Gestational Hypertension > Maternal & Newborn
Exam Review
Introduction
Total Questions : 5
Showing 5 questions, Sign in for moreA nurse is caring for a client who is diagnosed with gestational hypertension at 28 weeks of gestation.
Which of the following findings should alert the nurse to the possibility of preeclampsia? (Select all that apply.).
Explanation
The correct answer is choice A, B, C and E.These are all possible symptoms of preeclampsia, a condition that can occur in the second half of pregnancy and cause high blood pressure, proteinuria and organ damage.
Preeclampsia can be dangerous for both the mother and the baby if not treated promptly.
Choice D is wrong because polyuria (increased urination) is not a symptom of preeclampsia.In fact, some women with preeclampsia may have reduced urine output due to kidney damage.
Normal ranges for blood pressure during pregnancy are below 140/90 mmHg.Normal ranges for protein in urine are below 300 mg per 24 hours.Normal ranges for reflexes are 1+ to 2+ on a scale of 0 to 4.
These are all possible symptoms of preeclampsia, a condition that can occur in the second half of pregnancy and cause high blood pressure, proteinuria and organ damage.
Preeclampsia can be dangerous for both the mother and the baby if not treated promptly.
Explanation
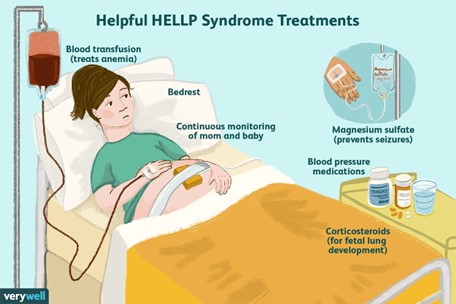
The correct answer is choice B. Platelets 80,000/mm3.This is because HELLP syndrome is a severe form of preeclampsia characterized byHemolysis,Elevated Liver enzymes, andLow Platelets.Platelets are blood cells that help with clotting, and a normal range is 150,000 to 450,000/mm3.A low platelet count (<100,000/mm3) indicates a risk of bleeding and organ damage.
Choice A is wrong because hemoglobin 12 g/dL is within the normal range for pregnant women (11 to 16 g/dL).Hemoglobin is a protein in red blood cells that carries oxygen, and hemolysis is the breakdown of red blood cells.
Choice C is wrong because AST 15 U/L is within the normal range for women (10 to 35 U/L).AST is a liver enzyme that indicates liver function, and elevated liver enzymes (>70 U/L) indicate liver damage.
Choice D is wrong because LDH 90 U/L is within the normal range for women (85 to 225 U/L).LDH is another liver enzyme that indicates liver function, and elevated LDH (>600 U/L) indicates liver damage.
A nurse is teaching a client who has gestational hypertension about the importance of bed rest.
Which of the following statements by the client indicates an understanding of the teaching?
Explanation
The correct answer is choice C.“Bed rest will help decrease the workload on my heart and improve oxygen delivery to my baby.” This is because gestational hypertension is a condition where the blood pressure is elevated after 20 weeks of pregnancy, which can affect the blood flow to the placenta and reduce the oxygen and nutrients that reach the fetus.Bed rest can help lower the blood pressure and increase the blood flow to the placenta.
Choice A is wrong because bed rest alone may not be enough to lower the blood pressure and reduce the risk of complications.Some women may need medications or hospitalization to control their blood pressure and prevent preeclampsia, a serious complication of gestational hypertension.
Choice B is wrong because bed rest does not directly affect the kidney function or prevent proteinuria, which is the presence of protein in the urine.Proteinuria is a sign of preeclampsia, not gestational hypertension.
Bed rest may help prevent the progression of gestational hypertension to preeclampsia, but it does not treat proteinuria.
Choice D is wrong because bed rest does not prevent fluid retention or reduce the swelling in the legs.
Fluid retention and swelling are common symptoms of pregnancy, not specific to gestational hypertension.They are caused by hormonal changes and increased blood volume, not by high blood pressure.
Bed rest may worsen the swelling by reducing the circulation in the legs.
A nurse is preparing to administer magnesium sulfate IV to a client who has severe preeclampsia.
Which of the following actions should the nurse take? (Select all that apply.)
Explanation
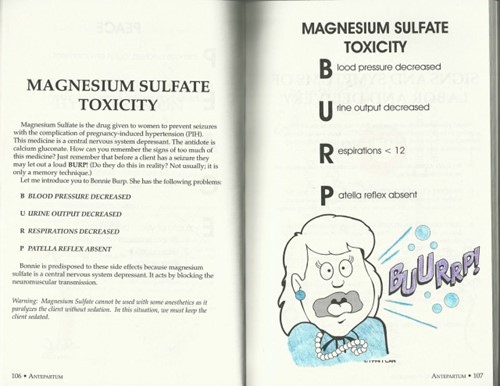
Choice A is correct because magnesium sulfate is excreted in the urine and a decreased urine output places the client at risk for magnesium toxicity.The nurse should monitor the client’s urine output hourly and report any decrease to the provider.
Choice B is wrong because hyperactive (3+ or 4+) deep tendon reflexes are a common physical finding of preeclampsia or eclampsia and do not require an action.The nurse should check the client’s deep tendon reflexes more frequently than every 4 hours to detect any signs of magnesium toxicity, such as absent or hypoactive reflexes.
Choice C is correct because calcium gluconate is the antidote for magnesium toxicity and should be readily available in case of respiratory depression, cardiac arrest, or other signs of overdose.The nurse should administer 10 mL of 10% calcium gluconate IV push over 3 to 5 minutes if needed.
Choice D is correct because magnesium sulfate should be administered via a piggyback infusion using an infusion pump to ensure accurate and safe delivery.The nurse should not administer magnesium sulfate as a bolus or through a primary IV line.
Choice E is wrong because the infusion rate of magnesium sulfate should not be titrated according to the client’s blood pressure, but according to the client’s serum magnesium level, which should range from 4 to 7 mEq/L.The nurse should notify the provider of any low or high serum magnesium level and adjust the infusion rate accordingly.The nurse should also administer antihypertensive medications other than magnesium for sustained hypertension.
Normal ranges:
• Urine output: at least 30 mL/hour
• Deep tendon reflexes: 1+ or 2+
• Respiratory rate: 12 to 20 breaths/minute
• Serum magnesium level: 4 to 7 mEq/L
• Blood pressure: less than 140/90 mm Hg

A nurse is assessing a client who has eclampsia and is receiving magnesium sulfate IV.
Which of the following findings should indicate to the nurse that the client is experiencing magnesium toxicity?
Explanation
The correct answer is choice A. Respiratory rate of 10/min.This indicates that the client is experiencingmagnesium toxicity, which can causemuscle weakness,lethargy, andrespiratory depression.
Magnesium sulfate is a medication used to prevent seizures in clients with eclampsia, but it can also have adverse effects if the dose is too high or the kidney function is impaired.
Choice B. Urine output of 40 mL/hr is wrong because this is within the normal range for urine output.
The minimum urine output should be at least 30 mL/hr.
Choice C. Serum magnesium level of 6 mg/dL is wrong because this is within the normal range for serum magnesium.The normal range is 1.7–2.3 mg/dL.
Choice D. Patellar reflex 2+ is wrong because this is a normal finding for deep tendon reflexes.
A decreased or absent patellar reflex could indicate magnesium toxicity, as magnesium sulfate
Sign Up or Login to view all the 5 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
