ATI RN maternal Newborn 2019 with NGN
Total Questions : 66
Showing 25 questions, Sign in for moreAfter completing post anesthesia recovery assessments, the registered nurse (RN) asks the practical nurse (PN) to transfer four clients, each two hours post-birth, to the postpartum unit. Which client should the PN ask the RN to reassess prior to transfer?
Explanation
This client should be reassessed by the RN prior to transfer, as worsening perineal pain may indicate a hematoma, infection, or inadequate pain management. The RN should inspect the perineum, check the vital signs, and evaluate the effectiveness of the medication.
The other options are not correct because:
B .A multigravida whose peri-pad is 1/4 saturated with lochia rubra after one hour does not need to be reassessed by the RN, as this is a normal finding for a client two hours post-birth. Lochia rubra is the red-colored vaginal discharge that contains blood and debris from the placental site, and it usually lasts for 3 to 4 days after delivery. A peri-pad that is 1/4 saturated after one hour is within the expected range of blood loss.
C. A multigravida complaining of strong afterbirth pains when breastfeeding does not need to be reassessed by the RN, as this is a normal finding for a client two hours post-birth. Afterbirth pains are cramps caused by uterine contractions that help shrink the uterus and prevent bleeding. They are more common and intense in multiparous women and during breastfeeding, as oxytocin is released and stimulates the contractions.
D. A primigravida who passed a small clot when she sat up on the edge of the bed does not need to be reassessed by the RN, as this is a normal finding for a client two hours post-birth. Small clots may form in the uterus or vagina due to pooling of blood during rest or anesthesia, and they are usually expelled when changing position or ambulating. As long as the clot is smaller than a plum and there is no excessive bleeding or pain, it is not a cause for concern.
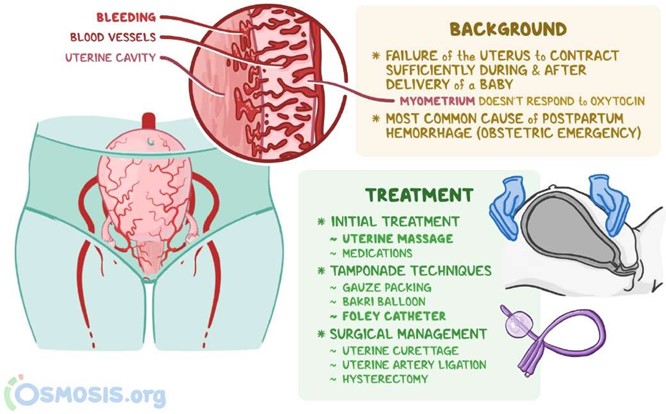
A nurse is discussing risk factors of postpartum hemorrhage with a newly licensed nurse.
Which of the following conditions is a risk factor for postpartum hemorrhage that the nurse should include in the teaching?
Explanation
Retained placental fragments is a risk factor for postpartum hemorrhage. After delivery, the uterus continues to contract to deliver the placenta.
Contractions also help to compress the blood vessels where the placenta was atached to the uterine wall.
Postpartum hemorrhage can happen if parts of the placenta stay atached to the
uterine wall.
Choice A is incorrect because pregnancy-induced hypertension is a risk factor for
postpartum hemorrhage.
Choice B is incorrect because meconium-stained fluid is not mentioned as a risk factor for postpartum hemorrhage in my sources.
Choice D is incorrect because oligohydramnios is not mentioned as a risk factor for postpartum hemorrhage in my sources.
A nurse is planning care for a client who is pregnant and has HIV.
Which of the following actions should the nurse include in the plan of care?
Explanation

Bathing the newborn before initiating skin-to-skin contact is an action that the nurse should include in the plan of care for a client who is pregnant and has HIV.
Choice A is incorrect because using a fetal scalp electrode during labor and delivery is not mentioned as an action that should be included in the plan of care for a client who is pregnant and has HIV in my sources.
