RN Nursing Care of Children 2019
Total Questions : 70
Showing 25 questions, Sign in for moreA nurse is assessing a 6-month-old infant who has respiratory syncytial virus.
The nurse should immediately report which of the following findings to the provider?
Explanation

This is because oxygen saturation below 90% indicates that the infant is not getting enough oxygen and central cyanosis (bluish color of the skin due to lack of oxygen) is a sign of severe respiratory distress.
Both of these findings require immediate medical attention.
Choice A is wrong because cough or difficulty in breathing, while concerning, may not require immediate reporting to the provider as they are common symptoms of RSV infection.
Choice C is wrong because severe respiratory distress (e.g grunting, very severe chest indrawing), while concerning, may not require immediate reporting to the provider as they are common symptoms of RSV infection.
Choice D is wrong because signs of pneumonia with a general danger, while concerning, may not require immediate reporting to the provider as they are common symptoms of RSV infection.
A nurse in an emergency department is caring for a preschool-age child who has acute acetylsalicylic acid poisoning.
Which of the following should the nurse expect?
Explanation
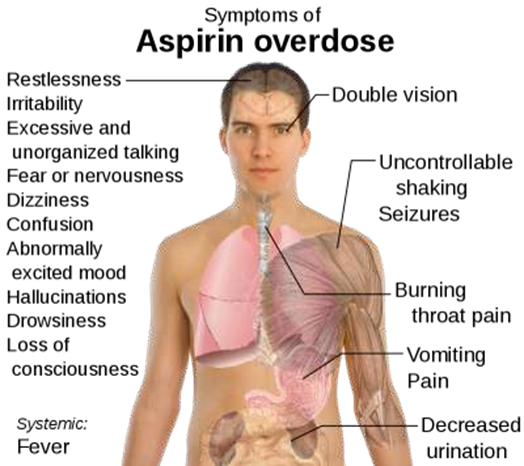
When a child ingests a toxic dose of acetylsalicylic acid, it can lead to salicylate toxicity, which can cause hyperpyrexia (high fever), among other symptoms such as vomiting, tinnitus, confusion, and dehydration. Hyperpyrexia is a serious complication that can lead to neurological damage and is a medical emergency that requires prompt intervention.
The nurse should monitor the child's temperature and administer antipyretic medications as necessary to reduce the fever.
Choice B is wrong because Polyuria, is not a common symptom of acute acetylsalicylic acid poisoning.
Salicylate toxicity can cause dehydration due to vomiting, which can lead to decreased urine output.
Choice C is wrong because Neck vein distention, is not typically associated with acetylsalicylic acid poisoning.
Neck vein distention is commonly seen in patients with heart failure, tension pneumothorax, or cardiac tamponade.
Choice D is wrong because Jaundice, is not a common symptom of acetylsalicylic acid poisoning. Jaundice is usually seen in liver diseases or hemolytic anemias.
A nurse is providing teaching to the parents of a child who has impetigo. Which of the following instructions should the nurse include in the teaching?
Explanation

Impetigo is treated with antibiotics, either topical antibiotics (medicine rubbed onto the sores) or oral antibiotics (medicine taken by mouth). A doctor might recommend a topical ointment for only a few sores.
Choice B is wrong because Soak hairbrushes in boiling water for 10 minutes, is not a recommended instruction for the treatment of impetigo.
Choice C is wrong because Administer acyclovir PO two times per day, is not a recommended instruction for the treatment of impetigo as acyclovir is an antiviral medication and impetigo is caused by bacteria.
Choice D is wrong because Seal soft toys in a plastic bag for 14 days, is not a recommended instruction for the treatment of impetigo.
A nurse is providing teaching to the parents of a school-age child newly diagnosed with a seizure disorder.
The nurse should teach the parents to take which of the following actions during a seizure?
Explanation
During a seizure, it is important to clear the area around the person of anything hard or sharp to prevent injury.
Choice A is wrong because Minimize movement of the limbs, is not a recommended action during a seizure as it is important not to hold the person down or try to stop their movements.
Choice B is wrong because Insert a tongue blade between the teeth, is not a recommended action during a seizure as it is important not to put anything in the person’s mouth.
Choice D is wrong because Place the child in a prone position, is not a recommended action during a seizure as it is important to turn the person gently onto one side to help them breathe.
A nurse in an emergency department is assessing an adolescent who reports inhalation of gasoline.
Which of the following findings should the nurse expect?
Explanation

