Final med surg comprehensive exam(Brooklyn university)
Total Questions : 75
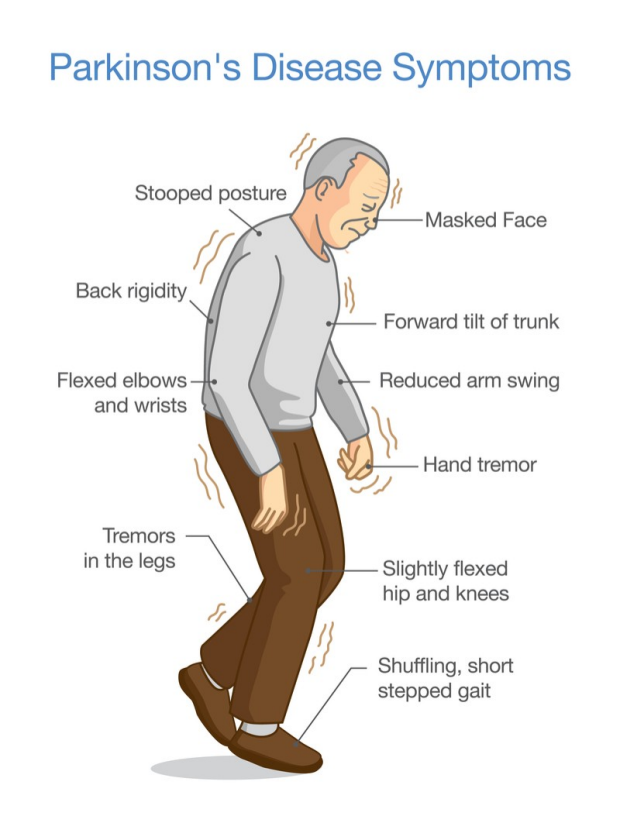
Showing 25 questions, Sign in for moreA client with Parkinson’s disease (PD) is being discharged home with his wife. To ensure success with the management plan, which discharge action is most effective?
Explanation
Choice A Reason:
Telling his wife what the client needs is not the most effective discharge action. While it is important for the wife to understand the client’s needs, this approach is too passive and does not actively engage the client or his wife in the care process. Effective management of Parkinson’s disease requires active participation from both the client and the caregiver to ensure adherence to the care plan and to address any concerns or preferences they may have.
Choice B Reason:
Setting up visitations by a home health nurse can be beneficial, but it is not the most effective discharge action on its own. Home health nurses can provide valuable support and monitoring, but the success of the management plan also depends on the involvement and commitment of the client and his wife. Without their active participation, the care plan may not be fully effective.
Choice C Reason:
Involving the client and his wife in developing a plan of care is the most effective discharge action. This approach ensures that both the client and his wife are fully engaged in the care process, understand the management plan, and are more likely to adhere to it. Collaborative care planning allows for the consideration of the client’s and caregiver’s preferences, needs, and concerns, leading to a more personalized and effective care plan. This active involvement can also empower the client and his wife, improving their confidence in managing the disease.
Choice D Reason:
Writing up a detailed plan of care according to standards is important, but it is not the most effective discharge action if done in isolation. A standardized care plan may not address the unique needs and preferences of the client and his wife. Without their involvement in the development of the plan, there may be a lack of understanding or commitment to the care plan, reducing its effectiveness. Personalizing the care plan through active involvement of the client and his wife is crucial for successful management.
The nurse administers amiodarone to a client with ventricular tachycardia. Which monitoring by the nurse is necessary with this drug? (Select all that apply)
Explanation
Choice A Reason:
Monitoring the QT interval is crucial when administering amiodarone because this drug can prolong the QT interval, increasing the risk of torsades de pointes, a potentially life-threatening form of ventricular tachycardia. The QT interval represents the time it takes for the heart’s ventricles to depolarize and repolarize, and prolongation can lead to arrhythmias. Regular monitoring helps in early detection and prevention of such adverse effects.
Choice B Reason:
Heart rate monitoring is essential when administering amiodarone because the drug can cause bradycardia (a slower than normal heart rate). Amiodarone affects the electrical conduction system of the heart, which can lead to significant changes in heart rate. Monitoring the heart rate ensures that any bradycardia is detected early and managed appropriately to prevent complications such as hypotension or heart failure.
Choice C Reason:
While respiratory rate monitoring is important in general patient care, it is not specifically necessary for monitoring the effects of amiodarone. Amiodarone primarily affects the heart’s electrical activity and has less direct impact on respiratory function. However, in cases of severe adverse reactions, such as pulmonary toxicity, respiratory monitoring may become relevant.
Choice D Reason:
Monitoring heart rhythm is vital when administering amiodarone because the drug is used to treat arrhythmias and can also cause new arrhythmias or exacerbate existing ones. Continuous ECG monitoring helps in detecting any abnormal heart rhythms early, allowing for timely intervention. This is particularly important in patients with a history of arrhythmias or those receiving high doses of amiodarone.
Choice E Reason:
Urine output monitoring is not specifically necessary for patients receiving amiodarone. While maintaining adequate urine output is important for overall patient health, amiodarone does not typically affect renal function directly. Therefore, urine output monitoring is not a primary concern when administering this medication.