Choice C is incorrect because instructing the client to stop taking antiretroviral medications at 32 weeks of gestation is not mentioned as an action that should be included in the plan of care for a client who is pregnant and has HIV in my sources.
Choice D is incorrect because administering a pneumococcal immunization to the newborn within 4 hours following birth is not mentioned as an action that should be included in the plan of care for a client who is pregnant and has HIV in my sources.
A nurse is teaching a client and her partner about the technique of counterpressure during labor.
Which of the following statements by the nurse is appropriate?
Explanation
“Your partner will apply upward pressure on you” is an appropriate statement by the nurse when teaching a client and her partner about the technique of counterpressure during labor.
Counterpressure consists of steady, strong force applied to one spot on the lower back during contractions using the heel of the hand, or pressure on the side of each hip using both hands.

Choice A is incorrect because applying continuous, firm pressure between the thumb and index finger is not mentioned as a technique of counterpressure during labor in my sources.
Choice B is incorrect because applying pressure to the top of the uterus during contractions is not mentioned as a technique of counterpressure during labor in my sources.
Choice C is incorrect because applying steady pressure with a tennis ball to the finger is not mentioned as a technique of counterpressure during labor in my sources.
A nurse is providing dietary teaching to a client who is at 32 weeks of gestation and has cholelithiasis.
Which of the following foods should the nurse recommend for the client to include in her diet?
Explanation
Baked chicken is a food that the nurse should recommend for a client who is at
32 weeks of gestation and has cholelithiasis to include in her diet.
Eating healthy fats, like those found in lean meats such as chicken, can help the gallbladder contract and empty on a regular basis.

Choice B is incorrect because French fries are not a food that the nurse should recommend for a client who is at 32 weeks of gestation and has cholelithiasis to include in her diet.
Unhealthy fats, like those often found in fried foods, should be avoided.
Choice C is incorrect because whole milk is not a food that the nurse should recommend for a client who is at 32 weeks of gestation and has cholelithiasis to include in her diet.
Unhealthy fats, like those often found in whole milk, should be avoided.
Choice D is incorrect because a bacon cheeseburger is not a food that the nurse should recommend for a client who is at 32 weeks of gestation and has cholelithiasis to include in her diet.
Unhealthy fats, like those often found in bacon and cheeseburgers, should be avoided.
A nurse is providing discharge instructions to a client who is 24 hours postpartum and has decided not to breastfeed.
Which of the following instructions should the nurse include in the teaching?
Explanation
“Apply ice packs to your breasts using a 15 minutes on, 45 minutes off schedule.”
This can help reduce swelling and relieve discomfort from engorgement.

Choice B is incorrect because warm water can increase blood flow and may worsen engorgement.
Choice C is incorrect because a supportive bra can help reduce discomfort from engorgement.
Choice D is incorrect because pumping can stimulate milk production and may worsen engorgement.
A nurse is performing a heel stick on a newborn. Which of the following actions should the nurse take?
Explanation
“Use an automatic puncture device on the heel.” This is the most common and minimally invasive method to draw capillary blood from an infant for medical testing.
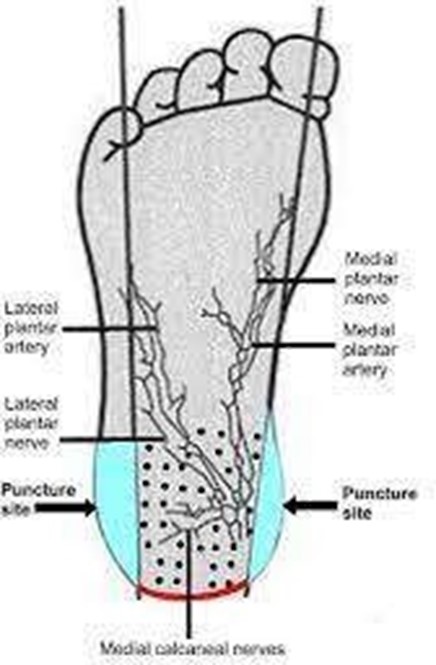
Choice A is incorrect because the heel should be punctured on the outer aspect of the foot to avoid damaging the calcaneus bone.
