ATI RN Pharmacology Exam
Total Questions : 50
Showing 25 questions, Sign in for moreWhich of the following are the five main rights of medication administration?(Select all that apply.)
Explanation
Choice A reason: The right route means that the medication is given through the appropriate and prescribed method, such as oral, intravenous, subcutaneous, intramuscular, etc. This ensures that the medication reaches the intended site of action and avoids complications or adverse effects.
Choice B reason: The right to refuse means that the patient has the autonomy and capacity to decline the medication after being informed of the benefits and risks. This is not one of the main rights of medication administration, but it is an ethical and legal principle that nurses should respect and document.
Choice C reason: The right dose means that the medication is given in the correct and safe amount, as prescribed by the doctor or authorized prescriber. This ensures that the medication achieves the desired therapeutic effect and prevents overdose or underdose.
Choice D reason: The right person means that the medication is given to the intended and identified patient, by checking their name, identification band, and other identifiers. This prevents medication errors and ensures patient safety and quality of care.
Choice E reason: The right documentation means that the medication is recorded accurately and timely in the patient's chart, medication administration record, or other relevant documents. This provides evidence of care, facilitates communication, and enables evaluation and monitoring of the medication's effectiveness and outcomes.
Choice F reason: The right medication means that the medication is given as prescribed, with the correct name and form. This prevents confusion and errors with lookalike or soundalike medications, and ensures that the patient receives the appropriate and intended drug.
A nurse is caring for a client with asthma who is prescribed metoprolol. The nurse should monitor the client for which of the following?
Explanation
Choice A reason: Increased respiratory rate is not a sign of adverse reaction to metoprolol, but rather a normal response to hypoxia or distress. Metoprolol is a betablocker that can lower the heart rate and blood pressure, but it does not affect the respiratory rate directly.
Choice B reason: Bronchodilation is not a sign of adverse reaction to metoprolol, but rather a desired effect of asthma medications such as betaagonists or anticholinergics. Metoprolol is a betablocker that can block the beta receptors in the lungs, which can cause bronchoconstriction or narrowing of the airways. This is why metoprolol is contraindicated or used with caution in clients with asthma.
Choice C reason: Decreased sputum production is not a sign of adverse reaction to metoprolol, but rather a result of effective asthma management. Metoprolol is a betablocker that does not have any direct effect on the mucus secretion or inflammation in the lungs.
Choice D reason: Wheezing is a sign of adverse reaction to metoprolol, as it indicates bronchoconstriction or narrowing of the airways. Metoprolol is a betablocker that can block the beta receptors in the lungs, which can reduce the bronchodilation effect of beta agonists or other asthma medications. This can worsen the asthma symptoms and cause wheezing, coughing, dyspnea, or chest tightness. The nurse should monitor the client for these signs and report them to the prescriber immediately.
A nurse prepares to replace the nearly empty container of total parenteral nutrition (TPN) for a client when she finds that there has been a delay in receiving the new container of solution from the pharmacy. Which of the following solutions should the nurse infuse until the next container of TPN solution becomes available?
Explanation
Choice A reason: 3% sodium chloride is a hypertonic solution that can cause fluid shifts and dehydration. It is not a suitable replacement for TPN, which is also hypertonic but provides calories, electrolytes, vitamins, and minerals. Infusing 3% sodium chloride can lead to hypernatremia, increased intracranial pressure, and cellular damage.
Choice B reason: Dextrose 10% in water is a hypertonic solution that can provide some calories and prevent hypoglycemia. It is the best option among the choices to replace TPN temporarily, until the new container arrives. However, it does not provide adequate nutrition or electrolytes, so it should not be used for a long time.
Choice C reason: Lactated Ringer's is an isotonic solution that can maintain fluid balance and electrolytes. It is not a suitable replacement for TPN, which is hypertonic and provides more calories and nutrients. Infusing Lactated Ringer's can lead to fluid overload, hyponatremia, and metabolic alkalosis.
Choice D reason: 0.9% sodium chloride is an isotonic solution that can maintain fluid balance and sodium levels. It is not a suitable replacement for TPN, which is hypertonic and provides more calories and nutrients. Infusing 0.9% sodium chloride can lead to fluid overload, hyponatremia, and metabolic acidosis.
The nurse is monitoring a client taking a potassium sparing diuretic. Which of the following findings would prompt the nurse to notify the health care provider?
Explanation
Choice A reason: Serum sodium level of 140 mEq/L is within the normal range of 135145 mEq/L. It does not indicate any adverse effect of the potassium sparing diuretic, which does not affect sodium excretion significantly. The nurse does not need to notify the health care provider about this finding.
Choice B reason: Blood pressure of 130/80 mmHg is slightly above the normal range of 120/80 mmHg, but it is not a cause for concern. The potassium sparing diuretic can lower the blood pressure by reducing the fluid volume and preventing sodium retention. The nurse should monitor the blood pressure regularly but does not need to notify the health care provider about this finding.
Choice C reason: Serum potassium level of 5.5 mEq/L is above the normal range of 3.55.0 mEq/L. It indicates hyperkalemia, which is a serious and potentially life-threatening complication of the potassium sparing diuretic. The potassium sparing diuretic can increase the potassium level by inhibiting its secretion in the distal tubule of the kidney. The nurse should notify the health care provider immediately and prepare to administer interventions such as calcium gluconate, insulin, or sodium bicarbonate to lower the potassium level and prevent cardiac arrhythmias.
Choice D reason: Serum potassium level of 3.5 mEq/L is at the lower end of the normal range of 3.55.0 mEq/L. It does not indicate any adverse effect of the potassium sparing diuretic, which does not cause potassium loss. The nurse does not need to notify the health care provider about this finding.
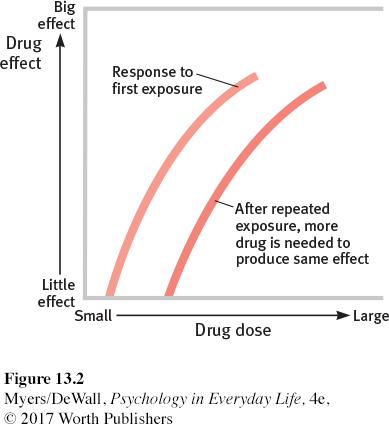
A patient who has been taking opioids for several weeks tells the nurse, "The medication doesn't seem to work as well anymore." The nurse recognizes this as a sign of:
Explanation
Choice A reason: Allergy is an immune mediated reaction to a substance that causes symptoms such as rash, itching, swelling, or anaphylaxis. It is not related to the duration or effectiveness of the medication. The patient does not report any signs of allergy to the opioids.
Choice B reason: Addiction is a chronic and compulsive disorder that involves seeking and using a substance despite harmful consequences. It is characterized by loss of control, craving, and impaired functioning. The patient does not show any signs of addiction to the opioids, such as increasing the dose, obtaining the medication illegally, or neglecting other responsibilities.
Choice C reason: Withdrawal is a syndrome that occurs when a substance is abruptly discontinued or reduced after prolonged use. It causes physical and psychological symptoms such as anxiety, agitation, sweating, nausea, or tremors. The patient does not experience any signs of withdrawal from the opioids, as they are still taking the medication as prescribed.