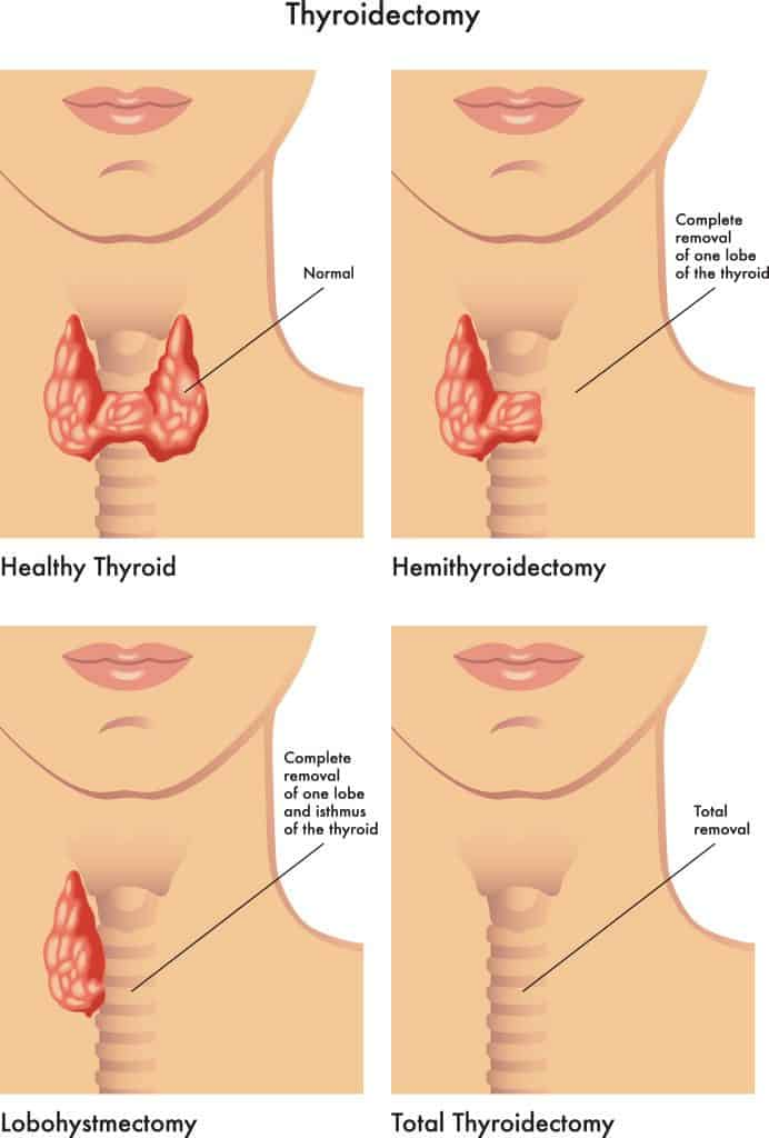
A postoperative client following a thyroidectomy suddenly develops difficulty breathing, stridor, and an increase in swelling of the anterior neck area. What should the nurse do first?
Explanation
Choice A reason: The first priority in this situation is to ensure the client’s airway is secure. Difficulty breathing and stridor indicate a potential airway obstruction, which can be life-threatening. Activating the hospital’s emergency or rapid response system ensures that the client receives immediate medical attention from a team equipped to handle such emergencies. This step is crucial to prevent respiratory arrest and other complications.
Choice B reason: While placing a heart monitor on the client and observing for dysrhythmias is important, it is not the immediate priority in this scenario. The client’s airway and breathing take precedence over monitoring heart rhythms. Once the airway is secured and breathing is stabilized, then monitoring for dysrhythmias can be considered.
Choice C reason: Asking the charge nurse to come see the client immediately is a reasonable action, but it is not the most effective first step. The charge nurse may not have the necessary equipment or expertise to handle an acute airway obstruction. Activating the emergency or rapid response system ensures that a specialized team responds quickly.
Choice D reason: Checking the client’s blood pressure and heart rate is important for overall assessment, but it is not the immediate priority when there is a potential airway obstruction. Ensuring the client can breathe is the most critical action. Vital signs can be checked once the airway is secured.
Choice E reason: Providing a calm and assuring environment for the client is beneficial for reducing anxiety, but it does not address the immediate threat to the client’s airway. While maintaining a calm environment is important, the nurse must first ensure the client’s airway is open and breathing is adequate.
Choice F reason: Placing the emergency cart at the bedside is a preparatory step that can be useful, but it is not the first action to take. The nurse should first activate the emergency or rapid response system to get immediate help. The emergency cart can be brought to the bedside by the responding team.
The nurse is caring for a patient on a telemetry unit who has a regular heart rhythm and rate of 60 beats/min; a P wave precedes each QRS complex, and the PR interval is 0.20 seconds. Additional vital signs are: blood pressure 118/68 mm Hg, respiratory rate 16 breaths/min, and temperature 98.8°F (37°C). All of these medications are available on the medication record. What action will the nurse take?
Explanation
Choice A Reason:
Continuing to monitor is the most appropriate action in this scenario. The patient has a regular heart rhythm and a heart rate of 60 beats per minute, which is within the normal range for sinus bradycardia. The PR interval is 0.20 seconds, which is at the upper limit of normal. The patient’s vital signs are stable, with a blood pressure of 118/68 mm Hg, a respiratory rate of 16 breaths per minute, and a temperature of 98.8°F (37°C). There are no signs of hemodynamic instability or symptoms that would necessitate immediate intervention. Therefore, ongoing monitoring is sufficient to ensure the patient’s condition remains stable.
Choice B Reason:
Administering clonidine is not appropriate in this situation. Clonidine is an antihypertensive medication that can lower blood pressure and heart rate. Given that the patient’s blood pressure and heart rate are within normal ranges, administering clonidine could potentially cause hypotension and bradycardia, leading to adverse effects. Therefore, clonidine is not indicated for this patient.
Choice C Reason:
Administering atropine is not necessary for this patient. Atropine is used to treat symptomatic bradycardia, where the heart rate is abnormally slow and causing symptoms such as dizziness, hypotension, or syncope. In this case, the patient’s heart rate is 60 beats per minute, which is within the normal range for sinus bradycardia, and there are no symptoms indicating the need for atropine. Therefore, atropine is not required.
Choice D Reason:
Administering digoxin is also not appropriate. Digoxin is a cardiac glycoside used to treat heart failure and certain types of arrhythmias, such as atrial fibrillation. It can slow the heart rate and increase the force of cardiac contractions. In this scenario, the patient does not have any indications for digoxin therapy, such as heart failure or atrial fibrillation, and their heart rate is already within the normal range. Therefore, digoxin is not indicated.
An adult client who has been experiencing a seizure for approximately 15 minutes is brought to the emergency department by private vehicle. Which intervention should the nurse implement first?
Explanation
Choice A Reason:
Administering levetiracetam intravenously is not the first intervention. While levetiracetam is an antiepileptic drug used to control seizures, it is not the first-line treatment for an ongoing seizure, especially one lasting as long as 15 minutes. The priority in this situation is to stop the seizure activity immediately to prevent further complications, such as neuronal damage or status epilepticus. Levetiracetam may be used later for maintenance therapy, but it is not the initial emergency intervention.
Choice B Reason:
Obtaining a STAT electroencephalogram (EEG) is important for diagnosing and understanding the type of seizure activity, but it is not the first intervention. The immediate priority is to stop the seizure. An EEG can be performed after the seizure has been controlled to assess brain activity and guide further treatment. Delaying the administration of an anticonvulsant to perform an EEG could result in prolonged seizure activity and increased risk of complications.
