it is coupled with addressing the client's needs and expectations.
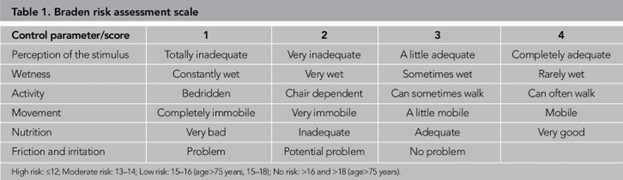
A nurse is teaching a group of newly licensed nurses about the Braden scale. Which of the following responses by a newly licensed nurse indicates an understanding of the teaching?
Explanation
The Braden scale is a commonly used tool for assessing a patient's risk of developing pressure injuries (also known as pressure ulcers or bedsores). It evaluates six specific elements to determine the patient's risk level. These elements include sensory perception, moisture, activity, mobility, nutrition, and friction/shear. Each element is assessed and assigned a score, with a lower score indicating a higher risk for developing pressure injuries.
A nurse is providing care for a client who is to undergo a total laryngectomy. Which of the following interventions is the nurse's priority?
Explanation
After a total laryngectomy, the client will no longer have a vocal cord and will need to learn alternative methods of communication. Esophageal speech is one of the techniques that can be taught to the client. It involves the client swallowing air and then using the air to produce speech sounds by burping or belching it back up from the esophagus. Teaching the client this technique is crucial to facilitate effective communication and help them adjust to their new way of speaking.
While scheduling a support session, determining the client's reading ability, and reviewing the use of an artificial larynx are also important aspects of care for a client undergoing a total laryngectomy, explaining the techniques of esophageal speech takes priority as it directly addresses the client's immediate need for communication.
A nurse is planning care for a client who is scheduled for an intravenous pyelogram. Which of the following actions is appropriate for the nurse to include?
Explanation
An IVP is a radiographic procedure that involves injecting a contrast dye into the vein to visualize the urinary tract. Metal objects can interfere with the imaging process and may need to be removed or avoided during the procedure. The nurse should assess the client for any metal objects, such as jewelry or clothing accessories, and ensure they are removed before the procedure to ensure accurate imaging.
Monitoring the client for pain in the suprapubic region is not directly related to an IVP. Suprapubic pain may be associated with other urinary tract procedures or conditions, but it is not a specific concern during an IVP.
Assisting the client with a bowel cleansing is not necessary for an IVP. Bowel cleansing is typically done for procedures involving the lower gastrointestinal tract, such as colonoscopy or barium enema.
Administering oral contrast before the procedure is also not necessary for an IVP. In an IVP, the contrast dye is administered intravenously, not orally. Oral contrast is typically used for imaging studies of the gastrointestinal tract, such as an upper GI series or CT scan of the abdomen.
A nurse is caring for a client who has a tracheostomy. Which of the following actions should the nurse take?
Explanation
The tracheostomy ties should be secure enough to keep the tracheostomy tube in place but loose enough to allow for proper circulation and prevent skin breakdown. Allowing one finger to fit snugly underneath ensures that the ties are not too tight, which can compromise blood flow
A nurse is teaching a newly licensed nurse about the care of a client who has a methicillin-resistant Staphylococcus aureus (MRSA) infection. Which of the following statements by the newly licensed nurse Indicates an understanding of the teaching?
Explanation
MRSA is a highly contagious infection that can spread through direct contact or through contaminated surfaces. Placing the client in a private room helps minimize the risk of spreading
the infection to other patients or healthcare providers. This measure is known as "contact precautions" and is a standard practice for managing MRSA infections.
When removing personal protective equipment (PPE) after caring for a client with MRSA, it is important to remove the gloves first, followed by the gown. This sequence helps prevent contamination of the hands.
While it is generally important for visitors to practice good hand hygiene, wearing a mask when they are within 3 feet of the client may not be necessary unless they are providing direct care and are in close proximity to the client's respiratory secretions.
The use of N95 respirator masks is primarily indicated for airborne precautions, such as in cases of tuberculosis. For MRSA, the primary mode of transmission is through direct contact or contaminated surfaces, so standard precautions and appropriate hand hygiene are the key preventive measures.
A nurse is preparing to administer several medications via NG tube to a client who is receiving continuous tube feeding. Which of the following actions should the nurse take?
