Custom ATI Maternity Final 2023
Total Questions : 54
Showing 25 questions, Sign in for moreA nurse is assisting in the care of a client who is scheduled for a cesarean birth based on the fetal lungs having reached maturity. Which of the following findings indicates that the fetal lungs are mature?
Explanation
Choice A reason: This statement is false. PG is a phospholipid that is present in the amniotic fluid when the fetal lungs are mature. Its absence indicates immature lungs.
Choice B reason: This statement is false. A biophysical profile is a test that assesses the fetal well-being by measuring five parameters: fetal movement, fetal tone, fetal breathing, amniotic fluid volume, and fetal heart rate. A score of 8 out of 10 is normal, but it does not indicate lung maturity.
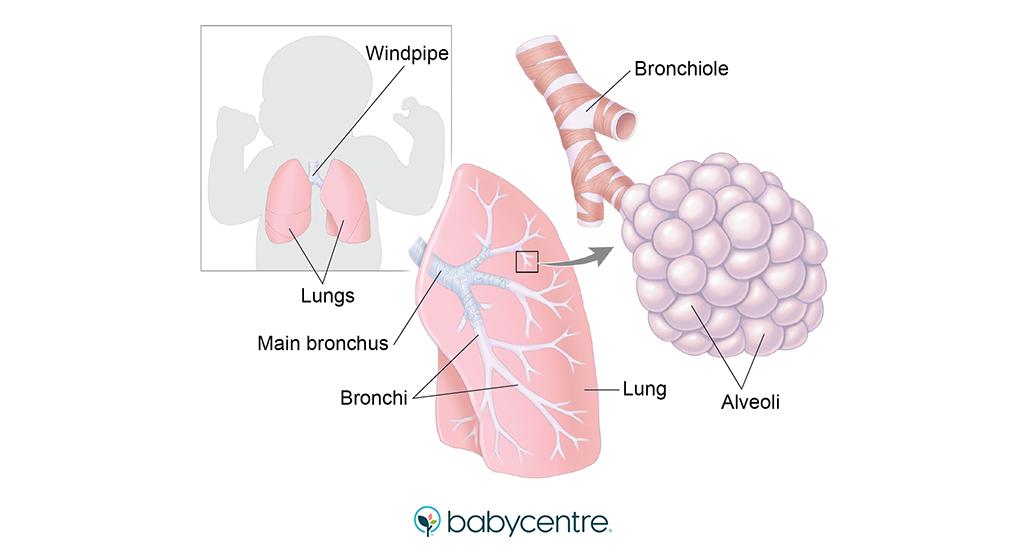
Choice C reason: This statement is true. L/S ratio is a test that measures the amount of two surfactants, lecithin and sphingomyelin, in the amniotic fluid. Surfactants are substances that reduce the surface tension of the alveoli and prevent them from collapsing. A ratio of 2:1 or higher indicates that the fetal lungs are mature and can produce enough surfactant.
Choice D reason: This statement is false. A nonstress test is a test that monitors the fetal heart rate in response to fetal movement. A reactive test means that the fetal heart rate increases by at least 15 beats per minute for at least 15 seconds after a fetal movement. This indicates that the fetus is healthy, but it does not indicate lung maturity.
A nurse is reinforcing teaching with the parents of a newborn about caring for the umbilical cord stump. Which of the following instructions should the nurse include?
Explanation
Choice A reason: This statement is true. Giving the newborn a sponge bath until the cord stump falls off helps to keep the cord dry and prevent infection. The cord stump usually falls off within 10 to 14 days after birth.
Choice B reason: This statement is false. Wrapping the cord in petroleum jelly gauze is not recommended, as it can trap moisture and bacteria and delay the healing process. The cord should be exposed to air as much as possible.
Choice C reason: This statement is false. Washing the cord daily with mild soap and water is not necessary, as it can irritate the skin and increase the risk of infection. The cord should be cleaned only when it is soiled with urine or stool, using a clean, damp cloth and then patting it dry.
