Custom ati maternity exam 2
Total Questions : 23
Showing 23 questions, Sign in for moreThe nurse is assisting in the care of a client who is in active labor. The nurse notes late decelerations on the fetal monitor tracing. Which of the following actions should the nurse take first?
Explanation
Choice A reason: This is incorrect. Increasing the infusion rate of the IV fluid is not the first action the nurse should take. IV fluid can help increase the blood volume and improve the placental perfusion, but it is not the most effective way to relieve the uteroplacental insufficiency that causes late decelerations. It may also cause fluid overload or edema in the mother or the fetus.
Choice B reason: This is correct. Positioning the client on her side is the first action the nurse should take. Lateral position can reduce the compression of the inferior vena cava and the aorta by the gravid uterus, which can improve the maternal and fetal circulation. It can also enhance the uterine blood flow and oxygen delivery to the fetus, which can prevent or correct fetal hypoxia.
Choice C reason: This is incorrect. Administering oxygen via face mask is not the first action the nurse should take. Oxygen can increase the oxygen saturation and the partial pressure of oxygen in the maternal blood, which can benefit the fetus. However, it is not the most immediate way to address the cause of late decelerations, which is the reduced blood flow to the placenta. It may also have adverse effects, such as hyperoxia or oxidative stress.
Choice D reason: This is incorrect. Elevating the client's legs is not the first action the nurse should take. Elevating the legs can help increase the venous return and the cardiac output, which can improve the maternal and fetal hemodynamics. However, it is not the most urgent way to resolve the problem of late decelerations, which is the impaired placental function. It may also worsen the compression of the major vessels by the uterus, which can decrease the blood flow to the placenta.
A nurse is assisting with the care of a client who is in the first stage of labor. The nurse observes the umbilical cord protruding from the vagina. Which of the following actions should the nurse take first?
Explanation
Choice A reason: This is incorrect. Covering the cord with a sterile, moist saline dressing is not the first action the nurse should take. This can help prevent the cord from drying out and becoming infected, but it does not address the main issue, which is the compression of the cord by the fetal head or the uterine wall. This can compromise the fetal oxygenation and circulation, leading to fetal distress or death.
Choice B reason: This is correct. Placing the client in a knee-chest or Trendelenburg position is the first action the nurse should take. This can help relieve the pressure of the cord by shifting the fetal head upward or backward, which can restore the blood flow to the cord and the fetus. It can also reduce the risk of cord rupture or spasm, which can cause fetal hemorrhage or shock.
Choice C reason: This is incorrect. Explaining to the client what is happening is not the first action the nurse should take. This can help calm the client and gain their cooperation, but it does not deal with the immediate danger, which is the loss of fetal oxygen and nutrients due to the cord prolapse. The nurse should prioritize the interventions that can save the fetal life.
Choice D reason: This is incorrect. Preparing the client for an emergency cesarean birth is not the first action the nurse should take. This is the definitive treatment for cord prolapse, as it can deliver the fetus as quickly as possible and prevent further complications. However, it is not the most rapid way to manage the situation, as it requires time to prepare the operating room, the anesthesia, and the surgical team. The nurse should first implement the measures that can maintain the fetal well-being until the surgery.
A nurse is assisting with the care of a client who is in the first stage of labor. The nurse observes the umbilical cord protruding from the vagina. Which of the following actions should the nurse take first?
Explanation
Choice A reason: This is incorrect. Covering the cord with a sterile, moist saline dressing is not the first action the nurse should take. This can help prevent the cord from drying out and becoming infected, but it does not address the main issue, which is the compression of the cord by the fetal head or the uterine wall. This can compromise the fetal oxygenation and circulation, leading to fetal distress or death.
Choice B reason: This is correct. Placing the client in a knee-chest or Trendelenburg position is the first action the nurse should take. This can help relieve the pressure of the cord by shifting the fetal head upward or backward, which can restore the blood flow to the cord and the fetus. It can also reduce the risk of cord rupture or spasm, which can cause fetal hemorrhage or shock.
Choice C reason: This is incorrect. Explaining to the client what is happening is not the first action the nurse should take. This can help calm the client and gain their cooperation, but it does not deal with the immediate danger, which is the loss of fetal oxygen and nutrients due to the cord prolapse. The nurse should prioritize the interventions that can save the fetal life.
Choice D reason: This is incorrect. Preparing the client for an emergency cesarean birth is not the first action the nurse should take. This is the definitive treatment for cord prolapse, as it can deliver the fetus as quickly as possible and prevent further complications. However, it is not the most rapid way to manage the situation, as it requires time to prepare the operating room, the anesthesia, and the surgical team. The nurse should first implement the measures that can maintain the fetal well-being until the surgery.
A nurse is caring for a client who is requesting to go to the bathroom immediately after a vaginal birth. Which of the following actions should the nurse take?
Explanation
Choice A reason: This is incorrect. Informing the client that she can go to the bathroom whenever needed is not the best action the nurse should take. The client may have a decreased sensation of bladder fullness or a weak bladder tone after a vaginal birth, which can lead to urinary retention or overflow incontinence. The nurse should encourage the client to void within 4 to 6 hours after delivery and monitor the urine output and characteristics.
