Ivytech Community College Med Surg Final Exam
Total Questions : 32
Showing 25 questions, Sign in for moreA nurse is preparing to initiate intravenous (IV) antibiotic therapy for a newly admitted 12-month-old infant. Which of the following actions should the nurse plan to take?
Explanation
Choice A reason: A 24-gauge catheter is appropriate for a small and fragile vein of a 12-month-old infant. It minimizes the risk of damaging the vein and ensures the comfort of the infant during IV therapy.
Choice B reason: Starting an IV in the infant's foot is not the first choice due to the risk of movement dislodging the catheter. The hand or the antecubital fossa are preferred sites for IV insertion in infants.
Choice C reason: While it is important to cover the IV insertion site, an opaque dressing is not necessary. A transparent dressing is preferred as it allows for continuous visibility of the site for signs of infection or phlebitis.
Choice D reason: The IV site should not be routinely changed every 3 days. It should be changed based on clinical indications such as signs of infection, infiltration, or phlebitis, or if the IV becomes dislodged.

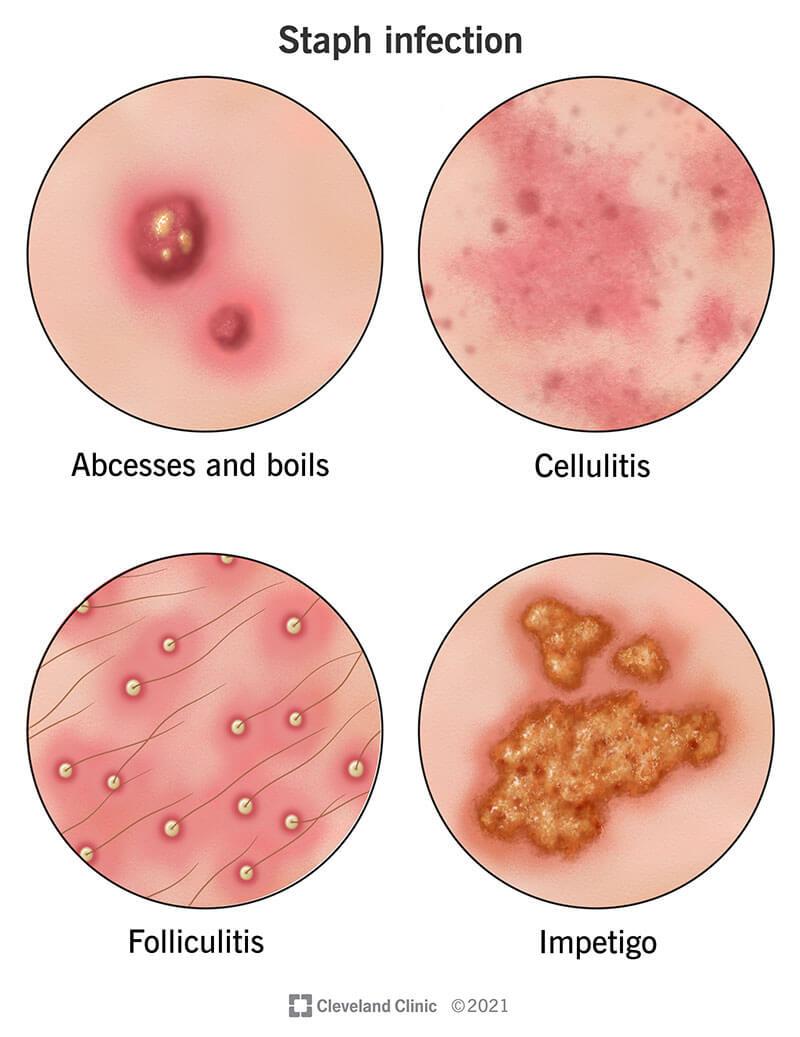
The student nurse is preparing a presentation on parasitic skin infestations. What should the student include in the presentation?
Explanation
Choice A reason: Rosacea is not a parasitic skin infestation, but a chronic inflammatory skin condition that causes redness, flushing, and bumps on the face.
Choice B reason: Pediculosis corporis is a parasitic skin infestation caused by body lice, but it is not the only one. The question asks for what the student should include in the presentation, not what is the most common or severe type of parasitic skin infestation.
Choice C reason: Sarcoptes scabiei is a parasitic skin infestation caused by scabies mites, which burrow into the skin and cause intense itching, rash, and secondary infections. This is a correct choice to include in the presentation, as scabies is a common and contagious condition that affects people of all ages and backgrounds.