Choice D reason: This statement is false. Covering the cord with the diaper can cause friction and pressure on the cord, which can lead to bleeding or infection. The diaper should be folded below the cord to avoid contact.
A nurse is assisting with the admission of a client who is in preterm labor at 30 weeks of gestation and has a new prescription for betamethasone. Which of the following statements should the nurse make?
Explanation
Choice A reason: This statement is false. Betamethasone is a corticosteroid that does not affect the fetal heart rate. It is given to the mother to accelerate the development of the fetal lungs and reduce the risk of respiratory distress syndrome and other complications.
Choice B reason: This statement is false. Betamethasone is not a tocolytic agent that can stop preterm labor contractions. It is given to the mother to improve the fetal outcomes in case of preterm delivery.
Choice C reason: This statement is false. Betamethasone does not have any effect on the cervical dilation. It is given to the mother to enhance the production of surfactant in the fetal lungs and prevent alveolar collapse.
Choice D reason: This statement is true. Betamethasone is a corticosteroid that stimulates the maturation of the fetal lungs and increases the synthesis of surfactant. It is given to the mother 24 to 48 hours before the expected preterm delivery to reduce the incidence and severity of neonatal respiratory distress syndrome and other morbidities.
A nurse is assisting with the care of a newborn following a vaginal delivery. Which of the following actions should the nurse perform first?
Explanation
Choice A reason: This statement is false. Stimulating the infant to cry is not the first action that the nurse should perform. Crying can cause the infant to lose heat and increase the risk of hypothermia. The nurse should first dry the infant off and cover the head to prevent heat loss and then assess the respiratory status.
Choice B reason: This statement is true. Drying the infant off and covering the head is the first action that the nurse should perform. This helps to prevent heat loss through evaporation and radiation and maintain the infant's body temperature. The nurse should also place the infant on the mother's chest or abdomen to promote skin-to-skin contact and bonding.
Choice C reason: This statement is false. Clamping the umbilical cord is not the first action that the nurse should perform. The nurse should wait until the cord stops pulsating before clamping and cutting it. This allows the infant to receive more blood from the placenta and reduce the risk of anemia and hemorrhage.
Choice D reason: This statement is false. Clearing the respiratory tract is not the first action that the nurse should perform. The nurse should only suction the mouth and nose of the infant if there is evidence of meconium, blood, or mucus that can obstruct the airway. The nurse should first dry the infant off and cover the head to prevent heat loss and then assess the respiratory status.
A nurse is reviewing the medical record of a client who experienced a vaginal birth 2 hr ago. The nurse should identify that which of the following findings places the client at risk for a postpartum hemorrhage?
Explanation
Choice A reason: This statement is false. A small for gestational age newborn does not increase the risk of postpartum hemorrhage. In fact, a large for gestational age newborn or a multiple gestation can cause overdistension of the uterus and impair its ability to contract after delivery, leading to postpartum hemorrhage.
Choice B reason: This statement is false. Gestational hypertension does not directly increase the risk of postpartum hemorrhage. However, it can be associated with other complications such as preeclampsia, placental abruption, or coagulopathy that can cause bleeding after delivery.
Choice C reason: This statement is true. A precipitous birth is a birth that occurs in less than 3 hours from the onset of labor. It can cause trauma to the birth canal, uterine atony, or retained placental fragments, resulting in postpartum hemorrhage.
Choice D reason: This statement is false. A two-vessel umbilical cord is a cord that has one artery and one vein instead of the normal two arteries and one vein. It does not increase the risk of postpartum hemorrhage, but it can indicate other congenital anomalies or fetal growth restriction.
A nurse is reinforcing teaching about umbilical cord care with a client who is postpartum. Which of the following instructions should the nurse include?
Explanation
Choice A reason: This statement is false. Baby oil is not recommended for umbilical cord care, as it can trap moisture and bacteria and delay the healing process. The cord should be kept dry and exposed to air as much as possible.
Choice B reason: This statement is false. Covering the cord with the diaper can cause friction and pressure on the cord, which can lead to bleeding or infection. The diaper should be folded below the cord to avoid contact.