Ataxia is a neurological sign that refers to a lack of muscle coordination and can cause staggering. Inhalation of gasoline vapors can cause symptoms such as dizziness or lightheadedness, headache, facial flushing, coughing or wheezing, staggering, slurred speech, blurry vision and weakness.
Choice B is wrong because Hypothermia is not an answer because hypothermia refers to a dangerously low body temperature and is not a symptom of gasoline inhalation.
Choice C is wrong because Hyperactive reflexes are not an answer because hyperactive reflexes refer to overactive or overresponsive reflexes and are not a symptom of gasoline inhalation.
Choice D is wrong because Pinpoint pupils are not an answer because pinpoint pupils refer to abnormally small pupils and are not a symptom of gasoline inhalation.
A nurse is caring for a 4-year-old child who has meningitis and is receiving gentamicin.
Which of the following laboratory values should the nurse report to the provider?
Explanation
Gentamicin is an aminoglycoside antibiotic that can cause nephrotoxicity. Nephrotoxicity refers to kidney damage and can be demonstrated by rising serum creatinine levels. A creatinine level of.4 mg/dL is higher than the normal range and may indicate impaired kidney function 2.
Choice B is wrong because Creatinine 0.3 mg/dL is not an answer because it falls within the normal range for creatinine levels.
Choice C is wrong because BUN 12 mg/dL is not an answer because it falls within the normal range for BUN levels.
Choice D is wrong because BUN 6 mg/dL is not an answer because it falls within the normal range for BUN levels.
A nurse is preparing to administer immunizations to a 3-month-old infant.
Which of the following is an appropriate action for the nurse to take to deliver atraumatic care?
Explanation

Oral sucrose solution has been shown to have analgesic effects and can help reduce pain and discomfort in infants during procedures such as immunizations.
Choice B is wrong because Use a 20-gauge needle for the injections is not an answer because a 20-gauge needle is larger than the recommended size for infant immunizations.
Choice C is wrong because Apply eutectic mixture of local anesthetics (EMLA) cream immediately before the injections is not an answer because EMLA cream needs to be applied at least 1 hour before the procedure to be effective.
Choice D is wrong because Inject the immunizations into the deltoid muscle is not an answer because the deltoid muscle is not recommended for infants under 12 months of age.
A school nurse is assessing a 7-year-old student.
The nurse should identify which of the following findings as a potential indicator of physical abuse?
Explanation