Choice D reason: Tolerance is a phenomenon that occurs when a substance loses its effectiveness over time due to repeated exposure. It requires higher doses or more frequent administration to achieve the same effect. The patient reports a sign of tolerance to the opioids, as they feel that the medication does not work as well anymore. The nurse should assess the patient's pain level, monitor the opioid dose, and consult with the prescriber about possible adjustments or alternatives.
The nurse is preparing to administer Reglan to a patient. She is most concerned by the following information in the patient's medical record?
Explanation
Choice A reason: Past medical history of benign prostatic hyperplasia (BPH) is not a contraindication or a concern for administering Reglan, which is a medication that stimulates the motility of the upper gastrointestinal tract and treats nausea, heartburn, and gastroparesis¹. Reglan does not affect the prostate or urinary function.
Choice B reason: Blood pressure of 132/82 is slightly above the normal range of 120/80, but it is not a cause for concern or a reason to withhold Reglan. Reglan can lower the blood pressure by reducing the fluid volume and preventing sodium retention¹. The nurse should monitor the blood pressure regularly, but does not need to notify the health care provider about this finding.
Choice C reason: Allergy to corn is a concern for administering Reglan, as some formulations of Reglan may contain corn starch as an inactive ingredient. Corn starch can trigger an allergic reaction in people who are sensitive to corn, causing symptoms such as rash, itching, swelling, or anaphylaxis. The nurse should check the label of the Reglan product and avoid using it if it contains corn starch. The nurse should also notify the health care provider and the pharmacy about the patient's allergy and request an alternative medication or formulation.
Choice D reason: Past medical history of gout is not a contraindication or a concern for administering Reglan, which is a medication that stimulates the motility of the upper gastrointestinal tract and treats nausea, heartburn, and gastroparesis¹. Reglan does not affect the uric acid levels or the joints.
A patient is prescribed Flexeril (cyclobenzaprine) for muscle spasms. Which of the following is the most common side effect that the nurse should educate the patient about?
Explanation
Choice A reason: Tinnitus is a rare side effect of Flexeril, which is a medication that relaxes the muscles and relieves pain and stiffness¹. Tinnitus is a ringing or buzzing sound in the ears that can be caused by various factors, such as ear infections, noise exposure, or certain medications. Flexeril does not affect the auditory system directly, but it can cause confusion or dizziness, which may worsen the perception of tinnitus.
Choice B reason: Drowsiness is the most common side effect of Flexeril, which is a medication that relaxes the muscles and relieves pain and stiffness¹. Drowsiness occurs because Flexeril has sedative and anticholinergic properties, which means that it blocks the action of acetylcholine, a neurotransmitter that regulates arousal and alertness. Flexeril can impair the mental and physical abilities, especially in elderly patients or those who take other medications that cause drowsiness¹. The nurse should educate the patient about the risk of drowsiness and advise them to avoid driving or operating machinery while taking Flexeril.
Choice C reason: Diarrhea is not a common side effect of Flexeril, which is a medication that relaxes the muscles and relieves pain and stiffness¹. Diarrhea is a condition that causes loose or watery stools, which can be caused by various factors, such as infections, food intolerance, or certain medications. Flexeril does not affect the gastrointestinal system directly, but it can cause dry mouth, nausea, or constipation, which may alter the bowel movements¹.
Choice D reason: Palpitations are not a common side effect of Flexeril, which is a medication that relaxes the muscles and relieves pain and stiffness¹. Palpitations are a sensation of rapid or irregular heartbeat, which can be caused by various factors, such as stress, anxiety, caffeine, or certain medications. Flexeril does not affect the cardiac system directly, but it can lower the blood pressure or interact with other medications that affect the heart rate, such as betablockers or antidepressants¹.
A patient with renal impairment is prescribed a medication that is primarily excreted by the kidneys. What adjustment should the nurse anticipate?
Explanation
Choice A reason: Administering the medication with meals only is not a valid adjustment for a medication that is primarily excreted by the kidneys. The food intake does not affect the renal clearance of the drug, unless it alters the pH of the urine or the blood flow to the kidneys. The nurse should follow the instructions on the medication label or the prescriber's order regarding the timing of the administration.
Choice B reason: No dose adjustment is required is an incorrect statement for a medication that is primarily excreted by the kidneys. The renal impairment can reduce the elimination of the drug and increase its concentration in the blood. This can cause adverse effects and toxicity. The nurse should consult with the prescriber or the pharmacist about the appropriate dose reduction or frequency change for the patient's level of renal function.
Choice C reason: Increasing the dose to ensure therapeutic effect is a dangerous and inappropriate adjustment for a medication that is primarily excreted by the kidneys. The renal impairment can reduce the elimination of the drug and increase its concentration in the blood. This can cause adverse effects and toxicity. The nurse should not increase the dose without the prescriber's order and should monitor the patient for signs of overdose or toxicity.
Choice D reason: Decreasing the dose to prevent toxicity is the correct and rational adjustment for a medication that is primarily excreted by the kidneys. The renal impairment can reduce the elimination of the drug and increase its concentration in the blood. This can cause adverse effects and toxicity. The nurse should consult with the prescriber or the pharmacist about the appropriate dose reduction or frequency change for the patient's level of renal function. The nurse should also monitor the patient for the therapeutic response and the adverse effects of the drug.
When educating a patient about Lorazepam (Ativan), the nurse should advise against the concurrent use of which substance?
Explanation
Choice A reason: Vitamin C supplements are not a concern for the concurrent use with Lorazepam, which is a medication that reduces anxiety and insomnia by enhancing the effects of a neurotransmitter called gammaaminobutyric acid (GABA) in the brain¹. Vitamin C is an essential nutrient that supports the immune system and the synthesis of collagen, a protein that forms the connective tissue in the body. Vitamin C does not interact with Lorazepam or affect its metabolism or clearance.
Choice B reason: Caffeinated beverages are not a concern for the concurrent use with Lorazepam, but they may reduce its effectiveness or cause unwanted effects. Caffeine is a stimulant that increases the activity of the central nervous system and counteracts the sedative and calming effects of Lorazepam. Caffeine may also cause side effects such as nervousness, insomnia, or palpitations, especially in high doses or in sensitive individuals. The nurse should advise the patient to limit or avoid caffeine intake while taking Lorazepam, and to monitor their response to the medication.
Choice C reason: Alcohol is a concern for the concurrent use with Lorazepam, as it can increase the risk of serious and potentially fatal side effects. Alcohol is a depressant that slows down the activity of the central nervous system and enhances the effects of Lorazepam. Alcohol can cause additive effects such as excessive sedation, respiratory depression, coma, or death when taken with Lorazepam. The nurse should advise the patient to avoid alcohol consumption while taking Lorazepam, and to seek immediate medical attention if they experience any signs of overdose or toxicity.
Choice D reason: Dairy products are not a concern for the concurrent use with Lorazepam, as they do not affect its absorption, distribution, metabolism, or excretion. Dairy products are a source of calcium, protein, and other nutrients that support the bone health and the muscle function. Dairy products do not interact with Lorazepam or alter its pharmacokinetics or pharmacodynamics.
The nurse is caring for a patient diagnosed with asthma on a medical surgical unit. The nurse is concerned when the patient makes the following statement after completing their Albuterol nebulizer treatment:
Explanation
Choice A reason: "I am not ready to eat lunch yet." is not a concerning statement for the patient who has completed their Albuterol nebulizer treatment. Albuterol is a medication that relaxes the muscles in the airways and increases the airflow to the lungs, which can improve the breathing and reduce the wheezing in patients with asthma¹. Albuterol does not affect the appetite or the digestion directly, but it may cause some side effects such as nausea, vomiting, or dry mouth, which may reduce the desire to eat. The nurse should respect the patient's preference and offer them food later when they are ready.