Explanation
When administering medications via an NG tube to a client who is receiving a continuous tube feeding, it is important to flush the tube with water before and after each medication to ensure that the medication is delivered and to prevent any medication from remaining in the tube and causing a blockage. Flushing the tube with 5 mL of sterile water prior to administration will help clear the tube and ensure that the medication is delivered effectively.
Mixing the medications together in a single syringe or combining the medications with the formula in the feeding bag can lead to medication interactions or decreased medication efficacy. Diluting each crushed medication with sterile water may not be necessary, as long as the medication is crushed into a fine powder and flushed properly before and after administration
A nurse is planning care for a client who has a latex allergy and is scheduled for surgery. Which of the following actions is appropriate for the client's plan of care?
No explanation
A nurse is reviewing a client's intake and output and notes the following: 0.9% sodium chloride 600 mL IV infusion, cefazolin 250 mg in dextrose 5% in water 100 mL. Intermittent IV bolus, 200 mL emesis, 40 mL voided urine, and 20 mL urine from straight catheterization. The nurse should record the client's net fluid intake as how many mL? (Round the answer to the nearest whole number. Use a leading zero if it applies. Do not use a trailing zero.)
Explanation
To calculate the client's net fluid intake, we need to subtract the output (emesis and urine) from
the intake (IV infusion and IV bolus). Intake:
- 0.9% sodium chloride IV infusion: 600 mL
- Cefazolin in dextrose 5% in water IV bolus: 100 mL Output:
- Emesis: 200 mL
- Voided urine: 40 mL
- Urine from straight catheterization: 20 mL Net fluid intake = Intake - Output
Net fluid intake = (600 mL + 100 mL) - (200 mL + 40 mL + 20 mL) Net fluid intake = 700 mL - 260 mL
Net fluid intake = 440 mL
Therefore, the nurse should record the client's net fluid intake as 440 mL.
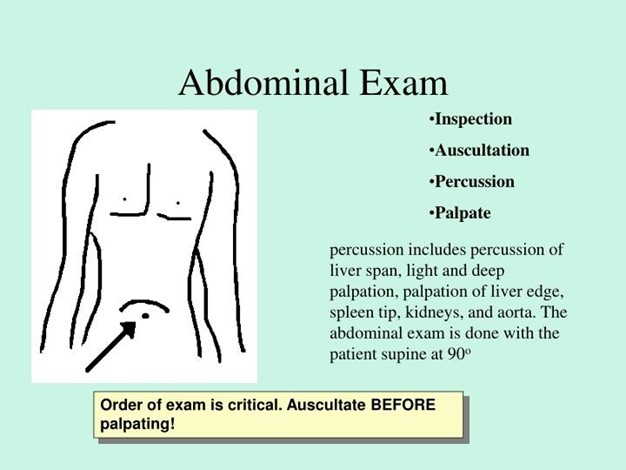
A nurse is preparing to perform a physical assessment of a client's abdomen. Identify the sequence in which the nurse should perform the following steps. (Move the steps into the box on the right, placing them in the order of performance. Use all the steps.)
Explanation
To perform a physical assessment of a client's abdomen, the nurse should follow the following sequence:
1. Provide adequate lighting to inspect the abdomen.
2. Listen to the abdominal arteries using the bell of a stethoscope.
3. Percuss all four quadrants of the abdomen to measure sound quality.
4. Check for areas of tenderness by pressing fingers 1.3 cm (0.5 in) into the abdomen.
5. Locate liver and spleen borders by pressing hands 2.5 to 7.5 cm (1 to 3 in) into the abdomen.
A nurse receives a new prescription over the telephone from a client's provider. Which of the following actions should the nurse take first
Explanation
When receiving a new prescription over the telephone, it is crucial to ensure accuracy and prevent medication errors. Reading back the prescription to the provider is an essential step to confirm that the nurse has understood the prescription correctly. This allows for immediate clarification if there are any discrepancies or misunderstandings. By reading back the prescription, the nurse and the provider can confirm the accuracy of the order before further actions are taken.
A nurse is preparing to administer an injection to a client. Which of the following actions should the nurse plan to take after Injection?
Explanation
Proper disposal of used needles is crucial to prevent needlestick injuries and the transmission of infectious diseases. The nurse should follow safe needle disposal practices, which typically involve placing the used needle immediately into a puncture-proof container, such as a sharps container. This container is specifically designed to safely store used needles and prevent accidental needlesticks.