Bruises in areas of the body not typically injured by accident or normal childhood activities can be a potential indicator of physical abuse.
Choice A is wrong because Weight in 45th percentile is not an answer because it falls within the normal range for weight.
Choice B is wrong because Abrasions on the knees are not an answer because they are a common injury in children and can occur during normal play.
Choice D is wrong because Front deciduous teeth missing is not an answer because it is normal for children to lose their deciduous teeth.
A nurse is planning to teach an adolescent who is lactose intolerant about dietary guidelines.
Which of the following instructions should the nurse include in the teaching?
Explanation
People with lactose intolerance can replace milk and dairy products with nondairy sources of calcium such as calcium-fortified products, fish with soft bones, broccoli and leafy green vegetables, oranges, almonds, Brazil nuts, and dried beans.
Choice A is wrong because “You can drink milk on an empty stomach” is not an answer because it may worsen symptoms of lactose intolerance.
Choice B is wrong because “You might tolerate plain milk better than chocolate milk” is not an answer because both plain and chocolate milk contain lactose.
Choice D is wrong because “You should consume flavored yogurt instead of plain yogurt” is not an answer because both flavored and plain yogurt contain lactose.
A nurse is prioritizing care for four clients.
Which of the following clients should the nurse assess first?
Explanation
An adolescent who has sickle cell anemia and slurred speech should be assessed first.
Slurred speech can be a sign of a stroke, which is a known complication of sickle cell anemia.
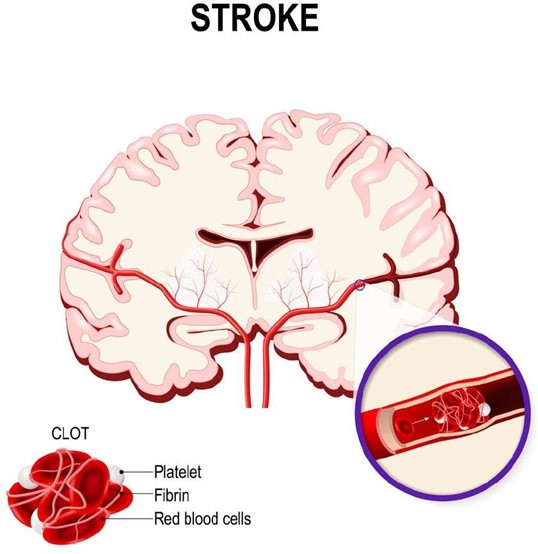
This requires immediate medical attention.
Choice B is wrong because while pain management is important, it is not as urgent as a potential stroke.
Choice C is wrong because while administering medication is important, it is not as urgent as a potential stroke.
Choice D is wrong because while wound care is important, it is not as urgent as a potential stroke.
A nurse in the emergency department is caring for a child who has a temperature of 39.1° C (102.4° F) and a suspected diagnosis of bacterial meningitis.
Which of the following actions should the nurse take first?
Explanation
The nurse should first implement droplet precautions for the child.
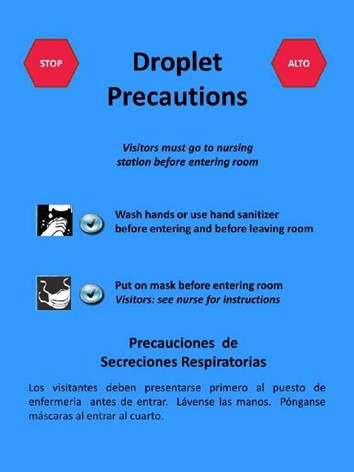
Bacterial meningitis can be spread through respiratory and throat secretions, so it is important to take precautions to prevent the spread of infection.
Choice A is wrong because while a lumbar puncture may be necessary for diagnosis, preventing the spread of infection is a higher priority.
Choice C is wrong because while dimming the lights may provide comfort, preventing the spread of infection is a higher priority.
Choice D is wrong because while administering an antipyretic may provide comfort, preventing the spread of infection is a higher priority.
A nurse in a provider's office is preparing to administer immunizations to a 12- year-old client during a well-child visit.
Which of the following immunizations should the nurse plan to administer?
Explanation
The nurse should plan to administer the human papillomavirus (HPV) vaccine to the 12-year-old client.

The Centers for Disease Control and Prevention (CDC) recommends that children aged 11-12 years old receive two doses of the HPV vaccine separated by 6-12 months.
Choice A is wrong because Hepatitis A vaccine is typically given to children at age.
Choice B is wrong because Varicella vaccine is typically given to children at ages 12-15 months and 4-6 years.
Choice C is wrong because DTaP vaccine is typically given to children at ages 2, 4, and 6 months, and between ages 15-18 months and 4-6 years.
A nurse is caring for an infant who has rotavirus.
Which of the following findings indicates that the infant is moderately dehydrated?
Explanation
A weight loss of 7% indicates that the infant is moderately dehydrated.