Choice C is incorrect because the heel should be cleansed with an alcohol swab
before, not after, the procedure.
Choice D is incorrect because there is no need to place an ice pack on the newborn’s heel before the procedure.
A nurse is assessing a full-term newborn upon admission to the nursery.
Which of the following clinical findings should the nurse report to the provider?
Explanation
Rust-stained urine.
Rust-stained urine in a newborn can be a sign of a serious medical condition and should be reported to the provider.

Choice B is not the answer because subconjunctival hemorrhage in a newborn is usually normal and harmless.
It may be caused by pressure changes during vaginal delivery and will disappear on its own after two or three weeks.
Choice C is not the answer because single palmar creases develop while a baby
is growing in the womb and appear in about 1 out of 30 people.
While some single palmar creases may indicate problems with development and be linked with certain disorders, it is not necessarily a cause for concern.
Choice D is not the answer because transient circumoral cyanosis refers to blue discoloration around the mouth only and is usually seen in infants.
It’s often considered a type of acrocyanosis which happens when small blood vessels shrink in response to cold.
This is very normal in infants during the first few days after birth.
A nurse is caring for a client who is at 30 weeks of gestation and is receiving magnesium sulfate for preeclampsia.
The nurse should recognize which of the following manifestations as an adverse reaction to the medication?
Explanation
This can be a sign of magnesium toxicity and should be reported to the provider.
Choice A is incorrect because magnesium sulfate is used to treat hypertension associated with preeclampsia.
Choice B is incorrect because a respiratory rate of 16/min is within normal range.
Choice D is incorrect because hyperglycemia is not a known adverse reaction to magnesium sulfate.
A nurse is caring for a client who has a placenta previa.
Which of the following findings should the nurse expect?
Explanation
This is the most common symptom of placenta previa and can occur after 20 weeks of gestation.
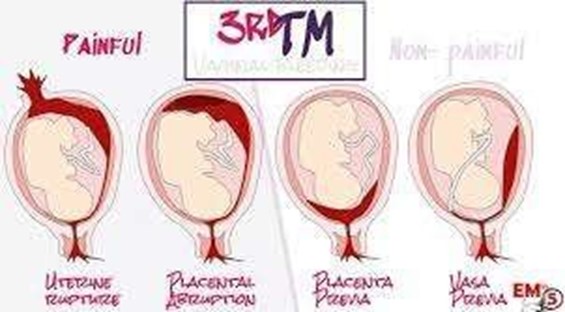
Choice B is incorrect because a persistent headache is not a known symptom of placenta previa.
Choice C is incorrect because uterine hypertonicity is not a known symptom of placenta previa.
Choice D is incorrect because a firm, rigid abdomen is not a known symptom of placenta previa.
A nurse is caring for a client who has hyperemesis gravidarum.
Which of the following laboratory tests should the nurse anticipate?
Explanation
A nurse caring for a client who has hyperemesis gravidarum should anticipate urine ketones test.
Hyperemesis gravidarum is severe nausea and vomiting during pregnancy that results in dehydration, weight loss, and ketosis.
Urine ketones test is done to check for ketosis which is a sign of starvation 2.
Choice A, Rapid plasma reagin, is not an answer because it is a blood test used to screen for syphilis.
Choice B, Prothrombin time, is not an answer because it is a blood test used to measure how long it takes for blood to clot.
Choice D, Urine culture, is not an answer because it is a test used to detect and identify bacteria or yeast that may be causing a urinary tract infection.
A nurse is caring for a client who is receiving prenatal care and is at her 24-week appointment.
Which of the following laboratory tests should the nurse plan to conduct?
