HESI RN Med Surg
Total Questions : 40
Showing 25 questions, Sign in for moreThe nurse is assessing the lung sounds of a preschooler. Which action should the nurse implement to ensure the child's cooperation?
Explanation
Choice A reason: Having the child blow a cotton ball and have the parent catch it is not a good strategy to ensure the child's cooperation. This activity might distract the child from the assessment and make it difficult for the nurse to listen to the lung sounds.
Choice B reason: Allowing the child to use a stethoscope on a stuffed animal is a good strategy to ensure the child's cooperation. This activity helps the child to understand the purpose of the stethoscope and reduces the fear of the unfamiliar device. It also allows the nurse to observe the child's breathing pattern and chest movement.
Choice C reason: Offering the child bubbles before the stethoscope is placed is not a good strategy to ensure the child's cooperation. This activity might alter the child's breathing pattern and interfere with the accuracy of the assessment.
Choice D reason: Placing a toy in the child's hands while listening to the breath sounds is not a good strategy to ensure the child's cooperation. This activity might distract the child from the assessment and make it difficult for the nurse to listen to the lung sounds.

A child diagnosed with Kawasaki disease is brought to the clinic. The mother reports that her child is irritable, refuses to eat, and has skin peeling on both hands and feet. Which intervention should the nurse instruct the mother to implement first?
Explanation
Choice A reason: Encouraging the parents to rest when possible is not the first intervention that the nurse should instruct the mother to implement. While it is important for the parents to take care of themselves, the priority is to address the child's needs and comfort.
Choice B reason: Making a list of foods that the child likes is not the first intervention that the nurse should instruct the mother to implement. While it is important to maintain the child's nutrition and hydration, the child may not have an appetite due to the fever and inflammation caused by Kawasaki disease.
Choice C reason: Placing the child in a quiet environment is the first intervention that the nurse should instruct the mother to implement. This is because Kawasaki disease causes irritability and sensitivity to light and sound in the child. A quiet environment can help reduce the child's stress and discomfort.
Choice D reason: Applying lotion to hands and feet is not the first intervention that the nurse should instruct the mother to implement. While it is important to moisturize the skin and prevent cracking and infection, the lotion may not relieve the child's pain and inflammation.
During a follow-up clinic visit, a mother tells the nurse that her 5-month-old son who had surgical correction for tetralogy of Fallot (TOF) has rapid breathing, often takes a long time to eat, and requires frequent rest periods. The infant is not crying while being held and his growth is in the expected range. Which intervention should the nurse implement?
Explanation
Choice A reason: Obtaining a 12-lead electrocardiogram is not the first intervention that the nurse should implement. An electrocardiogram is a test that measures the electrical activity of the heart and can detect abnormalities in the heart rhythm or structure. However, it is not a priority for an infant who has already had surgical correction for TOF and is not showing signs of distress.
Choice B reason: Stimulating the infant to cry to produce cyanosis is not an intervention that the nurse should implement at all. Cyanosis is a bluish discoloration of the skin due to low oxygen levels in the blood. It is a common symptom of TOF and can be triggered by crying or other stressors. However, it is not a desirable outcome and can cause harm to the infant. The nurse should avoid provoking cyanosis and instead provide comfort and oxygen to the infant.
Choice C reason: Auscultating heart and lungs while the infant is held is the first intervention that the nurse should implement. This is a simple and noninvasive way to assess the infant's respiratory and cardiac status. The nurse can listen for any abnormal sounds, such as crackles, wheezes, or murmurs, that may indicate a problem. The nurse can also monitor the infant's heart rate and oxygen saturation. Holding the infant can provide comfort and security to the infant and the mother.
Choice D reason: Evaluating the infant for failure to thrive (FTT) is not the first intervention that the nurse should implement. FTT is a condition where an infant does not grow or gain weight as expected. It can be caused by various factors, such as inadequate nutrition, chronic illness, or psychosocial issues. However, the infant in this scenario is not showing signs of FTT, as his growth is in the expected range. The nurse should focus on the infant's current symptoms and needs.
The mother of a one-month-old infant calls the clinic to report that the back of her infant's head is flat. How should the nurse respond?
Explanation
Choice A reason: Positioning the infant on the stomach occasionally when awake and active is the best response that the nurse can give to the mother. This is because it can help prevent and correct the flat head syndrome, also known as plagiocephaly, by taking pressure off the back of the head and allowing the skull to reshape naturally. It can also promote the infant's motor development and strengthen the neck and shoulder muscles. However, the nurse should also remind the mother to always place the infant on the back when sleeping, as this is the safest position to reduce the risk of sudden infant death syndrome (SIDS) .
Choice B reason: Turning the infant on the left side braced against the crib when sleeping is not a good response that the nurse can give to the mother. This is because it can increase the risk of SIDS, as the infant may roll over to the stomach or suffocate from the bedding or the crib. It can also worsen the flat head syndrome by creating another flat spot on the left side of the head.
Choice C reason: Placing a small pillow under the infant's head while lying on the back is not a good response that the nurse can give to the mother. This is because it can increase the risk of SIDS, as the pillow may cover the infant's face or cause the infant to overheat. It can also interfere with the natural reshaping of the skull and cause neck strain.
Choice D reason: Propping the infant in a sitting position with a cushion when not sleeping is not a good response that the nurse can give to the mother. This is because it can put too much pressure on the spine and the pelvis, which are still developing in the infant. It can also limit the infant's movement and exploration, which are important for learning and development.