Removing the needle from the syringe before proper disposal can increase the risk of needlestick injuries. It is recommended to dispose of the needle while it is still attached to the syringe.
Placing the needle on the bedside table is not a safe practice. It can lead to accidental needlestick injuries for both the healthcare provider and others who may come into contact with the needle.
Recapping the needle increases the risk of needlestick injuries. It is generally discouraged to recap needles, as it can result in accidental needlestick injuries.

A nurse is assisting in the use of a fracture bedpan for a client who is immobile due to a cast. Which of the following actions should the nurse take?
Explanation
When using a fracture bedpan, it is important to position the pan correctly to provide proper support and comfort to the client. The shallow end of the fracture pan should be placed under the client's buttocks, as this end is designed to accommodate the body shape and offer a more comfortable position.
Hyperextending the client's back while the fracture pan is in place can cause discomfort, strain, or potential injury to the client. It is important to maintain a comfortable and neutral position for the client during bedpan use.
Encouraging the client to try to defecate for a specific time period, such as 20 minutes, is not recommended. It is more appropriate to allow the client adequate time and privacy to attempt to defecate without time constraints.
Keeping the bed flat while the client is on the fracture pan may not provide the optimal position for comfort and ease of use. Slight elevation of the head of the bed (Fowler's position) can provide a more comfortable position for the client during bedpan use.
A home health nurse is teaching a client about home safety. Which of the following statements by the client indicates an understanding of the teaching? (Select all that apply.)
Explanation
"I will apply tape over frayed areas of electrical cords": This statement shows an understanding of the importance of addressing frayed electrical cords promptly. Applying tape can help prevent electrical hazards and reduce the risk of electric shocks or fires.
"I need to check my medications for expiration dates": Checking medication expiration dates is crucial to ensure the effectiveness and safety of the medications. Expired medications may lose their potency or become potentially harmful.
"I will use the grab bars when getting in and out of the bathtub": Using grab bars provides stability and support, reducing the risk of falls when entering or exiting the bathtub. This demonstrates an understanding of the importance of using assistive devices for safety.
"I need to have a fire escape plan with my family": Having a fire escape plan is essential for emergency preparedness. It indicates that the client recognizes the importance of having a plan in place to ensure everyone's safety in the event of a fire.
The statement "I need to set my hot water heater to 140 degrees Fahrenheit" is not a correct understanding of home safety. The recommended safe temperature for hot water heaters is typically set at 120 degrees Fahrenheit or below to prevent scalding injuries. Therefore, this statement indicates a misunderstanding of the proper temperature setting for hot water heaters.
A nurse is performing postural drainage with percussion and vibration for a client who has cystic fibrosis. Which of the actions should the nurse take?
Explanation
It is recommended to perform postural drainage on an empty stomach to minimize the risk of vomiting and aspiration during the procedure. Therefore, scheduling it before meals or after an adequate time interval is important.
During percussion and vibration, the client should be instructed to exhale slowly and deeply to facilitate the mobilization and removal of mucus from the airways. Exhaling quickly may not provide the same beneficial effect.
Percussion is typically performed over the chest, not the lower back, to help loosen and mobilize secretions in the lungs. It involves rhythmic tapping with cupped hands over the specific lung segments while the client is in specific postural positions to facilitate drainage.
When performing percussion, placing a towel or cloth over the area being percussed dampens the vibrations during percussion.
A nurse is delegating client care tasks to an assistive personnel. Which of the following tasks should the nurse delegate?
Explanation
Performing a simple dressing change is a task that can be safely delegated to an assistive personnel who has received appropriate training and competency validation. It involves removing the old dressing, cleaning the wound if necessary, and applying a new dressing
A charge nurse in a long-term care facility is preparing an educational program about delirium for newly hired nurses. Which of the following statements should the nurse plan to Include?
Explanation
Delirium is an acute confusional state that develops rapidly over a short period of time, often within hours or days. It is characterized by a disturbance in consciousness and attention, along with changes in cognition and perception.
Delirium can significantly impact a client's perception of their environment. Clients with delirium may experience hallucinations, delusions, and misinterpretations of their surroundings. They may become disoriented, have difficulty recognizing familiar people or places, and exhibit altered levels of awareness and attention.
