ATI RN Paediatric Assessment 2022
Total Questions : 71
Showing 25 questions, Sign in for moreA nurse teaching the parents of a 10-month-old infant about home safety. Which of the following information should the nurse include in the teaching? (Select all that apply.)
Explanation
A. Set the water heater at 65.6° C (150° F):
Correct Answer: Incorrect.
Explanation: The recommended temperature for a water heater is around 49°C (120°F) to prevent burns. Setting it at 65.6°C (150°F) can lead to scald injuries.
B. Install accordion-style gates:
Correct Answer: Correct.
Explanation: Accordion-style gates can be used to block off certain areas and prevent the infant from accessing potentially dangerous areas like staircases. These gates are considered safe for use.
C. Fit the mattress so that it is snug against the sides of the crib:
Correct Answer: Incorrect.
Explanation: While it's essential to have a firm mattress in the crib, there should be no gaps between the mattress and the sides of the crib to prevent the risk of suffocation. The mattress should fit snugly, but there should be no spaces where the infant could get trapped.
D. Tie plastic bags in knots before discarding them:
Correct Answer: Incorrect.
Explanation: Tying plastic bags in knots can create a suffocation hazard. It's safer to keep plastic bags out of reach or securely dispose of them to avoid the risk of a child putting a bag over their head.
E. Serve food in small, non-circular pieces:
Correct Answer: Correct.
Explanation: Serving food in small, non-circular pieces reduces the risk of choking. Infants should be given age-appropriate foods to minimize the risk of choking, and cutting food into small, easy-to-manage pieces is recommended.
A parent of a 9-year-old child newly diagnosed with diabetes mellitus is very concerned about the child participating in social events at school. The nurse creating a plant of care would formulate which goals to address these concerns? Select all that apply.
Explanation
A. The child and family will integrate diabetes care into patterns of daily activity:
Correct Answer: Correct.
Explanation: Integrating diabetes care into daily activities helps the child manage their condition more effectively. This goal encourages normalization of the routine, making it easier for the child to participate in social events.
B. The child and family will discuss all aspects of the illness and its treatments:
Correct Answer: Correct.
Explanation: Open communication about the illness and its treatments is crucial for understanding and managing diabetes. This goal promotes family education and support, which can help alleviate concerns.
C. The child will use effective coping mechanisms to manage anxiety:
Correct Answer: Correct.
Explanation: Managing anxiety is important for overall well-being. Teaching the child effective coping mechanisms helps them navigate the emotional aspects of living with diabetes and participating in social events.
D. The child and family will discuss their concerns with the child's teachers and the school nurse:
Correct Answer: Correct.
Explanation: Communication with school personnel is essential to ensure a supportive environment for the child. Discussing concerns with teachers and the school nurse promotes awareness and collaboration in managing the child's diabetes at school.
E. The child's normal growth and development will be maintained:
Correct Answer: Correct.
Explanation: Maintaining normal growth and development is a crucial goal. It ensures that the child can engage in age-appropriate activities and social events while managing their diabetes effectively.
A nurse is caring for a 4-year-old child who has a new diagnosis of diabetes mellitus and is distressed after an insulin injection. Which of the following play activities should the nurse recognize is therapeutic in helping the child deal with the injection?
Explanation
A. A period of play in the playroom:
Incorrect: While play is generally therapeutic, simply engaging in general play may not directly address the child's distress related to the insulin injection.
B. A video game:
Incorrect: Playing a video game might serve as a distraction, but it may not specifically help the child cope with the distress of the injection in the way that hands-on play with a needleless syringe and a doll can.
C. A needleless syringe and a doll:
Correct Answer: Correct.
Explanation: Allowing the child to play with a needleless syringe and a doll provides a hands-on, interactive experience that can help the child become more familiar and comfortable with the idea of injections. This play activity allows the child to express and understand their feelings in a safe and controlled environment.
D. A story book about a child who has diabetes:
Incorrect: While a storybook can be educational and provide information, it may not directly address the child's immediate distress after an insulin injection. The hands-on play with a needleless syringe and a doll is more focused on the specific experience of receiving injections
The nurse caring for a child diagnosed with rubeola (measles) notes that the pediatrician has documented the presence of Koplik's spots. On the basis of this documentation, which observation is expected?
Explanation
A. Whitish vesicles located across the chest:
Incorrect: This description does not match the characteristic appearance or location of Koplik's spots in measles.
B. Small blue-white spots with a red base found on the buccal mucosa:
Correct Answer: Koplik's spots are small, blue-white spots with a red base that typically appear on the buccal mucosa (inner lining of the cheeks). These spots are characteristic of measles and are considered a diagnostic feature.
C. Pinpoint petechiae noted on both legs:
Incorrect: Petechiae are small, reddish-purple spots that result from bleeding under the skin. They are not characteristic of Koplik's spots in measles.
D. Petechiae spots that are reddish and pinpoint on the soft palate:
Incorrect: While petechiae can occur in various conditions, they are not characteristic of Koplik's spots in measles. Koplik's spots specifically manifest as small blue-white spots on the buccal mucosa.