Choice B reason: This is incorrect. Advising the client to remain in bed for the next few hours is not the best action the nurse should take. The client may benefit from early ambulation after a vaginal birth, as it can promote circulation, prevent thrombosis, and enhance bowel and bladder function. The nurse should assist the client to get out of bed safely and gradually, and observe for signs of orthostatic hypotension or bleeding.
Choice C reason: This is correct. Assisting the client to the bathroom and assessing the lochia is the best action the nurse should take. The client may need help to walk to the bathroom, as she may feel weak, dizzy, or sore after a vaginal birth. The nurse should also assess the lochia, which is the vaginal discharge that consists of blood, mucus, and tissue. The nurse should check the amount, color, odor, and consistency of the lochia, and report any abnormal findings, such as excessive bleeding, clots, or infection.
Choice D reason: This is incorrect. Evaluating the side effects of any analgesics used during labor is not the best action the nurse should take. The client may have received analgesics, such as opioids or epidural, during labor, which can cause side effects, such as nausea, vomiting, itching, or respiratory depression. The nurse should monitor theclient for these effects and provide appropriate interventions, but this is not the priority action after a vaginal birth.
A nurse is preparing to administer dinoprostone gel to a client who is pregnant. The client asks the nurse about the purpose of the medication. Which of the following responses should the nurse make?
Explanation
Choice A reason: This is correct. Dinoprostone is a prostaglandin, a hormone-like substance that is naturally produced by tissues in the body. Dinoprostone topical is used in a pregnant woman to relax the muscles of the cervix (cervical ripening) in preparation for inducing labor at the end of a pregnancy.
Choice B reason: This is incorrect. Dinoprostone does not increase the frequency of contractions. Dinoprostone may cause mild contractions, but it is not intended to induce labor. It is used to prepare the cervix for labor, not to start it. Other medications, such as oxytocin, are used to stimulate uterine contractions.
Choice C reason: This is incorrect. Dinoprostone does not decrease the risk of infection. Dinoprostone may increase the risk of infection, especially if the membranes are ruptured or the gel is left in the vagina for too long. The nurse should monitor the client for signs of infection, such as fever, chills, or foul-smelling discharge.
Choice D reason: This is incorrect. Dinoprostone does not reduce the pain of labor. Dinoprostone may cause cramping, backache, or pelvic pain, which can be similar to labor pain. The nurse should provide comfort measures and analgesics as needed.
A nurse is assisting with the care of a client who is receiving oxytocin via IV infusion following a vaginal delivery. Which of the following findings should the nurse monitor to evaluate effectiveness of this medication?
Explanation
Choice A reason: This is incorrect. Urinary output is not the best indicator of the effectiveness of oxytocin. Urinary output may be affected by various factors, such as fluid intake, fluid loss, bladder tone, or kidney function. The nurse should monitor the urinary output to prevent urinary retention or infection, but it does not reflect the action of oxytocin².
Choice B reason: This is incorrect. Pulse rate is not the best indicator of the effectiveness of oxytocin. Pulse rate may be influenced by various factors, such as pain, anxiety, blood loss, or dehydration. The nurse should monitor the pulse rate to assess the hemodynamic status of the client, but it does not reflect the action of oxytocin².
Choice C reason: This is correct. Fundal consistency is the best indicator of the effectiveness of oxytocin. Oxytocin is a natural hormone that stimulates uterine contractions in childbirth and lactation after childbirth. It also helps the uterus to contract and return to its normal size and position after delivery. The nurse should palpate the fundus (the upper part of the uterus) to check its firmness, height, and location. A firm, midline, and below-the-umbilicus fundus indicates that oxytocin is working properly and preventing postpartum hemorrhage².
Choice D reason: This is incorrect. Blood pressure is not the best indicator of the effectiveness of oxytocin. Blood pressure may be affected by various factors, such as pain, anxiety, blood loss, or dehydration. The nurse should monitor the blood pressure to assess the hemodynamic status of the client, but it does not reflect the action of oxytocin².
A nurse is collecting data from a client who is 12 hr postpartum following a spontaneous vaginal delivery. The nurse should expect to find the uterine fundus at which of the following positions on the client's abdomen?
Explanation
Choice A reason: This is incorrect. Three fingerbreadths above the umbilicus is not the expected position of the uterine fundus 12 hr postpartum. The uterine fundus is the upper part of the uterus that can be palpated through the abdomen. Immediately after delivery, the fundus is at the level of the umbilicus or slightly below. It then descends about one fingerbreadth per day until it reaches the pelvic cavity by the tenth day. If the fundus is higher than expected, it may indicate uterine atony, distended bladder, or retained placenta.
Choice B reason: This is incorrect. One fingerbreadth above the symphysis pubis is not the expected position of the uterine fundus 12 hr postpartum. The symphysis pubis is the joint where the two halves of the pelvis meet in the front. The fundus is normally at this level by the tenth day postpartum, not the first day. If the fundus is lower than expected, it may indicate uterine inversion, subinvolution, or infection.
