Indiana University Medical Surgical Nursing Exam 1
Total Questions : 41
Showing 25 questions, Sign in for moreA patient is admitted for treatment of Cushing's syndrome. The nurse correlates this disease process to which alteration in endocrine function?
Explanation
Choice A reason: Cushing's syndrome is caused by excess cortisol, a type of glucocorticoid hormone, in the body. This can result from overproduction of cortisol by the adrenal glands, or from prolonged use of corticosteroid medications. Elevated glucocorticoid level is the correct alteration in endocrine function for this condition.
Choice B reason: Decreased aldosterone level is not related to Cushing's syndrome. Aldosterone is another hormone produced by the adrenal glands, but it regulates the balance of sodium and potassium in the body. Decreased aldosterone level can cause low blood pressure, dehydration, and electrolyte imbalance.
Choice C reason: Elevated aldosterone secretion is also not related to Cushing's syndrome. Elevated aldosterone secretion can cause high blood pressure, fluid retention, and hypokalemia (low potassium level). This condition is known as hyperaldosteronism or Conn's syndrome.
Choice D reason: Diminished glucocorticoid level is the opposite of Cushing's syndrome. Diminished glucocorticoid level can cause low blood sugar, fatigue, weight loss, and poor stress response. This condition is known as Addison's disease or adrenal insufficiency.
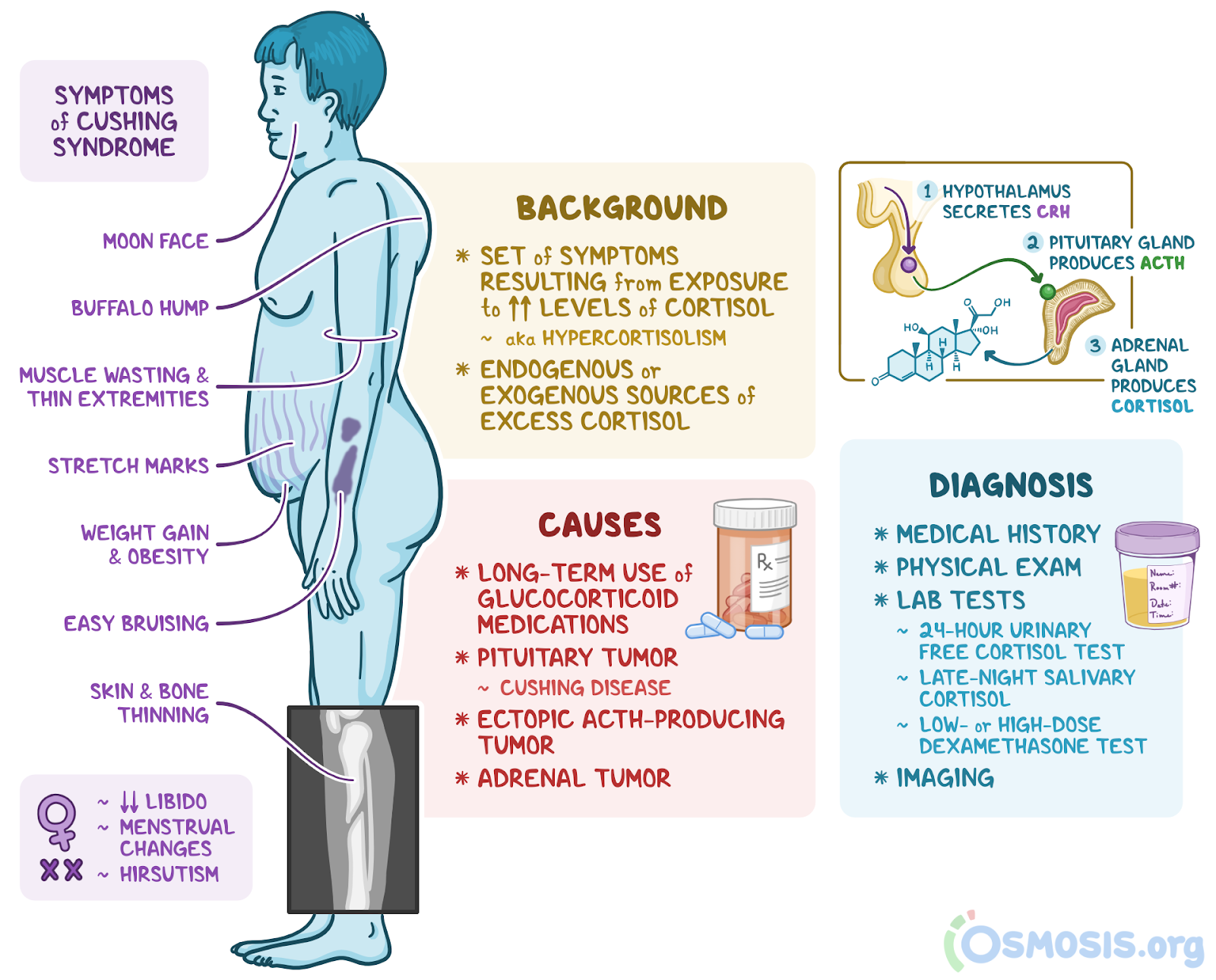
A patient is being admitted with a diagnosis of Cushing syndrome. Which findings will the nurse expect during the assessment?
Explanation
Choice A reason: Purplish streaks on the abdomen are also known as striae. They are caused by the thinning and weakening of the skin due to excess cortisol, a hormone that is elevated in Cushing syndrome. Striae are a common sign of Cushing syndrome, along with weight gain, moon face, and buffalo hump.
Choice B reason: Chronically low blood pressure is not associated with Cushing syndrome. Cushing syndrome can cause high blood pressure, due to the effects of cortisol on the cardiovascular system. Low blood pressure can be a sign of adrenal insufficiency, which is the opposite of Cushing syndrome.
Choice C reason: Bronzed appearance of the skin is not related to Cushing syndrome. Bronzed skin can be a sign of Addison's disease, which is a condition of low cortisol and low aldosterone. Addison's disease can cause hyperpigmentation of the skin, especially in the areas exposed to sun, such as the face, neck, and hands.
Choice D reason: Decreased axillary and pubic hair is also not related to Cushing syndrome. Cushing syndrome can cause increased hair growth, especially on the face, chest, and back. This is due to the androgenic effects of cortisol. Decreased hair growth can be a sign of hypothyroidism, which is a condition of low thyroid hormone.
Which patient statement indicates a need for further education regarding medications after a bilateral adrenalectomy?