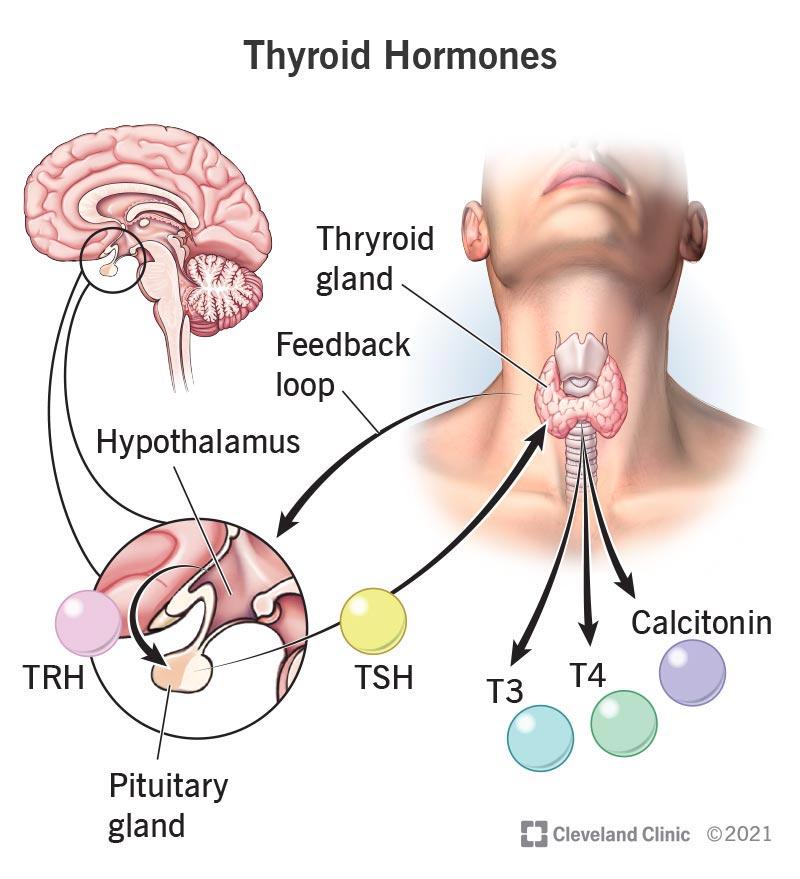
The nurse is caring for a one-month-old infant admitted for suspected congenital hypothyroidism. Which diagnostic test results should the nurse report to the healthcare provider?
Explanation
Choice A reason: Luteinizing hormone (LH) levels are not relevant for the diagnosis of congenital hypothyroidism. LH is a hormone that regulates the reproductive system and is not affected by thyroid function.
Choice B reason: Thyroxine (T4) is the main hormone produced by the thyroid gland and is essential for growth and development. Low levels of T4 indicate hypothyroidism and require treatment with thyroid hormone replacement. High levels of T4 indicate hyperthyroidism and require treatment with anti-thyroid drugs.
Choice C reason: Growth hormone (GH) levels are not relevant for the diagnosis of congenital hypothyroidism. GH is a hormone that stimulates growth and metabolism and is not affected by thyroid function.
Choice D reason: Follicle stimulating hormone (FSH) levels are not relevant for the diagnosis of congenital hypothyroidism. FSH is a hormone that regulates the reproductive system and is not affected by thyroid function.
An adolescent with a congenital heart defect is admitted for diagnostic testing with surgery scheduled in 3 days. Which intervention should the nurse implement to best support the client's psychosocial needs?
Explanation
Choice A reason: Enabling limited time for cell phone use is not the best intervention that the nurse can implement to support the client's psychosocial needs. While cell phone use can help the client stay connected with their peers and social media, it can also be a source of distraction and stress. The nurse should encourage the client to balance their cell phone use with other activities that promote their well-being.
Choice B reason: Providing an activity room to spend time with other adolescents is the best intervention that the nurse can implement to support the client's psychosocial needs. This intervention can help the client cope with the anxiety and isolation that may result from their condition and hospitalization. It can also provide an opportunity for the client to interact with other adolescents who have similar experiences and challenges, and to engage in fun and meaningful activities that enhance their self-esteem and mood.
Choice C reason: Delivering 3 meals and snacks each day upon request is not the best intervention that the nurse can implement to support the client's psychosocial needs. While it is important to maintain the client's nutrition and hydration, it is not enough to address their emotional and social needs. The nurse should also encourage the client to eat with other adolescents or family members when possible, and to express their preferences and concerns about their food.
Choice D reason: Allowing family and friends to be present during assessments is not the best intervention that the nurse can implement to support the client's psychosocial needs. While it is important to involve the client's family and friends in their care, it is not necessary to have them present during every assessment. The nurse should respect the client's privacy and autonomy, and ask for their consent before allowing others to observe or participate in their assessments. The nurse should also provide the client with opportunities to talk to their family and friends in a comfortable and confidential setting.
An infant who is developmentally delayed has a ventricular peritoneal (VP) shunt for hydrocephalus. The nurse makes a postoperative home visit to assess the child's progress. During the visit, the mother tells the nurse, "When the shunt is removed, the pressure in my baby's head will be gone." Which response should the nurse provide?
Explanation
Choice A reason: "Many infants outgrow the need for a shunt after the neonatal period." is not a correct response that the nurse should provide. This statement is false, as most infants with hydrocephalus will need a shunt for life. Only a small percentage of infants with post-hemorrhagic hydrocephalus may outgrow the need for a shunt .