Choice B reason: "It feels like my heart is racing." is a concerning statement for the patient who has completed their Albuterol nebulizer treatment. Albuterol is a medication that relaxes the muscles in the airways and increases the airflow to the lungs, but it also stimulates the beta receptors in the heart, which can increase the heart rate and the blood pressure¹. This can cause side effects such as palpitations, chest pain, or arrhythmias, especially in patients with underlying heart conditions or those who take other medications that affect the heart. The nurse should monitor the patient's vital signs, report the finding to the prescriber, and prepare to administer interventions such as betablockers or calcium channel blockers to lower the heart rate and prevent complications.
Choice C reason: "It is easier to breathe now." is not a concerning statement for the patient who has completed their Albuterol nebulizer treatment. Albuterol is a medication that relaxes the muscles in the airways and increases the airflow to the lungs, which can improve the breathing and reduce the wheezing in patients with asthma¹. This is the expected and desired outcome of the Albuterol nebulizer treatment, which indicates that the medication is effective and the patient is responding well. The nurse should document the patient's response and continue to assess the patient's respiratory status and oxygen saturation.
Choice D reason: "I can breathe better now." is not a concerning statement for the patient who has completed their Albuterol nebulizer treatment. Albuterol is a medication that relaxes the muscles in the airways and increases the airflow to the lungs, which can improve the breathing and reduce the wheezing in patients with asthma¹. This is the expected and desired outcome of the Albuterol nebulizer treatment, which indicates that the medication is effective and the patient is responding well. The nurse should document the patient's response and continue to assess the patient's respiratory status and oxygen saturation.
A nurse is administering codeine cough syrup to a patient for a dry cough. This medication is a Schedule V medication. Which of the following measures should the nurse take?
Explanation
Choice A reason: Monitor the patient for addiction is not a necessary measure for the nurse to take when administering codeine cough syrup, which is a medication that suppresses the cough reflex by acting on the brain¹. Codeine is a Schedule V medication, which means that it has a low potential for abuse and dependence compared to other opioids. The nurse should follow the prescriber's order and the label instructions and use the lowest effective dose for the shortest duration. The nurse should also assess the patient's pain level, respiratory status, and cough frequency and severity.
Choice B reason: Advise the patient that the medication helps to thin out their secretions is an incorrect statement for the nurse to make when administering codeine cough syrup, which is a medication that suppresses the cough reflex by acting on the brain¹. Codeine does not affect the viscosity or production of the mucus in the airways, but rather reduces the urge to cough. The nurse should advise the patient to drink plenty of fluids, use a humidifier, or use saline nasal spray to help loosen and clear the secretions.
Choice C reason: Advise the patient to minimize intake of beets is not a relevant measure for the nurse to take when administering codeine cough syrup, which is a medication that suppresses the cough reflex by acting on the brain¹. Beets are a vegetable that are rich in antioxidants, fiber, and nitrates, which can lower blood pressure and improve blood flow. Beets do not interact with codeine or affect its metabolism or clearance. The nurse should encourage the patient to eat a balanced and nutritious diet, unless they have any dietary restrictions or allergies.
Choice D reason: Advise the patient that constipation is an adverse effect of the medication is the correct and appropriate measure for the nurse to take when administering codeine cough syrup, which is a medication that suppresses the cough reflex by acting on the brain¹. Codeine can also act on the opioid receptors in the gastrointestinal tract, which can reduce the peristalsis and cause constipation. The nurse should advise the patient to prevent or treat constipation by increasing their fluid and fiber intake, exercising regularly, and using laxatives or stool softeners as needed.
A nurse is providing discharge teaching to a client who has asthma and new prescriptions for Albuterol and Atrovent, both by nebulizer. Which of the following statements by the client indicates an understanding of the teaching?
Explanation
Choice A reason: "If my breathing begins to feel tight, I will use the cromolyn immediately." is an incorrect statement for the client who has asthma and new prescriptions for Albuterol and Atrovent, both by nebulizer. Cromolyn is a medication that prevents the release of inflammatory substances from the mast cells in the airways, which can cause bronchospasm and asthma symptoms¹. Cromolyn is not a rescue medication, but a maintenance medication that should be used regularly to prevent asthma attacks. The client should use Albuterol, a short acting beta agonist, to relieve acute bronchospasm and wheezing.
Choice B reason: "I will be sure to take the albuterol before taking the Atrovent." is a correct statement for the client who has asthma and new prescriptions for Albuterol and Atrovent, both by nebulizer. Albuterol is a medication that relaxes the muscles in the airways and increases the airflow to the lungs, which can improve the breathing and reduce the wheezing in patients with asthma. Atrovent is a medication that blocks the action of acetylcholine, a neurotransmitter that causes bronchoconstriction and mucus secretion, which can worsen the asthma symptoms. The client should take the Albuterol before the Atrovent, as this will allow the Albuterol to open the airways and enhance the absorption and effectiveness of the Atrovent.
Choice C reason: "I will administer the medications 10 minutes apart." is an unnecessary statement for the client who has asthma and new prescriptions for Albuterol and Atrovent, both by nebulizer. The client does not need to wait 10 minutes between the administration of the two medications, as they can be given together in the same nebulizer chamber. This will save time and simplify the treatment regimen for the client. The client should follow the instructions on the medication label or the prescriber's order regarding the dosage and frequency of the nebulizer treatments.
Choice D reason: "I will use both medications immediately after exercising." is an inappropriate statement for the client who has asthma and new prescriptions for Albuterol and Atrovent, both by nebulizer. The client should not use both medications immediately after exercising, as this may not prevent or relieve exercise induced bronchospasm, a condition that causes the airways to narrow during or after physical activity. The client should use Albuterol, a short acting beta agonist, before exercising, as this will prevent the bronchospasm and allow the client to exercise safely and comfortably. The client should use Atrovent, an anticholinergic, as prescribed, usually twice a day, to control the chronic symptoms of asthma.
The nurse is caring for a client who is taking metformin (Glucophage) for hyperglycemia prior to admission. The nurse would question the following order for this client:
Explanation
Choice A reason: CT scan with contrast is an order that the nurse should question for the client who is taking metformin for hyperglycemia. Metformin is a medication that lowers the blood glucose level by decreasing the hepatic glucose production and increasing the insulin sensitivity¹. Metformin can cause a rare but serious complication called lactic acidosis, which is a buildup of lactic acid in the blood that can cause symptoms such as weakness, nausea, vomiting, or breathing problems. CT scan with contrast involves injecting iodinated contrast material into the bloodstream, which can affect the kidney function and increase the risk of lactic acidosis in patients taking metformin. The nurse should consult with the prescriber and the pharmacist about the need to stop metformin before and after the CT scan with contrast, and to monitor the kidney function and the blood glucose level of the client.
Choice B reason: Chest X-ray 1 view is not an order that the nurse should question for the client who is taking metformin for hyperglycemia. Chest X-ray is a diagnostic test that uses a small amount of radiation to produce images of the lungs, heart, and chest wall. Chest X-ray does not involve any contrast material or affect the kidney function or the blood glucose level. The nurse should follow the standard precautions and procedures for performing a chest X-ray, such as verifying the client's identity, checking for pregnancy, removing any metal objects, and positioning the client properly.