Explanation
A nurse caring for a client who is receiving prenatal care and is at her 24-week appointment should plan to conduct a one-hour glucose tolerance test.
This test is done to screen for gestational diabetes that can develop during pregnancy.
Choice A, Group B strep culture, is not an answer because it is a test usually done between 35-37 weeks of pregnancy to check for the presence of Group B streptococcus bacteria.
Choice B, Rubella titer, is not an answer because it is a blood test usually done early in pregnancy to check for immunity to rubella.
Choice C, Blood type and Rh, is not an answer because it is a blood test usually done early in pregnancy to determine the mother’s blood type and Rh factor.
A nurse is providing teaching to a client who is receiving medroxyprogesterone IM for contraception.
Which of the following statements by the client indicates an understanding of the teaching?
Explanation
“I should increase my calcium intake while taking this medication.” A client who is receiving medroxyprogesterone IM for contraception should increase their calcium intake while taking this medication .
Medroxyprogesterone can cause loss of bone mineral density which can increase the risk of osteoporosis. Increasing calcium intake can help maintain bone health.

Choice B, “I should discontinue this medication if I experience spotting,” is not an answer because spotting is a common side effect of medroxyprogesterone and does not require discontinuation of the medication.
Choice C, “I will need to return to the clinic in 8 weeks for my next injection,” is not an answer because medroxyprogesterone IM is given every 3 months, not every 8 weeks.
Choice D, “I will get two shots each time I receive this medication,” is not an answer because only one injection is given at a time.
A nurse is caring for a newborn.
Which of the following assessment findings should indicate to the nurse that suctioning of the nasopharynx is needed?
Explanation
None of the choices provided indicate that suctioning of the nasopharynx is needed for a newborn.
Nasopharyngeal suctioning is performed to remove mucus or saliva from the back of the throat when a newborn is unable to cough or swallow. It is commonly used in infants with bronchiolitis.
Choice A, “The newborn’s respiratory rate is 32/min,” is not an answer because a respiratory rate of 32/min is within the normal range for a newborn.
Choice B, “The newborn’s respiratory rate is irregular,” is not an answer because irregular breathing paterns are common in newborns.
Choice C, “The newborn is beginning to cough,” is not an answer because coughing is a normal reflex that helps clear the airway.
Choice D, “The newborn’s pulse oximetry is 91,” is not an answer because pulse oximetry measures oxygen saturation and does not indicate the need for nasopharyngeal suctioning.
A nurse is assessing a client during her first prenatal visit. The client reports March 20 as her last menstrual period.
Use Naegele's rule to calculate the estimated date of delivery.
(Use the MMDD format with four numerals and no spaces or punctuation: MMDD.)
Explanation
Naegele’s rule is a method for estimating the due date of a baby based on the woman’s last menstrual period (LMP).
It involves adding seven days and subtracting three months from the first day of the LMP.
It assumes a 28-day menstrual cycle and a 280-day gestation period, which may vary for different women 1.
Using this rule, if the client’s last menstrual period was March 20, then adding seven days would give March 27.
Subtracting three months would give December 27 of the previous year.
Adding one year would give December 27 of the current year, which is the estimated date of delivery in MMDD format: 1227.
A nurse is providing discharge instructions to a client who is breastfeeding her newborn.
Which of the following instructions should the nurse include?
Explanation
The American Academy of Pediatrics (AAP) strongly recommends exclusive breastfeeding for at least 6 months.
Exclusive breastfeeding means that your baby has only breastmilk for 6 months. That means giving your baby breastmilk from your breasts or from botles.
Don’t give your baby water, sugar water, or formula.
The other choices are not recommended:
A. Newborns do not need water between feedings.
C. The length of time a newborn feeds per breast can vary and is not necessarily
limited to 5-10 minutes.
D. Newborns typically have more than two to four wet diapers every 24 hours.
A nurse is caring for a client who is at 30 weeks of gestation.