Choice D reason: Furuncles are not a parasitic skin infestation, but a bacterial infection of the hair follicles that causes painful, pus-filled boils on the skin.
Choice E reason: Impetigo is not a parasitic skin infestation, but a bacterial infection of the skin that causes red, oozing, and crusted sores.
A nurse in a busy emergency department provides care for many clients who present with contusions, strains, or sprains. Treatment modalities that are common to all of these musculoskeletal injuries include which of the following?
Explanation
Choice A reason: Corticosteroids are not a common treatment modality for contusions, strains, or sprains. They are anti-inflammatory drugs that may be used for chronic conditions such as arthritis, asthma, or allergies, but they have side effects such as weakening the immune system, increasing the risk of infection, and delaying wound healing.
Choice B reason: Resting the affected extremity is a common treatment modality for contusions, strains, or sprains. It helps to reduce pain, swelling, and inflammation, and to prevent further injury or damage to the tissues.
Choice C reason: Applying ice is a common treatment modality for contusions, strains, or sprains, but only for the first 24 to 48 hours after the injury. It helps to reduce pain, swelling, and inflammation by constricting the blood vessels and decreasing the blood flow to the injured area. After 48 hours, heat may be applied to increase the blood flow and promote healing.
Choice D reason: Massage is not a common treatment modality for contusions, strains, or sprains. It may be beneficial for some chronic musculoskeletal conditions, but it should be avoided for acute injuries as it may increase the pain, swelling, and inflammation by stimulating the blood flow and aggravating the damaged tissues.
Choice E reason: Compression dressings are a common treatment modality for contusions, strains, or sprains. They help to reduce pain, swelling, and inflammation by applying pressure to the injured area and limiting the movement of the tissues. They also provide support and stability to the affected extremity.
A nurse is caring for a 78-year-old obese client with a history of osteoarthritis. When planning the client's care, what goals should the nurse include?
Explanation
Choice A reason: Pain management is an important goal for a client with osteoarthritis, but it is not the only one. The question asks for what goals the nurse should include, not what is the most essential or urgent goal.
Choice B reason: Improvement of joint mobility is a correct goal for a client with osteoarthritis, as it helps to prevent stiffness, contractures, and deformities of the affected joints. It also improves the client's function, quality of life, and independence.
Choice C reason: Client will recover from osteoarthritis within 6 months is not a realistic or attainable goal, as osteoarthritis is a chronic and progressive condition that has no cure. The nurse should focus on managing the symptoms and preventing complications, not on curing the disease.
Choice D reason: Weight loss promotion is a relevant goal for a client with osteoarthritis, especially if the client is obese, as it helps to reduce the stress and pressure on the weight-bearing joints. However, it is not a specific or measurable goal, as it does not indicate how much weight the client should lose or how the nurse will monitor the progress.
Choice E reason: The client will deny symptoms of osteoarthritis is not a desirable or appropriate goal, as it implies that the client is not honest or aware of their condition. The nurse should encourage the client to report any symptoms or changes in their joints, as it helps to assess the effectiveness of the treatment and to adjust the plan of care accordingly.
A nurse is caring for a client who has been diagnosed with psoriasis. The nurse is creating an education plan for the client. What information should be included in this plan?
Explanation
Choice A reason: Pain management is not a key information to include in the education plan for a client with psoriasis, as psoriasis is not usually a painful condition. It may cause itching, burning, or soreness, but these are not severe enough to require pain medication.
Choice B reason: Watching skin every hour to prevent infection is not a realistic or necessary information to include in the education plan for a client with psoriasis, as psoriasis is not an infectious condition. It is an autoimmune disorder that causes the skin cells to grow faster than normal, resulting in thick, scaly, red patches on the skin.
Choice C reason: Avoiding public places until symptoms subside is not a helpful or appropriate information to include in the education plan for a client with psoriasis, as psoriasis is not a contagious condition. It does not pose a risk to others, and isolating oneself may worsen the client's mental and emotional health.
Choice D reason: Antifungal ointment will not be part of the long-term management for a client with psoriasis, as psoriasis is not a fungal infection. It is an immune-mediated condition that requires different types of treatments, such as topical steroids, vitamin D analogues, phototherapy, or biologics.
Choice E reason: Moisturizing skin regularly and avoiding triggers is a correct information to include in the education plan for a client with psoriasis, as it helps to reduce the dryness, scaling, and inflammation of the skin. Triggers may vary from person to person, but some common ones are stress, infections, cold weather, alcohol, smoking, or certain medications.

A client has been diagnosed with herpes zoster present on the upper right side of the torso, extending around to the client's back. Which client statement indicates the need for further teaching regarding this diagnosis?