Choice C reason: V/Q scan is not an order that the nurse should question for the client who is taking metformin for hyperglycemia. V/Q scan is a diagnostic test that measures the ventilation and perfusion of the lungs, and can detect any abnormalities such as pulmonary embolism or chronic obstructive pulmonary disease. V/Q scan involves injecting a radioactive tracer into the bloodstream and inhaling a radioactive gas, which are then detected by a special camera. V/Q scan does not affect the kidney function or the blood glucose level. The nurse should follow the standard precautions and procedures for performing a V/Q scan, such as verifying the client's identity, checking for allergies, explaining the procedure, and monitoring the vital signs.
Choice D reason: Bilateral lower extremity ultrasound is not an order that the nurse should question for the client who is taking metformin for hyperglycemia. Bilateral lower extremity ultrasound is a diagnostic test that uses sound waves to produce images of the blood vessels in the legs, and can detect any abnormalities such as deep vein thrombosis or peripheral arterial disease. Bilateral lower extremity ultrasound does not involve any contrast material or affect the kidney function or the blood glucose level. The nurse should follow the standard precautions and procedures for performing a bilateral lower extremity ultrasound, such as verifying the client's identity, explaining the procedure, and applying a gel and a probe to the legs.
The nurse is monitoring a client taking Lasix (furosemide). Which of the following findings would prompt the nurse to notify the health care provider?
Explanation
Choice A reason: Serum potassium level of 5.5 mEq/L is above the normal range of 3.55.0 mEq/L, but it is not a concern for the client taking Lasix, which is a medication that increases the urine output and lowers the blood pressure by inhibiting the reabsorption of sodium and water in the kidney. Lasix can also cause the loss of potassium in the urine, which can lead to hypokalemia, a condition that causes muscle weakness, cramps, arrhythmias, or cardiac arrest. The nurse should monitor the serum potassium level and administer potassium supplements or potassium sparing diuretics as prescribed to prevent hypokalemia.
Choice B reason: Blood pressure of 130/80 mmHg is slightly above the normal range of 120/80 mmHg, but it is not a concern for the client taking Lasix, which is a medication that increases the urine output and lowers the blood pressure by inhibiting the reabsorption of sodium and water in the kidney. Lasix can reduce the fluid volume and the peripheral resistance, which can lower the blood pressure and prevent or treat hypertension, edema, or heart failure. The nurse should monitor the blood pressure regularly and adjust the dose of Lasix as prescribed to maintain a normal blood pressure.
Choice C reason: Serum potassium level of 3.0 mEq/L is below the normal range of 3.55.0 mEq/L, and it is a concern for the client taking Lasix, which is a medication that increases the urine output and lowers the blood pressure by inhibiting the reabsorption of sodium and water in the kidney. Lasix can also cause the loss of potassium in the urine, which can lead to hypokalemia, a condition that causes muscle weakness, cramps, arrhythmias, or cardiac arrest. The nurse should notify the health care provider immediately and prepare to administer interventions such as potassium supplements or potassium sparing diuretics to correct hypokalemia.
Choice D reason: Serum sodium level of 140 mEq/L is within the normal range of 135145 mEq/L, and it is not a concern for the client taking Lasix, which is a medication that increases the urine output and lowers the blood pressure by inhibiting the reabsorption of sodium and water in the kidney. Lasix can cause the loss of sodium in the urine, which can lead to hyponatremia, a condition that causes confusion, seizures, coma, or death. The nurse should monitor the serum sodium level and administer sodium supplements or fluids as prescribed to prevent hyponatremia.
A nurse is providing teaching for a client who has a new prescription for an antibiotic. Which of the following statements should the nurse make?
Explanation
Choice A reason: "Antibiotics are administered to treat viral infections." is an incorrect statement for the nurse to make when providing teaching for a client who has a new prescription for an antibiotic. Antibiotics are medicines that fight bacterial infections in people and animals. They work by killing the bacteria or by making it hard for the bacteria to grow and multiply. Antibiotics do not work against viruses, such as those that cause colds, flu, or COVID19. Taking antibiotics when they are not needed can cause harm and increase the risk of antibiotic resistance¹.
Choice B reason: "Bloody stools are expected while taking antibiotics." is an incorrect statement for the nurse to make when providing teaching for a client who has a new prescription for an antibiotic. Bloody stools are not a normal or expected side effect of antibiotics. They can indicate a serious condition, such as intestinal bleeding, ulcerative colitis, or Clostridioides difficile infection. C. diff is a type of bacteria that can cause severe diarrhea, abdominal pain, and bloody stools. It can occur when antibiotics disrupt the normal balance of bacteria in the gut and allow C. diff to grow and produce toxins. The nurse should instruct the client to report any signs of bloody stools or severe diarrhea to the health care provider immediately.
Choice C reason: "Take the entire course of antibiotics as prescribed." is a correct statement for the nurse to make when providing teaching for a client who has a new prescription for an antibiotic. Taking the entire course of antibiotics as prescribed is important to ensure that the infection is completely treated and to prevent the bacteria from becoming resistant to the antibiotic. Stopping the antibiotic too soon or skipping doses can allow some bacteria to survive and multiply, which can cause the infection to come back or spread to other parts of the body. The nurse should also remind the client to follow the instructions on the medication label or the prescriber's order regarding the dosage, frequency, and duration of the antibiotic therapy.
Choice D reason: "Discontinue the medication when you feel better." is an incorrect statement for the nurse to make when providing teaching for a client who has a new prescription for an antibiotic. Discontinuing the medication when the client feels better is not advisable, as it can lead to incomplete treatment and antibiotic resistance. Feeling better does not mean that the infection is gone or that the bacteria are all killed. The client should continue to take the antibiotic until the end of the prescribed course, even if they have no symptoms or feel better. The nurse should also advise the client to contact the health care provider if they have any questions or concerns about the antibiotic or if they experience any side effects or allergic reactions.

Which of the following interventions is most appropriate for a nurse to perform prior to administering Lasix to a client with heart failure?
Explanation
Choice A reason: Advise the client to avoid highfiber foods with the medication is not an appropriate intervention for a nurse to perform prior to administering Lasix to a client with heart failure. Lasix is a medication that increases the urine output and lowers the blood pressure by inhibiting the reabsorption of sodium and water in the kidney. Lasix does not interact with highfiber foods or affect the digestion directly. Highfiber foods can actually help prevent or treat constipation, which can be a side effect of Lasix. The nurse should encourage the client to eat a balanced and nutritious diet, unless they have any dietary restrictions or allergies.
Choice B reason: Encourage the client to consume a potassium rich diet is not an appropriate intervention for a nurse to perform prior to administering Lasix to a client with heart failure. Lasix is a medication that increases the urine output and lowers the blood pressure by inhibiting the reabsorption of sodium and water in the kidney. Lasix can also cause the loss of potassium in the urine, which can lead to hypokalemia, a condition that causes muscle weakness, cramps, arrhythmias, or cardiac arrest. The nurse should monitor the serum potassium level and administer potassium supplements or potassiumsparing diuretics as prescribed to prevent hypokalemia. Consuming a potassium rich diet may not be sufficient or safe to correct the potassium imbalance caused by Lasix, especially in clients with kidney impairment or other medications that affect the potassium level.