Explanation
Choice A reason: I will always need to take hydrocortisone pills is a correct statement. Hydrocortisone is a synthetic form of cortisol, a hormone that is normally produced by the adrenal glands. After a bilateral adrenalectomy, the patient will have no adrenal glands and will need to take hydrocortisone pills for life to replace the missing hormone.
Choice B reason: I have a way to inject hydrocortisone in case of emergency is also a correct statement. Hydrocortisone injections are used to treat acute adrenal crisis, a life-threatening condition that can occur when the patient has low cortisol levels due to stress, illness, injury, or surgery. The patient should have an emergency kit with hydrocortisone injections and instructions on how to use them.
Choice C reason: I will stop taking hydrocortisone when I feel better is an incorrect statement. This indicates a need for further education regarding medications after a bilateral adrenalectomy. The patient should never stop taking hydrocortisone without consulting their doctor, as this can cause severe symptoms of adrenal insufficiency, such as low blood pressure, low blood sugar, weakness, fatigue, and confusion.
Choice D reason: I have nausea or vomiting often is a statement that requires further assessment by the nurse. Nausea or vomiting can be signs of inadequate or excessive hydrocortisone dosage, or other complications after a bilateral adrenalectomy. The nurse should monitor the patient's vital signs, blood glucose, electrolytes, and weight, and report any abnormal findings to the doctor. The patient may need to adjust their hydrocortisone dose or take other medications to manage their symptoms.
A college student is newly diagnosed with type 1 diabetes. She now has a headache, changes in her vision, and is anxious, but does not have her portable blood glucose monitor with her. Which action should the campus nurse advise her to take?
Explanation
Choice A reason: Eating a piece of pizza is not a good option for the student. Pizza is a complex carbohydrate that contains fat and protein, which can delay the absorption of glucose and cause unpredictable blood sugar levels. The student needs a simple carbohydrate that can quickly raise her blood sugar level, such as glucose tablets, fruit juice, or candy.
Choice B reason: Taking an extra dose of rapid-acting insulin is a dangerous option for the student. Insulin lowers the blood sugar level, and the student already has symptoms of hypoglycemia (low blood sugar), such as headache, vision changes, and anxiety. Taking more insulin can worsen her condition and cause seizures, coma, or death.
Choice C reason: Eating 15 g of simple carbohydrates is the best option for the student. Simple carbohydrates are easily digested and absorbed into the bloodstream, and can raise the blood sugar level within 15 minutes. The student should eat 15 g of simple carbohydrates, such as four glucose tablets, half a cup of fruit juice, or three pieces of hard candy, and then check her blood sugar level if possible.
Choice D reason: Drinking some diet pop is not a helpful option for the student. Diet pop does not contain any sugar or calories, and will not affect the blood sugar level. The student needs a source of glucose to treat her hypoglycemia, and diet pop will not provide that.
The nurse may notice which clinical manifestation in the pediatric client diagnosed with type 1 diabetes mellitus?
Explanation
Choice A reason: Weight loss is a common clinical manifestation of type 1 diabetes mellitus in children. Type 1 diabetes mellitus is a condition where the pancreas does not produce enough insulin, a hormone that helps the cells use glucose for energy. Without insulin, the glucose stays in the blood and causes high blood sugar levels. The body then breaks down fat and muscle for energy, resulting in weight loss.
Choice B reason: Low urine output is not a typical clinical manifestation of type 1 diabetes mellitus in children. In fact, the opposite is true: high urine output is a sign of type 1 diabetes mellitus. This is because the excess glucose in the blood draws water from the cells and tissues, causing dehydration and increased thirst. The kidneys then try to flush out the glucose and water through urine, leading to frequent urination.
Choice C reason: Weight gain is not a usual clinical manifestation of type 1 diabetes mellitus in children. As explained in choice A, type 1 diabetes mellitus causes weight loss due to the lack of insulin and the breakdown of fat and muscle. Weight gain can be a sign of type 2 diabetes mellitus, which is a condition where the cells become resistant to insulin and the pancreas cannot produce enough insulin to overcome the resistance. Weight gain can also be a side effect of insulin therapy, which is used to treat both types of diabetes mellitus.
Choice D reason: Hand tremors are not a specific clinical manifestation of type 1 diabetes mellitus in children. Hand tremors can be caused by many factors, such as anxiety, stress, caffeine, medication, or neurological disorders. Hand tremors can also be a symptom of hypoglycemia, which is a condition of low blood sugar that can occur in people with diabetes mellitus. However, hypoglycemia is not exclusive to diabetes mellitus, and can affect anyone who has a low intake of food, a high expenditure of energy, or a high dose of insulin or oral hypoglycemic agents.
A patient with type 2 diabetes is scheduled for a follow-up visit in the clinic several months from now. Which test will the nurse schedule to evaluate the effectiveness of treatment for the patient?
Explanation
Choice A reason: Urine dipstick for glucose is not a reliable test to evaluate the effectiveness of treatment for type 2 diabetes. Urine glucose testing can only detect glucose in the urine when the blood glucose level is very high, above the renal threshold of 180 mg/dL. Urine glucose testing does not reflect the average blood glucose level over time, and can be affected by factors such as hydration, medication, and urinary tract infections.
Choice B reason: Fasting blood glucose is a test that measures the blood glucose level after an overnight fast of at least 8 hours. Fasting blood glucose is a useful test to diagnose diabetes, but it is not the best test to evaluate the effectiveness of treatment for type 2 diabetes. Fasting blood glucose only reflects the blood glucose level at one point in time, and can vary depending on the time of day, the amount and type of food eaten, and the activity level.
Choice C reason: Oral glucose tolerance is a test that measures the blood glucose level before and after drinking a solution containing 75 g of glucose. Oral glucose tolerance is another test that can diagnose diabetes, but it is not the most convenient or accurate test to evaluate the effectiveness of treatment for type 2 diabetes. Oral glucose tolerance requires the patient to fast for at least 8 hours, drink the glucose solution, and have blood samples taken at 0, 30, 60, 90, and 120 minutes. Oral glucose tolerance can also be influenced by factors such as stress, illness, medication, and menstrual cycle.
Choice D reason: Glycosylated hemoglobin (Hemoglobin A1C) is a test that measures the percentage of hemoglobin that has glucose attached to it. Hemoglobin is a protein in the red blood cells that carries oxygen. Red blood cells have a lifespan of about 120 days, so the hemoglobin A1C test reflects the average blood glucose level over the past 2 to 3 months. Hemoglobin A1C is the best test to evaluate the effectiveness of treatment for type 2 diabetes, as it shows how well the blood glucose level has been controlled over time, and is not affected by factors such as fasting, food intake, or daily fluctuations.