Choice B reason: "The shunt will be replaced as your child grows to reduce pressure in the brain." is the correct response that the nurse should provide. This statement is true, as the shunt will need to be adjusted or replaced as the child grows to accommodate the changes in the size and shape of the head and the amount of fluid drainage. The nurse should educate the mother about the signs and symptoms of shunt malfunction and the need for regular follow-up visits.
Choice C reason: "Other pathways in the brain will drain fluid after the shunt is removed." is not a correct response that the nurse should provide. This statement is false, as the shunt is not removed unless there is a serious complication or the child no longer needs it. The shunt is a permanent device that bypasses the blocked or impaired pathways in the brain and allows the fluid to drain into the abdomen. Without the shunt, the fluid will accumulate in the brain and cause increased pressure and damage.
Choice D reason: "The shunt will have to be reinserted only if an infection or blockage develops." is not a correct response that the nurse should provide. This statement is false, as the shunt is not removed and reinserted unless there is a serious complication or the child no longer needs it. The shunt is a permanent device that stays in place unless it malfunctions or becomes infected. The nurse should educate the mother about the signs and symptoms of shunt infection and the need for prompt treatment.
An infant who has a Wilms' tumor is admitted for surgery. Which intervention should the nurse implement during the preoperative period?
Explanation
Choice A reason: Careful bathing and handling that avoids abdominal manipulation is the best intervention that the nurse can implement during the preoperative period. This is because Wilms' tumor is a rare kidney cancer that mainly affects children and can rupture or spread if touched or pressed. The nurse should avoid any unnecessary pressure on the abdomen and use gentle movements when bathing and handling the infant.
Choice B reason: Administering pain medication based on the FACES pain scale is not the best intervention that the nurse can implement during the preoperative period. This is because the FACES pain scale is a tool that helps children aged 3 and older to communicate their pain level by pointing to a face that matches their pain. However, the infant in this scenario is too young to use this scale and may not be able to express their pain verbally. The nurse should use other methods to assess the infant's pain, such as observing their behavior, vital signs and facial expressions.
Choice C reason: Including the prone position in the every 2 hour turning schedule is not the best intervention that the nurse can implement during the preoperative period. This is because the prone position, which is lying on the stomach, can increase the risk of rupture or spread of the tumor. The nurse should avoid placing the infant in this position and instead use other positions that are comfortable and safe for the infant.
Choice D reason: Giving antiemetic medications to prevent nausea and vomiting is not the best intervention that the nurse can implement during the preoperative period. This is because antiemetic medications are drugs that prevent or treat nausea and vomiting caused by chemotherapy, radiation therapy or surgery. However, the infant in this scenario has not yet undergone any of these treatments and may not have any symptoms of nausea and vomiting. The nurse should only give antiemetic medications if the infant shows signs of nausea and vomiting or if prescribed by the doctor.
An infant born 2 days ago has not passed a meconium stool and begins to vomit bilious secretions. Which action should the nurse take first?
Explanation
Choice A reason: Measuring abdominal circumference is not the first action that the nurse should take. This is because abdominal circumference is not a reliable indicator of bowel obstruction or perforation, which are possible complications of meconium ileus. Measuring abdominal circumference may also delay more urgent interventions, such as fluid resuscitation and decompression.
Choice B reason: Gathering supplies for an intravenous (IV) infusion is the first action that the nurse should take. This is because the infant is at risk of dehydration, electrolyte imbalance, and shock due to vomiting and bowel obstruction. The nurse should prepare to administer IV fluids, antibiotics, and blood products as ordered by the healthcare provider.
Choice C reason: Monitoring strict urinary output is not the first action that the nurse should take. This is because urinary output is not the most sensitive indicator of fluid status in infants, especially those with renal insufficiency or oliguria. Monitoring urinary output may also delay more urgent interventions, such as fluid resuscitation and decompression.
Choice D reason: Preparing for anorectal manometry is not the first action that the nurse should take. This is because anorectal manometry is a diagnostic test that measures the pressure and function of the anal and rectal muscles. It is not indicated for infants with suspected meconium ileus, which is a mechanical obstruction of the bowel by thick and sticky meconium. Preparing for anorectal manometry may also delay more urgent interventions, such as fluid resuscitation and decompression.
The nurse is conducting an admission assessment of an infant with heart failure who is scheduled for repair of restenosis of coarctation of the aorta that was repaired 4 days after birth. Findings include blood pressure higher in the arms than the lower extremities, pounding brachial pulses, and slightly palpable femoral pulses. Which pathophysiologic mechanism supports these findings?
Explanation
Choice A reason: The lumen of the aorta reduces the volume of blood flow to the lower extremities is the correct pathophysiologic mechanism that supports the findings. This is because coarctation of the aorta is a congenital condition that causes a narrowing of the aorta, usually near the ductus arteriosus. This results in increased resistance to blood flow from the heart to the lower body, leading to higher blood pressure and stronger pulses in the upper extremities and lower blood pressure and weaker pulses in the lower extremities.
Choice B reason: The aortic semilunar valve obstructs blood flow into the systemic circulation is not the correct pathophysiologic mechanism that supports the findings. This is because the aortic semilunar valve is located at the base of the aorta and prevents blood from flowing back into the left ventricle. If the valve is obstructed, it would cause aortic stenosis, which is a different condition from coarctation of the aorta. Aortic stenosis would cause symptoms such as chest pain, shortness of breath, and fainting.