Explanation
Choice A reason: This statement indicates the need for further teaching, as it shows that the client does not understand the possible complication of postherpetic neuralgia, which is a chronic pain condition that can persist for months or years after the rash heals. The nurse should explain to the client that some people may experience this condition and that there are treatments available to manage the pain.
Choice B reason: This statement does not indicate the need for further teaching, as it shows that the client understands the importance of preventing the transmission of the virus to others, especially those who have not had chicken pox or the vaccine. The nurse should reinforce this behavior and remind the client to cover the rash with a dressing and avoid contact with pregnant women, newborns, and immunocompromised people.
Choice C reason: This statement does not indicate the need for further teaching, as it shows that the client knows the etiology of the infection. The nurse should confirm that the client is correct and explain that the virus remains dormant in the nerve cells after the initial infection and can reactivate later in life due to stress, aging, or other factors.
Choice D reason: This statement does not indicate the need for further teaching, as it shows that the client recognizes the prodromal symptom of the infection. The nurse should acknowledge that the client is correct and explain that the pain is caused by the inflammation of the nerve fibers where the virus resides. The nurse should also ask the client about the severity and frequency of the pain and provide appropriate interventions.
The nurse is providing care for a client who has just been diagnosed with peripheral arterial occlusive disease (PAD). What assessment finding is most consistent with this diagnosis?
Explanation
Choice A reason: Visible clubbing of the fingers and toes is not a typical finding of PAD, but a sign of chronic hypoxia or lung disease. It refers to the enlargement and rounding of the nail beds due to increased blood flow to the distal tissues.
Choice B reason: Stasis ulcer on the lower leg is not a common finding of PAD, but a sign of venous insufficiency or chronic venous stasis. It refers to the breakdown of the skin due to poor venous drainage and increased pressure in the veins.
Choice C reason: Unequal peripheral pulses between the lower extremities is not a specific finding of PAD, but a sign of arterial obstruction or aneurysm. It refers to the difference in the strength or quality of the pulses palpated in the arteries of the legs.
Choice D reason: Pale edematous extremities is not a characteristic finding of PAD, but a sign of heart failure or lymphedema. It refers to the pallor and swelling of the limbs due to fluid accumulation in the interstitial spaces.
Choice E reason: Intermittent claudication is a classic finding of PAD, as it indicates the reduced blood flow and oxygen delivery to the muscles of the legs. It refers to the pain, cramping, or fatigue that occurs in the calves, thighs, or buttocks during exercise and is relieved by rest.
A client comes to the clinic reporting a red rash of small, fluid-filled blisters and is suspected of having shingles. What presentation is most consistent with this diagnosis?
Explanation
Choice A reason: Grouped vesicles on the genitalia are not a typical presentation of shingles, but a sign of genital herpes, which is a sexually transmitted infection caused by a different type of herpes virus.
Choice B reason: Hematoma on upper right arm is not a common presentation of shingles, but a sign of bleeding or bruising under the skin, which may be caused by trauma, injury, or coagulation disorders.
Choice C reason: Group of vesicles in linear patches along the spinal nerves is a classic presentation of shingles, as it indicates the reactivation of the varicella-zoster virus, which causes chickenpox in childhood and remains dormant in the nerve cells. The virus can cause a painful rash that follows the distribution of the affected nerves, usually on one side of the body.
Choice D reason: Group of vesicles occurring on the lips and oral mucous membranes are not a characteristic presentation of shingles, but a sign of oral herpes, which is a common infection caused by a different type of herpes virus.
Choice E reason: None of the above is not a correct choice, as there is one option that matches the presentation of shingles
Upon assessment of a newly admitted client, the nurse finds warmth, redness, edema, and tenderness to the left arm following mastectomy surgery 2 weeks ago. What might these assessment findings indicate?
Explanation
Choice A reason: Atopic dermatitis is not a likely explanation for the assessment findings, as it is a chronic inflammatory skin condition that causes itching, scaling, and dryness of the skin, usually on the face, neck, and flexural areas.
Choice B reason: Cellulitis is a possible explanation for the assessment findings, as it is a bacterial infection of the skin and subcutaneous tissues that causes warmth, redness, swelling, and pain of the affected area. However, it is not the most likely explanation, as it usually occurs as a result of a break in the skin, such as a wound, insect bite, or ulcer, which is not mentioned in the scenario.
Choice C reason: Seborrheic keratosis is not a relevant explanation for the assessment findings, as it is a benign skin growth that causes brown, black, or tan lesions that have a waxy or scaly appearance, usually on the face, chest, or back.