Choice C reason: Assess the client’s respiratory rate and oxygen saturation is the most appropriate intervention for a nurse to perform prior to administering Lasix to a client with heart failure. Lasix is a medication that increases the urine output and lowers the blood pressure by inhibiting the reabsorption of sodium and water in the kidney. Lasix can help reduce the fluid overload and congestion in the lungs, which can cause shortness of breath, difficulty breathing, fatigue, and low oxygen levels in clients with heart failure. The nurse should assess the client’s respiratory rate and oxygen saturation to evaluate the severity of the pulmonary edema and the effectiveness of the Lasix therapy. The nurse should also monitor the client’s vital signs, fluid intake and output, and weight to ensure adequate fluid balance and hemodynamic stability.
Choice D reason: Instruct the client to increase fluid intake to prevent dehydration is not an appropriate intervention for a nurse to perform prior to administering Lasix to a client with heart failure. Lasix is a medication that increases the urine output and lowers the blood pressure by inhibiting the reabsorption of sodium and water in the kidney. Lasix can cause dehydration, which can lead to symptoms such as thirst, dry mouth, dark urine, and fatigue. However, increasing fluid intake to prevent dehydration can worsen the fluid overload and congestion in the lungs, which can cause shortness of breath, difficulty breathing, fatigue, and low oxygen levels in clients with heart failure. The nurse should advise the client to drink enough fluids to maintain hydration, but not to exceed the prescribed fluid restriction, which is usually around 1.52 liters per day. The nurse should also educate the client about the signs and symptoms of dehydration and fluid overload, and when to seek medical attention.
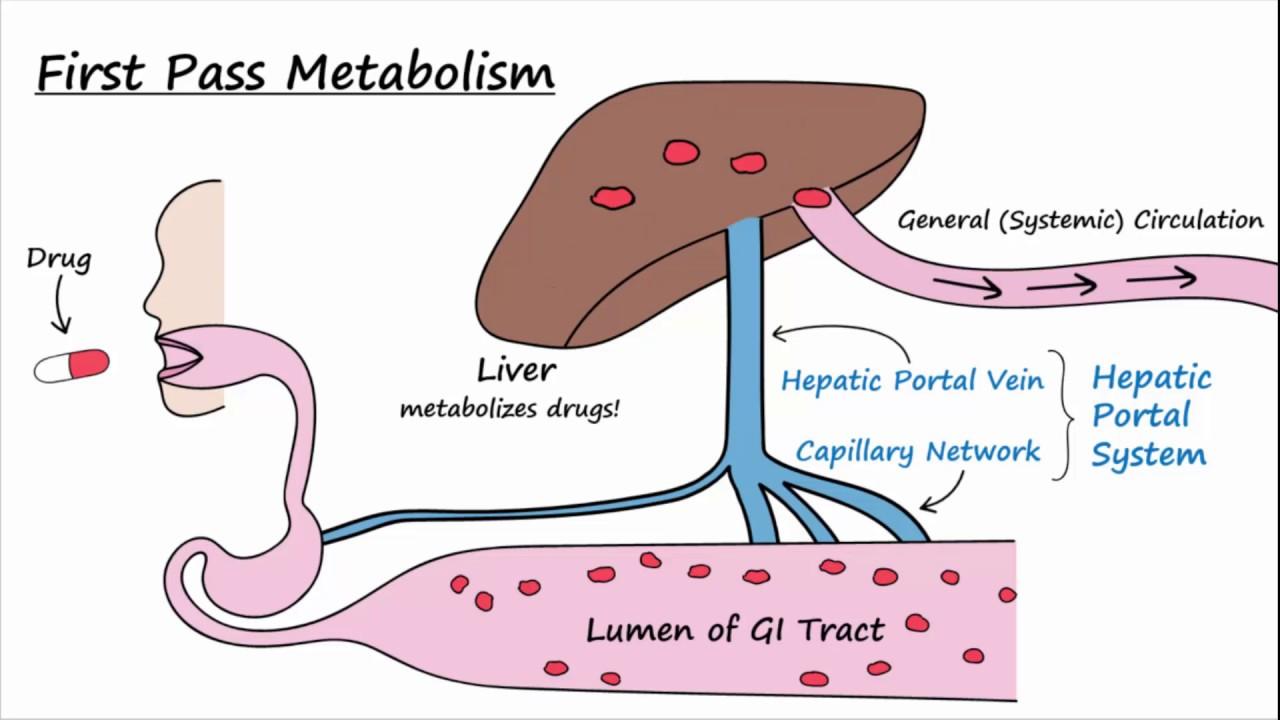
What does the term 'first pass effect' refer to?
Explanation
Choice A reason: The initial phase of drug distribution is not the correct definition of the term 'first pass effect'. Drug distribution is the process by which a drug moves from the bloodstream to the tissues and organs of the body. The initial phase of drug distribution is influenced by factors such as blood flow, tissue permeability, plasma protein binding, and tissue binding. The first pass effect is not related to drug distribution, but to drug metabolism, which is the chemical transformation of a drug in the body.
Choice B reason: The rapid absorption of a drug in the intestine is not the correct definition of the term 'first pass effect'. Drug absorption is the process by which a drug enters the bloodstream from the site of administration. The rapid absorption of a drug in the intestine depends on factors such as the drug formulation, the pH of the gastrointestinal tract, the presence of food or other drugs, and the surface area and motility of the intestine. The first pass effect is not related to drug absorption, but to drug metabolism, which is the chemical transformation of a drug in the body.
Choice C reason: The initial rapid excretion of a drug through the urinary system is not the correct definition of the term 'first pass effect'. Drug excretion is the process by which a drug or its metabolites are eliminated from the body. The initial rapid excretion of a drug through the urinary system is influenced by factors such as the renal blood flow, the glomerular filtration rate, the tubular secretion and reabsorption, and the urine pH. The first pass effect is not related to drug excretion, but to drug metabolism, which is the chemical transformation of a drug in the body.
Choice D reason: The metabolism of a drug before it reaches the systemic circulation is the correct definition of the term 'first pass effect'. Drug metabolism is the process by which a drug is chemically transformed in the body, usually by enzymes in the liver or other tissues. The first pass effect is a phenomenon of drug metabolism that occurs when a drug is administered orally and passes through the gastrointestinal tract and the liver before reaching the systemic circulation. The first pass effect can reduce the bioavailability and the effectiveness of the drug, as some or most of the drug may be metabolized and inactivated before reaching the site of action.
A nurse is preparing to administer atropine to a patient with symptomatic bradycardia. Which of the following is the primary therapeutic effect of atropine in this scenario?
Explanation
Choice A reason: Vasodilation is not the primary therapeutic effect of atropine in this scenario. Atropine is a medication that blocks the action of acetylcholine, a neurotransmitter that stimulates the parasympathetic nervous system. Atropine can cause vasodilation by inhibiting the muscarinic receptors on the blood vessels, which normally cause vasoconstriction. However, this effect is not significant or consistent, and it does not improve the symptoms of bradycardia, which is a slow heart rate that can cause dizziness, fatigue, or fainting. The nurse should monitor the blood pressure and the peripheral pulses of the patient after administering atropine.