Choice C reason: This statement is false. The stump should fall off in 10 to 14 days, not 10 to 12 days. The time may vary depending on the individual newborn and the type of cord care. The nurse should instruct the client to report any signs of infection, such as redness, swelling, foul odor, or discharge from the cord.
Choice D reason: This statement is true. Immersing the newborn’s abdomen in water can cause the cord to become wet and increase the risk of infection. The nurse should advise the client to give the newborn a sponge bath until the cord is dry and falls off.
A nurse is caring for a client in the prenatal clinic who has a possible ectopic pregnancy at 8 weeks of gestation. Which of the following findings should the nurse expect?
Explanation
Choice A reason: This statement is false. Copious vaginal bleeding is not a typical sign of ectopic pregnancy. It can occur in some cases, but it is more likely to indicate a miscarriage, placenta previa, or placental abruption.
Choice B reason: This statement is true. Pelvic pain is a common and early symptom of ectopic pregnancy. It can be sharp, stabbing, or cramping, and it can vary in intensity and location. It is caused by the implantation of the fertilized egg outside the uterus, usually in the fallopian tube, which can rupture and cause bleeding and inflammation.
Choice C reason: This statement is false. Severe nausea and vomiting are not specific signs of ectopic pregnancy. They can occur in any pregnancy, especially in the first trimester, due to hormonal changes and increased levels of human chorionic gonadotropin (hCG).
Choice D reason: This statement is false. Uterine enlargement greater than expected for gestational age is not a sign of ectopic pregnancy. It can indicate a multiple gestation, a molar pregnancy, or a large fibroid. In ectopic pregnancy, the uterus may be smaller than expected or normal in size.
A nurse is assisting with the care of a client who is in labor. The client’s labor is difficult and prolonged and she reports a severe backache. Which of the following factors is a contributing cause of difficult, prolonged labor?
Explanation
Choice A reason: This statement is false. Fetal lie is the relationship of the long axis of the fetus to the long axis of the mother. A longitudinal lie is the most common and favorable lie for vaginal delivery, as it allows the fetus to pass through the birth canal more easily.
Choice B reason: This statement is false. Fetal attitude is the relationship of the fetal body parts to one another. A general flexion attitude is the most common and favorable attitude for vaginal delivery, as it reduces the diameter of the fetal head and facilitates its descent.
Choice C reason: This statement is false. Maternal pelvis is the shape and size of the mother's bony pelvis. A gynecoid pelvis is the most common and favorable type of pelvis for vaginal delivery, as it has a round and wide inlet and outlet that can accommodate the fetal head.
Choice D reason: This statement is true. Fetal position is the relationship of a specific fetal landmark, usually the occiput, to the maternal pelvis. A persistent occiput posterior position is a common cause of difficult, prolonged labor, as it increases the diameter of the fetal head and makes it harder to rotate and descend. It can also cause severe backache for the mother, as the fetal head presses against the sacrum.
A nurse is caring for a client who is at 36 weeks of gestation and has suspected placenta previa. For which of the following findings should the nurse monitor the client?
Explanation
Choice A reason: This statement is false. Severe abdominal pain with increasing fundal height is not a sign of placenta previa. It can indicate a uterine rupture, which is a life-threatening complication that requires immediate surgical intervention.
Choice B reason: This statement is false. Abdominal pain with minimal red vaginal bleeding is not a sign of placenta previa. It can indicate a placental abruption, which is a partial or complete separation of the placenta from the uterine wall before delivery.
Choice C reason: This statement is true. A large amount of bright red vaginal bleeding without pain is the hallmark sign of placenta previa. It occurs when the placenta implants over or near the cervical os and covers part or all of the opening. The bleeding can be triggered by cervical dilation, contractions, or sexual intercourse.
Choice D reason: This statement is false. Intermittent abdominal pain following passage of bloody mucus is not a sign of placenta previa. It can indicate the onset of labor, as the bloody mucus is the mucus plug that seals the cervical canal during pregnancy.