Choice D reason: Pemphigus is not a plausible explanation for the assessment findings, as it is a rare autoimmune disorder that causes blisters and erosions of the skin and mucous membranes, usually on the trunk, scalp, or mouth.
Choice E reason: Lymphedema is the most likely explanation for the assessment findings, as it is a condition that causes swelling of the arm due to impaired lymphatic drainage after mastectomy surgery. It can also cause warmth, redness, and tenderness of the affected limb.
A client with a recent diagnosis of scabies will need what education?
Explanation
Choice A reason: Scabies can be cured with prescription medications that kill the mites and their eggs, such as permethrin cream or ivermectin pills. Steroid cream may help to reduce the itching and inflammation, but it does not eliminate the infection.
Choice B reason: Treatment should start as soon as possible after the diagnosis of scabies, but there is no specific time limit of 72 hours. The sooner the treatment begins, the faster the symptoms will improve and the risk of transmission will decrease.
Choice C reason: Washing clothes, towels, and sheets in hot water is an important part of the education for a client with scabies, as it helps to get rid of any mites or eggs that may have been transferred to the fabrics. The items should also be dried in a hot dryer or sealed in a plastic bag for at least 72 hours.
Choice D reason: Reducing intake of refined sugar has no effect on the risk of scabies, as scabies is not caused by dietary factors, but by a parasitic infestation of the skin by the Sarcoptes scabiei mite. The mite is transmitted by direct skin-to-skin contact or by sharing personal items with an infected person.
Choice E reason: Avoiding close contact with others until treated is another key part of the education for a client with scabies, as it helps to prevent the spread of the infection to other people. The client should also inform their household members, sexual partners, and close contacts, as they may need to be treated as well.
A client presents to a clinic complaining of a leg ulcer that isn't healing; subsequent diagnostic testing suggests osteomyelitis. The nurse is aware the most common pathogen to cause osteomyelitis is which pathogen?
Explanation
Choice A reason: Staphylococcus aureus is the most common pathogen to cause osteomyelitis, as it is a gram-positive bacterium that can invade the bone through the bloodstream, a wound, or a surgical site. It can cause acute or chronic inflammation and infection of the bone and bone marrow.
Choice B reason: Escherichia coli is not the most common pathogen to cause osteomyelitis, as it is a gram-negative bacterium that is usually found in the gastrointestinal tract. It can cause urinary tract infections, diarrhea, or sepsis, but it is not a frequent cause of bone infections.
Choice C reason: Proteus mirabilis is not the most common pathogen to cause osteomyelitis, as it is a gram-negative bacterium that is usually found in the urinary tract. It can cause urinary tract infections, kidney stones, or septicemia, but it is not a common cause of bone infections.
Choice D reason: Pseudomonas aeruginosa is not the most common pathogen to cause osteomyelitis, as it is a gram-negative bacterium that is usually found in moist environments. It can cause skin infections, pneumonia, or septic shock, but it is not a frequent cause of bone infections.
Choice E reason: None of the above is not a correct choice, as there is one option that matches the most common pathogen to cause osteomyelitis.
A client with severe osteoarthritis has been treated with total hip replacement. Which intervention will the nurse implement to help protect against the risk for deep venous thrombosis (DVT)?
Explanation
Choice A reason: Use of sequential compression devices (SCDs) during times of rest is a helpful intervention to prevent DVT, as it improves the venous return and reduces the stasis of blood in the lower extremities. However, it is not the only or the most effective intervention, as it does not promote the active contraction of the leg muscles.
Choice B reason: Use of abductor pillow while in bed is a necessary intervention to prevent hip dislocation after total hip replacement, as it maintains the alignment and stability of the hip joint. However, it is not a specific intervention to prevent DVT, as it does not enhance the blood circulation or prevent the formation of clots.
Choice C reason: Keeping the heels elevated is a useful intervention to prevent pressure ulcers on the heels, as it reduces the friction and shear forces on the skin. However, it is not a relevant intervention to prevent DVT, as it does not affect the venous flow or prevent the clotting of blood.
Choice D reason: Opioid pain medications as ordered are an important intervention to manage the postoperative pain after total hip replacement, as they provide analgesia and sedation. However, they are not a direct intervention to prevent DVT, as they do not influence the blood coagulation or prevent the thrombus formation. In fact, they may increase the risk of DVT by causing respiratory depression, hypotension, and immobility.
Choice E reason: Early ambulation and leg exercises are the most effective interventions to prevent DVT, as they stimulate the contraction of the leg muscles and improve the blood flow in the veins. They also prevent the pooling and clotting of blood in the lower extremities.
