Pre-eclampsia, Eclampsia > Maternal & Newborn
Exam Review
Diagnostic Criteria and Investigations
Total Questions : 16
Showing 16 questions, Sign in for moreA nurse is reviewing the results of a 24-hour urine collection for a client who is 32 weeks pregnant and has suspected pre-eclampsia.
Which of the following findings indicates proteinuria?
Explanation
Protein excretion of 450 mg indicates proteinuria.Proteinuria is the presence of excess protein in the urine, which can be a sign of kidney damage or disease.Normal protein excretion in a 24-hour urine collection is less than 150 mg.
Choice A is wrong because protein excretion of 150 mg is within the normal range.
Choice B is wrong because protein excretion of 250 mg is slightly above the normal range, but not enough to indicate proteinuria.
Choice C is wrong because protein excretion of 350 mg is also above the normal range, but not enough to indicate proteinuria.
Preeclampsia is a condition that affects some pregnant women, usually after 20 weeks of pregnancy.It causes high blood pressure and proteinuria, which can harm both the mother and the baby.A 24-hour urine collection is a simple lab test that measures what’s in the urine and checks kidney function.The test is done by collecting all the urine passed in a 24-hour period in a special container that must be kept cool until returned to the lab.
A nurse is performing a non-stress test (NST) for a client who is 34 weeks pregnant and has pre-eclampsia.
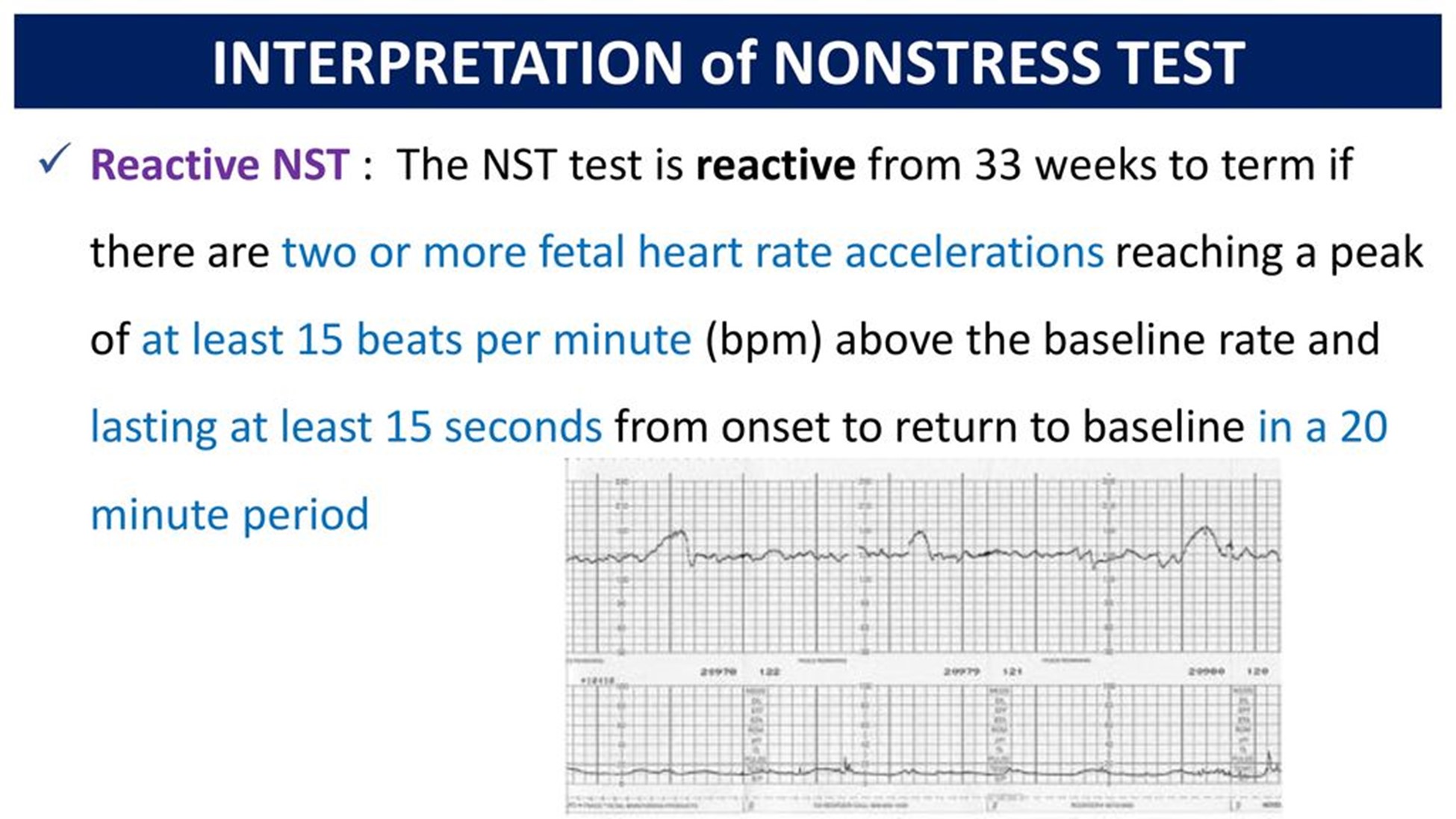
Which of the following fetal heart rate patterns indicates a reactive test?