Choice B reason: Bronchodilation is not the primary therapeutic effect of atropine in this scenario. Atropine is a medication that blocks the action of acetylcholine, a neurotransmitter that stimulates the parasympathetic nervous system. Atropine can cause bronchodilation by inhibiting the muscarinic receptors on the bronchial smooth muscle, which normally cause bronchoconstriction. However, this effect is not relevant or beneficial for the patient with symptomatic bradycardia, who does not have any respiratory problems. The nurse should assess the respiratory rate and the breath sounds of the patient after administering atropine.
Choice C reason: Increase in heart rate is the primary therapeutic effect of atropine in this scenario. Atropine is a medication that blocks the action of acetylcholine, a neurotransmitter that stimulates the parasympathetic nervous system. Atropine can increase the heart rate by inhibiting the muscarinic receptors on the sinoatrial node and the atrioventricular node, which normally slow down the heart rate. This effect is desirable and beneficial for the patient with symptomatic bradycardia, who has a slow heart rate that can cause dizziness, fatigue, or fainting. The nurse should monitor the electrocardiogram and the heart rate of the patient after administering atropine.
Choice D reason: Diuresis is not the primary therapeutic effect of atropine in this scenario. Atropine is a medication that blocks the action of acetylcholine, a neurotransmitter that stimulates the parasympathetic nervous system. Atropine can cause diuresis by inhibiting the muscarinic receptors on the bladder, which normally promote urination. However, this effect is not important or helpful for the patient with symptomatic bradycardia, who does not have any urinary problems. The nurse should measure the urine output and the specific gravity of the patient after administering atropine.
A nurse is providing teaching to a client who has asthma and a new prescription for inhaled fluticasone. Which of the following instructions should the nurse provide?
Explanation
Choice A reason: Limit caffeine intake is not an instruction that the nurse should provide to the client who has asthma and a new prescription for inhaled fluticasone. Fluticasone is a medication that reduces inflammation and swelling in the airways, which can improve breathing and prevent asthma attacks. Fluticasone does not interact with caffeine or affect the heart rate or blood pressure. Caffeine is a stimulant that can cause nervousness, insomnia, or palpitations in some people, but it does not worsen asthma symptoms or interfere with fluticasone therapy. The nurse should advise the client to consume caffeine in moderation and avoid it before bedtime.
Choice B reason: Take the medication with meals is not an instruction that the nurse should provide to the client who has asthma and a new prescription for inhaled fluticasone. Fluticasone is a medication that reduces inflammation and swelling in the airways, which can improve breathing and prevent asthma attacks. Fluticasone is administered by inhalation, not by mouth, and it does not affect the digestion or absorption of food. The nurse should instruct the client to use the inhaler as prescribed, usually twice a day, regardless of the mealtimes.
Choice C reason: Rinse the mouth after administration is an instruction that the nurse should provide to the client who has asthma and a new prescription for inhaled fluticasone. Fluticasone is a medication that reduces inflammation and swelling in the airways, which can improve breathing and prevent asthma attacks. Fluticasone is a corticosteroid, which can cause side effects such as oral thrush, hoarseness, or sore throat if it remains in the mouth after inhalation. The nurse should instruct the client to rinse the mouth with water and spit it out after each dose of fluticasone to prevent these side effects. The nurse should also teach the client how to use the inhaler properly and check the inhaler technique regularly.
Choice D reason: Check the pulse after medication administration is not an instruction that the nurse should provide to the client who has asthma and a new prescription for inhaled fluticasone. Fluticasone is a medication that reduces inflammation and swelling in the airways, which can improve breathing and prevent asthma attacks. Fluticasone does not affect the heart rate or blood pressure, and it is not a rescue medication that should be used for acute asthma symptoms. The nurse should monitor the respiratory rate and the oxygen saturation of the client after administering fluticasone and advise the client to use a short acting bronchodilator, such as albuterol, for quick relief of wheezing or shortness of breath.
A nurse is preparing to administer phenylephrine as a vasopressor to treat a patient for hypotension. The desired therapeutic effect of phenylephrine in this context is:
Explanation
Choice A reason: Vasoconstriction is the desired therapeutic effect of phenylephrine in this context. Phenylephrine is a medication that stimulates the alpha1 receptors on the blood vessels, causing them to constrict or narrow. This increases the resistance to blood flow and raises the blood pressure. Phenylephrine is used as a vasopressor to treat hypotension, which is a condition of low blood pressure that can cause dizziness, fainting, or organ damage. The nurse should monitor the blood pressure and the peripheral pulses of the patient after administering phenylephrine.
Choice B reason: Bronchodilation is not the desired therapeutic effect of phenylephrine in this context. Phenylephrine is a medication that stimulates the alpha1 receptors on the blood vessels, causing them to constrict or narrow. It has no effect on the beta2 receptors on the bronchial smooth muscle, which are responsible for bronchodilation or widening of the airways. Phenylephrine is not used to treat respiratory conditions, such as asthma or chronic obstructive pulmonary disease, that cause bronchoconstriction or narrowing of the airways. The nurse should assess the respiratory rate and the breath sounds of the patient after administering phenylephrine.
Choice C reason: Diuresis is not the desired therapeutic effect of phenylephrine in this context. Phenylephrine is a medication that stimulates the alpha1 receptors on the blood vessels, causing them to constrict or narrow. It has no effect on the kidney function or the urine output. Phenylephrine is not used to treat fluid retention or edema, which are conditions of excess fluid in the body that can cause swelling, weight gain, or heart failure. The nurse should measure the urine output and the specific gravity of the patient after administering phenylephrine.
Choice D reason: Decreased heart rate is not the desired therapeutic effect of phenylephrine in this context. Phenylephrine is a medication that stimulates the alpha1 receptors on the blood vessels, causing them to constrict or narrow. It has little or no effect on the beta1 receptors on the heart, which are responsible for increasing the heart rate and the contractility. Phenylephrine may actually cause a reflex bradycardia, which is a slow heart rate that occurs when the baroreceptors in the blood vessels sense an increase in blood pressure and send signals to the brain to lower the heart rate. Phenylephrine is not used to treat tachycardia, which is a fast heart rate that can cause palpitations, chest pain, or arrhythmias. The nurse should monitor the electrocardiogram and the heart rate of the patient after administering phenylephrine.
The nurse is caring for a client diagnosed with beta lactam resistant bacteria. The nurse anticipates administering which broad spectrum antibiotic?
Explanation
Choice A reason: Ancef (ciprofloxacin) is not the correct answer for the nurse who anticipates administering a broad-spectrum antibiotic to a client diagnosed with a beta lactam resistant bacteria. Ancef is the brand name of cefazolin, which is a firstgeneration cephalosporin, a subclass of beta lactam antibiotics. Cefazolin is effective against gram-positive bacteria, but has limited activity against gram negative bacteria and anaerobes. Cefazolin is also susceptible to beta-lactamase enzymes, which are produced by some bacteria to degrade beta lactam antibiotics and confer resistance. The nurse should avoid using Ancef or any other beta lactam antibiotic for a client with a beta lactam resistant bacteria.
Choice B reason: Merrem (meropenem) is the correct answer for the nurse who anticipates administering a broad-spectrum antibiotic to a client diagnosed with a beta lactam resistant bacteria. Merrem is the brand name of meropenem, which is a carbapenem, a subclass of beta lactam antibiotics. Meropenem is effective against a wide range of bacteria, including gram-positive, gram negative, and anaerobic bacteria. Meropenem is also resistant to most beta-lactamase enzymes, except for metallo-beta-lactamase’s, which are rare and can be detected by laboratory tests. The nurse should consider using Merrem or another carbapenem for a client with a beta lactam resistant bacteria, unless they have a history of allergy or intolerance to beta lactam antibiotics .