Choice C Reason:
Administering lorazepam intravenously is the most appropriate first intervention. Lorazepam is a benzodiazepine that acts quickly to stop seizure activity. It is the drug of choice for treating status epilepticus and prolonged seizures because of its rapid onset and effectiveness. Administering lorazepam helps to quickly terminate the seizure, reducing the risk of complications and stabilizing the patient for further evaluation and treatment.
Choice D Reason:
Obtaining a STAT 12-lead electrocardiogram (ECG) is not the first intervention. While an ECG can provide valuable information about the patient’s cardiac status, it does not address the immediate need to stop the seizure. The priority is to administer an anticonvulsant to terminate the seizure. Once the seizure is controlled, an ECG can be performed to assess any potential cardiac issues, especially if the patient has a history of cardiac problems or if the seizure was triggered by a cardiac event.
A client with chronic lung disease is prescribed 40% oxygen via face mask. Which finding indicates to the nurse that the client is experiencing oxygen toxicity? Select all that apply.
Explanation
Choice A reason: Pink frothy sputum is a classic sign of pulmonary edema, which can occur as a result of oxygen toxicity. When the alveoli in the lungs fill with fluid, it can lead to this type of sputum. This is a critical indicator that the client is experiencing severe respiratory distress and requires immediate medical attention.
Choice B reason: Substernal discomfort or chest pain is another symptom of oxygen toxicity. This discomfort arises due to the irritation and inflammation of the lung tissues caused by high levels of oxygen. It is essential to monitor and address this symptom promptly to prevent further complications.
Choice C reason: Nail clubbing is typically associated with chronic hypoxia and long-term lung diseases, but it is not an acute indicator of oxygen toxicity. Therefore, it is not relevant in this context.
Choice D reason: Restlessness is a common early sign of hypoxia and can also indicate oxygen toxicity. When the brain does not receive adequate oxygen, it can lead to symptoms such as restlessness, confusion, and agitation. This symptom should be taken seriously and addressed immediately.
Choice E reason: Cyanosis at the nail beds indicates a lack of oxygen in the blood, but it is not specific to oxygen toxicity. It can occur in various conditions where there is inadequate oxygenation, such as chronic obstructive pulmonary disease (COPD) or heart failure.
The nurse administers amiodarone to a client with ventricular tachycardia. Which monitoring by the nurse is necessary with this drug? (Select all that apply)
Explanation
Choice A reason: Monitoring the heart rate is crucial when administering amiodarone, as this drug can cause bradycardia (a slower than normal heart rate). Amiodarone affects the electrical conduction system of the heart, and close monitoring helps ensure that the heart rate remains within a safe range. The normal resting heart rate for adults is typically between 60 and 100 beats per minute.
Choice B reason: Respiratory rate monitoring is essential because amiodarone can cause pulmonary toxicity, which may manifest as interstitial pneumonitis or pulmonary fibrosis. Early detection of respiratory changes can help prevent severe complications. The normal respiratory rate for adults is 12 to 20 breaths per minute.
Choice C reason: Monitoring heart rhythm is necessary because amiodarone is used to treat arrhythmias, and it can also cause new arrhythmias or exacerbate existing ones. Continuous ECG monitoring helps detect any abnormal rhythms early, allowing for prompt intervention. Normal sinus rhythm is characterized by a regular rhythm with a rate of 60 to 100 beats per minute.
Choice D reason: Cardiac output monitoring is important because amiodarone can affect the contractility of the heart and overall cardiac function. Cardiac output is a measure of the amount of blood the heart pumps in one minute, and it is crucial for ensuring adequate tissue perfusion. Normal cardiac output ranges from 4 to 8 liters per minute in adults.
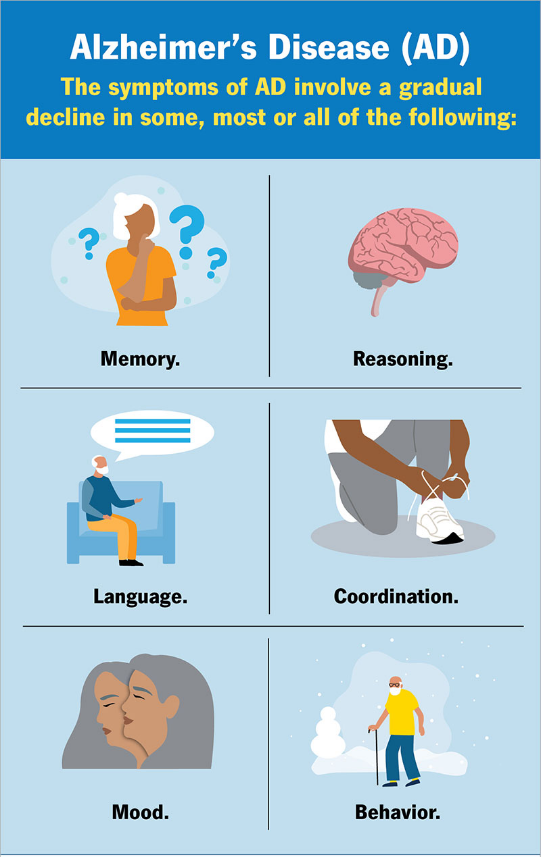
The nurse is planning health teaching for a client starting on donepezil for Alzheimer’s disease (AD). For which side effect will the nurse teach the family to monitor?
Explanation
Choice A Reason:
Low oxygen saturation is not a common side effect of donepezil. Donepezil is a cholinesterase inhibitor used to treat symptoms of Alzheimer’s disease by increasing the levels of acetylcholine in the brain. While it can have various side effects, respiratory issues like low oxygen saturation are not typically associated with this medication. Therefore, monitoring for low oxygen saturation is not a primary concern for patients starting donepezil.
Choice B Reason:
High blood pressure is also not a common side effect of donepezil. The medication primarily affects the central nervous system and does not typically cause significant changes in blood pressure. While it is always important to monitor a patient’s overall health, high blood pressure is not a side effect specifically linked to donepezil use. Therefore, it is not a primary focus for monitoring in this context.
Choice C Reason:
Elevated body temperature is not commonly associated with donepezil. The side effects of donepezil are more likely to involve gastrointestinal issues such as nausea, vomiting, and diarrhea, as well as muscle cramps and fatigue. Elevated body temperature is not a typical reaction to this medication, so it is not a primary concern for monitoring.