Which information obtained by the nurse in the endocrine clinic about a patient who has been taking prednisone 40 mg daily for 3 weeks is most important to report to the health care provider?
Explanation
Choice A reason: Patient stopped taking the medication 2 days ago is the most important information to report to the health care provider. Prednisone is a corticosteroid medication that suppresses the immune system and reduces inflammation. Prednisone also affects the production of cortisol, a hormone that regulates the stress response, blood pressure, blood sugar, and metabolism. Prednisone should not be stopped abruptly, as this can cause adrenal insufficiency, a condition where the adrenal glands cannot produce enough cortisol. Adrenal insufficiency can cause symptoms such as fatigue, weakness, nausea, vomiting, low blood pressure, and hypoglycemia. The patient should be instructed to resume taking the prednisone and taper the dose gradually under the supervision of the health care provider.
Choice B reason: Patient has not been taking the prescribed vitamin D is not as important as choice A, but still requires further education by the nurse. Vitamin D is a fat-soluble vitamin that helps the body absorb calcium and phosphorus, and maintain bone health. Prednisone can interfere with the metabolism of vitamin D and cause bone loss, osteoporosis, and fractures. The patient should be advised to take the prescribed vitamin D supplement and eat foods rich in vitamin D, such as fatty fish, egg yolks, cheese, and fortified milk.
Choice C reason: Patient has bilateral 2+ pitting ankle edema is not as critical as choice A, but still needs to be monitored by the nurse. Ankle edema is swelling of the ankles due to fluid accumulation in the tissues. Prednisone can cause ankle edema by increasing the sodium and water retention in the body, and reducing the potassium excretion by the kidneys. The patient should be assessed for signs of fluid overload, such as weight gain, shortness of breath, and crackles in the lungs. The patient should also be encouraged to limit the intake of salt and fluids, and elevate the legs when sitting or lying down.
Choice D reason: Patient's blood pressure is 148/94 mm Hg is not as urgent as choice A, but still needs to be addressed by the nurse. Blood pressure is the force of blood against the walls of the arteries. Prednisone can increase the blood pressure by stimulating the renin-angiotensin-aldosterone system, a hormonal system that regulates the blood volume and pressure. The patient should be advised to check the blood pressure regularly, and report any readings above 140/90 mm Hg to the health care provider. The patient should also be counseled to follow a healthy lifestyle, such as exercising, quitting smoking, reducing stress, and eating a balanced diet low in sodium, fat, and cholesterol.
Which patient statement indicates to the nurse the need for further teaching regarding the new diagnosis of type 1 diabetes mellitus (DM)?
Explanation
Choice A reason: I will need to take medication by mouth until my blood sugar is within normal limits again is an incorrect statement that indicates the need for further teaching. Type 1 diabetes mellitus (DM) is a condition where the pancreas does not produce any insulin, a hormone that helps the cells use glucose for energy. Patients with type 1 DM need to take insulin injections or use an insulin pump for life to replace the missing hormone. Oral medications for diabetes are not effective for type 1 DM, as they work by stimulating the pancreas to produce more insulin or by increasing the sensitivity of the cells to insulin.
Choice B reason: If I get the flu, the dose of my insulin may need to be altered to control my blood glucose is a correct statement that shows understanding of the disease process. Illnesses such as the flu can increase the blood glucose level, as the body releases hormones that counteract the effects of insulin. Patients with type 1 DM may need to adjust their insulin dose, monitor their blood glucose more frequently, and check for ketones in their urine or blood when they are sick. Ketones are acidic substances that are produced when the body breaks down fat for energy, and can lead to a serious complication called diabetic ketoacidosis.
Choice C reason: I will monitor my blood glucose to help determine whether my medication is working as anticipated is another correct statement that demonstrates knowledge of the disease management. Blood glucose monitoring is an essential part of diabetes care, as it helps the patients and the health care providers to evaluate the effectiveness of the insulin therapy, the diet, and the exercise plan. Blood glucose monitoring also helps to prevent or detect hypoglycemia (low blood sugar) and hyperglycemia (high blood sugar), and to adjust the insulin dose accordingly.
Choice D reason: The things that I eat may impact the dose of my medication used to control my blood glucose is also a correct statement that reflects awareness of the disease implications. The amount and type of carbohydrates that the patients eat can affect their blood glucose level, as carbohydrates are the main source of glucose in the diet. Patients with type 1 DM need to balance their insulin dose with their carbohydrate intake, and follow a consistent and healthy eating pattern. They may also use carbohydrate counting, a method of estimating the grams of carbohydrates in the foods they eat, to help them plan their meals and snacks.
Jo is a client with Type 1 Diabetes. Jo has a blood glucose level of 644 mg/dL. The nurse interprets that this client is most at risk of developing which type of acid-base imbalance?
Explanation
Choice A reason: Metabolic acidosis is a condition where the blood pH is lower than normal, due to an excess of acids or a loss of bases in the body. Jo is most at risk of developing metabolic acidosis, because of the high blood glucose level. High blood glucose can cause diabetic ketoacidosis, a complication of Type 1 Diabetes, where the body breaks down fat for energy and produces ketones, which are acidic substances. Ketones can accumulate in the blood and lower the pH, causing symptoms such as nausea, vomiting, abdominal pain, fruity breath, and confusion.
Choice B reason: Metabolic alkalosis is a condition where the blood pH is higher than normal, due to an excess of bases or a loss of acids in the body. Jo is not likely to develop metabolic alkalosis, because of the high blood glucose level. Metabolic alkalosis can be caused by conditions such as vomiting, diuretic use, or excessive antacid intake, which can increase the bicarbonate level or decrease the chloride level in the blood. These conditions are not related to Jo's diabetes.
Choice C reason: Respiratory acidosis is a condition where the blood pH is lower than normal, due to an accumulation of carbon dioxide in the body. Jo is not prone to developing respiratory acidosis, because of the high blood glucose level. Respiratory acidosis can be caused by conditions that impair the lung function, such as asthma, chronic obstructive pulmonary disease (COPD), or pneumonia, which can reduce the ventilation and increase the carbon dioxide level in the blood. These conditions are not related to Jo's diabetes.
Choice D reason: Respiratory alkalosis is a condition where the blood pH is higher than normal, due to a loss of carbon dioxide in the body. Jo is not susceptible to developing respiratory alkalosis, because of the high blood glucose level. Respiratory alkalosis can be caused by conditions that increase the breathing rate, such as anxiety, fever, or hyperventilation, which can reduce the carbon dioxide level in the blood. These conditions are not related to Jo's diabetes.