Choice C reason: The pulmonic valve prevents adequate blood volume into the pulmonary circulation is not the correct pathophysiologic mechanism that supports the findings. This is because the pulmonic valve is located at the base of the pulmonary artery and prevents blood from flowing back into the right ventricle. If the valve is obstructed, it would cause pulmonic stenosis, which is a different condition from coarctation of the aorta. Pulmonic stenosis would cause symptoms such as cyanosis, fatigue, and heart murmur.
Choice D reason: An opening in the atrial septum causes a murmur due to a turbulent left to right shunt is not the correct pathophysiologic mechanism that supports the findings. This is because an opening in the atrial septum is a defect in the wall that separates the two upper chambers of the heart. It would cause a condition called atrial septal defect, which is different from coarctation of the aorta. Atrial septal defect would cause symptoms such as difficulty breathing, frequent respiratory infections, and heart palpitations.
A 10-year-old boy has been seen frequently by the school nurse over the past three weeks after school begins in the fall. He reports headaches, stomach aches, and difficulty sleeping. Which intervention should the nurse implement?
Explanation
Choice A reason: Asking the boy to describe a typical day at school is the best intervention that the nurse can implement. This can help the nurse identify any possible sources of stress or anxiety that may be causing the boy's physical symptoms. The nurse can also provide emotional support and guidance to the boy and his parents on how to cope with the school-related challenges.
Choice B reason: Conducting a complete neurological assessment is not the best intervention that the nurse can implement. This is not necessary unless the boy has other signs of neurological problems, such as seizures, vision changes, or altered mental status. A neurological assessment may also be invasive and uncomfortable for the boy and may increase his anxiety.
Choice C reason: Counseling the parents to pay more attention to the child is not the best intervention that the nurse can implement. This may imply that the parents are neglectful or irresponsible, which may not be true. The nurse should avoid making assumptions or judgments about the parents' behavior and instead collaborate with them to find the best solutions for the child's well-being.
Choice D reason: Comparing the child's vital signs over the past three weeks is not the best intervention that the nurse can implement. This may not provide much useful information, as the child's vital signs may vary depending on the time of day, activity level, and emotional state. The nurse should focus more on the child's subjective complaints and psychosocial factors.
The clinic nurse receives a call from a parent of a 10-year-old who reports that their child just returned from summer camp and has developed an expanding circular red rash on the arm. The parent asks the nurse which over-the-counter (OTC) product is safe to use. How should the nurse respond?
Explanation
Choice A reason: Encouraging the parent to come to the clinic if the child develops a fever is not the best response that the nurse can give. This is because a fever may indicate a serious infection, such as Lyme disease, that requires prompt treatment. The nurse should not wait for the child to develop a fever before advising the parent to seek medical attention.
Choice B reason: Instructing the parent to apply an antihistamine ointment for one week is not the best response that the nurse can give. This is because an antihistamine ointment may not be effective for a fungal infection, such as ringworm, or a bacterial infection, such as Lyme disease, that may cause a circular rash. The nurse should not recommend any OTC product without knowing the exact cause of the rash.
Choice C reason: Offering reassurance that OTC corticosteroid creams are safe and effective is not the best response that the nurse can give. This is because corticosteroid creams may worsen a fungal infection, such as ringworm, or mask the symptoms of a bacterial infection, such as Lyme disease, that may cause a circular rash. The nurse should not recommend any OTC product without knowing the exact cause of the rash.
Choice D reason: Explaining the need for the child to have an immediate medical evaluation is the best response that the nurse can give. This is because a circular rash can be a sign of a serious condition, such as Lyme disease, that requires urgent diagnosis and treatment. The nurse should inform the parent that the rash may not be ringworm, as many people assume, and that it may be caused by a tick bite or another factor. The nurse should also advise the parent to avoid touching or scratching the rash and to keep it clean and dry until the child sees a doctor.
An adolescent client reports to the nurse of walking with a limp due to pain localized in the right knee which worsens at night but denies any recent injury or trauma. The nurse observes swelling and tenderness in the right lower thigh and imaging results reveal radial ossification in the soft tissues. Which condition should the nurse consider as the probable cause of the findings?
Explanation
Choice A reason: Rhabdomyolysis is not the probable cause of the findings. Rhabdomyolysis is a condition that occurs when damaged muscle tissue breaks down and releases substances into the bloodstream that can harm the kidneys. It is usually caused by trauma, infection, drugs, or extreme exercise. It does not cause radial ossification in the soft tissues, but rather dark urine, muscle weakness, and kidney failure.
Choice B reason: Osteosarcoma is the probable cause of the findings. Osteosarcoma is a type of bone cancer that usually affects the long bones of the arms and legs. It is more common in adolescents and young adults. It can cause pain, swelling, and limping in the affected area, as well as radial ossification in the soft tissues, which is a sign of tumor invasion.
Choice C reason: Growing pains are not the probable cause of the findings. Growing pains are a common cause of leg pain in children and adolescents, but they are not associated with any physical abnormality or disease. They usually occur in both legs, not just one, and they are more likely to affect the calves, shins, or thighs, not the knees. They do not cause swelling, tenderness, or radial ossification in the soft tissues.