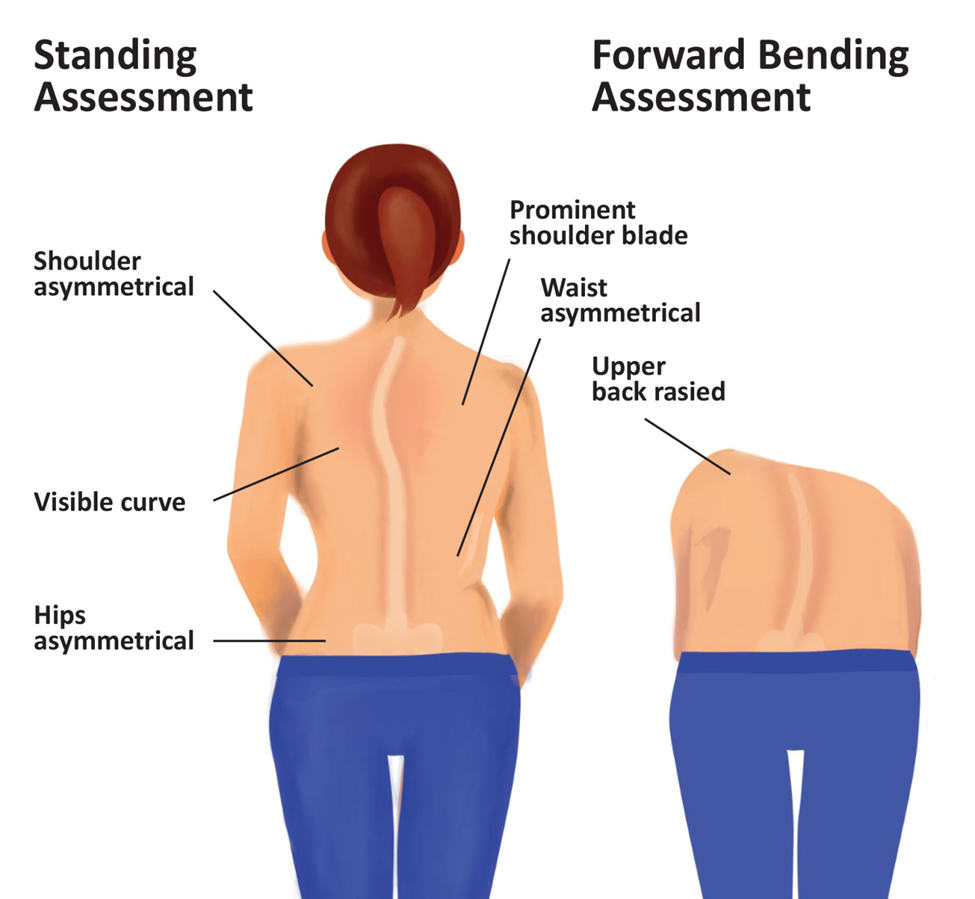
A school nurse is performing screening examinations for scoliosis. Which signs of scoliosis should the nurse assess for? Select all that apply.
Explanation
A. Lateral deviation and rotation of each vertebra:
Correct Answer: Correct.
Explanation: Scoliosis involves a lateral (side-to-side) curvature of the spine and often includes some degree of vertebral rotation. Assessing for these deviations is crucial in diagnosing scoliosis.
B. Equal rib prominences:
Correct Answer: Incorrect.
Explanation: In scoliosis, the ribs may appear more prominent on one side due to the lateral curvature of the spine. Therefore, equal rib prominences would not typically be observed in scoliosis.
C. Unequal rib heights:
Correct Answer: Correct.
Explanation: Unequal heights of the ribs are commonly seen in scoliosis due to the asymmetrical nature of the spine's curvature.
D. Chest asymmetry:
Correct Answer: Correct.
Explanation: Asymmetry in the chest area, including differences in the shape or appearance of the chest, can be indicative of scoliosis, especially when associated with the spinal curvature.
E. Equal shoulder heights:
Correct Answer: Incorrect.
Explanation: In scoliosis, one shoulder might appear higher than the other due to the lateral curvature of the spine. Therefore, equal shoulder heights would not typically be observed in scoliosis.
F. Equal waist angles:
Correct Answer: Incorrect.
Explanation: Scoliosis often causes an asymmetrical appearance of the waistline due to the lateral curvature of the spine, resulting in unequal waist angles rather than equal ones.
The nurse is assessing a child admitted with a diagnosis of rheumatic fever. Which significant question would the nurse ask the child's parent during the assessment?
Explanation
A. "Has your child been exposed to anyone with chicken pox?"
While chickenpox is caused by a different virus (varicella-zoster virus) and is not directly linked to rheumatic fever, the nurse might inquire about exposure to contagious illnesses as a general part of the assessment.
B. "Has any family member had a sore throat within the past few weeks?"
This question is relevant because rheumatic fever often follows an untreated or inadequately treated group A streptococcal infection, such as strep throat. A sore throat in a family member could indicate the presence of streptococcal infection, which is a crucial factor in the development of rheumatic fever.
C. "Has any family member had a gastrointestinal disorder in the past few weeks?"
Gastrointestinal disorders are not directly associated with the development of rheumatic fever. However, a comprehensive medical history might include questions about recent illnesses to understand the overall health context.
D. "Has your child had difficulty urinating?"
Difficulty urinating is not a typical symptom or risk factor associated with rheumatic fever. This symptom would likely prompt investigation into other potential issues but is not specifically related to rheumatic fever.
A nurse is caring for a child who is experiencing a seizure. Which of the following actions should the nurse take?