Choice C reason: This is correct. At the level of the umbilicus is the expected position of the uterine fundus 12 hr postpartum. The fundus is normally at this level or slightly below immediately after delivery, and then descends gradually until it reaches the pelvic cavity by the tenth day. This indicates that the uterus is contracting and involuting properly, which prevents postpartum hemorrhage and infection.
Choice D reason: This is incorrect. To the right of the umbilicus is not the expected position of the uterine fundus 12 hr postpartum. The fundus should be midline and symmetrical, not deviated to either side. If the fundus is displaced to the right, it may indicate a full bladder, which can interfere with the uterine contraction and involution. The nurse should encourage the client to void and reassess the fundal position.
A nurse is assisting with the care of a client who is in labor. Which of the following findings should the nurse report to the provider?
Explanation
Choice A reason: This is correct. Fetal heart rate 100/min for a 10-min period is a finding that the nurse should report to the provider. The normal range of fetal heart rate is 110 to 160 beats per minute. A fetal heart rate below 110 beats per minute for more than 10 minutes is called fetal bradycardia, which can indicate fetal distress, hypoxia, acidosis, or cord compression. The nurse should notify the provider and intervene to improve the fetal oxygenation and circulation.
Choice B reason: This is incorrect. Four contractions in a 10-min period is not a finding that the nurse should report to the provider. This is a normal frequency of contractions during the active phase of labor, which occurs when the cervix is dilated from 4 to 7 cm. The nurse should monitor the contractions and the fetal heart rate, but there is no need to alert the provider unless there are signs of complications.
Choice C reason: This is incorrect. Contraction resting period 35 seconds is not a finding that the nurse should report to the provider. This is a normal duration of the interval between contractions during the active phase of labor, which allows the uterus and the placenta to relax and replenish the blood and oxygen supply to the fetus. The nurse should monitor the contractions and the fetal heart rate, but there is no need to alert the provider unless there are signs of complications.
Choice D reason: This is incorrect. Contraction lasting 85 seconds is not a finding that the nurse should report to the provider. This is a normal duration of contractions during the active phase of labor, which helps the cervix to efface and dilate. The nurse should monitor the contractions and the fetal heart rate, but there is no need to alert the provider unless there are signs of complications.
A nurse is assisting with the admission of a client who is at 39 weeks of gestation and has heavy vaginal bleeding. Which of the following actions should the nurse take?
Explanation
Choice A reason: This is incorrect. Initiating an IV infusion of magnesium sulfate is not the appropriate action for a client who has heavy vaginal bleeding. Magnesium sulfate is a medication that is used to prevent seizures in clients who have preeclampsia or eclampsia, which are conditions that cause high blood pressure and proteinuria during pregnancy. It does not stop bleeding or improve the condition of the placenta or the fetus.
Choice B reason: This is incorrect. Administering antibiotics is not the appropriate action for a client who has heavy vaginal bleeding. Antibiotics are medications that are used to treat or prevent infections caused by bacteria. They do not stop bleeding or improve the condition of the placenta or the fetus.
Choice C reason: This is incorrect. Requesting the RN perform a cervical examination is not the appropriate action for a client who has heavy vaginal bleeding. A cervical examination is a procedure that involves inserting a gloved finger into the vagina to check the dilation and effacement of the cervix. It can cause more bleeding or damage the placenta or the fetus, especially if the client has placenta previa, which is a condition where the placenta covers the opening of the cervix.
Choice D reason: This is correct. Preparing for cesarean birth is the appropriate action for a client who has heavy vaginal bleeding. A cesarean birth is a surgical procedure that involves delivering the baby through an incision in the abdomen and the uterus. It is indicated for clients who have heavy vaginal bleeding due to placental abruption, which is a condition where the placenta separates from the uterine wall before delivery, or placenta previa, which is a condition where the placenta covers the opening of the cervix. It can save the life of the mother and the baby.
A nurse is collecting data from a client who is 14 hr postpartum. The nurse notes: breasts soft, fundus firm, slightly deviated to the right, moderate lochia rubra, temperature 37.7 C (100 F), pulse rate 88/min, respiratory rate 18/min. Which of the following actions should the nurse perform?
Explanation
Choice A reason: This is correct. Asking the client to empty her bladder is the appropriate action for a nurse who notes that the fundus is slightly deviated to the right. The fundus is the upper part of the uterus that can be palpated through the abdomen. It should be firm, midline, and below the umbilicus after delivery. A deviated fundus may indicate a full bladder, which can interfere with the uterine contraction and involution, and increase the risk of bleeding and infection. The nurse should encourage the client to void and reassess the fundal position.
Choice B reason: This is incorrect. Increasing IV fluids is not the appropriate action for a nurse who notes that the fundus is slightly deviated to the right. IV fluids can help maintain hydration and blood volume, but they do not address the cause of the fundal deviation, which is a full bladder. Excessive IV fluids may also cause fluid overload or edema in the mother or the baby.