Choice D Reason:
Low pulse rate, or bradycardia, is a known side effect of donepezil. Donepezil can increase the levels of acetylcholine, which can affect the heart’s electrical conduction system and lead to a slower heart rate. This can be particularly concerning in elderly patients or those with pre-existing heart conditions. Therefore, it is crucial for the nurse to teach the family to monitor the client’s pulse rate regularly and report any significant decreases to the healthcare provider.
A nurse is providing teaching for a client who has a new diagnosis of gastroesophageal reflux disease (GERD). The client asks about foods he should avoid eating. Which of the following foods should the nurse tell him to avoid?
Explanation
Choice A Reason:
Nonfat milk is generally considered safe for individuals with GERD. While full-fat dairy products can exacerbate GERD symptoms due to their high-fat content, nonfat milk does not have this effect. It is low in fat and unlikely to trigger acid reflux. Therefore, nonfat milk is not a food that needs to be avoided by someone with GERD.
Choice B Reason:
Apples are typically safe for individuals with GERD. In fact, non-citrus fruits like apples are often recommended as part of a GERD-friendly diet. They are low in acid and unlikely to cause reflux symptoms. Therefore, apples do not need to be avoided by someone with GERD.
Choice C Reason:
Chocolate is a common trigger for GERD symptoms. It contains caffeine and theobromine, both of which can relax the lower esophageal sphincter (LES), allowing stomach acid to escape into the esophagus and cause reflux. Additionally, chocolate is high in fat, which can further exacerbate GERD symptoms. Therefore, it is advisable for individuals with GERD to avoid chocolate to prevent worsening of their symptoms.
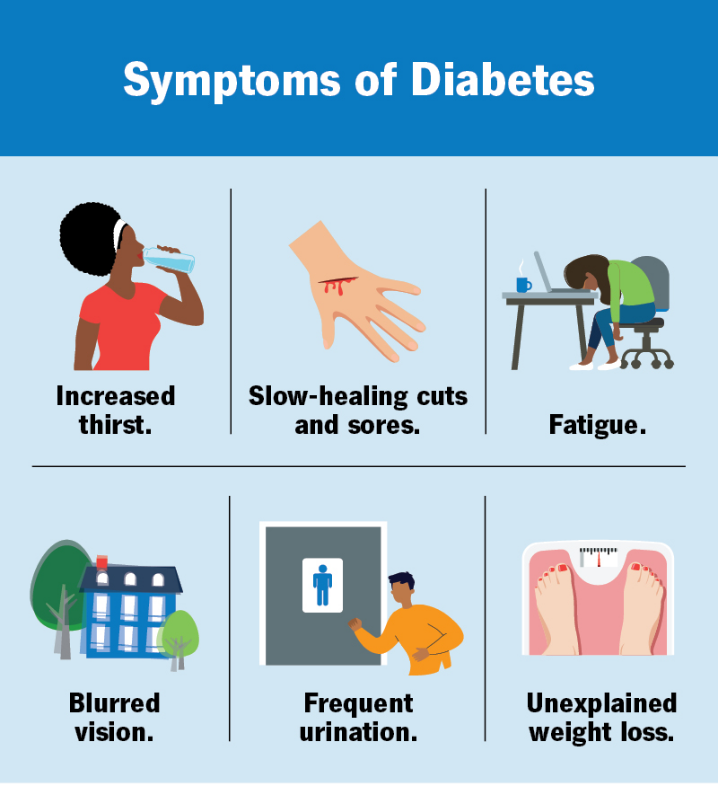
A nurse is providing teaching to a client who has diabetes mellitus about carbohydrate intake needs when exercising. Which of the following foods should the nurse include as containing a 15 g serving of carbohydrates?
Explanation
Choice A reason: One cup of milk contains approximately 15 grams of carbohydrates. Milk is a good source of carbohydrates, protein, and calcium, making it a suitable option for maintaining blood glucose levels during exercise. It is important for individuals with diabetes to monitor their carbohydrate intake to manage their blood sugar levels effectively.
Choice B reason: Half a cup of regular ice cream contains around 15 grams of carbohydrates. However, ice cream also contains high levels of sugar and fat, which may not be the healthiest option for regular consumption, especially for individuals with diabetes. While it can be included occasionally, it is better to choose healthier carbohydrate sources.
Choice C reason: One slice of bread typically contains about 15 grams of carbohydrates. Bread, especially whole grain or whole wheat varieties, can be a good source of carbohydrates for individuals with diabetes. It provides fiber, which helps in maintaining stable blood sugar levels.
Choice D reason: One cup of sugar-free yogurt does not contain 15 grams of carbohydrates. Sugar-free yogurt usually has fewer carbohydrates compared to regular yogurt. It is important to read the nutritional labels to determine the exact carbohydrate content. Regular yogurt, on the other hand, can be a good source of carbohydrates.
A nurse in a PACU is assessing a client who has a newly created colostomy. Which of the following findings should the nurse report to the provider?
Explanation
Choice A Reason:
A rosebud-like stoma orifice is a normal finding for a newly created colostomy. This appearance indicates that the stoma is healthy and well-formed. The stoma should protrude slightly from the abdomen and have a pink or red color, similar to the inside of the mouth. This indicates good blood flow and proper healing. Therefore, a rosebud-like stoma orifice does not need to be reported to the provider.
Choice B Reason:
A stoma oozing red drainage can be concerning, but it is not uncommon for a new stoma to have some minor bleeding or oozing, especially in the immediate postoperative period. This can occur due to the delicate nature of the tissue and the recent surgical intervention. However, if the drainage is excessive or persistent, it should be monitored closely and reported if it does not improve. Minor oozing is generally expected and does not necessarily indicate a serious problem.
Choice C Reason:
A shiny, moist stoma is a normal finding and indicates that the stoma is healthy. The stoma should be moist and have a shiny appearance, similar to the inside of the mouth. This moisture is necessary for the proper function and health of the stoma. Therefore, a shiny, moist stoma does not need to be reported to the provider.
Choice D Reason:
A purplish-colored stoma is an abnormal finding and should be reported to the provider immediately. This discoloration can indicate compromised blood flow to the stoma, which can lead to tissue necrosis if not addressed promptly. A healthy stoma should be pink or red, indicating good blood circulation. Any deviation from this color, especially a purplish or dark color, is a sign of potential ischemia or other serious complications that require immediate medical attention.