Explanation
Two or more accelerations of at least 15 beats/min above baseline lasting for at least 15 seconds in a 20-minute period.This indicates a reactive test, which means that the fetus is well oxygenated and not in distress.
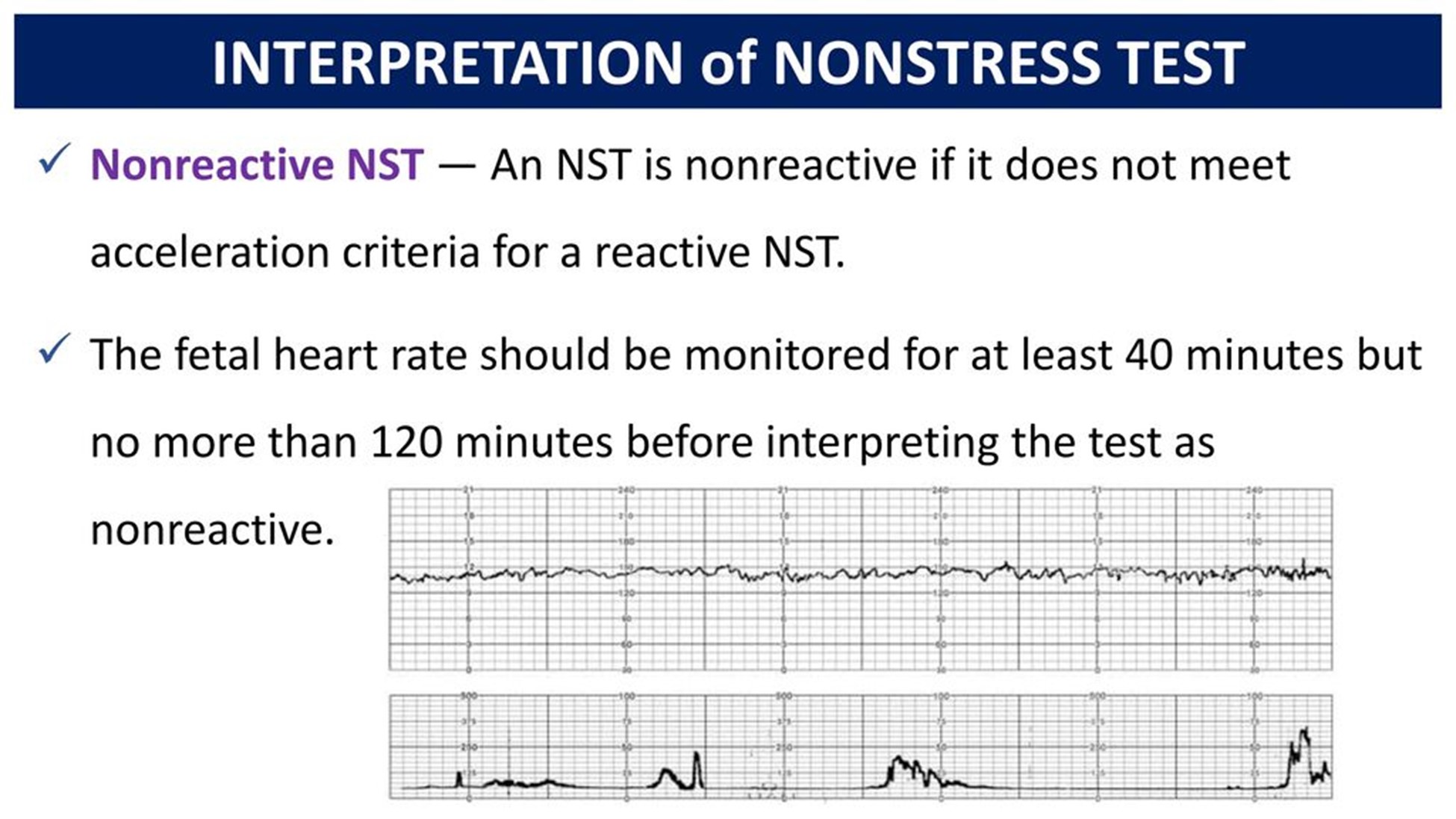
Choice B is wrong because no accelerations or decelerations in a 20-minute period indicate a non-reactive test, which may suggest fetal hypoxia or acidosis.
Choice C is wrong because one acceleration of at least 10 beats/min above baseline lasting for at least 10 seconds in a 20-minute period is the criterion for a reactive test for gestational age less than 32 weeks, not 34 weeks.
Choice D is wrong because variable decelerations with normal variability in a 20-minute period indicate cord compression or fetal head compression, not a reactive test.
A nurse is preparing to administer magnesium sulfate IV to a client who has severe pre-eclampsia.
Which of the following actions should the nurse take? (Select all that apply.)
Explanation
The correct answer is choice A, B, C and E.The nurse should monitor the client’s deep tendon reflexes hourly because magnesium sulfate can cause neuromuscular blockade and decreased reflexes.The nurse should keep calcium gluconate readily available because it is the antidote for magnesium toxicity.The nurse should maintain a urine output of at least 40 mL/hr because magnesium is excreted by the kidneys and low urine output can indicate renal impairment or fluid overload.The nurse should check the client’s blood pressure every 15 minutes because magnesium sulfate can cause hypotension and preeclampsia can cause hypertension.