A few weeks after an 82-year-old patient with a new diagnosis of type 2 diabetes has been placed on metformin (Glucophage) therapy and taught about appropriate diet and exercise, the home health nurse makes a visit. Which finding should the nurse promptly discuss with the health care provider?
Explanation
Choice A reason: Last eye examination was 18 months ago is not a finding that requires immediate attention from the health care provider. However, the nurse should remind the patient of the importance of regular eye examinations, as diabetes can increase the risk of eye problems, such as cataracts, glaucoma, and diabetic retinopathy. The American Diabetes Association (ADA) recommends that patients with type 2 diabetes have a comprehensive eye examination at least once every two years¹.
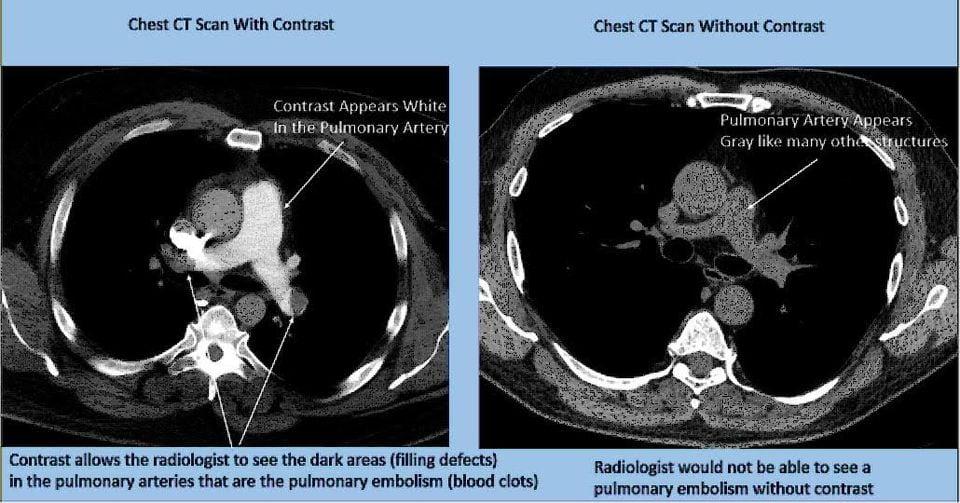
Choice B reason: Patient states they are scheduled for a CT scan with contrast dye the next day is a finding that should be promptly discussed with the health care provider. Metformin is a medication that lowers the blood glucose level by reducing the liver's production of glucose and increasing the cells' sensitivity to insulin. Metformin can interact with contrast dye, which is a substance that is injected into the veins to enhance the visibility of organs and tissues in imaging tests, such as CT scans. Contrast dye can impair the kidney function and increase the risk of lactic acidosis, a rare but serious condition where the blood becomes too acidic due to the accumulation of lactic acid. Lactic acidosis can cause symptoms such as nausea, vomiting, abdominal pain, muscle weakness, and breathing difficulties. To prevent this complication, the ADA recommends that patients stop taking metformin at the time of or before the imaging procedure, and resume it 48 hours after the procedure, only if the kidney function is normal².
Choice C reason: Hemoglobin A1C level is 7.9% is not a finding that needs urgent discussion with the health care provider. Hemoglobin A1C is a test that measures the average blood glucose level over the past two to three months. It reflects how well the diabetes is controlled over time. The ADA recommends that most patients with type 2 diabetes aim for a hemoglobin A1C level of less than 7%, as this can reduce the risk of diabetes complications, such as heart disease, kidney disease, nerve damage, and eye damage. A hemoglobin A1C level of 7.9% indicates that the patient's blood glucose level is slightly above the target range, and may need some adjustment in the medication, diet, or exercise plan. However, this is not an emergency situation, and the nurse can review the patient's self-monitoring records, medication adherence, and lifestyle factors, and provide education and support as needed.
Choice D reason: Patient has questions about the prescribed diet is not a finding that warrants immediate communication with the health care provider. However, the nurse should address the patient's questions and concerns, and provide clear and consistent information about the dietary recommendations for type 2 diabetes. A healthy diet for type 2 diabetes should include a variety of foods, such as vegetables, fruits, whole grains, lean proteins, low-fat dairy, and healthy fats. The patient should also limit the intake of added sugars, refined carbohydrates, saturated fats, trans fats, and sodium. The nurse can help the patient plan their meals and snacks, and use tools such as carbohydrate counting, portion control, or the plate method to balance their food choices and blood glucose levels..
The patient received Humalog (rapid acting) insulin 5 units subcutaneously at 8:00 AM. The nurse plans to monitor this patient for signs of hypoglycemia at which time related to the insulin's peak action?
Explanation
Choice A reason: 1:00 PM is not the correct time to monitor the patient for signs of hypoglycemia related to the insulin's peak action. Humalog is a rapid acting insulin that starts to work within 15 minutes, peaks in about an hour, and lasts for 2 to 4 hours. Therefore, the peak action of Humalog given at 8:00 AM would be around 9:00 AM, not 1:00 PM.
Choice B reason: 8:00 PM is also not the correct time to monitor the patient for signs of hypoglycemia related to the insulin's peak action. As explained in choice A, Humalog peaks in about an hour and lasts for 2 to 4 hours. Therefore, the effect of Humalog given at 8:00 AM would wear off by 12:00 PM, not 8:00 PM.
Choice C reason: There is no peak action for this insulin is an incorrect statement. Humalog does have a peak action, as described in choice A. The peak action of an insulin is the time when the insulin is most effective in lowering the blood glucose level. The peak action of an insulin can vary depending on the type, dose, and individual response of the patient.
Choice D reason: 9:00 AM is the correct time to monitor the patient for signs of hypoglycemia related to the insulin's peak action. Hypoglycemia is a condition of low blood glucose level, which can cause symptoms such as sweating, shaking, hunger, headache, dizziness, confusion, and loss of consciousness. Hypoglycemia can occur when the insulin dose is too high, the food intake is too low, or the physical activity is too high. The nurse should monitor the patient for signs of hypoglycemia around the peak action of the insulin, as this is when the blood glucose level is most likely to drop. The nurse should also teach the patient how to prevent, recognize, and treat hypoglycemia.
After change-of-shift report, which patient will the nurse assess first?
Explanation
Choice A reason: A 68-year-old patient with type 2 diabetes who has peripheral neuropathy and complains of burning foot pain is not the most urgent patient to assess. Peripheral neuropathy is a complication of diabetes that affects the nerves, especially in the feet and legs. It can cause symptoms such as numbness, tingling, burning, or pain. The nurse should assess the patient's foot condition, provide pain relief, and educate the patient on foot care. However, this patient is not in immediate danger, and can wait until the nurse finishes assessing the more critical patient.