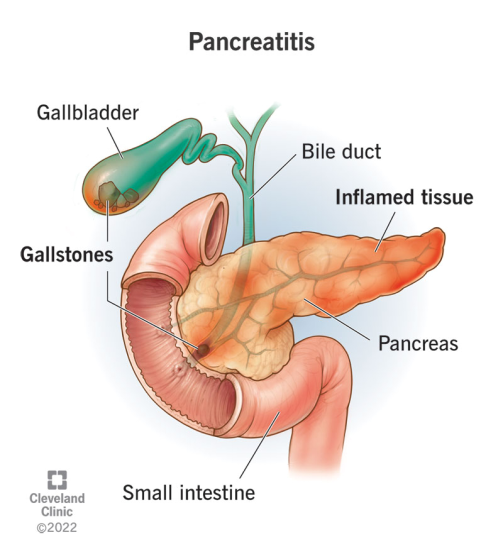
A nurse admits a client to the emergency department who reports nausea and vomiting that worsens when he lies down. Antacids do not help. The provider suspects acute pancreatitis. Which of the following laboratory test results should the nurse expect to see?
Explanation
Choice A Reason:
Increased serum amylase is a key indicator of acute pancreatitis. Amylase is an enzyme produced by the pancreas to help digest carbohydrates. In cases of acute pancreatitis, the pancreas becomes inflamed, leading to the release of amylase into the bloodstream. Elevated levels of serum amylase, typically more than three times the upper limit of normal, are a strong indication of acute pancreatitis. This enzyme level usually rises within a few hours of the onset of pancreatitis and can remain elevated for several days.
Choice B Reason:
Increased serum calcium is not typically associated with acute pancreatitis. In fact, acute pancreatitis can often lead to hypocalcemia (low calcium levels) due to fat saponification in the pancreas, where calcium binds with fatty acids. Therefore, an increase in serum calcium would not be expected in a patient with acute pancreatitis. Monitoring calcium levels is important, but an increase is not a diagnostic marker for this condition.
Choice C Reason:
Decreased WBC (white blood cell count) is not a characteristic finding in acute pancreatitis. On the contrary, acute pancreatitis often leads to an elevated WBC count due to the inflammatory response in the body. Leukocytosis (increased WBC) is a common finding in many inflammatory and infectious conditions, including acute pancreatitis. Therefore, a decreased WBC count would not be expected and does not support the diagnosis of acute pancreatitis.
Choice D Reason:
Decreased serum lipase is incorrect. Similar to amylase, lipase is another enzyme produced by the pancreas, which helps in the digestion of fats. In acute pancreatitis, serum lipase levels also increase significantly, often more than three times the upper limit of normal. Lipase levels tend to rise slightly later than amylase but remain elevated for a longer period, making it a useful marker for diagnosing acute pancreatitis. Therefore, decreased serum lipase would not be expected in this condition.
A nurse is teaching self-management to a client who has hepatitis B. Which of the following instructions should the nurse include in the teaching?
Explanation
Choice A reason: Consuming a high-protein diet is not typically recommended for clients with hepatitis B. While protein is essential for overall health, excessive protein intake can put additional strain on the liver. Instead, a balanced diet with adequate carbohydrates, fruits, and vegetables is advised to support liver function.
Choice B reason: Resting frequently throughout the day is crucial for clients with hepatitis B. The liver is responsible for many vital functions, including detoxification, protein synthesis, and the production of biochemicals necessary for digestion. When the liver is inflamed or damaged, as in hepatitis B, it needs ample rest to recover and function properly.
Choice C reason: Clients with hepatitis B should not donate blood. Hepatitis B is a bloodborne virus, and donating blood can transmit the infection to others. Blood donation guidelines strictly prohibit individuals with hepatitis B from donating blood, regardless of the time elapsed since completing medication.
Choice D reason: Taking acetaminophen every 4 hours for discomfort is not advisable for clients with hepatitis B. Acetaminophen is metabolized by the liver, and excessive use can lead to liver damage. Clients with liver conditions should use acetaminophen sparingly and under medical supervision to avoid exacerbating liver damage.
What does the nurse recognize as clinical manifestations consistent with ascites? Select all that apply.
Explanation
Choice A reason: Stretch marks, also known as striae, are not specific to ascites. They can occur due to rapid weight gain or loss, pregnancy, or other conditions that cause the skin to stretch. While they may be present in individuals with ascites due to rapid abdominal expansion, they are not a primary clinical manifestation of ascites.
Choice B reason: Foul-smelling breath, or halitosis, is not a typical symptom of ascites. It can be associated with various conditions, including poor oral hygiene, gastrointestinal disorders, or liver disease, but it is not a direct indicator of ascites.
Choice C reason: Increased abdominal girth is a primary clinical manifestation of ascites. Ascites is characterized by the accumulation of fluid in the peritoneal cavity, leading to noticeable abdominal distension. This symptom is often accompanied by a feeling of fullness or bloating.
Choice D reason: Visible distended veins, particularly around the abdomen, can be a sign of ascites. This occurs due to increased pressure in the abdominal veins as a result of fluid accumulation. The veins become more prominent and visible under the skin.
Choice E reason: Rapid weight gain is another key indicator of ascites. The accumulation of fluid in the abdomen leads to a significant increase in body weight over a short period. This rapid weight gain is often one of the first signs that prompts further investigation for ascites.
The nurse is planning care for a client diagnosed with SIADH. Which of the following would be included in the plan of care? Select all that apply.
Explanation
Choice A Reason:
Administering 0.45% NS (normal saline) at 50 mL/hr is not appropriate for a client with SIADH. This hypotonic solution can exacerbate the condition by increasing the water retention and further diluting the serum sodium levels, worsening hyponatremia. Instead, fluid restriction and hypertonic saline (such as 3% saline) are typically used to manage SIADH.
Choice B Reason:
Obtaining daily weight is crucial in managing SIADH. Daily weights help monitor fluid retention and detect any sudden changes in body weight, which can indicate worsening fluid overload or effective treatment. Accurate weight measurements are essential for assessing the client’s fluid balance and guiding treatment decisions.
Choice C Reason:
Maintaining seizure precautions is necessary for clients with SIADH because severe hyponatremia can lead to neurological symptoms, including seizures. Implementing seizure precautions helps ensure the client’s safety and allows for prompt intervention if a seizure occurs.
Choice D Reason:
Administering 3% saline as ordered is appropriate for treating severe hyponatremia in SIADH. Hypertonic saline helps increase serum sodium levels and reduce the risk of neurological complications. It must be administered carefully and under close monitoring to avoid rapid correction of sodium levels, which can lead to osmotic demyelination syndrome.