Explanation
A. Use a padded tongue blade:
Incorrect: Inserting anything into the child's mouth, including a padded tongue blade, is not recommended during a seizure. It can lead to oral and airway injuries. It's important to keep the airway clear, but this is achieved by positioning the child laterally.
B. Position the child laterally.
Correct Answer: This is the correct action. Placing the child on their side helps prevent aspiration of fluids and promotes a clear airway during the seizure. It also reduces the risk of injury.
C. Restrain the child's arms:
Incorrect: Restraining the child's arms can increase the risk of injury and is not recommended during a seizure. It's crucial to ensure a safe environment and prevent injury, but physically restraining the child is not the appropriate approach.
D. Attempt to stop the seizure:
Incorrect: It is not within the nurse's capacity to immediately stop a seizure. Seizures are neurological events, and they need to run their course. The focus should be on ensuring the safety of the child during the seizure.
The parent of a child with mumps calls the health care clinic to tell the nurse that the child has been lethargic and vomiting. What instruction would the nurse give to the parent?
Explanation
A. That lethargy and vomiting are normal with mumps:
Incorrect: Lethargy and vomiting are not typical symptoms of mumps. These symptoms could indicate a separate issue that requires medical attention.
B. To continue to monitor the child:
Incorrect: Given the reported symptoms of lethargy and vomiting, a passive approach of continuing to monitor may delay necessary medical intervention. The child should be assessed promptly.
C. To bring the child to the clinic to be seen by the pediatrician:
Correct Answer: Lethargy and vomiting are not typical symptoms of uncomplicated mumps. These symptoms could be indicative of other issues, and it's important for the pediatrician to evaluate the child to determine the cause and provide appropriate care.
D. That there is nothing to be concerned about as long as there is no fever:
Incorrect: While fever is a common symptom of mumps, the absence of fever does not negate the need for further evaluation when there are concerning symptoms like lethargy and vomiting. The child should be seen by a healthcare provider to determine the cause of these symptoms.
A nurse is caring for a 12-month-old toddler who is hospitalized and confined to a room with contact precautions in place. Which of the following toys should the nurse recommend in order to meet the developmental needs of the client?
Explanation
A. Crayons and a coloring book:
Incorrect: Crayons and coloring books may not be appropriate for a 12-month-old, as they may pose a choking hazard. Additionally, they might require more direct contact, which may not be ideal under contact precautions.
B. Modeling clay:
Incorrect: Modeling clay may also pose a choking hazard for a toddler. Moreover, it can be messy and may not be suitable for use in a hospital room with contact precautions.
C. Hanging crib toys.
Correct Answer: Hanging crib toys can provide visual and tactile stimulation for the toddler without the need for direct contact. These toys can be attached to the crib, allowing the child to engage with them safely.
D. Large building blocks:
Incorrect: While large building blocks can be suitable for a toddler's developmental needs, they may not be the best option in a confined hospital room under contact precautions. The child's access to and handling of the blocks may be limited in this setting.
The nurse is providing home-care instructions to a mother of a 12-month-old infant with mild diarrhea. Which would the nurse instruct the mother to do?
Explanation
A. Bottle-feed with diluted fruit juice:
Incorrect: Diluted fruit juice is not recommended for infants with diarrhea. Fruit juices, even when diluted, may contain sugars that can exacerbate diarrhea. It's important to focus on water or rehydration solutions.
B. Discontinue breast-feeding until the diarrhea resolves:
Incorrect: Breast milk is an essential source of nutrition for infants, and discontinuing breastfeeding is not recommended, even during episodes of mild diarrhea. Breast milk helps maintain hydration and provides essential nutrients.
C. Provide an increased intake of water.
Correct Answer: Maintaining hydration is crucial during episodes of diarrhea. Offering the infant increased water intake helps prevent dehydration. Rehydration solutions specifically designed for infants can also be recommended.
D. Avoid all solid foods:
Incorrect: While avoiding certain solid foods may be recommended in some cases, it's not necessary to completely avoid all solid foods for a 12-month-old with mild diarrhea. The emphasis should be on maintaining hydration and offering easily digestible foods.
The nurse is collecting data on a 2 month-old-child with left-sided congestive heart failure. Which clinical manifestation would support this diagnosis of left-sided congestive heart failure?
Explanation
A. Edema in the lower extremities:
Incorrect: Edema in the lower extremities is more characteristic of right-sided heart failure. In left-sided failure, pulmonary congestion is more prominent.
B. Ascites:
Incorrect: Ascites, or fluid accumulation in the abdominal cavity, is also more commonly associated with right-sided heart failure.
C. Shortness of breath:
Correct Answer: Left-sided congestive heart failure can lead to pulmonary congestion, resulting in difficulty breathing or shortness of breath. This is often observed as increased work of breathing, rapid breathing, or other signs of respiratory distress in infants.
D. Hepatomegaly:
Incorrect: Hepatomegaly, or enlargement of the liver, is another manifestation more commonly associated with right-sided heart failure.
A nurse is caring for a school-age child who has mild persistent asthma. Which of the following is an expected finding? (Select all that apply.)
Explanation
A. Symptoms are continuous throughout the day:
Incorrect: Continuous symptoms throughout the day are more indicative of moderate or severe persistent asthma, not mild persistent asthma.
B. Daytime symptoms occur more than twice a week:
Correct Answer: Children with mild persistent asthma may experience symptoms more than twice a week, but less than once a day.