Choice D reason: Hemosiderosis is not the probable cause of the findings. Hemosiderosis is a condition that occurs when excess iron deposits in the tissues, usually as a result of repeated blood transfusions or hemolytic anemia. It can affect various organs, such as the liver, lungs, heart, and skin, but not the bones. It does not cause pain, swelling, or radial ossification in the soft tissues, but rather fatigue, shortness of breath, chest pain, and skin discoloration.

When providing care for a child who is in balanced suspension skeletal traction using a Thomas splint and Pearson attachment to the right femur, which intervention is most important for the nurse to implement?
Explanation
Choice A reason: Changing position every 2 hours is not the most important intervention that the nurse should implement. This is because the child's position is limited by the traction and the splint, and frequent repositioning may interfere with the alignment and stability of the fracture. The nurse should only change the position of the child as ordered by the physician and with the assistance of another nurse.
Choice B reason: Assessing skin for redness and signs of tissue breakdown is not the most important intervention that the nurse should implement. This is because the skin is not directly in contact with the traction or the splint, and the risk of pressure ulcers is low. The nurse should still inspect the skin regularly and provide skin care as needed, but this is not the priority.
Choice C reason: Cleansing pin sites as prescribed is not the most important intervention that the nurse should implement. This is because the pin sites are not the main source of infection or complication in this type of traction. The nurse should still follow the protocol for pin site care and monitor for signs of infection, such as redness, swelling, drainage, or odor, but this is not the priority.
Choice D reason: Monitoring peripheral pulses and sensation in the right leg is the most important intervention that the nurse should implement. This is because the traction and the splint can impair the circulation and nerve function of the affected extremity, leading to complications such as compartment syndrome, ischemia, or nerve damage. The nurse should check the pulses, temperature, color, capillary refill, and sensation of the right leg at least every hour and report any changes or abnormalities to the physician.
A school-aged child is admitted to the hospital with a diagnosis of acute rheumatic fever. In obtaining a health history from the child's parent, the recent occurrence of which illness is most significant?
Explanation
Choice A reason: Chickenpox is not the most significant illness that may be associated with acute rheumatic fever. Chickenpox is a viral infection that causes an itchy rash and blisters. It is not caused by group A streptococcus (GAS) bacteria, which are the main trigger of acute rheumatic fever.
Choice B reason: Sore throat is the most significant illness that may be associated with acute rheumatic fever. Sore throat can be caused by GAS bacteria, which can also cause strep throat or scarlet fever. If these infections are not properly treated with antibiotics, they can lead to acute rheumatic fever, which is an inflammatory disease that can affect the heart, joints, skin, and brain.
Choice C reason: Mumps is not the most significant illness that may be associated with acute rheumatic fever. Mumps is a viral infection that causes swelling of the salivary glands. It is not caused by GAS bacteria, which are the main trigger of acute rheumatic fever.
Choice D reason: Influenza is not the most significant illness that may be associated with acute rheumatic fever. Influenza is a viral infection that causes fever, cough, sore throat, and muscle aches. It is not caused by GAS bacteria, which are the main trigger of acute rheumatic fever.
The nurse is caring for an infant admitted with dehydration, irritability, signs of extreme hunger, and a palpable olive-like mass in the upper right abdominal quadrant. When feeding the infant, the nurse should monitor for which development?
Explanation
Choice A reason: Coffee-ground emesis is not the development that the nurse should monitor for. This is a sign of bleeding in the upper gastrointestinal tract, which can be caused by ulcers, gastritis, or esophageal varices. It is not related to the infant's condition, which is likely pyloric stenosis, a narrowing of the opening between the stomach and the small intestine.
Choice B reason: Frequent pauses are not the development that the nurse should monitor for. This is a normal behavior for infants during feeding, as they need to take breaks to breathe and swallow. It is not indicative of any problem or complication.
Choice C reason: Projectile vomiting is the development that the nurse should monitor for. This is a common symptom of pyloric stenosis, a condition that affects about 3 out of 1,000 infants. It occurs when the muscle at the end of the stomach becomes thickened and blocks the passage of food into the small intestine. This causes the infant to vomit forcefully after feeding, leading to dehydration, hunger, and weight loss. The olive-like mass in the upper right abdomen is the enlarged pylorus muscle that can be felt through the skin.
Choice D reason: Arched back is not the development that the nurse should monitor for. This is a sign of pain or discomfort in infants, which can have various causes, such as colic, reflux, or ear infection. It is not specific to pyloric stenosis, although the infant may arch their back due to the abdominal pain caused by the condition. .
An 8-year-old girl with precocious sexual development is being treated medically with injections of luteinizing hormone-releasing hormone (LHRH) to regulate the pituitary gland. Which statement by the parents indicates that they understand the treatment?
Explanation
Choice A reason: Starting the daughter on birth control pills is not necessary and may interfere with the LHRH treatment. LHRH injections suppress the production of sex hormones and prevent ovulation and menstruation. Birth control pills contain synthetic hormones that may have unwanted side effects and may not be effective in preventing pregnancy in girls with precocious puberty.
Choice B reason: Encouraging the daughter to dress in clothing that suits her sexual maturity level is not advisable and may cause psychological distress. Girls with precocious puberty may feel self-conscious and embarrassed about their early physical development and may face teasing or bullying from their peers. Dressing in clothing that accentuates their sexual maturity may make them feel more uncomfortable and isolated. They should be allowed to dress in clothing that matches their age and emotional development.
Choice C reason: The daughter will not be on this hormone treatment the rest of her life. LHRH injections are usually given until the age of normal puberty, around 11 or 12 years old. Then, the treatment is stopped and the natural puberty process resumes. The injections are meant to delay puberty, not stop it permanently.