Choice E Reason:
Encouraging fluid intake is not appropriate for clients with SIADH. Fluid restriction is a key component of managing SIADH to prevent further dilution of serum sodium levels. Encouraging fluid intake would counteract this goal and worsen the client’s condition.
A nurse is providing pneumonia vaccinations in a community setting. Due to limited finances, the event organizers must limit giving the vaccination to priority groups. What clients would be considered a priority when administering the pneumonia vaccination? (Select all that apply)
Explanation
Choice A reason: A 22-year-old client with asthma is considered a priority for pneumonia vaccination. Asthma is a chronic respiratory condition that can increase the risk of complications from pneumonia. Vaccination helps protect against pneumococcal infections, which can be particularly severe in individuals with underlying respiratory conditions.
Choice B reason: A healthy 72-year-old client is also a priority for pneumonia vaccination. The Centers for Disease Control and Prevention (CDC) recommends pneumococcal vaccination for all adults aged 65 years and older. Older adults are at higher risk for pneumococcal disease due to age-related decline in immune function.
Choice C reason: A client with well-controlled diabetes should be prioritized for pneumonia vaccination. Diabetes can weaken the immune system, making individuals more susceptible to infections, including pneumonia. Vaccination is an important preventive measure for individuals with chronic health conditions.
Choice D reason: A client who is taking medication for hypertension is not necessarily a priority for pneumonia vaccination based solely on their hypertension. While hypertension is a common condition, it does not directly increase the risk of pneumococcal disease. However, if the client has other risk factors or comorbidities, they may still be considered for vaccination.
Choice E reason: A client who had a cholecystectomy last year is not a priority for pneumonia vaccination based on this surgical history alone. A cholecystectomy, which is the removal of the gallbladder, does not increase the risk of pneumococcal disease. Priority for vaccination is typically given to individuals with chronic health conditions, older adults, and those with weakened immune systems.
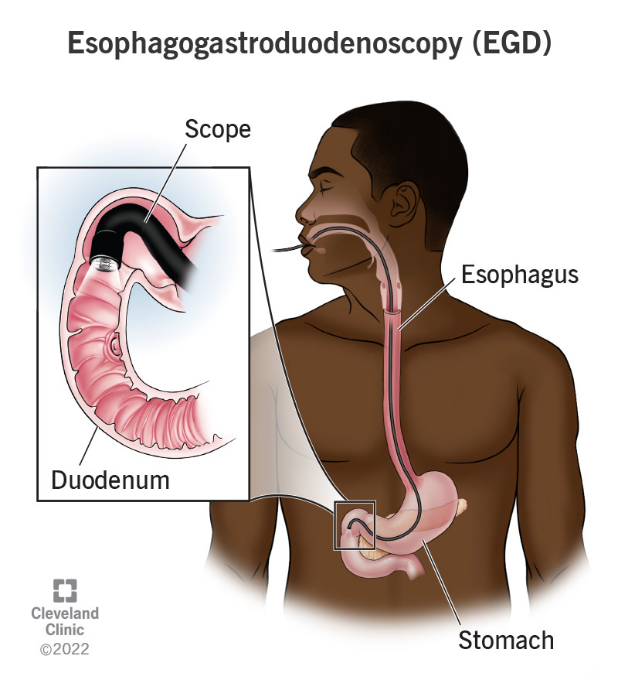
The nurse is caring for a client recovering from an esophagogastroduodenoscopy (EGD). Which of the following client symptoms would require further nursing assessment?
Explanation
Choice A Reason:
Thirst is a common and expected symptom after an EGD, especially if the client has been fasting before the procedure. It does not typically indicate a complication and can be managed by gradually reintroducing fluids as tolerated. Therefore, thirst does not require further nursing assessment beyond routine post-procedure care.
Choice B Reason:
A sore throat is also a common symptom following an EGD. The procedure involves passing an endoscope through the throat, which can cause temporary irritation and discomfort. This symptom usually resolves on its own within a few days and does not indicate a serious complication. Therefore, a sore throat does not require further nursing assessment beyond providing comfort measures such as lozenges or warm saltwater gargles.
Choice C Reason:
Abdominal distention is a concerning symptom that requires further nursing assessment. It can indicate complications such as perforation, bleeding, or infection following the EGD. Perforation of the gastrointestinal tract is a rare but serious complication that can lead to peritonitis and sepsis if not promptly addressed. Therefore, any signs of abdominal distention should be reported to the provider immediately for further evaluation and intervention.
Choice D Reason:
Drowsiness is a common side effect of the sedatives used during the EGD procedure. It is expected that the client may feel drowsy or sleepy for a few hours after the procedure as the sedative wears off. This symptom does not typically require further nursing assessment unless it persists for an unusually long time or is accompanied by other concerning symptoms such as difficulty breathing or altered mental status.
A client is on intravenous heparin to treat DVT in the right leg. The client’s most recent partial thromboplastin time (PTT) was 25 seconds. What order would the nurse anticipate?
Explanation
Choice A reason: No change to the heparin rate is not appropriate in this scenario. The normal range for PTT is generally between 25 to 35 seconds. However, for a client on heparin therapy, the target PTT is typically 1.5 to 2.5 times the normal range, which would be approximately 60 to 80 seconds. Since the client’s PTT is only 25 seconds, it indicates that the blood is clotting too quickly, and the heparin dose is insufficient.
Choice B reason: Decreasing the heparin rate would further reduce the anticoagulant effect, which is not advisable given the current PTT of 25 seconds. Lowering the heparin rate could increase the risk of thrombus formation and worsen the deep vein thrombosis (DVT) condition.
Choice C reason: Stopping heparin and starting warfarin is not an immediate solution. Warfarin takes several days to achieve its full
anticoagulant effect, and during this transition period, the client would be at risk of clot formation. Heparin provides immediate anticoagulation, which is crucial in the acute management of DVT.
Choice D reason: Increasing the heparin rate is the correct action. The current PTT of 25 seconds is below the therapeutic range for a client on heparin therapy. Increasing the heparin rate will help achieve the desired anticoagulant effect, prolonging the PTT to the target range of 60 to 80 seconds.
A nurse is caring for a client who returns to the nursing unit from the recovery room after a sigmoid colon resection for adenocarcinoma. The client had an episode of intraoperative bleeding. Which finding indicates to the nurse that the client may be developing hypovolemic shock?
Explanation
Choice A reason: An increase in temperature is not a primary indicator of hypovolemic shock. While fever can occur due to infection or inflammation, it is not directly related to hypovolemic shock, which is primarily characterized by a significant loss of blood or fluids leading to decreased perfusion and oxygenation of tissues.