Choice C reason: This is incorrect. Encouraging the client to nurse more frequently is not the appropriate action for a nurse who notes that the fundus is slightly deviated to the right. Nursing can stimulate the release of oxytocin, which is a hormone that helps the uterus contract and prevent bleeding. However, it does not address the cause of the fundal deviation, which is a full bladder. Nursing may also be uncomfortable or difficult for the client if her bladder is distended.
Choice D reason: This is incorrect. Reporting the client's temperature is not the appropriate action for a nurse who notes that the fundus is slightly deviated to the right. The client's temperature is within the normal range for a postpartum client, as it may be slightly elevated due to dehydration, exertion, or breast engorgement. It does not indicate an infection or a complication that needs to be reported. It also does not address the cause of the fundal deviation, which is a full bladder.
A nurse is caring for a client who has unrelieved episiotomy pain 8 hr following delivery. Which of the following actions should the nurse take?
Explanation
Choice A reason: This is incorrect. Preparing a warm sitz bath is not the best action for a client who has unrelieved episiotomy pain. A sitz bath is a shallow bath that covers the hips and buttocks. It can help soothe the perineal area and promote healing, but it is not recommended until 24 hours after delivery. A warm sitz bath may also increase swelling and bleeding in the episiotomy site.
Choice B reason: This is correct. Applying an ice pack to the perineum is the best action for a client who has unrelieved episiotomy pain. An ice pack can help reduce swelling and inflammation in the episiotomy site and provide pain relief. It should be applied for 10 to 20 minutes at a time, several times a day, for the first 24 to 48 hours after delivery. The ice pack should be wrapped in a towel or cloth to prevent frostbite.
Choice C reason: This is incorrect. Placing a soft pillow under the client's buttocks is not the best action for a client who has unrelieved episiotomy pain. A soft pillow can provide some comfort and support for the client, but it does not address the cause of the pain, which is the episiotomy wound. A pillow may also increase pressure and friction on the perineal area, which can delay healing and increase the risk of infection.
Choice D reason: This is incorrect. Positioning a heating lamp toward the episiotomy is not the best action for a client who has unrelieved episiotomy pain. A heating lamp can provide some warmth and dryness to the episiotomy site, but it is not recommended until 48 hours after delivery. A heating lamp may also cause burns, dehydration, or irritation to the perineal area.
A nurse is reinforcing teaching with a client who is in labor about why epidural anesthesia is not initiated until a good labor pattern has been established. Which of the following explanations should the nurse include?
Explanation
Choice A reason: This is correct. Epidural anesthesia is a type of regional anesthesia that blocks the pain sensation from the lower part of the body. It is usually given when the cervix is dilated to 4 cm or more, and the contractions are regular and strong. If it is given too soon, it may interfere with the natural hormones that stimulate labor, such as oxytocin and prostaglandins. It may also reduce the urge to push and the ability to bear down. These effects can lead to a longer labor and an increased risk of instrumental delivery or cesarean section¹².
Choice B reason: This is incorrect. Epidural anesthesia does not delay rupture of fetal membranes. Rupture of fetal membranes, also known as breaking the water, is the process of the amniotic sac tearing and releasing the fluid that surrounds the baby. It can occur spontaneously or artificially during labor. It is not affected by the timing or the type of anesthesia³.
Choice C reason: This is incorrect. Epidural anesthesia does not cause maternal hypertension. Maternal hypertension, also known as high blood pressure, is a condition that affects some pregnant women. It can cause complications, such as preeclampsia, eclampsia, or placental abruption. Epidural anesthesia can actually lower the blood pressure by dilating the blood vessels in the lower part of the body. This can help prevent or treat maternal hypertension, but it can also cause hypotension, or low blood pressure, which can affect the blood flow to the placenta and the fetus. The nurse should monitor the blood pressure and the fetal heart rate, and administer fluids or medications as needed.
Choice D reason: This is incorrect. Epidural anesthesia does not cause fetal depression. Fetal depression, also known as fetal distress, is a condition that indicates that the fetus is not getting enough oxygen or nutrients. It can be caused by various factors, such as cord compression, placental insufficiency, or maternal hypoxia. Epidural anesthesia can improve the oxygenation and the circulation of the mother and the fetus by reducing the pain and the stress of labor. It can also prevent or treat maternal hypertension, which can affect the placental function. The nurse should monitor the fetal heart rate and the uterine contractions, and intervene if there are signs of fetal distress.
A nurse is collecting data from a client who is 3 days postpartum and is breastfeeding. Her fundus is three fingerbreadths below the umbilicus, and her lochia rubra is moderate. Her breasts feel hard and warm. Which of the following recommendations should the nurse give the client?
Explanation
Choice A reason: This is correct. Expressing milk from both breasts is the best recommendation for a client who has hard and warm breasts. This is a sign of breast engorgement, which is a condition where the breasts become swollen, tender, and painful due to the accumulation of milk and fluid. Expressing milk can help relieve the pressure and discomfort, and prevent mastitis, which is an infection of the breast tissue. The client can express milk by hand, with a pump, or by breastfeeding the baby frequently.