Choice D reason: Sexual maturity differences between the daughter and her peers will disappear within a few years is the correct statement that shows understanding of the treatment. LHRH injections slow down the growth and development of the sex organs and secondary sexual characteristics, such as breasts and pubic hair. This allows the girl to grow at a normal rate and reach her full adult height potential. It also reduces the social and emotional problems that may arise from being sexually mature too early. Once the treatment is stopped, the girl will go through puberty at the same time as her peers and the differences will no longer be noticeable.
A 9-year-old admitted to the unit with severe abdominal pain and fever is diagnosed with appendicitis and is placed on the surgery schedule for an appendectomy. The child reports to the nurse of experiencing sudden relief in abdominal pain. Which action should the nurse take first?
Explanation
Choice A reason: Giving prescribed intravenous antibiotics is not the first action that the nurse should take. Antibiotics are used to treat the infection and inflammation caused by appendicitis, but they are not enough to prevent the complications of a ruptured appendix. The nurse should administer the antibiotics as ordered, but only after notifying the healthcare provider of the change in the child's condition.
Choice B reason: Inquiring about the client's last meal is not the first action that the nurse should take. The last meal may be relevant for the preparation of the surgery, but it is not urgent or related to the sudden relief of pain. The nurse should ask about the last meal as part of the preoperative assessment, but only after contacting the healthcare provider.
Choice C reason: Contacting the healthcare provider is the first action that the nurse should take. Sudden relief of pain in a child with appendicitis may indicate a perforation or rupture of the appendix, which is a life-threatening emergency. The nurse should immediately report this finding to the healthcare provider, who may order additional tests or expedite the surgery.
Choice D reason: Documenting the client's relief of pain is not the first action that the nurse should take. Documentation is an important part of nursing care, but it is not a priority in this situation. The nurse should document the child's pain level, vital signs, and interventions, but only after contacting the healthcare provider and taking appropriate actions.
A school-age child with bronchial asthma has a prescription for albuterol. The child's parent tells the nurse that the medication is used when the child is having difficulty breathing. Which is the best response by the nurse?
Explanation
Choice A reason: Recommending that the parent bring the child in for immediate evaluation is not the best response by the nurse. This may cause unnecessary anxiety and expense for the parent and the child. Albuterol is a bronchodilator that relaxes the muscles in the airways and increases air flow to the lungs. It is used to treat or prevent bronchospasm, or narrowing of the airways, in people with asthma or chronic obstructive pulmonary disease (COPD). It is also used to prevent exercise-induced bronchospasm. It is a quick-relief medication that can be used as needed when the child has difficulty breathing.
Choice B reason: Advising the parent that over-use of the medication may cause chronic bronchitis is not the best response by the nurse. This is not true and may discourage the parent from giving the medication to the child when needed. Chronic bronchitis is a type of COPD that causes inflammation and mucus production in the airways. It is usually caused by smoking or exposure to air pollution, not by albuterol. Albuterol does not cause chronic bronchitis, but it can help relieve the symptoms of bronchospasm in people who have it.
Choice C reason: Confirming that the medication helps to reduce airway inflammation is not the best response by the nurse. This is not accurate and may confuse the parent. Albuterol does not reduce airway inflammation, but it relaxes the muscles around the airways so that they open up and the child can breathe more easily. Albuterol is not an anti-inflammatory medication, but a bronchodilator. Anti-inflammatory medications, such as corticosteroids, are used to prevent or reduce inflammation in the airways, but they are not quick-relief medications like albuterol.
Choice D reason: Assuring the parent that they are using the medication correctly is the best response by the nurse. This shows that the nurse understands the purpose and the proper use of albuterol and that the nurse supports the parent's decision to give the medication to the child when needed. The nurse should also educate the parent on how to use the inhaler device correctly, how to monitor the child's symptoms and peak flow, and when to seek medical attention if the child's condition worsens.