C. Peak expiratory flow (PEF) is greater than or equal to 80% of the predicted value:
Incorrect: In mild persistent asthma, the peak expiratory flow (PEF) is generally between 80% and 100% of the predicted value. A PEF greater than or equal to 80% is expected in mild asthma, but it is not a specific finding for mild persistent asthma. It can be present in intermittent asthma as well.
D. Nighttime symptoms occur approximately twice a month:
Correct Answer: In mild persistent asthma, nighttime symptoms, such as coughing or wheezing, may occur approximately twice a month.
E. Minor limitations occur with normal activity:
Correct Answer: Children with mild persistent asthma may experience minor limitations in their normal activities. These limitations are not severe and do not significantly impact daily life.
A nurse is providing health promotion teaching to the parents of a toddler. Which of the following information should the nurse include in the teaching? (Select all that apply.)
Explanation
A. Need for increased caloric intake:
Incorrect: While toddlers may have specific nutritional needs, it is important to focus on a balanced diet rather than emphasizing increased caloric intake. The emphasis should be on providing nutritious and age-appropriate foods.
B. How to encourage cooperative play:
Correct Answer: Encouraging cooperative play is important for a toddler's social development. It involves teaching sharing, taking turns, and interacting with other children.
C. Management of tantrums:
Incorrect: While guidance on managing tantrums can be part of parenting education, it may not be the primary focus in health promotion teaching. The emphasis is typically on positive guidance, effective communication, and setting age-appropriate limits.
D. Dental care:
Correct Answer: Dental care is crucial for toddlers to promote oral health. The nurse should provide information on proper oral hygiene practices, including tooth brushing, and discuss the importance of regular dental check-ups.
E. How to establish trust:
Correct Answer: Establishing trust is a vital aspect of toddler development. The nurse can provide guidance on building a secure and trusting relationship between the child and parents.
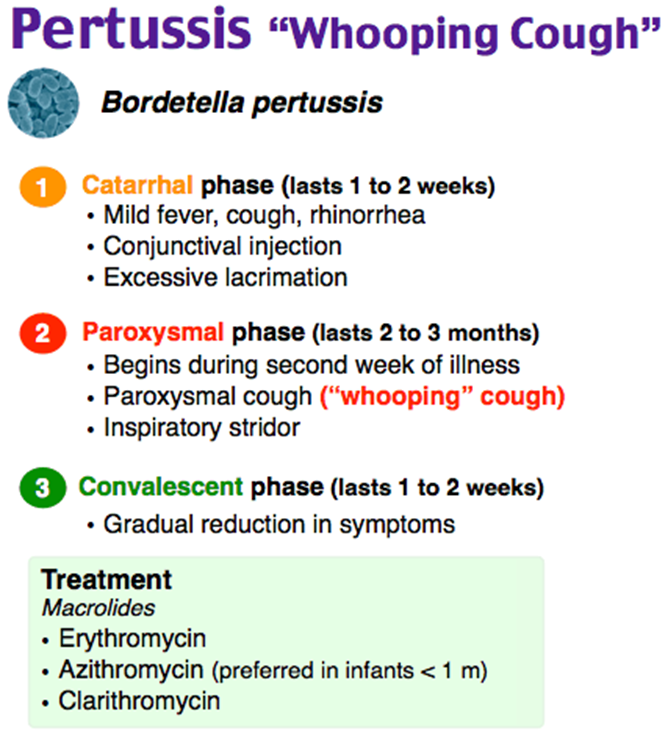
The nurse provides home care instructions to the parents of a child hospitalized with pertussis who is in the convalescent stage and is being prepared for discharge. Which statement by a parent indicates a need for further instruction?
Explanation
A. Coughing spells may be triggered by dust or smoke:
Incorrect: This is a correct statement. Irritants like dust or smoke can trigger coughing spells in a child recovering from pertussis.
B. We need to maintain droplet precautions and a quiet environment for at least 2 weeks.
Correct Answer: Pertussis is highly contagious during the catarrhal and paroxysmal stages, but once the child has reached the convalescent stage (usually after 2-4 weeks of illness), the risk of spreading the infection decreases significantly. Continuing strict droplet precautions and a quiet environment for two weeks after the convalescent stage is not necessary.
C. "We need to encourage our child to drink fluids":
Incorrect: This is a correct statement. Encouraging fluid intake is important to prevent dehydration, especially during coughing spells.
D. Vomiting may occur when our child has coughing episodes:
Incorrect: This is a correct statement. Vomiting can be a common occurrence during coughing episodes in pertussis due to the forceful nature of the cough. Parents should be aware of this symptom.
The parent of a 6-year-old child arrives at a clinic because the child has been experiencing itchy, red, and swollen eyes. The nurse notes a discharge from the eyes and sends a culture to the laboratory for analysis. Chlamydial conjunctivitis is diagnosed. On the basis of this diagnosis. the nurse determines that which requires further investigation?
Explanation
A. Possible sexual abuse.
Correct Answer: Chlamydial conjunctivitis in a child can raise concerns about possible sexual abuse. Chlamydia trachomatis, the bacterium responsible for chlamydial conjunctivitis, is commonly transmitted through contact with infected genital secretions. Therefore, the presence of chlamydial conjunctivitis in a child may warrant further investigation into the possibility of sexual abuse.
B. Possible trauma:
Incorrect: While trauma can cause eye-related symptoms, chlamydial conjunctivitis is specifically associated with an infection caused by Chlamydia trachomatis.