A nurse is providing a class on osteoporosis at the local seniors' center. Which statement related to osteoporosis is most accurate?
Explanation
Choice A reason: Excess growth of bone formation does not cause the bones to weaken, but rather the opposite. Osteoporosis is a condition that causes the bones to lose density and become brittle due to the imbalance between bone resorption and formation. The bone resorption exceeds the bone formation, leading to low bone mass and increased fracture risk.
Choice B reason: Men are not less likely than women to have secondary causes of osteoporosis, but rather more likely. Secondary osteoporosis is a type of osteoporosis that is caused by other diseases or medications that affect the bone metabolism. Men are more likely to have secondary osteoporosis due to conditions such as hypogonadism, hyperparathyroidism, hyperthyroidism, or chronic kidney disease, or medications such as glucocorticoids, anticonvulsants, or anticoagulants.
Choice C reason: A modifiable risk factor for osteoporosis is a person's level of activity, as it affects the bone health and strength. Physical activity, especially weight-bearing and resistance exercises, can stimulate the bone formation and prevent the bone loss. It can also improve the muscle strength, balance, and coordination, which can reduce the risk of falls and fractures.
Choice D reason: Osteoporosis is not categorized as a disease for the elderly, but rather a disease that can affect people of any age. Osteoporosis is more common in older adults, especially postmenopausal women, due to the hormonal changes and the natural decline of bone mass with aging. However, osteoporosis can also occur in younger people due to genetic factors, lifestyle factors, or secondary causes.
Choice E reason: None of the above is not a correct choice, as there is one option that matches the most accurate statement related to osteoporosis.
A client with a new right leg cast is complaining of increasing pain in that injured extremity. The nurse has administered analgesics and elevated the limb. Thirty minutes after administering the analgesics, the client states the pain is unrelieved. The nurse should recognize the warning signs of what complication?
Explanation
Choice A reason: Fat embolism is not a likely complication of a leg cast, but a possible complication of a long bone fracture or a joint replacement surgery. It refers to the obstruction of the blood vessels by fat globules that are released from the bone marrow or adipose tissue. It can cause respiratory distress, neurological impairment, or skin petechiae.
Choice B reason: Subcutaneous emphysema is not a common complication of a leg cast, but a rare complication of a chest trauma or a lung disease. It refers to the presence of air or gas in the subcutaneous tissue, which can cause swelling, crepitus, or pain in the affected area.
Choice C reason: Disuse syndrome is not an acute complication of a leg cast, but a chronic complication of prolonged immobility or inactivity. It refers to the deterioration of the body systems due to the lack of physical stimulation. It can cause muscle atrophy, joint stiffness, osteoporosis, or metabolic changes.
Choice D reason: Compartment syndrome is the most likely complication of a leg cast, as it indicates the increased pressure within the muscle compartments of the leg due to the swelling, bleeding, or inflammation. It can cause severe pain, pallor, paresthesia, paralysis, or pulselessness of the affected limb. It is a medical emergency that requires prompt intervention to prevent tissue necrosis or limb loss.
Choice E reason: None of the above is not a correct choice, as there is one option that matches the complication of a leg cast.
The nursing care plan for a client in traction includes regular assessments for venous thromboembolism. When assessing a client's lower limbs, what sign or symptom is suggestive of deep vein thrombosis (DVT)?
Explanation
Choice A reason: Increased circulation of the calf is not a sign or symptom of DVT, but a normal finding of the blood flow in the leg. It can be assessed by palpating the pulses, checking the capillary refill, or observing the skin color and temperature.
Choice B reason: Pale-appearing calf is not a sign or symptom of DVT, but a sign of arterial insufficiency or ischemia. It indicates the reduced blood supply and oxygen delivery to the tissues, which can cause pain, numbness, or coldness of the leg.
Choice C reason: Increased warmth in the calf is not a specific sign or symptom of DVT, but a possible sign of inflammation or infection. It may be accompanied by redness, swelling, or fever, which can indicate a local or systemic inflammatory response.
Choice D reason: Loss of sensation to the calf is not a sign or symptom of DVT, but a sign of nerve damage or compression. It may be caused by trauma, injury, diabetes, or other conditions that affect the peripheral nervous system.
Choice E reason: Swelling and tenderness of the calf is a common sign or symptom of DVT, as it indicates the presence of a blood clot in the deep veins of the leg. It may also cause pain, cramping, or heaviness of the leg, which can worsen with movement or standing.
A nurse is reviewing a client's activities of daily living prior to discharge from total hip replacement. The nurse should identify what activity as posing a potential risk for hip dislocation?