As mentioned earlier, delirium has an abrupt onset, meaning it develops rapidly. Delirium is usually a transient condition that fluctuates throughout the day, with symptoms varying in severity.
Delirium can disrupt a client's sleep-wake cycle. Clients with delirium may experience disturbances in their sleep patterns, such as difficulty falling asleep, frequent awakening during the night, or excessive sleepiness during the day.
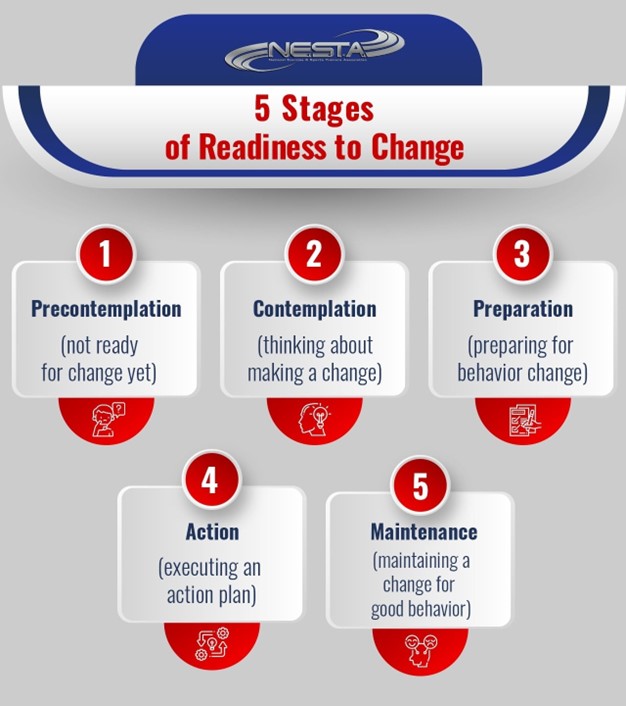
A nurse is planning care for a client who is concerned about her tobacco smoking habits and is in the contemplation stage of health behavior change. Which of the following actions should the nurse plan to take during this stage?
Explanation
The contemplation stage is characterized by the client's acknowledgment of the need for change but having mixed feelings and ambivalence about making the actual change. During this stage, the nurse should provide information and education to the client about the benefits of quitting smoking. This can include discussing the health risks associated with smoking, such as increased risk of cardiovascular diseases, respiratory problems, and certain types of cancer.
Presenting this information can help the client gain a better understanding of the positive impact quitting smoking can have on their health and well-being.
Developing a plan for the client to integrate the change into her lifestyle is more suitable for the preparation stage, where the client is actively planning and preparing to make the behavior change. During the contemplation stage, the client is not yet ready for detailed planning, but rather exploring their feelings and concerns about the behavior change.
Making small changes over time is more aligned with the action stage, where the client is actively making changes to their behavior. In the contemplation stage, the client is not yet ready for making immediate changes and is still weighing the pros and cons of quitting smoking.
Setting goals is more appropriate for the preparation stage, where the client is actively preparing to make the behavior change. During the contemplation stage, the client is still considering the change and may not be ready to set specific goals.
A nurse is reviewing the medical record of a client who asks about the use of magnet therapy for pain relief. The nurse should identify that which of the following findings is a contraindication for receiving this type of therapy?
Explanation
Magnet therapy involves the use of magnets to treat various conditions, including pain relief. However, certain precautions and contraindications exist for the use of magnet therapy, especially in individuals with implanted medical devices.
Implantable cardioverter-defibrillators (ICDs) are designed to detect and treat life-threatening arrhythmias. They often contain magnetic components and sensitive circuitry that can be affected by strong magnetic fields, including those used in magnet therapy. The magnetic field from the therapy may interfere with the proper functioning of the implanted defibrillator, potentially compromising the client's safety.

Having a prescription for metoprolol, which is a beta-blocker medication used to manage conditions such as high blood pressure and heart disease, is not a contraindication for receiving magnet therapy. There is no direct interaction between metoprolol and magnet therapy.
Having an allergy to penicillin does not directly contraindicate the use of magnet therapy for pain relief. Allergies to penicillin are specific to the medication itself and do not impact the use of magnets.
A history of alcohol use disorder is not a direct contraindication for receiving magnet therapy. However, it is important to consider the overall health status and any potential interactions with other treatments or medications related to the alcohol use disorder.
Sign Up or Login to view all the 48 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