Choice D is wrong because the medication should not be infused via a peripheral IV line, but rather through a central line or a large-bore IV catheter to prevent tissue damage.
A nurse is assessing a client who has eclampsia and is receiving magnesium sulfate IV.
Which of the following findings should alert the nurse to suspect magnesium toxicity?
Explanation
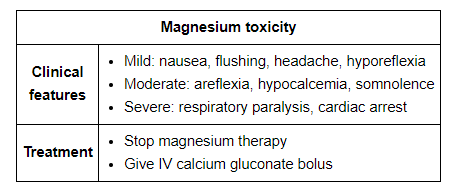
This indicates that the client has respiratory depression, which is a sign of magnesium toxicity.Magnesium sulfate is given to prevent and treat seizures in clients with eclampsia, but it can also cause adverse effects such as hypotension, decreased urine output, absent or diminished reflexes, and cardiac arrest.
Choice B is wrong because urine output of 50 mL/hr is within the normal range and does not indicate magnesium toxicity.The nurse should monitor the client’s urine output closely and report any decrease below 30 mL/hr.
Choice C is wrong because serum magnesium level of 6 mg/dL is within the therapeutic range of 4 to 7 mg/dL for clients receiving magnesium sulfate.The nurse should monitor the client’s serum magnesium level regularly and report any increase above 8 mg/dL, which indicates toxicity.
Choice D is wrong because patellar reflex of 2+ is normal and does not indicate magnesium toxicity.The nurse should assess the client’s deep tendon reflexes frequently and report any decrease or absence of reflexes, which indicates toxicity.