Explanation
Choice A reason: Transferring from sitting to standing position is not a high-risk activity for hip dislocation, as long as the client follows the proper precautions, such as keeping the operated leg slightly forward, using a chair with armrests, and avoiding twisting or pivoting the hip.
Choice B reason: Straining during a bowel movement is not a direct risk factor for hip dislocation, but it may cause constipation, which is a common problem after surgery. The nurse should educate the client on the importance of adequate hydration, fiber intake, and stool softeners to prevent constipation and reduce the need for straining.
Choice C reason: Bending down to put socks on is a risky activity for hip dislocation, as it violates the hip precautions of avoiding flexing the hip more than 90 degrees, adducting the hip, or internally rotating the hip. The nurse should instruct the client to use assistive devices, such as a sock aid or a long-handled reacher, to put on socks or shoes without bending the hip.
Choice D reason: Turning in bed with an abductor pillow in place is a safe activity for hip dislocation, as the abductor pillow helps to maintain the alignment and stability of the hip joint. The nurse should teach the client to use the abductor pillow while in bed for the first few weeks after surgery, and to turn from side to side with the assistance of a caregiver.
Choice E reason: Crossing the legs or ankles is a dangerous activity for hip dislocation, as it causes the hip to move out of its normal position. The nurse should remind the client to keep the legs apart at all times, and to use a pillow or a wedge between the legs when lying on the side.
The nurse would prioritize which assessment for a client with a new diagnosis of osteoarthritis?
Explanation
Choice A reason: Diet is not a priority assessment for a client with osteoarthritis, as it is not a direct cause or consequence of the condition. However, diet may play a role in the management of osteoarthritis, as it can affect the body weight, inflammation, and nutrition of the client.
Choice B reason: Skin surrounding the affected joint is not a priority assessment for a client with osteoarthritis, as it is not a common or serious complication of the condition. However, skin may be affected by the use of heat or cold therapy, topical medications, or joint braces, which may cause irritation, dryness, or infection.
Choice C reason: Pain is a priority assessment for a client with osteoarthritis, as it is the main symptom and the most distressing aspect of the condition. Pain can affect the client's quality of life, mobility, function, and mood. The nurse should assess the location, intensity, frequency, duration, and aggravating or relieving factors of the pain, and provide appropriate interventions to relieve the pain.
Choice D reason: Capillary refill of affected extremity is not a priority assessment for a client with osteoarthritis, as it is not a typical or significant finding of the condition. However, capillary refill may be affected by the circulation, temperature, or hydration of the client, which may influence the healing and recovery of the joint.
Choice E reason: Range of motion of affected joint is not a priority assessment for a client with osteoarthritis, but an important assessment to evaluate the function and mobility of the joint. Osteoarthritis can cause stiffness, swelling, and deformity of the joint, which can limit the range of motion and impair the activities of daily living. The nurse should assess the active and passive range of motion of the joint, and encourage the client to perform regular exercises to maintain the joint health.
A client with a total hip replacement is progressing well and expects to be discharged tomorrow. On returning to bed after ambulating, he complains of a new onset of pain at the surgical site. What is the nurse's best action?
Explanation
Choice A reason: Administering pain medication as ordered is not the best action, as it does not address the cause of the new onset of pain. The nurse should first assess the client and the surgical site to rule out any complications or problems that may require immediate intervention.
Choice B reason: Assessing the client for signs and symptoms of systemic infection is not the best action, as it is not the most likely cause of the new onset of pain. Systemic infection would manifest with fever, chills, malaise, or leukocytosis, which are not mentioned in the scenario. The nurse should focus on the local signs and symptoms of the surgical site and the affected extremity.
Choice C reason: Assessing the surgical site and the affected extremity is the best action, as it allows the nurse to identify any potential complications or problems that may explain the new onset of pain. The nurse should look for signs of infection, inflammation, bleeding, hematoma, or dislocation of the hip prosthesis, such as redness, swelling, warmth, drainage, bruising, or deformity.
Choice D reason: Reassuring the client that pain is a direct result of increased activity is not the best action, as it may dismiss the client's concern and delay the detection of any serious complications or problems. The nurse should not assume that the pain is normal or expected, but rather investigate the cause and severity of the pain.
Choice E reason: Notifying the surgeon immediately is not the best action, as it is premature and unnecessary without first assessing the client and the surgical site. The nurse should gather relevant data and information before contacting the surgeon, unless there is an obvious or urgent problem that requires immediate attention.
A nurse is providing discharge education to a client who is going home with a cast on his leg. What teaching point would be appropriate for the nurse to emphasize in the teaching session?