A client is concerned that her newborn has “crossed eyes.” Which of the following statements is a therapeutic response by the nurse?
Explanation
Choice A reason: This statement is not therapeutic. It does not address the client's feelings or provide reassurance. It may also imply that the nurse is not competent to handle the situation.
Choice B reason: This statement is not therapeutic. It does not explain the reason for taking the baby back to the nursery or involve the client in the decision. It may also increase the client's anxiety and interfere with bonding.
Choice C reason: This statement is therapeutic. It provides factual information and education about the normal development of the newborn's eyes. It also reassures the client that the condition is temporary and not a cause for concern.
Choice D reason: This statement is not therapeutic. It is inaccurate and misleading. Patching the baby's eyes is not a treatment for crossed eyes. It may also cause harm by depriving the baby of visual stimulation and interfering with eye alignment.
A nurse is reinforcing teaching about dietary intake with a client who is breastfeeding her newborn. Which of the following information should the nurse include in the teaching?
Explanation
Choice A reason: This statement is false. The client should not decrease her daily intake of protein, as protein is essential for the production of breast milk and the growth and development of the newborn. The client should consume about 71 grams of protein per day, which is 25 grams more than the recommended amount for non-pregnant women.
Choice B reason: This statement is false. The client should not consume 1500 calories per day, as this is too low for a breastfeeding woman. The client needs extra calories to support the production of breast milk and to meet her own nutritional needs. The client should consume about 500 calories more than the recommended amount for non-pregnant women, which is about 2000 to 2200 calories per day.
Choice C reason: This statement is true. The client should increase her daily intake of folic acid, as folic acid is important for the prevention of neural tube defects and the synthesis of DNA and red blood cells. The client should consume 0.5 milligrams of folic acid per day, which is 0.1 milligrams more than the recommended amount for non-pregnant women.
Choice D reason: This statement is false. The client should not drink enough decaffeinated fluids to quench her thirst, as this may not be sufficient to prevent dehydration and maintain milk supply. The client should drink at least 8 to 10 glasses of fluids per day, preferably water, milk, or juice. The client should limit her intake of caffeinated beverages, as caffeine can pass into the breast milk and cause irritability and sleep problems in the newborn.
A nurse is caring for a client who wants to know if it is possible to have a vaginal birth after a cesarean birth (VBAC). Which of the following statements by the nurse is appropriate?
Explanation
Choice A reason: This statement is not appropriate. It does not provide any information or guidance to the client. It may also make the client feel dismissed or confused.
Choice B reason: This statement is not appropriate. It does not address the client's concerns or needs. It may also make the client feel invalidated or discouraged.
Choice C reason: This statement is not appropriate. It does not reflect the current evidence or recommendations for VBAC. It may also make the client feel scared or pressured.
Choice D reason: This statement is appropriate. It provides factual and relevant information to the client. It also opens the door for further discussion and education about VBAC.
A nurse is collecting data from a client who is at 18 weeks of gestation and tells the nurse that she felt light fluttering in her stomach the previous day. The nurse should use which of the following terms to document this finding?
Explanation
Choice A reason: This statement is false. Balottement is a technique of palpating the uterus to detect the presence of a fetus. It is not a term used to describe the sensation of fetal movement.
Choice B reason: This statement is false. Fluttering is a common way that women describe the feeling of fetal movement, but it is not a medical term. The nurse should use a more precise and professional term to document this finding.
Choice C reason: This statement is false. Chloasma is a condition that causes patches of darkened skin on the face during pregnancy. It is not related to fetal movement or the sensation of it.
Choice D reason: This statement is true. Quickening is the term used to describe the first perception of fetal movement by the pregnant woman. It usually occurs between 16 and 20 weeks of gestation.
A nurse is caring for a newborn who was delivered by vacuum extraction and has swelling on his head that crosses the suture line. The newborn’s mother asks about the swelling on her newborn’s head. Which of the following responses should the nurse make?