Choice B reason: This is incorrect. Applying a heating pad to her breasts is not a good recommendation for a client who has hard and warm breasts. This can worsen the engorgement and inflammation, and increase the risk of infection. A cold compress or a cabbage leaf can help reduce the swelling and pain, but only after expressing milk or breastfeeding.
Choice C reason: This is incorrect. Wearing a nipple shield is not a good recommendation for a client who has hard and warm breasts. A nipple shield is a thin, flexible cover that fits over the nipple and areola. It can help protect sore or cracked nipples, or help the baby latch on better. However, it can also interfere with the milk flow and supply, and cause nipple confusion or preference. It should be used only under the guidance of a lactation consultant or a healthcare professional.
Choice D reason: This is incorrect. Obtaining a prescription for an antibiotic is not a good recommendation for a client who has hard and warm breasts. Antibiotics are medications that are used to treat or prevent bacterial infections. They are not indicated for breast engorgement, unless there are signs of mastitis, such as fever, redness, or pus. Antibiotics can also have side effects, such as nausea, diarrhea, or allergic reactions. They can also affect the baby's gut flora and immunity. They should be used only when prescribed by a healthcare professional.
A nurse is caring for a client following a cesarean birth. The client tells the nurse that she is hungry. Which of the following actions should the nurse take first?
Explanation
Choice A reason: This is incorrect. Checking the client's chart for a diet prescription is not the first action the nurse should take. The client may have a diet order from the provider, such as clear liquids, full liquids, or regular diet, depending on the type of anesthesia and the bowel function. However, the nurse should first assess the client's abdomen to determine if the client has bowel sounds, which indicate the return of peristalsis after surgery.
Choice B reason: This is correct. Auscultating the client's abdomen is the first action the nurse should take. The nurse should listen to the four quadrants of the abdomen for bowel sounds, which are gurgling or clicking noises that indicate the movement of gas and fluid through the intestines. Bowel sounds are usually absent or diminished after a cesarean birth due to the manipulation of the bowel during surgery and the effects of anesthesia. The nurse should wait until the bowel sounds are present and normal before advancing the client's diet.
Choice C reason: This is incorrect. Offering clear liquids is not the first action the nurse should take. Clear liquids are fluids that are transparent or translucent, such as water, broth, tea, or juice. They are easy to digest and absorb, and they can prevent dehydration and electrolyte imbalance. However, the nurse should not offer any oral intake to the client until the bowel sounds are present and normal, as the client may have nausea, vomiting, or abdominal distension.
Choice D reason: This is incorrect. Giving the client soda crackers is not the first action the nurse should take. Soda crackers are dry, salty biscuits that can help settle the stomach and provide some carbohydrates. However, they are not appropriate for a client who has just had a cesarean birth, as they are solid foods that require more digestion and peristalsis. The nurse should not give any solid foods to the client until the bowel sounds are present and normal, and the client has tolerated clear liquids.
A nurse is collecting data from a client who is postpartum. Which of the following findings should alert the nurse to the possibility of a postpartum complication?
Explanation
Choice A reason: This is incorrect. Urinary output 3,000 mL/12 hr is not a finding that should alert the nurse to a postpartum complication. This is a normal amount of urine output for a postpartum client, as the body eliminates the excess fluid that was retained during pregnancy. The nurse should monitor the urine output and characteristics, but there is no need to report this finding unless it is too low or too high.
Choice B reason: This is correct. Temperature 100.4 F for two days is a finding that should alert the nurse to a postpartum complication. This is a sign of a fever, which can indicate an infection in the uterus, the bladder, the breasts, or the wound. The nurse should report this finding and obtain a culture and sensitivity test to identify the causative organism and the appropriate antibiotic. The nurse should also monitor the client for other signs of infection, such as foul-smelling lochia, pelvic pain, or redness and swelling of the breasts or the incision.
Choice C reason: This is incorrect. Fundus at umbilicus level is not a finding that should alert the nurse to a postpartum complication. This is a normal position of the fundus, which is the upper part of the uterus that can be palpated through the abdomen. Immediately after delivery, the fundus is at the level of the umbilicus or slightly below. It then descends about one fingerbreadth per day until it reaches the pelvic cavity by the tenth day. The nurse should palpate the fundus to check its firmness, height, and location, but there is no need to report this finding unless it is higher or lower than expected.
Choice D reason: This is incorrect. Chills shortly following delivery is not a finding that should alert the nurse to a postpartum complication. This is a common occurrence after delivery, as the body adjusts to the sudden drop in temperature and hormones. The nurse should provide warm blankets and fluids to the client, but there is no need to report this finding unless it is accompanied by a fever, which can indicate an infection.
A nurse is caring for a group of clients on an intrapartum unit. Which of the following findings should be reported to the RN immediately?