Choice B reason: A decrease in urinary output is a critical sign of hypovolemic shock. When the body loses a significant amount of blood or fluids, the kidneys receive less blood flow, leading to reduced urine production. This is a compensatory mechanism to conserve fluids and maintain blood pressure. Normal urine output is typically around 30 to 50 mL per hour, so a drop below this range is concerning.
Choice C reason: An increase in heart rate is a common response to hypovolemic shock as the body attempts to maintain cardiac output and blood pressure despite the loss of blood volume. Tachycardia (increased heart rate) is one of the early signs of shock, indicating that the heart is working harder to pump blood to vital organs.
Choice D reason: A decrease in respiratory rate is not typical of hypovolemic shock. In fact, hypovolemic shock often leads to an increased respiratory rate (tachypnea) as the body tries to compensate for decreased oxygen delivery to tissues. A decrease in respiratory rate could indicate other issues but is not a hallmark of hypovolemic shock.
A nurse is caring for a client who has Cushing’s syndrome. The nurse should recognize that which of the following are manifestations of Cushing’s syndrome? (Select all that apply)
Explanation
Choice A reason: A buffalo hump is a characteristic sign of Cushing’s syndrome. It refers to the accumulation of fat on the back of the neck and shoulders. This symptom occurs due to the excessive production of cortisol, which leads to abnormal fat distribution in the body.
Choice B reason: Moon face is another hallmark of Cushing’s syndrome. It describes the rounding and fullness of the face, which results from fat deposits. This symptom is also caused by prolonged exposure to high levels of cortisol.
Choice C reason: Hypertension, or high blood pressure, is commonly associated with Cushing’s syndrome. Cortisol increases blood pressure by enhancing the sensitivity of blood vessels to catecholamines and by promoting sodium and water retention.
Choice D reason: Purple striations, or stretch marks, are often seen in individuals with Cushing’s syndrome. These marks typically appear on the abdomen, thighs, breasts, and arms. They result from the thinning of the skin and the breakdown of collagen due to elevated cortisol levels.
Choice E reason: Tremors are not typically associated with Cushing’s syndrome. While Cushing’s syndrome can cause a variety of symptoms, tremors are more commonly linked to other conditions such as hyperthyroidism or neurological disorders.
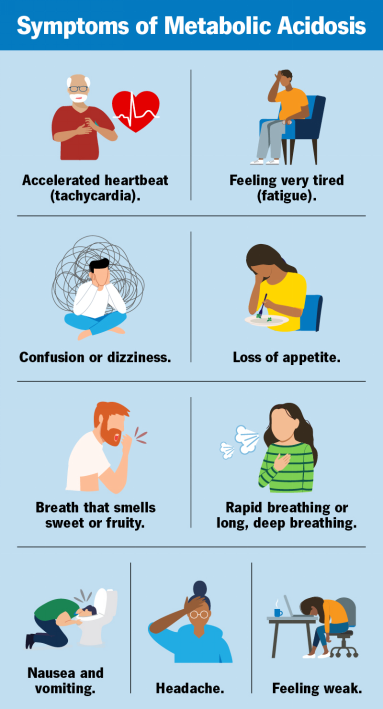
A nurse is caring for a client who has the following arterial blood gas results: HCO3 18 mEq/L, PaCO2 28 mm Hg, and pH 7.30. The nurse recognizes the client is experiencing which of the following acid-base imbalances?
Explanation
Choice A Reason:
Metabolic alkalosis is characterized by an elevated pH (greater than 7.45) and an increased bicarbonate (HCO3) level. In this case, the pH is 7.30, indicating acidosis, and the HCO3 level is 18 mEq/L, which is below the normal range (22-26 mEq/L). Therefore, metabolic alkalosis is not the correct diagnosis.
Choice B Reason:
Respiratory alkalosis is indicated by a high pH (greater than 7.45) and a low PaCO2 (less than 35 mm Hg). Although the PaCO2 is low at 28 mm Hg, the pH is 7.30, indicating acidosis rather than alkalosis. Therefore, respiratory alkalosis is not the correct diagnosis.
Choice C Reason:
Respiratory acidosis is characterized by a low pH (less than 7.35) and an elevated PaCO2 (greater than 45 mm Hg). In this case, the pH is low, indicating acidosis, but the PaCO2 is also low at 28 mm Hg, which does not fit the criteria for respiratory acidosis. Therefore, respiratory acidosis is not the correct diagnosis.
Choice D Reason:
Metabolic acidosis is indicated by a low pH (less than 7.35) and a low bicarbonate (HCO3) level (less than 22 mEq/L). In this case, the pH is 7.30, indicating acidosis, and the HCO3 level is 18 mEq/L, which is below the normal range. The low PaCO2 of 28 mm Hg suggests a compensatory respiratory response to the metabolic acidosis. Therefore, metabolic acidosis is the correct diagnosis.
A nurse is caring for a client who has hypernatremia and requires IV fluid therapy due to his NPO status. Which of the following solutions should the nurse prepare to infuse for this client?
Explanation
Choice A Reason:
0.45% sodium chloride (half-normal saline) is an appropriate solution for treating hypernatremia, especially in a client who is NPO (nothing by mouth). This hypotonic solution helps to gradually reduce the serum sodium levels by providing free water to the extracellular space, which dilutes the high sodium concentration. It is essential to administer this solution slowly to avoid rapid shifts in fluid balance, which can lead to cerebral edema.
Choice B Reason:
Dextrose 5% in 0.9% sodium chloride (D5NS) is not the best choice for treating hypernatremia. While it provides some free water, the presence of 0.9% sodium chloride makes it an isotonic solution, which does not effectively lower serum sodium levels. This solution is more suitable for maintaining fluid balance rather than correcting hypernatremia.
Choice C Reason:
Lactated Ringer’s is also not appropriate for treating hypernatremia. This isotonic solution contains electrolytes, including sodium, which can exacerbate hypernatremia rather than correct it. Lactated Ringer’s is typically used for fluid resuscitation and electrolyte replacement in other clinical scenarios.
Choice D Reason:
Dextrose 10% in water (D10W) is a hypertonic solution and is not suitable for treating hypernatremia. While it provides free water, the high concentration of dextrose can lead to rapid shifts in fluid balance and potential complications such as hyperglycemia. This solution is generally used for providing calories and preventing hypoglycemia in specific clinical situations.