Explanation
Choice A reason: This statement is true. A caput succedaneum is a localized swelling of the scalp that occurs due to the compression of the head during delivery. It can cross the suture lines and affect any part of the head. It usually resolves within a few days without treatment.
Choice B reason: This statement is false. A Mongolian spot is a bluish-gray or brown patch of skin that is present at birth or shortly after. It is more common in newborns of Asian, African, or Hispanic descent. It is not related to the delivery method or the swelling of the head.
Choice C reason: This statement is false. A cephalhematoma is a collection of blood between the skull and the periosteum that occurs due to the rupture of blood vessels during delivery. It does not cross the suture lines and is usually limited to one side of the head. It may take several weeks or months to resolve and can cause jaundice or anemia.
Choice D reason: This statement is false. Erythema toxicum is a benign rash that appears as red blotches with white or yellow papules in the center. It can occur anywhere on the body except the palms and soles. It is not related to the delivery method or the swelling of the head.
A nurse is caring for a newborn who is small for gestational age (SGA). Which of the following findings should the nurse expect?
Explanation
Choice A reason: This statement is false. Retinopathy is a condition that affects the blood vessels of the retina and can cause vision loss. It is more common in newborns who are large for gestational age (LGA) or have diabetes mellitus. It is not related to being SGA.
Choice B reason: This statement is false. Decreased circulating RBC is a condition that causes anemia and low oxygen levels. It is more common in newborns who have hemolytic disease, blood loss, or infection. It is not related to being SGA.
Choice C reason: This statement is false. A well rounded abdomen is a normal finding in a healthy newborn. It is not a sign of being SGA. In fact, a newborn who is SGA may have a scaphoid or sunken abdomen due to the lack of subcutaneous fat and muscle.
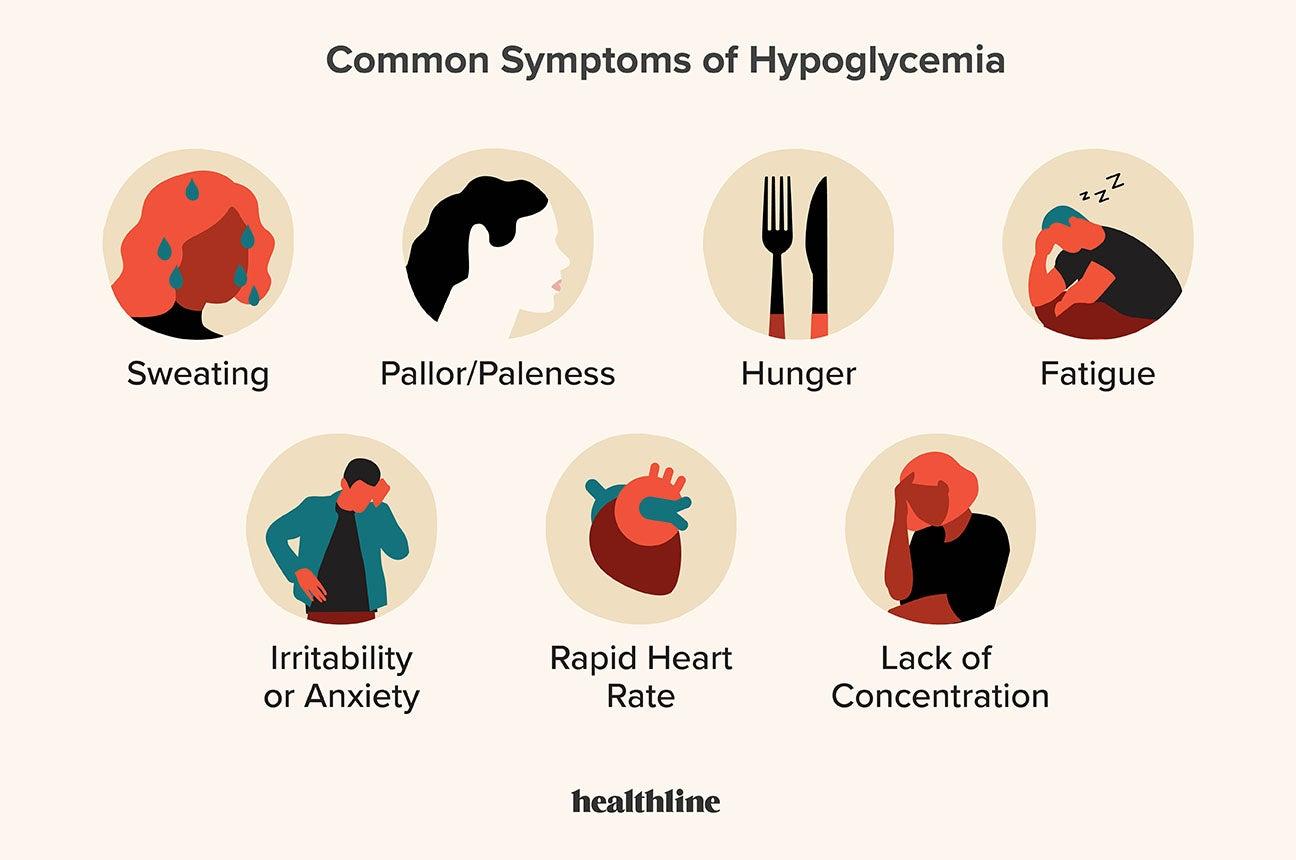
Choice D reason: This statement is true. Blood glucose instability is a condition that causes hypoglycemia or low blood sugar levels. It is more common in newborns who are SGA, as they have less glycogen stores and increased metabolic demands. It can cause jitteriness, lethargy, poor feeding, or seizures.
A nurse is caring for a couple who experienced a fetal death at 37 weeks of gestation. Which of the following responses by the nurse is therapeutic?