The nurse should plan to immunize the client with which of the following vaccines? (Select all that apply.)
Explanation
The nurse should plan to immunize the client with the inactivated influenza vaccine (A) and the diphtheria-acellular pertussis vaccine (E).

The Centers for Disease Control and Prevention (CDC) recommends that pregnant women get two vaccines during every pregnancy: the inactivated flu vaccine and the Tdap vaccine.
The other vaccines listed are not recommended during pregnancy:
- The human papillomavirus vaccine is not recommended during pregnancy.
- The varicella vaccine is not recommended during pregnancy.
- The measles, mumps, and rubella vaccine is not recommended during pregnancy.
A nurse is caring for a client who is in active labor and has gonorrhea.
For which of the following potential complications of gonorrhea should the nurse monitor?
Explanation
A. The nurse should monitor for chorioamnionitis, which is an infection of the amniotic sac and fluid.
The other choices are not potential complications of gonorrhea:
B. Vaginal laceration during birth is not a complication of gonorrhea.
C. Oligohydramnios is not a complication of gonorrhea.
D. Excessive bleeding after birth is not a complication of gonorrhea.
A nurse is conducting a class for a group of clients about birth control.
Which of the following information should the nurse include in the teaching?
Explanation
A nurse conducting a class for a group of clients about birth control should include information about having an annual examination to assess their diaphragm.
A diaphragm should be replaced at least every 2 years and it’s important to
bring it to an annual checkup so the healthcare provider can check the fit.
Choice A is incorrect because spermicide should be used immediately before sexual intercourse, not 3 hours prior.
Choice B is incorrect because fertility can return immediately after IUD removal.
Choice C is incorrect because emergency contraception is intended for backup contraception only and not as a primary method of birth control
A nurse is caring for a client following a vaginal delivery of a term fetal demise. Which of the following statements should the nurse make?
Explanation
A nurse caring for a client following a vaginal delivery of a term fetal demise should offer the client the option to bathe and dress their baby if they would like to.
Choice A is incorrect because it is not appropriate for the nurse to suggest that the client should name the baby.
Choice B is incorrect because it is not appropriate for the nurse to suggest that not holding the baby will make letting go much harder.
Choice C is incorrect because it is not appropriate for the nurse to make assumptions about future pregnancies.
A nurse is caring for a client who is at 36 weeks of gestation and has methicillin- resistant Staphylococcus aureus.
Which of the following types of isolation precautions should the nurse initiate?
Explanation
A nurse caring for a client who is at 36 weeks of gestation and has methicillin- resistant Staphylococcus aureus (MRSA) should initiate Contact Precautions.
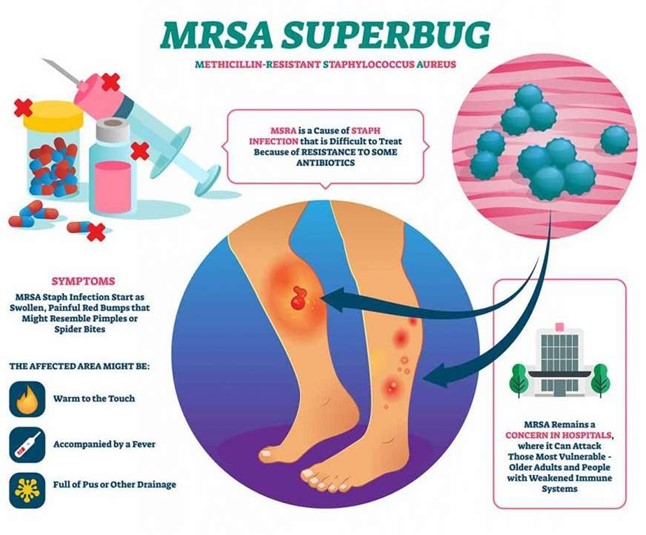
Choice A is incorrect because Droplet Precautions are not necessary for MRSA.