Explanation
Choice A reason: This is correct. A client who has preeclampsia and reports epigastric pain and unresolved headache should be reported to the RN immediately. These are signs of severe preeclampsia, which is a complication of pregnancy characterized by high blood pressure and protein in the urine. ¹ Epigastric pain and headache may indicate liver damage or increased intracranial pressure, which can lead to eclampsia, a life-threatening condition that causes seizures. ² The nurse should monitor the client's vital signs, urine output, and fetal heart rate, and administer antihypertensive and anticonvulsant medications as prescribed.
Choice B reason: This is incorrect. A client who has preeclampsia has 2+ patellar reflexes and 2+ proteinuria should not be reported to the RN immediately. These are expected findings in a client with mild preeclampsia, which is a complication of pregnancy characterized by high blood pressure and protein in the urine. ¹ Patellar reflexes are a measure of the knee jerk response, which can be increased in preeclampsia due to magnesium deficiency or hyperreflexia. ³ Proteinuria is the presence of excess protein in the urine, which indicates kidney damage. The nurse should monitor the client's blood pressure, urine protein, and fetal well-being, and provide education and support.
Choice C reason: This is incorrect. A client who is at 32 weeks of gestation and is experiencing irregular, frequent contractions is tearful should not be reported to the RN immediately. These are signs of preterm labor, which is the onset of labor before 37 weeks of gestation. Preterm labor can be caused by various factors, such as infection, dehydration, or placental problems. ⁶ The nurse should assess the client's cervix, fetal heart rate, and amniotic fluid, and administer tocolytic medications as prescribed to stop the contractions. The nurse should also provide emotional support and reassurance to the client.
Choice D reason: This is incorrect. A client who is at 28 weeks of gestation and receiving terbutaline reports fine tremors should not be reported to the RN immediately. These are common side effects of terbutaline, which is a medication used to treat asthma and bronchospasm, and to delay preterm labor. ⁷ Terbutaline works by relaxing the smooth muscles in the airways and the uterus, but it can also cause nervousness, tremor, headache, fast heart rate, and elevated blood pressure. ⁸ The nurse should monitor the client's vital signs, blood glucose, and fetal heart rate, and adjust the dose of terbutaline as needed. The nurse should also inform the client that these side effects are temporary and will subside after the medication is stopped..
A nurse is caring for a client following a cesarean birth. The client tells the nurse that she is hungry. Which of the following actions should the nurse take first?
Explanation
Choice A reason: This is incorrect. Checking the client's chart for a diet prescription is not the first action the nurse should take. The client may have a diet order from the provider, such as clear liquids, full liquids, or regular diet, depending on the type of anesthesia and the bowel function. However, the nurse should first assess the client's abdomen to determine if the client has bowel sounds, which indicate the return of peristalsis after surgery.
Choice B reason: This is correct. Auscultating the client's abdomen is the first action the nurse should take. The nurse should listen to the four quadrants of the abdomen for bowel sounds, which are gurgling or clicking noises that indicate the movement of gas and fluid through the intestines. Bowel sounds are usually absent or diminished after a cesarean birth due to the manipulation of the bowel during surgery and the effects of anesthesia. The nurse should wait until the bowel sounds are present and normal before advancing the client's diet.
Choice C reason: This is incorrect. Offering clear liquids is not the first action the nurse should take. Clear liquids are fluids that are transparent or translucent, such as water, broth, tea, or juice. They are easy to digest and absorb, and they can prevent dehydration and electrolyte imbalance. However, the nurse should not offer any oral intake to the client until the bowel sounds are present and normal, as the client may have nausea, vomiting, or abdominal distension.
Choice D reason: This is incorrect. Giving the client soda crackers is not the first action the nurse should take. Soda crackers are dry, salty biscuits that can help settle the stomach and provide some carbohydrates. However, they are not appropriate for a client who has just had a cesarean birth, as they are solid foods that require more digestion and peristalsis. The nurse should not give any solid foods to the client until the bowel sounds are present and normal, and the client has tolerated clear liquids.
A nurse is assisting a client out of bed for the first time since delivery. The client becomes frightened when she passes a large amount of lochia.
Which of the following responses should the nurse make?
Explanation
Choice A reason: This statement is true. Lochia is the vaginal discharge after giving birth, containing blood, mucus, and uterine tissue¹. It can accumulate in the vagina when the client is lying down, and then gush out when the client stands up or changes position. This is normal and does not indicate excessive bleeding. The nurse should reassure the client and explain the nature of lochia.
Choice B reason: This statement is false. The amount of lochia decreases during the postpartum period, as the uterus heals and contracts. Lochia has three stages: lochia rubra (red), lochia serosa (pinkish brown), and lochia alba (yellowish white)¹. Each stage lasts for a few days to weeks, and the flow becomes lighter and less bloody over time.
Choice C reason: This statement is false. Urinary tract infections (UTIs) are not associated with increased lochia. UTIs are infections of the bladder, urethra, or kidneys, and they cause symptoms such as burning, pain, frequency, urgency, or fever². Lochia is not affected by UTIs, unless the infection spreads to the uterus, which is rare and requires immediate medical attention.