C. Presence of an allergy:
Incorrect: Allergic conjunctivitis may cause itchy, red, and swollen eyes, but chlamydial conjunctivitis is caused by a bacterial infection and is not related to allergies.
D. Presence of a respiratory infection:
Incorrect: Chlamydial conjunctivitis is not typically associated with respiratory infections. It is primarily caused by Chlamydia trachomatis and is more commonly linked to genital tract infections.
A school nurse identifies that a child has pediculosis capitis and educates the child's parents about the condition. Which of the following statements by the parents indicates an understanding of the teaching?
Explanation
A. "All recently used clothing, bedding, and towels must be washed in hot water."
Incorrect: While washing recently used clothing, bedding, and towels in hot water can help in controlling lice, this statement alone doesn't ensure complete eradication of lice or nits.
B. "My child must be free from nits before returning to school."
Correct Answer: This statement shows an understanding that children should be free from nits (lice eggs) before returning to school. Many schools have "no-nit" policies, requiring that children be free from both live lice and nits before re-entry.
C. "Toys that can't be dry cleaned or washed must be thrown out."
Incorrect: It's not necessary to throw out toys that cannot be cleaned. Lice cannot survive off the scalp for more than a day or two. Items that cannot be washed can be sealed in a plastic bag for two weeks to ensure any potential lice or nits die off.
D. "We will treat all the family members to be on the safe side."
Incorrect: Treating all family members is a common but not strictly necessary practice unless others show symptoms or evidence of head lice. It's recommended to focus treatment on those with live lice or nits.
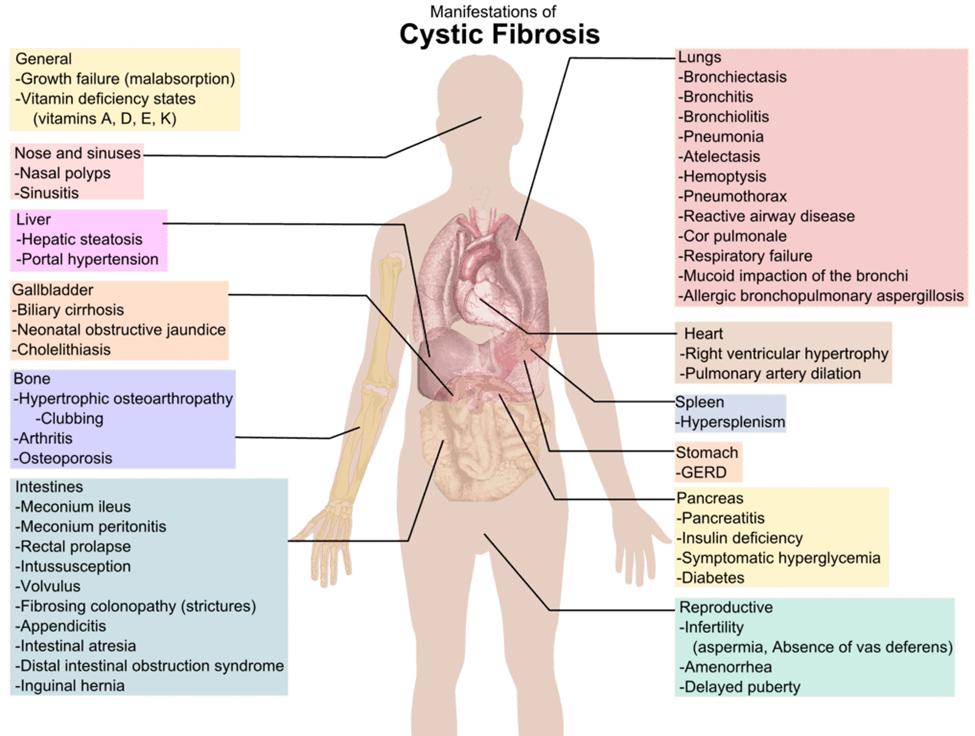
A nurse is providing discharge teaching about nutrition to the parents of a child who has cystic fibrosis (CF). Which of the following responses by the parents indicates an understanding of the teaching?
Explanation
A. "I will limit my child's fluid intake."
Incorrect: Limiting fluid intake is not typically recommended for children with CF. Maintaining hydration is important, especially since individuals with CF may have increased salt losses in sweat.
B. "We will give our child pancreatic enzymes with snacks and meals."
Correct Answer: This response indicates an understanding of the importance of giving pancreatic enzymes to assist with digestion, as individuals with CF often have pancreatic insufficiency. Pancreatic enzymes help in the absorption of nutrients from food.
C. "We will restrict the amount of salt in our child's food."
Incorrect: While it's true that individuals with CF may need to increase their salt intake due to increased salt losses in sweat, this response suggests restricting salt, which is not in line with the nutritional needs of a child with CF.
D. "I will prepare low-fat meals with limited protein for my child."
Incorrect: Children with CF often need a higher calorie intake, including healthy fats and adequate protein. Restricting fat and protein is not in line with the nutritional needs of a child with CF.
A nurse is caring for an infant who has gastroesophageal reflux. The nurse should recognize that which of the following findings are associated with this condition? (Select all that apply.)
Explanation
A. Fever:
Incorrect: Fever is not a typical symptom of uncomplicated gastroesophageal reflux. If fever is present, it may indicate another underlying condition.