Dehydration is classified as mild (3-5% weight loss), moderate (6-10% weight loss), or severe (>10% weight loss)1.
Choice A is wrong because a respiratory rate of 28/min is within the normal range for an infant.
Choice B is wrong because a capillary refill time of 1 second is within the normal range.
Choice D is wrong because bradycardia (a slow heart rate) is not a typical sign of moderate dehydration in infants.
A nurse is assessing a school-age child who has heart failure and is taking furosemide.
Which of the following findings should the nurse identify as an indication that the medication is effective?
Explanation
A decrease in peripheral edema is an indication that the furosemide medication is effective.
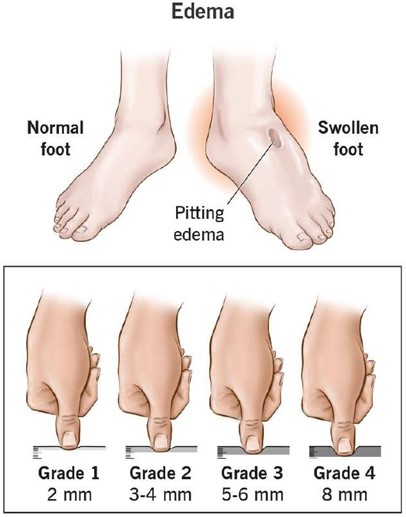
Furosemide is a diuretic that helps to reduce fluid buildup in the body, including peripheral edema, which is a common symptom of heart failure.
Choice B is wrong because furosemide does not directly decrease cardiac output.
Choice C is wrong because furosemide does not increase venous pressure.
Choice D is wrong because furosemide can actually cause a decrease in potassium levels, not an increase.
A nurse in a provider's office is assessing the vital signs of a 2-year-old child at a well-child visit.
Which of the following findings should the nurse report to the provider?
Explanation

According to the normal pediatric vital signs chart provided by Cleveland Clinic, the normal blood pressure range for a 2-year-old child should be between 90- 105/55-70 mm Hg. The blood pressure of 118/74 mm Hg is higher than the normal range for a 2- year-old child and should be reported to the provider.
Choice B is wrong because a respiratory rate of 26/min falls within the normal range of 20-30 breaths per minute for a child between ages 1 and.
Choice C is wrong because a pulse rate of 98/min falls within the normal range of 80-125 beats per minute for a child between ages 1 and.
Choice D is wrong because a temperature of 37.2° C (99° F) falls within the normal range for children which is around 98.6 degrees.
A nurse is providing teaching to the parents of a 2-month-old infant who has developmental dysplasia of the hip and has a prescription for a Pavlik harness.
Which of the following statements by the parents indicates an understanding of the teaching?
Explanation
According to UCSF Benioff Children’s Hospital Oakland Orthopaedic Department, you can change your baby’s diaper with the Pavlik harness in place and make sure the straps are kept outside of the diaper.
Choice A is wrong because while your child is being treated in the Pavlik harness, it is very important that you do not remove the harness or adjust the straps, unless you are given specific instructions by your doctor to do so.
Choice B is wrong because there are no instructions to apply lotion to the skin under the straps.
Choice D is wrong because the duration of treatment will be determined by your doctor and may vary.
A nurse is providing support to a family whose infant died from sudden infant death syndrome (SIDS).
Which of the following actions should the nurse take?
Explanation
Sudden infant death syndrome (SIDS) death has a devastating effect on parents.

There is no known cause, so parents experience guilt about what they might have done or not done to contribute to the death.
Acknowledging the family members’ feelings of guilt can help provide support to the family.
Choice A is wrong because there are no specific instructions discouraging the parents from allowing siblings to view the body.
Choice B is wrong because avoiding discussing details of the attempt to revive the infant may not necessarily provide support to the family.
Choice C is wrong because while providing a follow-up phone call 1 week following the infant’s death may be helpful, it is not the only action that should be taken by the nurse.
A nurse in a PACU is caring for a school-age child immediately following a tonsillectomy.
Which of the following actions should the nurse take?
Explanation