Explanation
Choice A reason: This statement is not therapeutic. It minimizes the couple's loss and implies that their grief is not valid. It may also make the couple feel guilty or angry.
Choice B reason: This statement is not therapeutic. It assumes the couple's religious beliefs and preferences. It may also make the couple feel pressured or judged.
Choice C reason: This statement is not therapeutic. It is intrusive and irrelevant. It may also make the couple feel blamed or defensive.
Choice D reason: This statement is therapeutic. It acknowledges the couple's pain and offers support and empathy. It also respects the couple's privacy and autonomy.
A nurse is reinforcing teaching about formula feeding to a group of parents of newborns. Which of the following statements by one of the parents indicates a need for further teaching?
Explanation
Choice A reason: This statement is true. Burping the baby half way through each feeding helps to release any air that the baby may have swallowed during feeding. This can prevent gas, colic, and spitting up.
Choice B reason: This statement is true. Giving formula to the baby at room temperature is acceptable and safe. There is no need to warm up the formula, unless the baby prefers it. However, if the formula is warmed, it should be tested before feeding to avoid burning the baby's mouth.
Choice C reason: This statement is false. Ensuring the baby's feedings last 10 to 15 minutes is not necessary or advisable. The duration of each feeding depends on the baby's appetite, hunger, and satisfaction. The baby should be allowed to feed at his or her own pace and stop when full. Forcing the baby to feed longer than he or she wants can cause overfeeding, vomiting, or obesity.
Choice D reason: This statement is true. Watching for signs that the baby is full and stopping the feeding is important to avoid overfeeding and respect the baby's cues. Some signs that the baby is full are turning away from the bottle, closing the mouth, falling asleep, or pushing the bottle away.
A nurse is caring for a couple who experienced a fetal death at 37 weeks of gestation. Which of the following responses by the nurse is therapeutic?
Explanation
Choice A reason: This statement is not therapeutic. It minimizes the couple's loss and implies that their grief is not valid. It may also make the couple feel guilty or angry.
Choice B reason: This statement is not therapeutic. It assumes the couple's religious beliefs and preferences. It may also make the couple feel pressured or judged.