B. Vomiting:
Correct Answer: Vomiting is a common symptom of gastroesophageal reflux in infants. It may occur shortly after feeding.
C. Rigid abdomen:
Incorrect: A rigid abdomen is not a common finding in uncomplicated gastroesophageal reflux. It may suggest another issue that needs evaluation.
D. Wheezing:
Correct Answer: Wheezing or respiratory symptoms can be associated with GER, especially if stomach contents are aspirated into the airways.
E. Weight loss:
Incorrect: Unexplained weight loss is not a typical finding in uncomplicated GER. If weight loss is occurring, it may be due to other underlying issues that need investigation.
A nurse is caring for a child who is on a clear liquid diet. At lunch, the child consumed ½ cup of juice, 3 oz gelatin, 1 oz of an ice pop, and 20 mL ginger ale. How many mL should the nurse record as the child's fluid intake?
Explanation
To calculate the total fluid intake, add the volumes of each item consumed:
Juice: ½ cup
1 cup = 240 mL
½ cup = 240 mL / 2 = 120 mL
Gelatin: 3 oz
1 oz ≈ 30 mL
3 oz = 3 * 30 mL = 90 mL
Ice pop: 1 oz
1 oz ≈ 30 mL
1 oz = 30 mL
Ginger ale: 20 mL
Now, add these values:
120 mL (juice) + 90 mL (gelatin) + 30 mL (ice pop) + 20 mL (ginger ale) = 260 mL
Therefore, the nurse should record 260 mL as the child's fluid intake.
The clinic nurse is providing instructions to the parent of a child with cystic fibrosis regarding the immunization schedule for the child. Which statement would the nurse make to the parent?
Explanation
A. "The immunization schedule will need to be altered."
Incorrect: This is too vague and does not provide specific information about the child's immunization schedule.
B. "The child will receive all of the immunizations except for the polio series."
Incorrect: There is no indication that the child should not receive the polio vaccine. Children with cystic fibrosis are generally recommended to receive all appropriate vaccinations.
C. "The child will receive the recommended basic series of immunizations along with a yearly influenza vaccination."
Correct Answer: Children with cystic fibrosis should receive the recommended basic series of immunizations, including vaccines for diseases such as diphtheria, pertussis, tetanus, measles, mumps, rubella, polio, Haemophilus influenzae type b (Hib), hepatitis B, and others. Additionally, they should receive a yearly influenza vaccination to help prevent respiratory complications.
D. "The child should not receive any hepatitis vaccines."
Incorrect: There is no general contraindication for children with cystic fibrosis to receive hepatitis vaccines. The nurse should recommend the appropriate vaccines, including those for hepatitis B, as per the standard immunization schedule.
A nurse is preparing to measure an infant's vital signs. The nurse should use which of the following sites to assess a heart rate?
Explanation
A. Brachial artery:
Incorrect: The brachial artery is commonly used for measuring blood pressure in infants but not for assessing heart rate.
B. Radial artery:
Incorrect: The radial artery is not typically used for assessing an infant's heart rate, especially in the clinical setting.
C. Carotid artery:
Incorrect: The carotid artery is not commonly used for assessing an infant's heart rate. It is more commonly used in adults, but in infants, the apex of the heart is the preferred site.
D. Apex of the heart.
Correct Answer: The apex of the heart is the most accurate site for counting an infant's heart rate. It is located at the point of maximum impulse (PMI), which is usually at the fifth intercostal space in the mid-clavicular line.
A nurse is preparing to administer vaccines to a 1-year-old child. Which of the following vaccines should the nurse give? (Select all that apply.)
Explanation
A. Varicella (VARI): Correct
Explanation: The varicella vaccine protects against chickenpox. The CDC recommends that children receive the first dose of the varicella vaccine at age 1.
B. Diphtheria, tetanus, and acellular pertussis (DTaP): Correct
Explanation: The DTaP vaccine protects against diphtheria, tetanus, and pertussis. The first dose is typically given at 2 months, with subsequent doses given at 4 months, 6 months, 15-18 months, and 4-6 years of age.
C. Human papillomavirus (HPV4): Incorrect
Explanation: The HPV vaccine is not typically administered at age 1. It is usually recommended for adolescents, starting around age 11 or 12. The HPV vaccine is given in a series of doses.
D. Measles, mumps, rubella (MMR): Correct
Explanation: The MMR vaccine protects against measles, mumps, and rubella. The first dose is usually given at age 1, with a second dose recommended at 4-6 years of age.
E. Rotavirus (RV): Incorrect
The rotavirus vaccine is usually given in a series of doses starting at 2 months of age, with the last dose administered by 8 months. It is not a vaccine that is typically given at age 1.