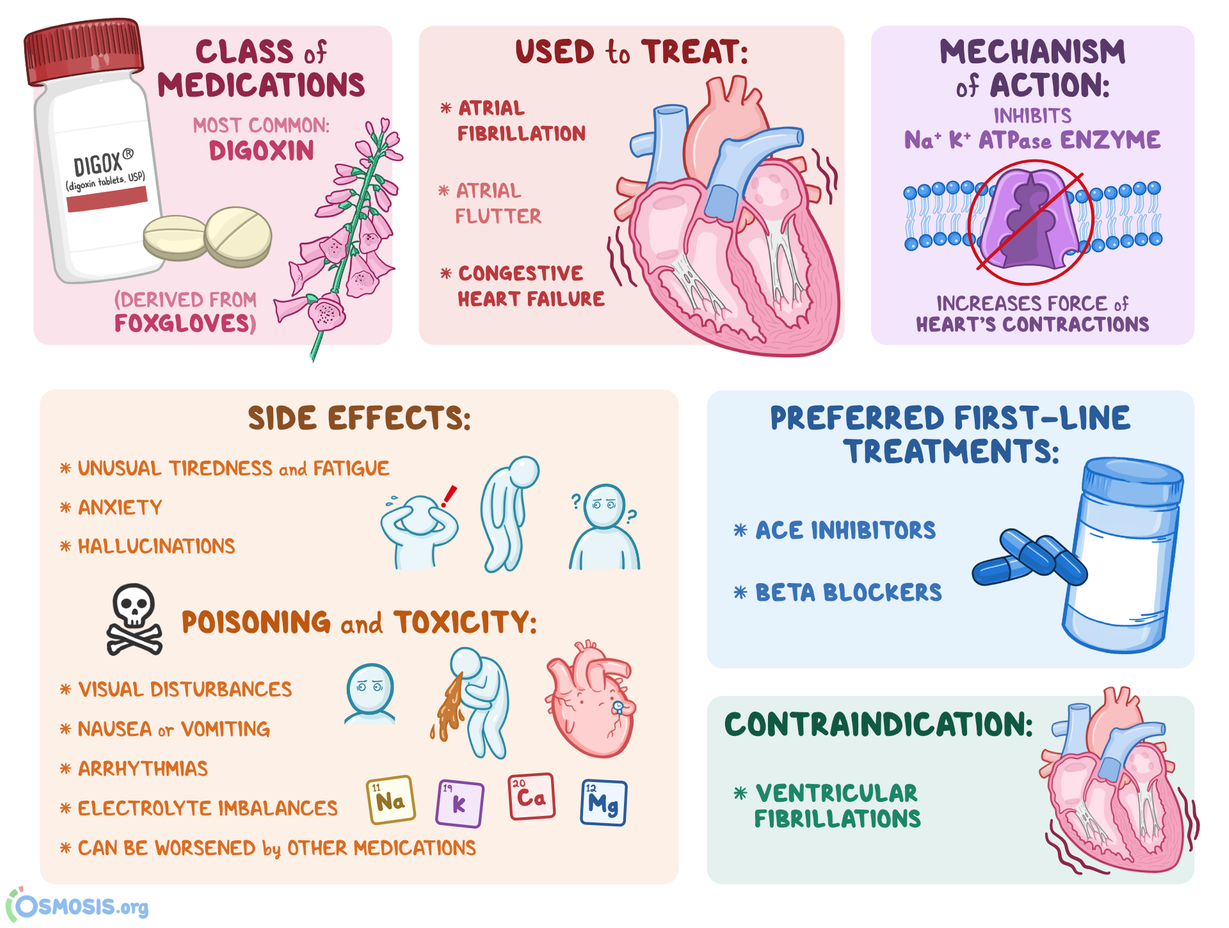
The nurse is preparing to administer medications for an eight-month-old infant with heart failure. The infant has a blood pressure of 114/66 mm Hg, apical pulse of 88 beats/minute, and respirations of 30 breaths/minute. Which medication should the nurse withhold until the health care provider is notified?
Explanation
Choice A reason: Enalapril is an angiotensin-converting enzyme (ACE) inhibitor that is used to treat heart failure in infants. It lowers blood pressure and reduces the workload of the heart. Enalapril is not contraindicated in this scenario and does not need to be withheld.
Choice B reason: Digoxin is a cardiac glycoside that is used to treat heart failure and arrhythmias in infants. It increases the contractility of the heart and slows down the heart rate. Digoxin has a narrow therapeutic range and can cause toxicity if the dose is too high or the infant is dehydrated. Digoxin should be withheld if the infant's apical pulse is less than 90 beats/minute, which is the case in this scenario. The nurse should notify the health care provider and monitor the infant for signs of digoxin toxicity, such as nausea, vomiting, bradycardia, and visual disturbances.
Choice C reason: Hydralazine is a vasodilator that is used to treat hypertension and heart failure in infants. It lowers blood pressure and reduces the afterload of the heart. Hydralazine is not contraindicated in this scenario and does not need to be withheld.
Choice D reason: Furosemide is a loop diuretic that is used to treat fluid overload and edema in infants with heart failure. It lowers blood pressure and reduces the preload of the heart. Furosemide is not contraindicated in this scenario and does not need to be withheld
The nurse is teaching the parents about important dietary changes for their child who is newly diagnosed with celiac disease. Which foods should the nurse include in the list of allowed foods for this child?
Explanation
Choice A reason: Rice is a gluten-free grain that is safe for people with celiac disease. Rice does not contain the protein gluten that triggers an immune reaction and damages the small intestine in people with celiac disease.
Choice B reason: Oats are generally not recommended for people with celiac disease because they are often contaminated with gluten from other grains during processing. Some people with celiac disease may also react to a protein in oats called avenin that is similar to gluten. Only certified gluten-free oats may be safe for some people with celiac disease, but they should consult their health care provider before consuming them³.
Choice C reason: Barley is a grain that contains gluten and is not safe for people with celiac disease. Barley can cause inflammation and damage to the small intestine in people with celiac disease. Barley is also used to make malt, which is a common additive in many processed foods and beverages.
Choice D reason: Rye is a grain that contains gluten and is not safe for people with celiac disease. Rye can cause the same symptoms and complications as wheat and barley in people with celiac disease. Rye is often used to make bread, crackers, and cereals.
The nurse is performing a routine assessment of a 3-year-old at a community health center. Which behavior by the child should alert the nurse to request a follow-up for a possible autism spectrum disorder (ASD)?
Explanation
Choice A reason: Showing indifference to verbal stimulation is not a specific sign of ASD. Some children may have hearing problems, language delays, or other developmental issues that affect their response to verbal cues. However, the nurse should still assess the child's hearing and language skills and refer them to a specialist if needed.