Choice C reason: This statement is not therapeutic. It is intrusive and irrelevant. It may also make the couple feel blamed or defensive.
Choice D reason: This statement is therapeutic. It acknowledges the couple's pain and offers support and empathy. It also respects the couple's privacy and autonomy.
A nurse is collecting data from a newborn who is 48 hours old. Which of the following findings should the nurse report to the provider?
Explanation
Choice A reason: This statement is false. Erythema toxicum is a benign rash that appears as red blotches with white or yellow papules in the center. It can occur anywhere on the body except the palms and soles. It is not related to the delivery method or the swelling of the head.
Choice B reason: This statement is true. Jaundiced skin and yellow tinge to the sclera are signs of hyperbilirubinemia, which is a high level of bilirubin in the blood. Bilirubin is a waste product that results from the breakdown of red blood cells. It can cause brain damage if left untreated. The nurse should report this finding to the provider and check the newborn's bilirubin level.
Choice C reason: This statement is false. A Mongolian spot is a bluish-gray or brown patch of skin that is present at birth or shortly after. It is more common in newborns of Asian, African, or Hispanic descent. It is not related to the delivery method or the swelling of the head.
Choice D reason: This statement is false. Telangiectatic nevi are also known as stork bites or salmon patches. They are flat, pink, or red marks that appear on the eyelids, nose, forehead, or nape of the neck. They are caused by dilated capillaries and usually fade by the second year of life. They are not related to the delivery method or the swelling of the head.
A nurse is reinforcing teaching with a client who is at 34 weeks of gestation and at risk for placental abruption. The nurse recognizes that which of the following is the most common risk factor for a placental abruption?
Explanation
Choice A reason: This statement is incorrect. Maternal cigarette smoking is a risk factor for placental abruption, but not the most common one. Smoking during pregnancy can reduce the blood flow to the placenta and increase the risk of placental separation, but the effect is less pronounced than that of hypertension.
Choice B reason: This statement is incorrect. Maternal cocaine use is a risk factor for placental abruption, but not the most common one. Cocaine use during pregnancy can cause vasoconstriction and spasms of the blood vessels that supply the placenta, leading to placental ischemia and abruption.
Choice C reason: This statement is correct. Maternal hypertension is the most common risk factor for placental abruption, accounting for about 44% of cases. Hypertension during pregnancy can cause damage to the blood vessels in the placenta, resulting in placental infarction and detachment.
Choice D reason: This statement is incorrect. Maternal battering is a risk factor for placental abruption, but not the most common one. Trauma or injury to the abdomen during pregnancy can cause direct or indirect damage to the placenta, causing it to separate from the uterus..
A nurse is reinforcing teaching about nutritional needs with a client who is pregnant. Which of the following nutrients should the nurse instruct the client to increase during pregnancy?
Explanation
Choice A reason: This statement is false. Calcium is an important nutrient for the development of the fetal bones and teeth, but the recommended intake for pregnant women is the same as for non-pregnant women, which is 1000 mg per day. The fetus can obtain enough calcium from the mother's diet or bones without increasing the maternal need.
Choice B reason: This statement is true. Iron is an essential nutrient for the production of hemoglobin, which carries oxygen to the tissues. The recommended intake for pregnant women is higher than for non-pregnant women, which is 27 mg per day. This is because the mother needs more iron to support the increased blood volume, the placenta, and the fetus.
Choice C reason: This statement is false. Vitamin E is an antioxidant that protects the cells from damage, but the recommended intake for pregnant women is the same as for non-pregnant women, which is 15 mg per day. There is no evidence that increasing vitamin E intake during pregnancy has any benefits or harms.
Choice D reason: This statement is false. Vitamin D is a hormone that helps the body absorb calcium and phosphorus, but the recommended intake for pregnant women is the same as for non-pregnant women, which is 15 mcg per day. Vitamin D deficiency can cause rickets in the fetus, but this is rare in developed countries.
A nurse is reinforcing teaching with a client who is pregnant and has phenylketonuria (PKU). Which of the following foods should the nurse instruct the client to eliminate from her diet?