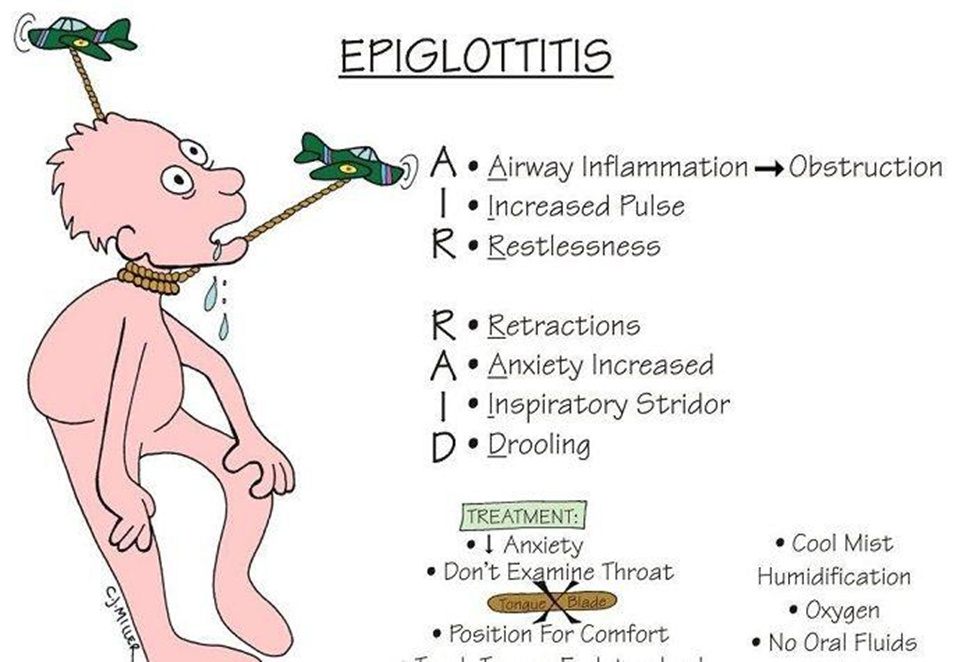
The nurse in the emergency department is caring for a child who appears extremely ill with a high fever, unable to control their oral secretions. with voice hoarseness and inspiratory stridor and inspiratory sternal retractions while breathing. The nurse suspects epiglottitis. Which would the nurse do next?
Explanation
A. Contact the assigned emergency room physician to evaluate the need for an advanced airway
Explanation:
Epiglottitis is a medical emergency that can rapidly progress to airway obstruction. The classic signs and symptoms include a high fever, difficulty swallowing, voice hoarseness, inspiratory stridor, and sternal retractions. Immediate intervention may be necessary to secure the airway. Therefore, contacting the emergency room physician to evaluate the need for an advanced airway (such as intubation) is a priority.
B. Administer intravenous corticosteroids
Explanation: While corticosteroids may be used in the management of epiglottitis to reduce airway inflammation, securing the airway is the priority in the acute phase. Corticosteroids would typically be administered after securing the airway.
C. Obtain a throat culture
Explanation: Obtaining a throat culture is not the immediate priority in the case of suspected epiglottitis. Prompt intervention to secure the airway takes precedence over diagnostic tests.
D. Inspect the throat to obtain further data to support the diagnosis
Explanation: Direct visualization of the throat (inspection) may exacerbate the airway obstruction and is not recommended in the acute management of suspected epiglottitis. The priority is to secure the airway while minimizing agitation and discomfort for the child. Diagnostic procedures, such as obtaining a throat culture, can be considered after the airway is stabilized.
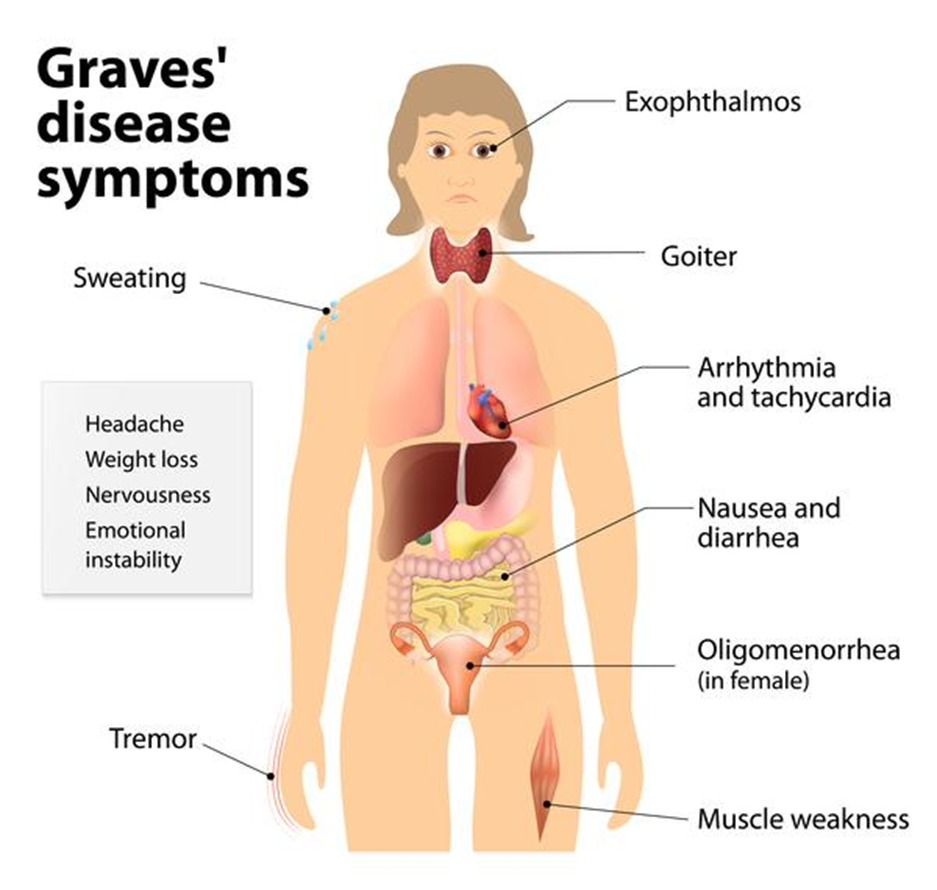
A nurse is assessing an adolescent who has an exacerbation of Graves' disease. Which of the following findings should the nurse expect?