Explanation
Choice A reason: Reporting any pain that is uncontrolled by elevating the affected limb or by analgesic agents is an appropriate teaching point for the nurse to emphasize, as it may indicate a serious complication such as compartment syndrome, infection, or nerve damage. The nurse should instruct the client to notify the health care provider immediately if the pain persists or worsens.
Choice B reason: Using intermittent heat packs as prescribed to control swelling is not an appropriate teaching point for the nurse to emphasize, as it may increase the blood flow and inflammation in the affected area. The nurse should advise the client to avoid heat sources such as heating pads, hot water bottles, or electric blankets, as they may also damage the cast or cause burns.
Choice C reason: Using a small hair brush to control any itching under the cast is not an appropriate teaching point for the nurse to emphasize, as it may cause skin irritation, infection, or damage to the cast. The nurse should suggest the client to use a cool air dryer, a gentle tapping, or an antihistamine to relieve the itching, and to avoid inserting any objects under the cast.
Choice D reason: Keeping the affected extremity below the level of the heart to prevent swelling is not an appropriate teaching point for the nurse to emphasize, as it may impair the venous return and increase the edema. The nurse should recommend the client to elevate the affected extremity above the level of the heart to reduce the swelling and promote the healing.
Choice E reason: Inspecting the cast daily for cracks, breaks, or signs of infection is not an appropriate teaching point for the nurse to emphasize, as it is not a specific or relevant instruction for the client with a cast on his leg. The nurse should teach the client to keep the cast dry and clean, to cover it with a plastic bag when showering or bathing, and to report any foul odor, drainage, or fever.
The medical-surgical nurse is caring for a client postoperatively after a total hip arthroplasty. The nurse is calculating the client's intake and output and notes a total of 100 mL of sanguineous drainage out of the hip drain in the 24 hours since surgery. What is the most appropriate action for the nurse to take?
Explanation
Choice A reason: Removing the drain is not an appropriate action for the nurse to take, as it may cause bleeding, infection, or hematoma at the surgical site. The drain is placed to prevent the accumulation of fluid and blood in the hip joint, and it should be removed only by the surgeon when the drainage is minimal and the wound is healing.
Choice B reason: Continuing to assess and monitor intake and output every shift is an appropriate action for the nurse to take, as it helps to evaluate the fluid balance and the renal function of the client. The nurse should record the amount, color, and consistency of the drainage, and compare it with the previous measurements. The nurse should also monitor the vital signs, the hemoglobin and hematocrit levels, and the signs of dehydration or fluid overload.
Choice C reason: Elevating the affected leg and placing the client in Trendelenburg position is not an appropriate action for the nurse to take, as it may cause hip dislocation, hypotension, or respiratory distress. The nurse should keep the affected leg slightly abducted and aligned with the body, and avoid flexing the hip more than 90 degrees. The nurse should also maintain the client in a semi-Fowler's or supine position, and avoid turning the client to the affected side.
Choice D reason: Notifying the surgeon and making aware of this finding is not an appropriate action for the nurse to take, as it is not an urgent or abnormal situation. The nurse should report the drainage to the surgeon only if it exceeds the expected amount, which is usually less than 200 mL in the first 24 hours after surgery, or if it changes in color, consistency, or odor.
Choice E reason: None of the above is not a correct choice, as there is one option that matches the most appropriate action for the nurse to take.
When providing care to a client in skeletal traction, what action would be included in the nurse's plan of care?
Explanation
Choice A reason: Providing cast care to bilateral lower extremities is not an action that would be included in the nurse's plan of care for a client in skeletal traction, as it is not relevant to the type of traction. Skeletal traction involves the insertion of pins, wires, or screws into the bone, and does not require a cast. Cast care is more applicable to clients in plaster or fiberglass casts.
Choice B reason: Instituting measures to prevent skin breakdown is an action that would be included in the nurse's plan of care for a client in skeletal traction, as it is a potential complication of prolonged immobilization and pressure. The nurse should inspect the skin regularly, change the bed linens frequently, use pressure-relieving devices, and encourage the client to shift positions as much as possible.
Choice C reason: Cleaning the pins every hour with peroxide to prevent infection is not an action that would be included in the nurse's plan of care for a client in skeletal traction, as it is excessive and harmful. The nurse should follow the facility's protocol for pin site care, which usually involves cleaning the pins once or twice a day with a mild antiseptic solution, such as chlorhexidine or saline. Peroxide is not recommended, as it can damage the tissue and delay the healing.