Choice B reason: Having a history of temper tantrums is not a specific sign of ASD. Many children have tantrums as a normal part of their emotional development, especially when they are frustrated, tired, or hungry. However, the nurse should still evaluate the frequency, intensity, and duration of the tantrums and provide guidance to the parents on how to manage them.
Choice C reason: Stroking the hair of a handheld doll is not a specific sign of ASD. This behavior may indicate that the child has a preference for tactile stimulation, which is common among children. It may also show that the child has an attachment to the doll, which is a positive sign of social development.
Choice D reason: Performing odd repetitive behaviors is a specific sign of ASD. These behaviors may include rocking, spinning, hand flapping, lining up objects, or repeating words or sounds. These behaviors are often used by children with ASD to cope with sensory overload, anxiety, or boredom. They may also interfere with the child's learning and social interaction. The nurse should request a follow-up for a possible ASD diagnosis and provide support to the child and the parents.
The nurse is assessing a 6-month-old infant. Which response requires further evaluation by the nurse?
Explanation
Choice A reason: Playing "peek-a-boo" is a normal behavior for a 6-month-old infant. It shows that the infant has developed object permanence, which is the understanding that objects and people still exist even when they are out of sight. This is a sign of cognitive development and social interaction.
Choice B reason: Turning head to locate sound is a normal behavior for a 6-month-old infant. It shows that the infant has developed auditory localization, which is the ability to identify the direction and distance of a sound source. This is a sign of sensory development and curiosity.
Choice C reason: Having doubled birth weight is a normal milestone for a 6-month-old infant. It shows that the infant has adequate growth and nutrition. The average birth weight for a full-term infant is about 3.4 kg (7.5 lb), and the average weight for a 6-month-old infant is about 6.8 kg (15 lb).
Choice D reason: Demonstrating startle reflex is an abnormal behavior for a 6-month-old infant. The startle reflex, also known as the Moro reflex, is an involuntary response to a sudden loud noise or movement. The infant will extend the arms and legs, arch the back, and then curl the arms and legs inward. This reflex is present at birth and usually disappears by 4 months of age. If the reflex persists beyond 6 months of age, it may indicate a neurological problem or developmental delay. The nurse should request further evaluation by the health care provider.
A 9-month-old with Tay-Sachs disease is admitted due to seizures. Which assessment is most important for the nurse to obtain?
Explanation
Choice A reason: The ability to crawl is not the most important assessment for the nurse to obtain. Tay-Sachs disease causes progressive loss of motor skills, so the infant may not be able to crawl or may have regressed from crawling. However, this is not a specific sign of the disease and does not indicate the severity of the condition.
Choice B reason: The eyes with cherry-red spot are not the most important assessment for the nurse to obtain. Tay-Sachs disease causes accumulation of gangliosides in the retina, which results in a cherry-red spot in the center of the macula. However, this is not a specific sign of the disease and does not indicate the severity of the condition.
Choice C reason: The difficulty with swallowing is not the most important assessment for the nurse to obtain. Tay-Sachs disease causes muscle weakness and spasticity, which may affect the infant's ability to swallow. However, this is not a specific sign of the disease and does not indicate the severity of the condition.
Choice D reason: The exaggerated startle reaction is the most important assessment for the nurse to obtain. Tay-Sachs disease causes increased sensitivity to sound and touch, which results in an exaggerated startle reaction. This is a specific sign of the disease and indicates the severity of the condition. The exaggerated startle reaction may also trigger seizures, which can be life-threatening. The nurse should monitor the infant's vital signs, seizure activity, and neurological status closely.
The nurse is caring for a child with sickle cell disease who is experiencing a sickle cell crisis. Which finding should the nurse report to the health care provider immediately?
Explanation
Choice A reason: Chest pain is a sign of acute chest syndrome, which is a life-threatening complication of sickle cell crisis. It occurs when the sickle-shaped red blood cells block the blood vessels in the lungs, causing inflammation, infection, and low oxygen levels. Chest pain may be accompanied by fever, cough, shortness of breath, and wheezes. The nurse should report chest pain to the health care provider immediately and monitor the child's vital signs, oxygen saturation, and respiratory status.
Choice B reason: Jaundice is a common finding in children with sickle cell disease, but it is not an urgent sign of sickle cell crisis. Jaundice occurs when the red blood cells break down faster than the liver can process them, resulting in a buildup of bilirubin in the blood and skin. Jaundice may cause yellowing of the skin, eyes, and mucous membranes, as well as itching and dark urine. The nurse should assess the child's liver function and hydration status, but jaundice does not require immediate intervention.
Choice C reason: Ulcers on the legs are a chronic complication of sickle cell disease, but they are not an acute sign of sickle cell crisis. Ulcers on the legs occur when the blood flow to the skin is impaired by the sickle-shaped red blood cells, causing tissue damage and infection. Ulcers on the legs may cause pain, swelling, and drainage, and they may take a long time to heal. The nurse should clean and dress the ulcers, apply topical antibiotics, and elevate the legs, but ulcers do not require immediate intervention.
Choice D reason: Swelling in the hands or feet is a common finding in children with sickle cell disease, especially in infants and toddlers, but it is not a critical sign of sickle cell crisis. Swelling in the hands or feet occurs when the sickle-shaped red blood cells block the blood vessels in the extremities, causing inflammation and fluid retention. Swelling in the hands or feet may cause pain, stiffness, and difficulty moving the joints. The nurse should apply warm compresses, massage the affected areas, and encourage the child to exercise the joints, but swelling does not require immediate intervention.
Sign Up or Login to view all the 40 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