Choice B is incorrect because a Protective Environment is not necessary for MRSA.
Choice D is incorrect because Airborne Precautions are not necessary for MRSA.
A nurse is caring for a newborn who has exstrophy of the bladder.
Which of the following actions should the nurse take prior to the beginning of surgical correction?
Explanation
A nurse caring for a newborn who has exstrophy of the bladder should cover the newborn’s bladder with a sterile, non-adherent dressing prior to the beginning of surgical correction.
Choice A is incorrect because it is not necessary to restrict the newborn’s fluid intake.
Choice B is incorrect because it is not necessary to keep the newborn in a side- lying position.
Choice D is incorrect because it is not appropriate to exert gentle pressure on
the newborn’s bladder with sterile gauze.
A nurse is assessing the results of a nonstress test for an antepartal client at 35 weeks of gestation.
Which of the following findings should indicate to the nurse the need for further diagnostic testing?
Explanation
A nurse assessing the results of a nonstress test for an antepartal client at 35 weeks of gestation should indicate the need for further diagnostic testing if there are no late decelerations noted with three uterine contractions of 60 seconds in duration within a 10-min testing period.
Choice A is incorrect because an increase in fetal heart rate to 150/min above the baseline of 140/min lasting 10 seconds in response to fetal movement within a 40-min testing period is a normal result.
Choice B is incorrect because irregular contractions of 10 to 20 seconds in duration that are not felt by the client do not indicate the need for further diagnostic testing.
Choice D is incorrect because three fetal movements perceived by the client in a 20-min testing period do not indicate the need for further diagnostic testing.
A nurse is observing an adolescent client who is offering her newborn a bottle while he is lying in the bassinet.
When the nurse offers to pick the newborn up and place him in the client's arms, the mother states, "No, the baby is too tired to be held." Which of the following actions should the nurse take?
Explanation
The nurse should demonstrate how to hold the newborn and allow the client to
practice.
This will help the mother learn how to properly hold her baby and feel more confident in her ability to care for her newborn.

Choice A is not the best answer because insisting that the mother pick up the
newborn to feed him may make her feel uncomfortable or pressured.
Choice C is not the best answer because persuading the client to breastfeed the newborn to promote bonding may not be appropriate if the mother has chosen to botle-feed her baby.
Choice D is not the best answer because offering to take the newborn to the nursery to finish his feeding may not address the mother’s concerns about holding her baby.
A nurse in a provider's office is caring for a 20-year-old client who is at 12 weeks of
gestation and requests an amniocentesis to determine the sex of the fetus. Which of the following responses should the nurse make?
Explanation
The nurse should inform the client that amniocentesis is a procedure that
determines if the baby has genetic or congenital disorders.
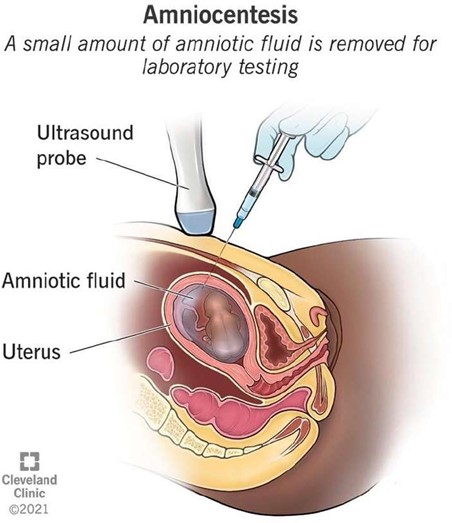
Choice B is not the best answer because amniocentesis is typically performed after 15 weeks of gestation.
Choice C is not the best answer because chorionic villus sampling (CVS) is a different procedure from amniocentesis.
Choice D is not the best answer because there is no age restriction for having an amniocentesis.
Sign Up or Login to view all the 66 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