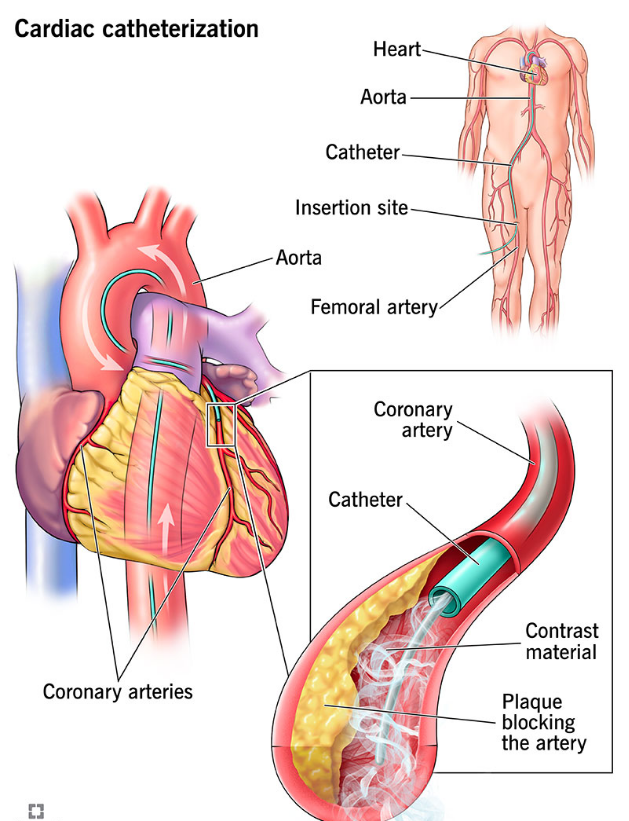
A nurse is collecting a medication history from a client who is scheduled to have a cardiac catheterization. Which of the following medications taken by the client interacts with contrast material and places the client at risk for acute kidney injury?
Explanation
Choice A: Metformin
Metformin is known to interact with contrast material, particularly iodinated contrast media, and can increase the risk of acute kidney injury (AKI). This interaction can lead to a condition known as contrast-induced nephropathy (CIN) or contrast-induced acute kidney injury (CI-AKI). Metformin is primarily excreted by the kidneys, and impaired renal function can lead to its accumulation, increasing the risk of lactic acidosis, a rare but serious complication. Therefore, it is generally recommended to withhold metformin before and after the administration of contrast media until renal function is confirmed to be normal.
Choice B: Carvedilol
Carvedilol is a beta-blocker used to treat high blood pressure and heart failure. It does not have a known interaction with contrast media that would increase the risk of acute kidney injury. Carvedilol primarily affects the cardiovascular system and does not significantly impact renal function or interact with contrast agents.
Choice C: Nitroglycerin
Nitroglycerin is used to treat angina and other heart conditions by dilating blood vessels. It does not interact with contrast media in a way that would increase the risk of acute kidney injury. Nitroglycerin’s primary effects are on the cardiovascular system, and it does not have nephrotoxic properties.
Choice D: Atorvastatin
Atorvastatin is a statin used to lower cholesterol levels. While it can have effects on liver enzymes and muscle tissue, it does not interact with contrast media to increase the risk of acute kidney injury. Atorvastatin is metabolized by the liver and does not significantly impact renal function.
After teaching a nursing student about mitral valve stenosis and mitral valve regurgitation, the nurse identifies effective learning when the student identifies which common feature of both disorders?
Explanation
Choice A Reason:
Hemoptysis, or coughing up blood, is a common feature of both mitral valve stenosis and mitral valve regurgitation. In mitral valve stenosis, the narrowing of the valve leads to increased pressure in the pulmonary veins, which can cause pulmonary congestion and hemoptysis. Similarly, in mitral valve regurgitation, the backflow of blood into the left atrium increases pulmonary pressure, potentially leading to pulmonary edema and hemoptysis. Therefore, hemoptysis is a shared symptom of both conditions.
Choice B Reason:
A high-pitched holosystolic murmur is more commonly associated with mitral valve regurgitation rather than mitral valve stenosis. In mitral valve regurgitation, the murmur is caused by the backflow of blood from the left ventricle into the left atrium during systole3. Mitral valve stenosis, on the other hand, typically presents with a diastolic murmur due to the turbulent flow of blood through the narrowed valve during diastole. Therefore, a high-pitched holosystolic murmur is not a common feature of both disorders.
Choice C Reason:
Hepatomegaly, or an enlarged liver, can occur in advanced cases of both mitral valve stenosis and mitral valve regurgitation due to right-sided heart failure. However, it is not a primary or common feature of these conditions. Hepatomegaly is more often associated with conditions that directly affect the right side of the heart or cause systemic congestion. Therefore, hepatomegaly is not a common feature of both mitral valve stenosis and mitral valve regurgitation.
Which sign or symptom would the nurse anticipate in a patient diagnosed with tuberculosis? Select all that apply. One, some, or all responses may be correct.
Explanation
Choice A Reason:
Weight gain is not typically associated with tuberculosis (TB). In fact, weight loss is a common symptom of TB due to the chronic nature of the infection and the body’s increased metabolic demands to fight the disease. Patients with TB often experience a loss of appetite and significant weight loss as the disease progresses.
Choice B Reason:
Low-grade fever is a common symptom of TB. The body’s immune response to the infection often results in a persistent low-grade fever, which can be one of the early signs of the disease. This fever is usually accompanied by other systemic symptoms such as night sweats and fatigue.
Choice C Reason:
Dyspnea, or difficulty breathing, can occur in patients with TB, especially if the infection has caused significant lung damage or if there is a large amount of fluid in the pleural space (pleural effusion). Dyspnea is a concerning symptom that indicates the need for further evaluation and treatment.
Choice D Reason:
Contusion, or bruising, is not a symptom associated with TB. TB primarily affects the lungs and can cause systemic symptoms, but it does not typically cause bruising. Contusions are more commonly associated with trauma or conditions that affect blood clotting.
Choice E Reason:
Lethargy, or a general sense of fatigue and weakness, is a common symptom of TB. The chronic nature of the infection and the body’s ongoing immune response can lead to significant fatigue. Patients with TB often feel tired and may have difficulty performing daily activities.
Choice F Reason:
Night sweats are a hallmark symptom of TB. Patients often experience drenching night sweats that can be quite severe. This symptom, along with fever and weight loss, is part of the classic triad of TB symptoms and is an important indicator for healthcare providers to consider TB in the differential diagnosis.
Sign Up or Login to view all the 75 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