Choice D reason: This statement is false. Retained fragments of the placenta are not a common cause of increased lochia. Retained placenta is a condition where part or all of the placenta remains in the uterus after delivery, and it can cause heavy bleeding, infection, or uterine rupture³. Retained placenta is usually diagnosed and treated within the first hour after delivery, and it does not affect the normal course of lochia.
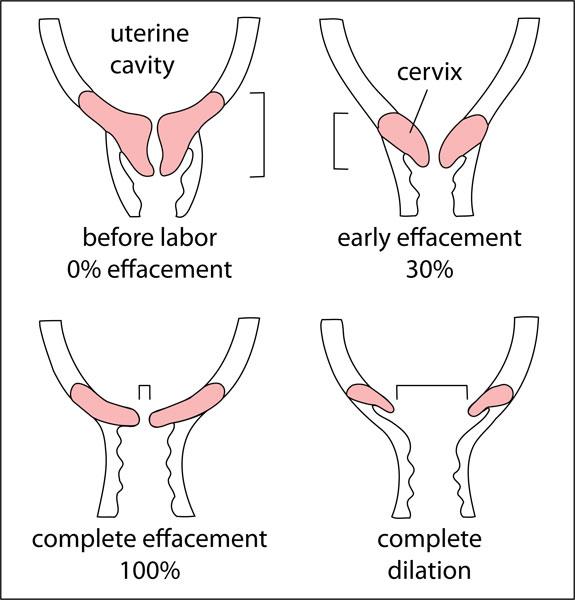
A nurse is assisting in the care of a client who is in labor. The doctor documents the vaginal examination as: 3 cm, 30%, and -1. The nurse evaluates this documentation to mean which of the following?
Explanation
Choice A reason: This statement is false. The cervix is not effaced 3 cm, but 30%. Effacement is the thinning of the cervix, measured in percentage from 0% (thick) to 100% (thin). The cervix is also not dilated 30%, but 3 cm. Dilation is the opening of the cervix, measured in centimeters from 0 cm (closed) to 10 cm (fully open).
Choice B reason: This statement is true. The cervix is dilated 3 cm, it is effaced 30%, and the presenting part is 1 cm above the ischial spines. The presenting part is the part of the fetus that is closest to the cervix, usually the head. The position of the presenting part is measured in relation to the ischial spines, which are bony landmarks in the pelvis. A positive number means the presenting part is below the ischial spines, a negative number means it is above the ischial spines, and zero means it is at the level of the ischial spines.
Choice C reason: This statement is false. The cervix is not effaced 30%, but 3 cm. Effacement is not measured in centimeters, but in percentage. The cervix is also not dilated 3 cm, but 30%. Dilation is not measured in percentage, but in centimeters.
Choice D reason: This statement is false. The cervix is not dilated 30%, but 3 cm. Dilation is not measured in percentage, but in centimeters. The cervix is also not effaced 3 cm, but 30%. Effacement is not measured in centimeters, but in percentage.
A nurse is caring for a postpartum client who saturates a perineal pad in 10 min. Which of the following actions should the nurse take first?
Explanation
Choice A reason: This statement is false. Administering oxytocin is not the first action the nurse should take. Oxytocin is a medication that stimulates uterine contractions and reduces bleeding. However, it should only be given after the nurse has assessed the cause and severity of the bleeding, and with a provider's order.
Choice B reason: This statement is false. Observing for pooling of blood under the buttocks is not the first action the nurse should take. Pooling of blood under the buttocks indicates that the client is bleeding heavily and may have a hematoma (a collection of blood in the tissues). However, it does not address the source or the treatment of the bleeding. The nurse should first try to stop the bleeding by massaging the fundus.
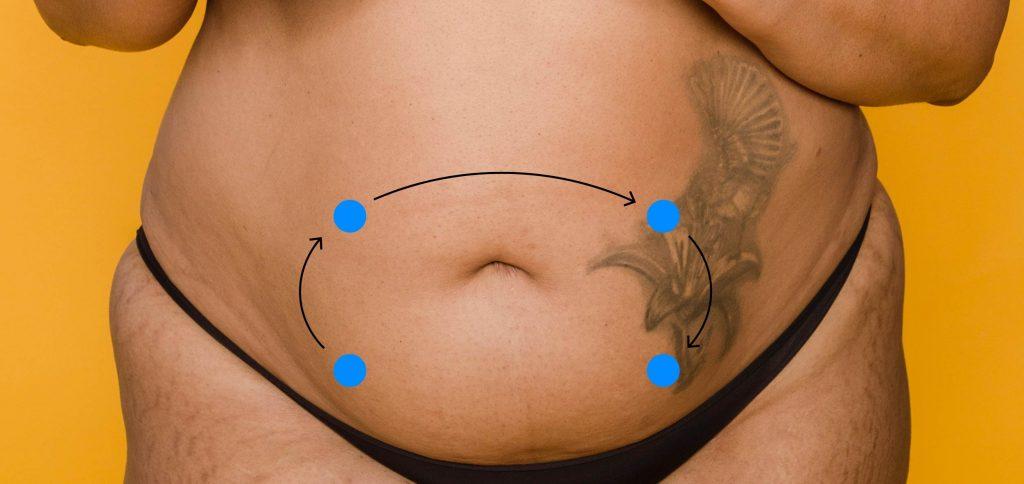
Choice C reason: This statement is true. Massaging the client's fundus is the first action the nurse should take. The fundus is the upper part of the uterus, and it should be firm and contracted after delivery. If the fundus is soft or boggy, it means that the uterus is not contracting well and may cause excessive bleeding. The nurse should massage the fundus gently but firmly until it becomes hard and contracts. This will help to expel any clots and reduce bleeding.