A nurse is caring for a client with severe pre-eclampsia who is receiving magnesium sulfate intravenously.
What is the primary reason for administering magnesium sulfate to this client?
Explanation
A. To prevent seizures.
Magnesium sulfate is a mineral that can reduce seizure risks in women with severe preeclampsia.It is often given intravenously and can also be used to prolong pregnancy for up to two days.Magnesium sulfate is also used to prevent and manage seizures in women with postpartum preeclampsia.
• Statement B is wrong because magnesium sulfate does not lower blood pressure.It may be given along with medications that help reduce blood pressure.
• Statement C is wrong because magnesium sulfate does not induce labor.It may be given to delay delivery for up to 48 hours to allow time for the administration of drugs that speed up the baby’s lung development.
• Statement D is wrong because magnesium sulfate does not reduce edema.Edema is a common symptom of preeclampsia, but it is not a direct cause of complications.
A nurse is monitoring a client with severe pre-eclampsia who is receiving magnesium sulfate intravenously.
Which of the following signs indicates magnesium toxicity and requires immediate intervention?
Explanation
According to Mayo Clinic, loss of reflexes is a sign of magnesium toxicity and requires immediate intervention.
Other signs of magnesium toxicity include:
• Decreased urine output
• Difficulty breathing
• Drowsiness or confusion
• Low blood pressure
• Slow heart rate
• Weakness
Choice B is wrong because headache is not a sign of magnesium toxicity.
It may be a symptom of preeclampsia or other conditions, but it does not indicate an overdose of magnesium sulfate.
Choice C is wrong because nausea is not a sign of magnesium toxicity.
It may be a side effect of magnesium sulfate or a symptom of preeclampsia or other conditions, but it does not indicate an overdose of magnesium sulfate.
Choice D is wrong because blurred vision is not a sign of magnesium toxicity.
It may be a symptom of preeclampsia or other conditions, but it does not indicate an overdose of magnesium sulfate.
A nurse is preparing to administer antihypertensive therapy to a client with severe pre-eclampsia.
Which of the following blood pressure readings is the target goal for this client?
Explanation
The target blood pressure goal for a client with severe pre-eclampsia is less than 160/110 mmHg.
This is because lowering the blood pressure too much or too fast can compromise the placental perfusion and fetal oxygenation.
Choice A is wrong because it is the target blood pressure goal for a client with chronic hypertension or gestational hypertension without severe features.
Choice B is wrong because it is the target blood pressure goal for a client with mild pre-eclampsia.
Choice D is wrong because it is too high and can increase the risk of maternal and fetal complications such as stroke, eclampsia, placental abruption, and fetal growth restriction.
Normal blood pressure ranges are less than 120/80 mmHg for systolic and diastolic pressures respectively.
A nurse is administering corticosteroids to a client with severe pre-eclampsia who is 32 weeks pregnant.
What is the main purpose of giving corticosteroids to this client?
Explanation
To accelerate fetal lung maturity.Corticosteroids are given to pregnant women with severe pre-eclampsia who are at risk of preterm delivery to help the development of the fetus’s lungs and reduce the risk of respiratory distress syndrome.
This can improve the survival and health outcomes of the newborn.
Choice A is wrong because corticosteroids do not reduce inflammation in pre-eclampsia.They are used for other inflammatory conditions such as asthma or arthritis.
Choice B is wrong because corticosteroids do not prevent infection in pre-eclampsia.They can actually increase the risk of infection by suppressing the immune system.
Choice D is wrong because corticosteroids do not increase platelet count in pre-eclampsia.They can actually decrease the platelet count by causing thrombocytopenia.
A nurse is assessing the fetal heart rate and uterine activity of a client with severe pre-eclampsia who is receiving magnesium sulfate intravenously.
Which of the following findings should the nurse report to the provider immediately?