Choice B reason: A 35-year-old patient with type 1 diabetes whose most recent blood glucose reading was 230 mg/dL is not the most critical patient to assess. Type 1 diabetes is a condition where the pancreas does not produce any insulin, a hormone that helps the cells use glucose for energy. Patients with type 1 diabetes need to take insulin injections or use an insulin pump to control their blood glucose level. A blood glucose reading of 230 mg/dL is above the normal range of 70 to 130 mg/dL before meals, and indicates hyperglycemia (high blood sugar). The nurse should check the patient's insulin dose, monitor the patient's symptoms, and provide education on blood glucose management. However, this patient is not in life-threatening condition, and can wait until the nurse attends to the more serious patient.
Choice C reason: A 60-year-old patient with hyperosmolar hyperglycemic syndrome with dry oral mucosa and low urine output is the most important patient to assess. Hyperosmolar hyperglycemic syndrome (HHS) is a severe complication of diabetes that occurs when the blood glucose level is extremely high, usually above 600 mg/dL. HHS can cause dehydration, electrolyte imbalance, and coma. Dry oral mucosa and low urine output are signs of dehydration, which can lead to shock and organ failure. The nurse should assess the patient's vital signs, blood glucose level, fluid and electrolyte status, and neurological function. The nurse should also administer intravenous fluids, insulin, and electrolytes as prescribed by the health care provider. This patient is in a medical emergency, and needs immediate intervention.
Choice D reason: A 19-year-old patient with type 1 diabetes who was admitted with possible dawn phenomenon is not the most acute patient to assess. Dawn phenomenon is a condition where the blood glucose level rises in the early morning, usually between 2:00 AM and 8:00 AM. This is due to the release of hormones that increase the blood glucose level, such as growth hormone, cortisol, and glucagon. The nurse should review the patient's blood glucose records, adjust the insulin dose or timing, and provide education on how to prevent or manage the dawn phenomenon. However, this patient is not in a critical situation, and can wait until the nurse evaluates the more unstable patient.
A patient with diabetes is starting on insulin therapy. Which type of insulin will the nurse discuss using for mealtime coverage?
Explanation
Choice A reason: Lispro (Humalog) is a type of insulin that is used for mealtime coverage. It is a rapid-acting insulin that starts to work within 15 minutes, peaks in about an hour, and lasts for 2 to 4 hours. It mimics the natural insulin response to food intake, and helps to lower the blood glucose level after meals. The nurse will discuss using lispro for mealtime coverage, and instruct the patient to inject it within 15 minutes before or after eating.
Choice B reason: NPH (Humulin N) is a type of insulin that is not used for mealtime coverage. It is an intermediate-acting insulin that starts to work within 2 to 4 hours, peaks in 4 to 12 hours, and lasts for 12 to 18 hours. It provides a steady background of insulin throughout the day, and helps to control the blood glucose level between meals and overnight. The nurse will discuss using NPH for basal coverage, and instruct the patient to inject it once or twice a day, usually in the morning and/or evening.
Choice C reason: Detemir (Levemir) is a type of insulin that is not used for mealtime coverage. It is a long-acting insulin that starts to work within 1 to 2 hours, has no peak, and lasts for up to 24 hours. It provides a constant level of insulin throughout the day, and helps to maintain the blood glucose level at a stable range. The nurse will discuss using detemir for basal coverage, and instruct the patient to inject it once or twice a day, depending on the individual needs.
Choice D reason: Glargine (Lantus) is a type of insulin that is not used for mealtime coverage. It is a long-acting insulin that starts to work within 1 to 2 hours, has no peak, and lasts for up to 24 hours. It provides a constant level of insulin throughout the day, and helps to maintain the blood glucose level at a stable range. The nurse will discuss using glargine for basal coverage, and instruct the patient to inject it once a day, usually at the same time every day.

Heparin 7.,000 units is ordered. Heparin S.000 units per mL is available, How many milliliters (mL) should the nurse administer?
(Do not round)
Explanation
The nurse should administer 1.4 mL of Heparin to the patient.
To calculate the number of milliliters (mL) the nurse should administer, we can use the following steps:
Step 1: Calculate the total amount of Heparin available in mL
Heparin concentration: 5,000 units per mL
Ordered Heparin dose: 7,000 units
Total mL of Heparin needed = Ordered dose / Heparin concentration
Total mL = 7,000 units / 5,000 units per mL = 1.4 mL
The nurse is caring for a patient who has diabetes and complains of chronic, burning leg pain even when taking oxycodone (OxyContin) twice daily. Which prescribed medication is the best choice for the nurse to administer as an adjuvant to decrease the patient's pain?
Explanation
Choice A reason: This statement is false. Acetaminophen (Tylenol) is not the best choice for the nurse to administer as an adjuvant to decrease the patient's pain, as acetaminophen is a mild analgesic that works by inhibiting the synthesis of prostaglandins, which are involved in inflammation and pain. Acetaminophen is not very effective for chronic, burning leg pain, which is likely caused by diabetic neuropathy, a nerve damage condition that affects the sensation and function of the legs.
Choice B reason: This statement is true. Gabapentin (Neurontin) is the best choice for the nurse to administer as an adjuvant to decrease the patient's pain, as gabapentin is an anticonvulsant that works by modulating the activity of calcium channels, which are involved in transmitting pain signals from the nerves to the brain. Gabapentin is effective for chronic, burning leg pain, as it can reduce the intensity and frequency of neuropathic pain.
Choice C reason: This statement is false. Hydrocodone-Acetaminophen (Norco) is not the best choice for the nurse to administer as an adjuvant to decrease the patient's pain, as hydrocodone-acetaminophen is a combination of an opioid analgesic and a mild analgesic that works by binding to opioid receptors in the brain and spinal cord, and by inhibiting the synthesis of prostaglandins, respectively. Hydrocodone-acetaminophen is not very effective for chronic, burning leg pain, as it can cause tolerance, dependence, and addiction, and can also interact with oxycodone, which the patient is already taking.
Choice D reason: This statement is false. Aspirin is not the best choice for the nurse to administer as an adjuvant to decrease the patient's pain, as aspirin is a nonsteroidal anti-inflammatory drug (NSAID) that works by inhibiting the synthesis of prostaglandins, which are involved in inflammation and pain. Aspirin is not very effective for chronic, burning leg pain, as it can cause gastrointestinal bleeding, ulcers, and kidney damage, and can also interact with other medications that the patient may be taking, such as anticoagulants or antiplatelets.