Choice D reason: This statement is false. Checking the client's blood pressure is not the first action the nurse should take. Blood pressure is an indicator of the client's hemodynamic status and may show signs of shock if the bleeding is severe. However, it does not address the cause or the treatment of the bleeding. The nurse should first try to stop the bleeding by massaging the fundus.
A nurse is reinforcing teaching about signs preceding the onset of labor with a client who is at 39 weeks of gestation. Which of the following statements should the nurse include?
Explanation
Choice A reason: This statement is true. A surge of energy, also known as nesting instinct, is a sign that labor may be near. It is a sudden burst of motivation and activity that some women feel before giving birth. They may feel the need to clean, organize, or prepare for the baby.
Choice B reason: This statement is false. A weight gain of 0.5 to 1.5 kilograms is not a sign of labor. In fact, some women may lose weight before labor due to hormonal changes, fluid loss, or reduced appetite.
Choice C reason: This statement is false. A decrease in vaginal discharge is not a sign of labor. On the contrary, some women may have an increase in vaginal discharge before labor, especially if it is bloody or mucous-like. This may indicate that the cervix is dilating and the mucus plug is dislodging.
Choice D reason: This statement is false. Urinary retention is not a sign of labor. It is a condition where the bladder cannot empty completely, causing discomfort, pain, or infection. It can be caused by various factors, such as medication, nerve damage, or obstruction.
A nurse is collecting data from a postpartum client and finds a large amount of lochia rubra with several clots on the client’s perineal pad. Which of the following actions should the nurse take first?
Explanation
Choice A reason: This statement is false. Requesting the provider perform a vaginal examination is not the first action the nurse should take. A vaginal examination may be necessary to rule out any retained placental fragments or lacerations, but it should only be done after the nurse has assessed the cause and severity of the bleeding, and with the provider's consent.
Choice B reason: This statement is true. Checking the client's fundus is the first action the nurse should take. The fundus is the upper part of the uterus, and it should be firm and contracted after delivery. If the fundus is soft or boggy, it means that the uterus is not contracting well and may cause excessive bleeding. The nurse should massage the fundus gently but firmly until it becomes hard and contracts. This will help to expel any clots and reduce bleeding.
Choice C reason: This statement is false. Measuring the client's vital signs is not the first action the nurse should take. Vital signs are indicators of the client's hemodynamic status and may show signs of shock if the bleeding is severe. However, they do not address the cause or the treatment of the bleeding. The nurse should first try to stop the bleeding by checking the fundus.
Choice D reason: This statement is false. Feeling for a full bladder is not the first action the nurse should take. A full bladder can interfere with uterine contraction and cause bleeding. However, it is not the most common cause of postpartum hemorrhage. The nurse should first try to stop the bleeding by checking the fundus.
A nurse is assisting a nurse midwife in examining a client who is a primigravida at 42 weeks of gestation and states that she thinks she is in labor. Which of the following findings confirm that the client is in labor?
Explanation
Choice A reason: This statement is false. Contractions every 3 to 4 min are not a definitive sign of labor. Contractions can occur before labor, during false labor (Braxton Hicks contractions), or early labor. They may or may not be regular, strong, or painful. The nurse should also assess the duration, intensity, and frequency of the contractions, as well as the cervical changes.
Choice B reason: This statement is false. Pain just above the navel is not a sign of labor. Pain in labor is usually felt in the lower back, abdomen, or pelvis. Pain just above the navel may indicate other problems, such as gallstones, gastritis, or pancreatitis.
Choice C reason: This statement is true. Cervical dilation is a sign of labor. Cervical dilation is the opening of the cervix, measured in centimeters from 0 cm (closed) to 10 cm (fully open). Cervical dilation indicates that the uterus is contracting and pushing the baby down the birth canal. The nurse should also assess the effacement (thinning) and position of the cervix.
Choice D reason: This statement is false. Amniotic fluid in the vaginal vault is not a sign of labor. Amniotic fluid is the fluid that surrounds and protects the baby in the uterus. It may leak or gush out of the vagina when the membranes rupture, also known as water breaking. However, this does not always happen before labor, and it does not indicate that the cervix is dilating. The nurse should also check the color, odor, and amount of the fluid.
Sign Up or Login to view all the 23 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