Explanation
C. Fetal heart rate decelerations.
Fetal heart rate decelerations are temporary drops in the fetal heart rate that can indicate fetal distress or lack of oxygen.There are three types of decelerations: early, late and variable.Early decelerations are benign and caused by compression of the fetus’s head during a uterine contraction.Late decelerations are caused by uteroplacental insufficiency, which is a decrease in blood flow to the placenta.Variable decelerations are the most common type and vary in shape, duration and intensity.They are often caused by cord compression or other factors that affect fetal oxygenation.
•
A. Fetal heart rate of 140 beats per minute.
Statement is wrong because this is a normal fetal heart rate.The normal range for fetal heart rate is 120-160 beats per minute.
•
B. Uterine contractions every 10 minutes.
Statement is wrong because this is a normal frequency for uterine contractions during early labor.
The normal range for uterine contractions is 5-10 minutes apart.
•
D. Uterine contractions lasting 60 seconds.
Statement is wrong because this is a normal duration for uterine contractions during active labor.
The normal range for uterine contractions is 45-90 seconds long.
A nurse is caring for a client with eclampsia who is receiving magnesium sulfate intravenously.
Which of the following findings indicates magnesium toxicity?
Explanation
Fetal heart rate decelerations indicate a possible compromise of fetal oxygenation and should be reported to the provider immediately.Decelerations can be caused by various factors such as cord compression, uterine hyperstimulation, maternal hypotension, or placental abruption.
Choice A is wrong because a fetal heart rate of 140 beats per minute is within the normal range of 110 to 160 beats per minute.
Choice B is wrong because uterine contractions every 10 minutes are not abnormal in a client with severe pre-eclampsia who is receiving magnesium sulfate.Magnesium sulfate is used to prevent seizures and lower blood pressure in pre-eclampsia, but it does not stop labor.
Choice D is wrong because uterine contractions lasting 60 seconds are not a sign of …
A nurse is preparing to administer hydralazine to a client with eclampsia who has a blood pressure of 180/120 mmHg.
What is the rationale for administering this medication?
Explanation
To increase placental perfusion.
Hydralazine is an antihypertensive drug that dilates the blood vessels and lowers the blood pressure.By doing so, it improves the blood flow to the placenta and reduces the risk of fetal hypoxia and growth restriction.
Choice A is wrong because hydralazine does not prevent cerebral edema.
Cerebral edema is a complication of severe preeclampsia or eclampsia that can cause seizures, headaches, and visual disturbances.Hydralazine may lower the blood pressure and reduce the risk of stroke, but it does not directly affect the brain swelling.
Choice B is wrong because hydralazine does not reduce uterine contractions.
Uterine contractions are stimulated by oxytocin and prostaglandins, which are not affected by hydralazine.Hydralazine may cause reflex tachycardia, which can increase the cardiac output and uterine blood flow, but it does not alter the uterine muscle activity.
Choice D is wrong because hydralazine does not promote diuresis.
Diuresis is the increased production of urine by the kidneys.
Hydralazine may cause fluid retention and edema by activating the renin-angiotensin-aldosterone system, which increases sodium and water reabsorption.Hydralazine may also cause a decrease in renal perfusion and glomerular filtration rate, which can impair the kidney function and urine output.
A nurse is assessing a client with eclampsia who is having a seizure.
Which of the following actions should the nurse take first?
Explanation
Turn the client to the side.This is because turning the client to the side will prevent aspiration and maintain a patent airway during a seizure.
Some possible explanations for the other choices are:
• Choice B. Insert an oral airway.This is wrong because inserting an oral airway during a seizure can cause injury to the client’s mouth or teeth, and it can also stimulate the gag reflex and increase the risk of vomiting and aspiration.
• Choice C. Administer oxygen via face mask.This is wrong because administering oxygen via face mask during a seizure can be difficult and ineffective, as the client may not be able to breathe through the mask or may dislodge it with their movements.Oxygen can be given after the seizure has stopped, if needed.
• Choice D. Document the duration of the seizure.
This is wrong because documenting the duration of the seizure is not a priority action during a seizure.The nurse should first ensure the client’s safety and airway patency, and then document the seizure characteristics after it has ended.
A nurse is teaching a client with eclampsia about the purpose of corticosteroid therapy.
Which of the following statements by the client indicates understanding of the teaching?