The nurse is caring for an infant who weighs 16 kg. Calculate the daily maintenance fluid requirement for this child. Round to the nearest whole number.
Explanation
Choice A reason: 363 is not the correct answer. This is the daily maintenance fluid requirement for an infant who weighs 3.5 kg, not 16 kg. The formula for calculating the daily maintenance fluid requirement for infants who weigh between 3.5 and 10 kg is 100 mL/kg¹.
Choice B reason: 727 is not the correct answer. This is the daily maintenance fluid requirement for an infant who weighs 10 kg, not 16 kg. The formula for calculating the daily maintenance fluid requirement for infants who weigh between 10 and 20 kg is 1000 mL plus 50 mL for every kg over 10¹.
Choice C reason: 1300 is the correct answer. This is the daily maintenance fluid requirement for an infant who weighs 16 kg. The formula for calculating the daily maintenance fluid requirement for infants who weigh between 10 and 20 kg is 1000 mL plus 50 mL for every kg over 10¹. Therefore, for an infant who weighs 16 kg, the daily maintenance fluid requirement is 1000 mL plus 50 mL times 6, which equals 1300 mL.
Choice D reason: 1600 is not the correct answer. This is the daily maintenance fluid requirement for an infant who weighs 20 kg, not 16 kg. The formula for calculating the daily maintenance fluid requirement for infants who weigh between 10 and 20 kg is 1000 mL plus 50 mL for every kg over 10¹. For infants who weigh more than 20 kg, the formula is 1500 mL plus 20 mL for every kg over 20¹.
The nurse is caring for a 10-month old client with dehydration. What method would the nurse use to measure urine output?
Explanation
Choice A reason: Performing an in/out catheterization is not a suitable method to measure urine output for a 10-month old client with dehydration. An in/out catheterization is a procedure where a catheter is inserted into the bladder through the urethra, and the urine is drained and measured. This method is invasive, painful, and carries the risk of infection and trauma. It is usually reserved for clients who have urinary retention or obstruction, or who need a sterile urine sample.
Choice B reason: Inserting a Foley catheter is also not an appropriate method to measure urine output for a 10-month old client with dehydration. A Foley catheter is a type of catheter that stays in the bladder and drains the urine into a collection bag. This method is also invasive, painful, and carries the risk of infection and trauma. It is usually used for clients who have urinary incontinence, surgery, or long-term bed rest.
Choice C reason: Collecting the client's urine in a cup is not a feasible method to measure urine output for a 10-month old client with dehydration. A cup is not a reliable or accurate device to collect and measure urine, especially for a young child who may not be toilet trained or cooperative. It is also difficult to ensure that all the urine is collected in the cup, and that the cup is not contaminated by other fluids or substances.
Choice D reason: Counting the number of wet diapers is the best method to measure urine output for a 10-month old client with dehydration. This method is non-invasive, simple, and practical. It can provide an estimate of the urine volume and frequency, and indicate the hydration status of the child. The nurse should weigh the diapers before and after use, and record the difference in grams. One gram of weight equals one milliliter of urine. The nurse should also observe the color, odor, and concentration of the urine. The normal urine output for a child is 1 to 2 mL/kg/hour.
An 18-month-old is brought to the emergency department with severe dehydration and weight loss secondary to acute diarrhea and vomiting. The nurse knows that therapeutic management of this child will begin with:
Explanation
Choice A reason: Administration of an anti-diarrheal is not the appropriate management for an 18-month-old with severe dehydration and weight loss secondary to acute diarrhea and vomiting. Anti-diarrheals are not recommended for children under 5 years, as they can have serious side effects, such as paralytic ileus, toxic megacolon, and worsening of dehydration. Anti-diarrheals do not address the underlying cause of diarrhea, and may prolong the duration of infection or toxin exposure.
Choice B reason: Clear liquids, 1 to 2 ounces at a time, are not sufficient to treat an 18-month-old with severe dehydration and weight loss secondary to acute diarrhea and vomiting. Clear liquids, such as water, tea, or broth, do not contain enough electrolytes, such as sodium, potassium, and bicarbonate, to replace the losses from diarrhea and vomiting. Clear liquids may also dilute the blood sodium level and cause hyponatremia, a condition of low sodium in the blood, which can lead to seizures, coma, and death.
Choice C reason: Oral rehydration solution (ORS) is the best management for an 18-month-old with severe dehydration and weight loss secondary to acute diarrhea and vomiting. ORS is a specially formulated solution that contains water, glucose, and electrolytes in the right proportions to replenish the fluid and electrolyte losses from diarrhea and vomiting. ORS can prevent or treat dehydration, and reduce the need for intravenous fluids. ORS can be given by mouth, spoon, cup, or syringe, depending on the child's ability to drink. The amount of ORS to give depends on the degree of dehydration and the weight of the child. The nurse should follow the guidelines from the World Health Organization (WHO) or the local health authority for the appropriate dosage and frequency of ORS administration¹.
Choice D reason: Intravenous fluids are not the first-line management for an 18-month-old with severe dehydration and weight loss secondary to acute diarrhea and vomiting. Intravenous fluids are only indicated for children who have severe dehydration and are unable to drink or tolerate ORS, or who have signs of shock, such as weak pulse, cold extremities, or altered consciousness. Intravenous fluids require hospitalization, skilled personnel, and sterile equipment, and carry the risk of infection, overhydration, or electrolyte imbalance. Intravenous fluids should be given according to the WHO or the local health authority guidelines, and should be switched to ORS as soon as the child is able to drink¹.
When Jo returns home, the nurse provides education about long-term complications. The nurse explains the importance of annual/yearly screenings, such as eye exams and...
Explanation
Choice A reason: Foot inspection is not an annual/yearly screening, but a daily self-care practice for people with diabetes. Foot inspection involves checking the feet for any signs of injury, infection, or ulceration, such as cuts, blisters, redness, swelling, or drainage. Foot inspection can help prevent or detect foot problems, such as neuropathy, ischemia, or infection, which can lead to amputation if left untreated. The nurse should teach Jo how to inspect his feet every day, and how to care for his feet, such as washing, drying, moisturizing, trimming nails, and wearing proper footwear.
Choice B reason: Serum creatinine (Cr) is an annual/yearly screening for people with diabetes. Serum creatinine is a blood test that measures the level of creatinine, a waste product that is filtered by the kidneys. Serum creatinine can indicate the kidney function, and detect kidney damage or disease, which is a common complication of diabetes. The nurse should explain to Jo that he needs to have his serum creatinine checked every year, and that he should keep his blood glucose and blood pressure under control, as these are the main risk factors for kidney problems.