Choice C reason: Flagyl (metronidazole) is not the correct answer for the nurse who anticipates administering a broad spectrum antibiotic to a client diagnosed with a beta lactam resistant bacteria. Flagyl is the brand name of metronidazole, which is a nitroimidazole antibiotic. Metronidazole is effective against anaerobic bacteria and some protozoa, but has no activity against aerobic bacteria. Metronidazole is not a beta lactam antibiotic, and it is not affected by beta-lactamase enzymes. However, metronidazole is not a broad spectrum antibiotic, and it is not suitable for treating infections caused by aerobic bacteria, which are more common than anaerobic bacteria. The nurse should use Flagyl only for specific indications, such as bacterial vaginosis, trichomoniasis, or Clostridioides difficile infection .
Choice D reason: Zosyn (piperacillin tazobactam) is not the correct answer for the nurse who anticipates administering a broad-spectrum antibiotic to a client diagnosed with a beta lactam resistant bacterium. Zosyn is the brand name of piperacillin tazobactam, which is a combination of penicillin, a subclass of beta lactam antibiotics, and a beta-lactamase inhibitor. Piperacillin is effective against some gram-positive and gram-negative bacteria, but it is susceptible to beta-lactamase enzymes. Tazobactam is a compound that binds to and inhibits some beta-lactamase enzymes, thereby protecting piperacillin from degradation and extending its spectrum of activity. However, piperacillin tazobactam is not effective against all types of beta-lactamase enzymes, especially those that are encoded by plasmids and can be transferred between bacteria. The nurse should not use Zosyn or any other beta lactam/beta-lactamase inhibitor combination for a client with a beta lactam resistant bacterium unless the specific type of beta-lactamase is known and susceptible to the inhibitor.
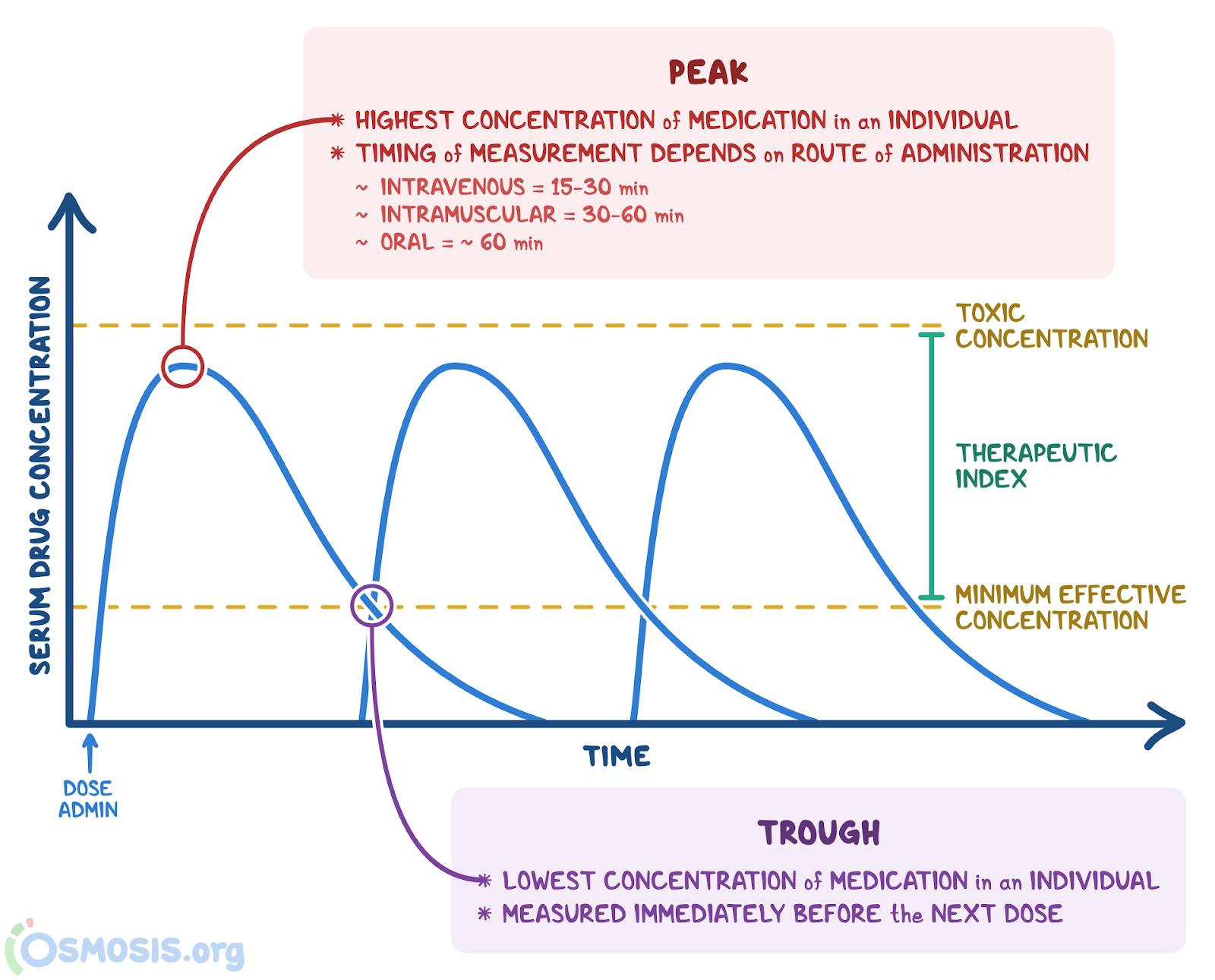
What term is used to describe the highest concentration of a drug in the blood after it is administered?
Explanation
Choice A reason: Peak level is the correct term to describe the highest concentration of a drug in the blood after it is administered. Peak level is also known as peak plasma concentration or Cmax, and it reflects the rate and extent of drug absorption. Peak level is influenced by factors such as the route of administration, the dose, the formulation, and the bioavailability of the drug. Peak level is important to monitor for drugs that have a narrow therapeutic range, meaning that there is a small difference between the effective and toxic doses. The nurse should measure the peak level at the appropriate time after the drug administration, and adjust the dose or the frequency as needed to achieve the desired therapeutic effect and avoid adverse effects .
Choice B reason: Halflife is not the correct term to describe the highest concentration of a drug in the blood after it is administered. Halflife is the time it takes for the concentration of a drug in the blood to decrease by 50%. Halflife reflects the rate of drug elimination, which depends on factors such as the metabolism and excretion of the drug. Halflife is important to determine the dosing interval and the time to reach steady state. The nurse should consider the halflife of the drug when prescribing or administering the drug, and avoid drug accumulation or subtherapeutic levels .
Choice C reason: Trough level is not the correct term to describe the highest concentration of a drug in the blood after it is administered. Trough level is the lowest concentration of a drug in the blood before the next dose is given. Trough level reflects the balance between drug absorption and elimination, and it indicates the minimum effective concentration of the drug. Trough level is important to monitor for drugs that have a narrow therapeutic range, meaning that there is a small difference between the effective and toxic doses. The nurse should measure the trough level just before the next dose of the drug, and adjust the dose or the frequency as needed to achieve the desired therapeutic effect and avoid adverse effects .