Explanation
Choice A reason: This statement is false. Potatoes are a low-protein food that can be included in the diet for PKU. They contain about 2 grams of protein and 60 mg of phenylalanine per 100 grams.
Choice B reason: This statement is true. Peanut butter is a high-protein food that should be eliminated from the diet for PKU. It contains about 25 grams of protein and 1,000 mg of phenylalanine per 100 grams.
Choice C reason: This statement is false. Broccoli is a low-protein food that can be included in the diet for PKU. It contains about 3 grams of protein and 70 mg of phenylalanine per 100 grams.
Choice D reason: This statement is false. Apple juice is a low-protein food that can be included in the diet for PKU. It contains about 0.1 grams of protein and 2 mg of phenylalanine per 100 grams.
A nurse is caring for a client who is at 38 weeks of gestation and has a positive contraction stress test. Which of the following actions should the nurse take?
Explanation
Choice A reason: This statement is true. A positive contraction stress test indicates that the fetal heart rate shows signs of deceleration or distress during uterine contractions. This can be a sign of placental insufficiency, fetal hypoxia, or cord compression. The nurse should prepare the client for admission to the hospital for further evaluation and possible delivery.
Choice B reason: This statement is false. Checking the client’s cervix for dilation is not a priority action for a positive contraction stress test. The nurse should focus on the fetal well-being and the need for immediate intervention.
Choice C reason: This statement is false. Documenting the findings as expected in the client records is not an appropriate action for a positive contraction stress test. The nurse should report the findings to the provider and follow the orders for the management of the situation.
Choice D reason: This statement is false. Repeating the contraction stress test in 24 hours is not a safe action for a positive contraction stress test. The nurse should not delay the diagnosis and treatment of the fetal compromise.
A nurse is collecting data from a newborn who weighs 5,160 g (11 lb, 6 oz) and whose mother has diabetes mellitus. For which of the following data should the nurse monitor?
Explanation
Choice A reason: This statement is false. Hypercalcemia is high levels of calcium in the blood and is not a common complication for a newborn of a diabetic mother. Hypercalcemia can cause muscle weakness, constipation, confusion, or kidney stones.
Choice B reason: This statement is false. Decreased RBC is low levels of red blood cells in the blood and is not a common complication for a newborn of a diabetic mother. Decreased RBC can cause anemia and low oxygen levels.
Choice C reason: This statement is true. Hypoglycemia is low levels of glucose in the blood and is a common complication for a newborn of a diabetic mother. Hypoglycemia can cause jitteriness, lethargy, poor feeding, or seizures.
Choice D reason: This statement is false. Hyperbilirubinemia is high levels of bilirubin in the blood and is not a common complication for a newborn of a diabetic mother. Hyperbilirubinemia can cause jaundice or yellowing of the skin and eyes.
A nurse is reinforcing teaching about a biophysical profile with a client who is at 40 weeks of gestation. The nurse should explain that this profile focuses on which of the following parameters? (Select all that apply.)
Explanation
Choice A reason: This statement is false. Nuchal translucency is a measurement of the fluid behind the neck of the fetus. It is done during the first trimester of pregnancy to screen for chromosomal abnormalities. It is not part of the biophysical profile.
Choice B reason: This statement is false. Fetal gender is the sex of the fetus. It can be determined by ultrasound or other tests, but it is not part of the biophysical profile.
Choice C reason: This statement is true. Fetal motion is one of the parameters of the biophysical profile. It assesses the activity and movement of the fetus. It indicates the fetal well-being and neurological development.
Choice D reason: This statement is true. Amniotic fluid volume is one of the parameters of the biophysical profile. It measures the amount of fluid surrounding the fetus. It indicates the fetal kidney function and placental function.
Choice E reason: This statement is true. Fetal breathing is one of the parameters of the biophysical profile. It evaluates the movement of the chest and diaphragm of the fetus. It indicates the fetal lung maturity and oxygenation.
Sign Up or Login to view all the 54 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