Explanation
“This medication will help my baby’s lungs develop faster.” Corticosteroid therapy is given to pregnant clients with eclampsia to accelerate fetal lung maturity and reduce the risk of respiratory distress syndrome in the newborn.
Some possible explanations for the other choices are:
• Choice A is wrong because corticosteroids do not lower blood pressure.Antihypertensive drugs such as hydralazine or labetalol are used to treat hypertension in eclampsia.
• Choice B is wrong because corticosteroids do not prevent seizures.Magnesium sulfate is the drug of choice for seizure prophylaxis and treatment in eclampsia.
• Choice D is wrong because corticosteroids do not reduce inflammation in the body.They may have anti-inflammatory effects in some conditions, but their main purpose in eclampsia is to enhance fetal lung development.
Normal ranges for blood pressure and proteinuria in pregnancy are:
• Blood pressure: less than 140/90 mm Hg
• Proteinuria: less than 300 mg/24 hours or less than 1+ on dipstick
(select all that apply) A nurse is planning care for a client with eclampsia who is scheduled for delivery as soon as possible.
Which of the following interventions should the nurse include in the plan? (Select all that apply.)
Explanation
Answer is A and C. Eclampsia is a life-threatening complication of pregnancy that causes seizures due to severe hypertension.The nurse should monitor the fetal heart rate and uterine activity continuously to assess for signs of fetal distress or placental abruption.The nurse should also maintain a dark and quiet environment to reduce stimuli that might trigger seizures.
Statement B is wrong because administering oxytocin to augment labor can increase the risk of uterine rupture and placental abruption in a patient with eclampsia.
Statement D is wrong because encouraging oral fluids and a high-protein diet can worsen the fluid retention and renal impairment in a patient with eclampsia.
Statement E is wrong because assessing for signs of placental abruption is not enough.The nurse should also monitor the vital signs, urine output, neurological status, and laboratory values of the patient with eclampsia.
Normal ranges for blood pressure are less than 120/80 mmHg for non-pregnant adults and less than 140/90 mmHg for pregnant women.Normal ranges for protein in urine are less than 150 mg/day for non-pregnant adults and less than 300 mg/day for pregnant women.
A nurse is caring for a client with HELLP syndrome who is receiving magnesium sulfate intravenously.
What is the main purpose of this medication?
Explanation
Maintain a dark and quiet environment.This intervention helps to reduce sensory stimulation and prevent seizures in a client with eclampsia.
Choice A is wrong becausemonitoring fetal heart rate and uterine activity continuouslyis not a priority intervention for a client with eclampsia.The priority is to prevent seizures and control blood pressure.
Choice B is wrong becauseadministering oxytocin to augment laboris contraindicated in a client with eclampsia.Oxytocin can increase blood pressure and cause uterine hyperstimulation, which can worsen the condition and endanger the mother and the fetus.
Choice D is wrong becauseencouraging oral fluids and a high-protein dietis not appropriate for a client with eclampsia.
The client should be kept NPO to prevent aspiration in case of a seizure.A high-protein diet can increase the risk of renal failure and hepatic dysfunction.
Choice E is wrong becauseassessing for signs of placental abruptionis not a specific intervention for a client with eclampsia.Placental abruption can occur as a complication of eclampsia, but it is not the main focus of care.
A nurse is reviewing the laboratory results of a client with HELLP syndrome.
Which of the following findings would indicate hemolysis?
Explanation
Elevated serum lactate dehydrogenase (LDH) indicates hemolysis, which is one of the components of HELLP syndrome.Hemolysis is the destruction of red blood cells that occurs when they pass through damaged blood vessels.
Choice A is wrong because elevated serum creatinine indicates kidney dysfunction, which is not specific for hemolysis.
Choice C is wrong because elevated serum alkaline phosphatase (ALP) indicates liver damage, which is another component of HELLP syndrome, but not specific for hemolysis.
Choice D is wrong because elevated serum uric acid indicates increased purine metabolism, which can be associated with preeclampsia and HELLP syndrome, but not specific for hemolysis.
Sign Up or Login to view all the 16 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