Choice D reason: Steady state is not the correct term to describe the highest concentration of a drug in the blood after it is administered. Steady state is the condition when the rate of drug administration is equal to the rate of drug elimination, and the concentration of the drug in the blood remains constant. Steady state is usually reached after four to five halflives of the drug, and it reflects the optimal therapeutic level of the drug. Steady state is important to maintain for drugs that have a long halflife or a narrow therapeutic range, meaning that there is a small difference between the effective and toxic doses. The nurse should ensure that the drug is administered at regular intervals and at the appropriate dose to achieve and maintain steady state.
A nurse is teaching a client about taking diphenhydramine. The nurse should explain to the client that which of the following is an adverse effect of this medication?
Explanation
Choice A reason: Bradycardia is not an adverse effect of diphenhydramine. Diphenhydramine is a medication that blocks the action of histamine, a chemical that causes allergic reactions and inflammation. Diphenhydramine can also block the action of acetylcholine, a neurotransmitter that stimulates the parasympathetic nervous system. Diphenhydramine does not affect the heart rate or blood pressure significantly, and it is not associated with bradycardia, which is a slow heart rate that can cause dizziness, fatigue, or fainting. The nurse should monitor the vital signs of the client after administering diphenhydramine, but bradycardia is not a common or expected outcome.
Choice B reason: Sedation is an adverse effect of diphenhydramine. Diphenhydramine is a medication that blocks the action of histamine, a chemical that causes allergic reactions and inflammation. Diphenhydramine can also block the action of acetylcholine, a neurotransmitter that stimulates the parasympathetic nervous system. Diphenhydramine can cross the bloodbrain barrier and block the histamine receptors in the brain, which are involved in regulating the sleepwake cycle and alertness. Diphenhydramine can cause sedation, sleepiness, drowsiness, dizziness, and impaired coordination, which can affect the performance and safety of the client. The nurse should instruct the client to avoid driving, operating machinery, or performing other tasks that require mental alertness after taking diphenhydramine, and to take the medication at bedtime or as needed for sleep.
Choice C reason: Constipation is not an adverse effect of diphenhydramine. Diphenhydramine is a medication that blocks the action of histamine, a chemical that causes allergic reactions and inflammation. Diphenhydramine can also block the action of acetylcholine, a neurotransmitter that stimulates the parasympathetic nervous system. Diphenhydramine does not affect the gastrointestinal motility or secretion significantly, and it is not associated with constipation, which is a condition of infrequent or difficult bowel movements. The nurse should encourage the client to eat a balanced and highfiber diet, drink plenty of fluids, and exercise regularly to prevent or treat constipation, but diphenhydramine is not a contributing factor.
Choice D reason: Hypertension is not an adverse effect of diphenhydramine. Diphenhydramine is a medication that blocks the action of histamine, a chemical that causes allergic reactions and inflammation. Diphenhydramine can also block the action of acetylcholine, a neurotransmitter that stimulates the parasympathetic nervous system. Diphenhydramine does not affect the blood pressure or the vascular tone significantly, and it is not associated with hypertension, which is a condition of high blood pressure that can cause headaches, chest pain, or stroke. The nurse should monitor the blood pressure of the client after administering diphenhydramine, but hypertension is not a common or expected outcome.
Which phase of pharmacokinetics involves the movement of a drug from its site of administration to the bloodstream?
Explanation
Choice A reason: Distribution is not the correct term to describe the movement of a drug from its site of administration to the bloodstream. Distribution is the process by which a drug moves from the bloodstream to the tissues and organs of the body. Distribution depends on factors such as blood flow, tissue permeability, plasma protein binding, and tissue binding. Distribution occurs after the drug has been absorbed into the bloodstream, and it determines how much drug reaches the site of action.
Choice B reason: Metabolism is not the correct term to describe the movement of a drug from its site of administration to the bloodstream. Metabolism is the process by which a drug is chemically transformed in the body, usually by enzymes in the liver or other tissues. Metabolism can affect the activity, duration, and elimination of a drug. Metabolism occurs after the drug has been absorbed into the bloodstream, and it can occur before or after the drug reaches the site of action.
Choice C reason: Excretion is not the correct term to describe the movement of a drug from its site of administration to the bloodstream. Excretion is the process by which a drug or its metabolites are eliminated from the body. Excretion can occur through various routes, such as urine, feces, sweat, or breath. Excretion occurs after the drug has been absorbed into the bloodstream, and it can occur before or after the drug reaches the site of action.
Choice D reason: Absorption is the correct term to describe the movement of a drug from its site of administration to the bloodstream. Absorption is the process by which a drug enters the bloodstream from the site of administration. Absorption depends on factors such as the route of administration, the dose, the formulation, and the bioavailability of the drug. Absorption is the first step of pharmacokinetics, and it determines how much and how fast a drug reaches the bloodstream and the site of action.
Escitalopram (Lexapro) belongs to which class of medications?
Explanation
Choice A reason: Monoamine oxidase inhibitors (MAOIs) are not the correct class of medications to which escitalopram (Lexapro) belongs. MAOIs are a group of antidepressants that work by inhibiting the enzyme monoamine oxidase, which breaks down neurotransmitters such as serotonin, norepinephrine, and dopamine. MAOIs can increase the levels of these neurotransmitters in the brain and improve mood and energy. However, MAOIs can also cause serious side effects and interactions with other drugs and foods, and they are not commonly used as firstline treatment for depression. Escitalopram is not an MAOI, and it should not be taken with MAOIs or within 14 days of stopping or starting MAOIs, as this can cause a dangerous drug interaction called serotonin syndrome.
Choice B reason: Betablockers are not the correct class of medications to which escitalopram (Lexapro) belongs. Betablockers are a group of drugs that work by blocking the beta receptors on the heart and blood vessels, which are stimulated by adrenaline and noradrenaline. Betablockers can lower the heart rate, blood pressure, and cardiac output, and they are used to treat conditions such as hypertension, angina, arrhythmias, and heart failure. Betablockers can also reduce anxiety and tremors, but they are not antidepressants and they do not affect serotonin levels. Escitalopram is not a betablocker, and it does not have any significant effect on the cardiovascular system.
Choice C reason: Benzodiazepines are not the correct class of medications to which escitalopram (Lexapro) belongs. Benzodiazepines are a group of drugs that work by enhancing the activity of the neurotransmitter gammaaminobutyric acid (GABA), which has a calming and sedating effect on the brain. Benzodiazepines are used to treat anxiety, insomnia, seizures, and muscle spasms, and they can also cause relaxation, drowsiness, and amnesia. Benzodiazepines are not antidepressants and they do not affect serotonin levels. Escitalopram is not a benzodiazepine, and it does not have any significant effect on GABA receptors .
Choice D reason: Selective serotonin reuptake inhibitors (SSRIs) are the correct class of medications to which escitalopram (Lexapro) belongs. SSRIs are a group of antidepressants that work by blocking the reuptake of serotonin by the nerve cells, which increases the availability of serotonin in the synaptic cleft. Serotonin is a neurotransmitter that regulates mood, appetite, sleep, and cognition, and low levels of serotonin are associated with depression and anxiety. SSRIs can improve the symptoms of depression and anxiety by enhancing the serotonin signaling in the brain. Escitalopram is an SSRI, and it is used to treat major depressive disorder and generalized anxiety disorder.
Sign Up or Login to view all the 50 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