Choice C reason: Chest X-ray is not an annual/yearly screening for people with diabetes, unless they have symptoms or risk factors for lung diseases, such as tuberculosis, pneumonia, or cancer. Chest X-ray is an imaging test that uses X-rays to produce pictures of the lungs and the chest cavity. Chest X-ray can help diagnose or monitor lung conditions, such as infections, inflammations, or tumors. The nurse should ask Jo about his history of smoking, exposure to environmental pollutants, or respiratory symptoms, such as cough, shortness of breath, or chest pain, and refer him to a doctor if he needs a chest X-ray.
Choice D reason: White blood cell count (WBC) is not an annual/yearly screening for people with diabetes, unless they have signs or risk factors for infections, such as fever, wounds, or immunosuppression. White blood cell count is a blood test that measures the number and types of white blood cells, which are the cells that fight infections and inflammation. White blood cell count can help diagnose or monitor infections, such as bacterial, viral, or fungal infections, or immune disorders, such as allergies, autoimmune diseases, or cancers. The nurse should assess Jo for any signs of infection, such as fever, chills, malaise, or pus, and advise him to seek medical attention if he has any.
The nurse reads the chart for a client with diabetes. The chart indicates 'history of autonomic neuropathy.' The nurse knows that autonomic neuropathy may cause which symptoms?
Explanation
Choice A reason: Burning pain and tingling in extremities are not symptoms of autonomic neuropathy, but of peripheral neuropathy. Peripheral neuropathy affects the sensory and motor nerves that innervate the skin, muscles, and joints. It can cause pain, numbness, weakness, and loss of sensation in the extremities. Autonomic neuropathy affects the nerves that control the involuntary functions of the body, such as digestion, blood pressure, heart rate, and sweating.
Choice B reason: Nausea and feeling of abdominal fullness are symptoms of autonomic neuropathy, specifically of gastroparesis. Gastroparesis is a condition where the stomach muscles are weakened or paralyzed, and cannot move food properly. It can cause delayed gastric emptying, nausea, vomiting, bloating, early satiety, and poor blood glucose control. Autonomic neuropathy can damage the vagus nerve, which regulates the stomach motility and secretion.
Choice C reason: Elevated blood pressure and delayed capillary refill are not symptoms of autonomic neuropathy, but of cardiovascular problems. Blood pressure is the force of blood against the walls of the arteries, and capillary refill is the time it takes for the color to return to the nail bed after pressing on it. Elevated blood pressure can indicate hypertension, which is a risk factor for heart disease and stroke. Delayed capillary refill can indicate poor blood circulation, which can be caused by atherosclerosis, peripheral artery disease, or shock. Autonomic neuropathy can affect the blood pressure and heart rate, but usually causes hypotension and tachycardia, not hypertension and delayed capillary refill.
Choice D reason: Increased thirst and excessive urination are not symptoms of autonomic neuropathy, but of diabetes mellitus. Diabetes mellitus is a condition where the body cannot produce or use insulin properly, and the blood glucose level becomes too high. Increased thirst and excessive urination are signs of hyperglycemia, which is a high blood glucose level. Hyperglycemia can cause dehydration, electrolyte imbalance, and ketoacidosis. Autonomic neuropathy can be a complication of diabetes mellitus, but it does not cause increased thirst and excessive urination.
A client is taking furosemide (Lasix) for management of mild hypertension. The nurse knows to assess laboratory results for a side effect of this diuretic. Select the lab value that matches a common side effect of this medication.
Explanation
Choice A reason: A serum potassium level of 5.6 mEq/L is not a common side effect of furosemide, but of hyperkalemia. Hyperkalemia is a condition where the blood potassium level is too high. It can cause muscle weakness, irregular heartbeat, and cardiac arrest. Furosemide is a loop diuretic that increases the urinary excretion of water, sodium, chloride, and potassium. It can cause hypokalemia, which is a low blood potassium level, not hyperkalemia.
Choice B reason: A serum sodium level of 142 mEq/L is not a common side effect of furosemide, but of normal sodium level. The normal range of serum sodium level is 135 to 145 mEq/L. Sodium is an electrolyte that helps regulate the fluid balance, nerve impulses, and muscle contractions in the body. Furosemide can cause hyponatremia, which is a low blood sodium level, but not a normal sodium level.
Choice C reason: A serum sodium level of 138 mEq/L is also not a common side effect of furosemide, but of normal sodium level. As explained in choice B, the normal range of serum sodium level is 135 to 145 mEq/L. Furosemide can cause hyponatremia, which is a low blood sodium level, but not a normal sodium level.
Choice D reason: A serum potassium level of 2.8 mEq/L is a common side effect of furosemide, and of hypokalemia. Hypokalemia is a condition where the blood potassium level is too low. It can cause muscle cramps, fatigue, weakness, arrhythmias, and paralysis. Furosemide is a loop diuretic that increases the urinary excretion of water, sodium, chloride, and potassium. It can cause hypokalemia, which is a low blood potassium level. The nurse should monitor the client's serum potassium level and signs of hypokalemia, and advise the client to eat potassium-rich foods, such as bananas, oranges, and potatoes. The nurse should also report the lab value to the prescriber, who may adjust the dose of furosemide or prescribe a potassium supplement.