Explanation
A. Heat intolerance
Explanation:
Graves' disease is an autoimmune disorder that results in hyperthyroidism, meaning there is an overproduction of thyroid hormones. Common symptoms of Graves' disease include heat intolerance, increased sweating, weight loss, palpitations, and anxiety. The hyperactivity of the thyroid gland leads to an increased metabolic rate, causing heat intolerance.
B. Bradycardia
Explanation: Bradycardia (slow heart rate) is not typically associated with Graves' disease. Hyperthyroidism usually leads to an increased heart rate (tachycardia) due to the stimulatory effects of thyroid hormones on the cardiovascular system.
C. Lethargy
Explanation: Lethargy (excessive tiredness or lack of energy) is more commonly associated with hypothyroidism, where there is an insufficient production of thyroid hormones. In Graves' disease, the excess thyroid hormones often lead to symptoms of hyperactivity, not lethargy.
D. Weight gain
Explanation: Weight gain is not a typical finding in Graves' disease. Hyperthyroidism often leads to unintentional weight loss due to increased metabolism and energy expenditure. Weight gain is more commonly associated with hypothyroidism.
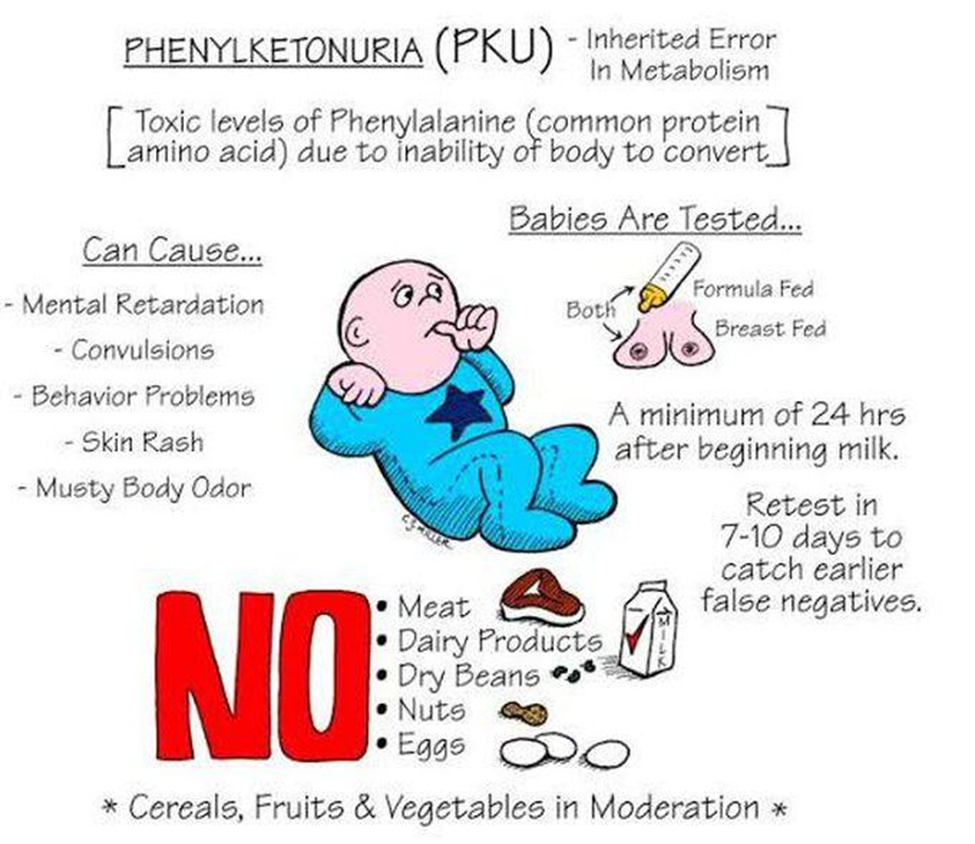
A parent brings a 2-week-old infant to a clinic for a phenylketonuria rescreening blood test. The test indicates a serum phenylalanine level of 1 mg/dL (60.5 mcmol/L). The nurse reviews this result and makes which interpretation?
Explanation
A. It is inconclusive
Explanation: A serum phenylalanine level within the normal range is considered conclusive in ruling out phenylketonuria. Inconclusive results typically occur when there are issues with the sample or testing process.
B. It is negative
Explanation:
A serum phenylalanine level of 1 mg/dL (60.5 mcmol/L) in a 2-week-old infant is within the normal range. In the context of phenylketonuria (PKU) screening, a "negative" result means that the phenylalanine levels are within the expected range, and there is no evidence of phenylketonuria.
C. It requires rescreening at age 6 weeks.
Explanation: If the initial screening result is within the normal range, rescreening at age 6 weeks may not be necessary for phenylketonuria. The timing and need for rescreening may vary based on local protocols and individual patient factors.
D. It is positive
Explanation: A positive result for phenylketonuria would indicate that the serum phenylalanine levels are elevated, suggesting a potential diagnosis of PKU. In this case, the result is negative, meaning there is no evidence of PKU.
Sign Up or Login to view all the 71 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