After a tonsillectomy surgery, it is important to place the child in a side-lying position to help keep their airway open and prevent aspiration 1.
Choice A is wrong because deep breathing and coughing may cause discomfort and bleeding after a tonsillectomy.
Choice B is wrong because while ice cream may be soothing for the throat, it is not the only food that can be offered when the child is alert.
Choice C is wrong because drinking fluids through a straw may cause discomfort and bleeding after a tonsillectomy.
A nurse is assessing a school-age child's cranial nerve function.
Which of the following actions should the nurse ask the child to take when assessing the accessory nerve?
Explanation
The accessory nerve is tested by evaluating the function of the trapezius and sternocleidomastoid muscles.
The trapezius muscle is tested by asking the patient to shrug their shoulders with and without resistance.
Choice A is wrong because following a light in the six cardinal positions tests the function of cranial nerves III, IV, and VI.
Choice B is wrong because moving their tongue in all directions tests the function of cranial nerve XII.
Choice C is wrong because showing their teeth while smiling tests the function of cranial nerve VII.
A nurse is caring for a 10-month-old child who was brought to the emergency department by his parents following a head injury.
Which of the following actions should the nurse take first?
Explanation
The first action the nurse should take is to assess the respiratory status of the infant.

After a head injury, it is important to ensure that the child’s airway is clear and that they are breathing adequately.
This is a crucial step in providing care for a patient with a head injury.
Choice B is wrong because inspecting for fluid leaking from the ears is not the first priority.
Choice C is wrong because examining the scalp for lacerations is not the first priority.
Choice D is wrong because checking pupil reactions is not the first priority.
A nurse is planning care for an 8-month-old infant who has heart failure. Which of the following actions should the nurse include in the plan of care?
Explanation
Infants with heart failure often present with breathing trouble1, and administering oxygen can help improve oxygen delivery.
Choice B is wrong because placing an infant in a prone position does not help with heart failure.
Choice C is wrong because if an infant vomits within 1 hour of administration of digoxin, the dosage should not be repeated without consulting a healthcare provider.
Choice D is wrong because infants with heart failure may have feeding issues and providing less frequent, higher volume feedings may not be helpful34.
A nurse is caring for an adolescent who is 1 hr postoperative following an appendectomy.
Which of the following findings should the nurse report to the provider?
Explanation
Muscle rigidity following an appendectomy could be a sign of a serious complication such as peritonitis and should be reported to the provider immediately.
Choice B is wrong because abdominal pain is a common occurrence following an appendectomy and may not necessarily require immediate attention from the provider.
Choice C is wrong because a temperature of 36.4° C (97.5° F) is within the normal range.
Choice D is wrong because a heart rate of 63/min is within the normal range for an adolescent.
A charge nurse is planning care for an infant who has failure to thrive. Which of the following actions should the nurse include in the plan of care?
Explanation
Consistent care from the same nursing staff can help establish a routine and build trust between the infant and caregivers.
Choice A is wrong because giving an infant fruit juice between feedings does not address the underlying causes of failure to thrive.
Choice B is wrong because using half-strength formula when feeding the infant can exacerbate the problem by providing insufficient nutrition.
Choice D is wrong because keeping the infant in a visually stimulating environment does not address the underlying causes of failure to thrive.
A nurse is caring for an infant who receives intermittent enteral feedings through a gastrostomy tube.
Which of the following actions should the nurse take when administering a feeding? (Select all that apply.).
Explanation

A. Offer the infant a pacifier during feedings.
B. Check for residual volumes by aspirating stomach contents.
D. Instill the formula over a period of 30 to 45 min.
Offering the infant a pacifier during feedings can help promote non-nutritive sucking and provide comfort to the infant.
Checking for residual volumes by aspirating stomach contents can help monitor gastric emptying and tolerance to enteral feeding.
Instilling the formula over a period of 30 to 45 min can help prevent overfeeding and reduce the risk of aspiration.
Choice C is wrong because placing the infant in a supine position during feedings increases the risk of aspiration.
The infant should be placed in an upright or semi-upright position during feedings.
Choice E is wrong because heating the formula to 39° C (102° F) prior to administration is not necessary and may even be harmful if the formula is overheated.
A nurse is caring for a school-age child following the application of a cast to a fractured right tibia.
Which of the following actions should the nurse take first?
Explanation
The first action the nurse should take is to elevate the child’s leg.

This is choice A. Elevating the child’s leg can help reduce swelling and improve circulation.
After elevating the child’s leg, the nurse can then administer pain medication (choice B), petal the edges of the cast (choice C), and teach the child about cast care (choice D).
Sign Up or Login to view all the 70 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