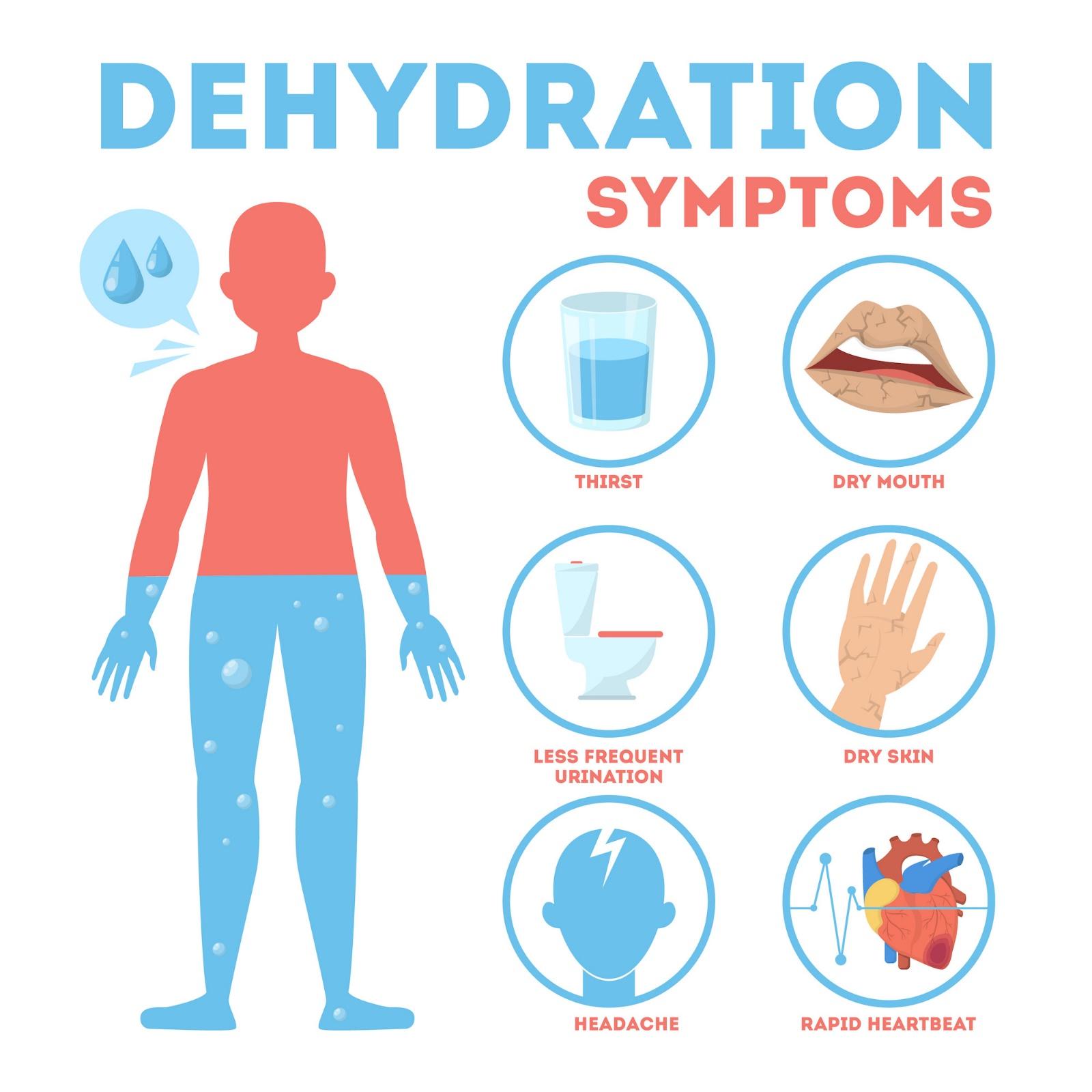
The home health nurse cares for an alert and oriented older adult patient with a history of dehydration. Which instructions should the nurse give this patient related to fluid intake?
Explanation
Choice A reason: This statement is false. Drinking more fluids in the late evening can cause nocturia, which is the need to urinate frequently at night. This can disrupt the sleep cycle and increase the risk of falls.
Choice B reason: This statement is true. Dry mouth is a sign of dehydration and indicates the need for more fluid intake. Older adults may have reduced thirst sensation and may not drink enough fluids throughout the day.
Choice C reason: This statement is false. Caffeine is a diuretic, which means it increases urine output and can worsen dehydration. Confusion is a symptom of dehydration and requires immediate medical attention.
Choice D reason: This statement is false. Feeling full is not a reliable indicator of hydration status. Older adults may have decreased appetite and gastric motility, which can make them feel full even when they are dehydrated.
A postoperative patient who had surgery for a perforated gastric ulcer has been receiving nasogastric suction for 3 days. The patient now has a serum sodium level of 127 mEq/L (127 mmol/L). Which prescribed therapy should the nurse question?
Explanation
Choice A reason: This statement is false. IV morphine sulfate is a pain medication that can be given as needed to the postoperative patient. It does not affect the serum sodium level.
Choice B reason: This statement is false. Dextrose 5% in 0.9% sodium chloride is a hypertonic solution that can be used to treat hyponatremia, or low serum sodium level. It provides both glucose and sodium to the patient.
Choice C reason: This statement is true. 5% dextrose in water is a hypotonic solution that can cause further dilution of the serum sodium level. It can worsen the hyponatremia and increase the risk of cerebral edema and seizures.
Choice D reason: This statement is false. Neurologic assessment Q2 hours is a necessary intervention for a patient with hyponatremia, as it can monitor for signs of neurologic deterioration such as confusion, lethargy, or coma.
A patient with multiple draining wounds is admitted for hypovolemia. Which assessment would be the most accurate way for the nurse to evaluate fluid balance?
Explanation
Choice A reason: This statement is false. Edema is a sign of fluid overload, not fluid deficit. Edema occurs when fluid accumulates in the interstitial space due to increased capillary hydrostatic pressure or decreased plasma oncotic pressure. Edema is more common in patients with heart failure, liver disease, or kidney disease¹.
Choice B reason: This statement is false. Skin turgor is a measure of skin elasticity and hydration. It can be affected by factors such as age, skin condition, and ambient temperature. Skin turgor is not a reliable indicator of fluid balance, as it can be normal in patients with mild to moderate hypovolemia².
Choice C reason: This statement is false. Urine output is a measure of kidney function and fluid excretion. It can be influenced by factors such as fluid intake, diuretics, hormones, and renal diseases. Urine output is not a sensitive indicator of fluid balance, as it can be normal or even increased in patients with hypovolemia due to compensatory mechanisms.
Choice D reason: This statement is true. Daily weight is a measure of body mass and fluid status. It can reflect changes in fluid balance more accurately than other methods, as long as the weight is measured at the same time, on the same scale, and with the same clothing each day. A decrease in weight can indicate fluid loss due to hypovolemia.
An older client receiving continuous tube feedings develops restlessness, agitation, and weakness. Which laboratory results are related to this finding, and should be reported to the health care provider immediately?
Explanation
Choice A reason: This statement is false. Glucose: 88 mg/dL is a normal blood sugar level and does not indicate any problem with fluid or electrolyte balance¹.
Choice B reason: This statement is false. WBCs: 4000 is slightly below the normal range, but not significantly low. It may indicate a mild infection or inflammation, but not a serious fluid or electrolyte imbalance².
Choice C reason: This statement is false. K+: 3.4 mEq/L is slightly below the normal range, but not dangerously low. It may indicate a mild potassium deficiency, which can cause muscle weakness, but not restlessness or agitation.
Choice D reason: This statement is true. Na+: 154 mEq/L is above the normal range and indicates hypernatremia, or high blood sodium level. This can cause dehydration, confusion, restlessness, agitation, and seizures. It is a medical emergency that requires immediate treatment. Continuous tube feedings can increase the risk of hypernatremia if the formula is too concentrated or the fluid intake is inadequate⁵.
Sign Up or Login to view all the 41 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