Choice D reason: Placing the client on contact precautions is not an action that would be included in the nurse's plan of care for a client in skeletal traction, as it is not indicated for this type of traction. Contact precautions are used for clients who have infections that can be transmitted by direct or indirect contact, such as MRSA, VRE, or C. difficile. Skeletal traction does not pose a high risk of infection, unless there is a pin site infection or osteomyelitis.
Choice E reason: Maintaining proper alignment and position of the traction is an action that would be included in the nurse's plan of care for a client in skeletal traction, as it is essential for the effectiveness and safety of the traction. The nurse should ensure that the traction is applied correctly, that the weights are hanging freely, that the ropes are not twisted or frayed, and that the pulleys are not obstructed. The nurse should also avoid lifting or moving the weights, as it can alter the traction force and cause complications.
The nurse is assessing a group of clients. Which client is most at risk for developing osteoporosis?
Explanation
Choice A reason: Males with a cardiac history between the ages of 30 and 40 years old are not the most at risk for developing osteoporosis, as they have several protective factors, such as their gender, age, and hormone levels. Males have higher peak bone mass and lower bone loss rate than females, and they do not experience the rapid decline of estrogen that occurs after menopause. Cardiac history may affect the bone health indirectly, by limiting the physical activity or affecting the calcium absorption, but it is not a major risk factor.
Choice B reason: Females with a history of diabetes and are between the ages of 20 and 30 years old are not the most at risk for developing osteoporosis, as they have some protective factors, such as their age and hormone levels. Females in their reproductive years have higher estrogen levels than post-menopausal females, which helps to preserve the bone density and prevent the bone resorption. Diabetes may increase the risk of osteoporosis, by affecting the insulin, glucose, and inflammatory pathways, but it is not a definitive risk factor.
Choice C reason: Males who have had a previous fracture are not the most at risk for developing osteoporosis, as they have some protective factors, such as their gender and hormone levels. Males have higher peak bone mass and lower bone loss rate than females, and they do not experience the rapid decline of estrogen that occurs after menopause. A previous fracture may indicate a low bone density or a high fall risk, but it is not a conclusive risk factor.
Choice D reason: Females who have a history of estrogen deficiency and are post-menopausal are the most at risk for developing osteoporosis, as they have several risk factors, such as their gender, age, and hormone levels. Females have lower peak bone mass and higher bone loss rate than males, and they experience a significant drop of estrogen after menopause, which leads to increased bone resorption and decreased bone formation. Estrogen deficiency may also cause other symptoms, such as hot flashes, mood swings, or vaginal dryness, which may affect the quality of life and the bone health.
A student is reviewing a client's medications for osteoporosis. Which medication(s) will have the least effect in increasing the client's bone mass?
Explanation
Choice A reason: Calcitriol (Fortica) is not the medication that will have the least effect in increasing the client's bone mass, as it is a synthetic form of vitamin D that helps the body absorb calcium and phosphorus, which are essential for bone health. Calcitriol also regulates the bone remodeling and prevents the bone resorption.
Choice B reason: Calcium (Caltrate) with Vitamin D (Caltria) is not the medication that will have the least effect in increasing the client's bone mass, as it is a combination of calcium and vitamin D that works synergistically to enhance the bone density and strength. Calcium is the main mineral component of the bone, and vitamin D helps the body absorb calcium and phosphorus.
Choice C reason: Alendronate (Fosamax) is not the medication that will have the least effect in increasing the client's bone mass, as it is a bisphosphonate that inhibits the activity of osteoclasts, which are the cells that break down the bone. Alendronate reduces the bone loss and increases the bone mass, and it is used to treat and prevent osteoporosis.
Choice D reason: Calcium (Caltrate) without Vitamin D (Calcio) is the medication that will have the least effect in increasing the client's bone mass, as it is a calcium supplement that does not contain vitamin D, which is necessary for the calcium absorption and utilization. Calcium alone may not be sufficient to prevent or treat osteoporosis, and it may also cause side effects such as constipation, kidney stones, or hypercalcemia.
Choice E reason: None of the above is not a correct choice, as there is one option that matches the medication that will have the least effect in increasing the client's bone mass.
A nurse is preparing to educate a client at risk for developing osteoporosis on the importance of increasing calcium in the diet. Which are the best foods to include in the teaching plan when educating a client on increased calcium intake?
Explanation
Choice A reason: Green vegetables, whole wheat pasta, and poultry are not the best foods to include in the teaching plan when educating a client on increased calcium intake, as they are not rich sources of calcium. Green vegetables, such as kale, spinach, or broccoli, contain some calcium, but they also have oxalates, which can reduce the calcium absorption. Whole wheat pasta and poultry have very little calcium, and they are more sources of carbohydrates and protein, respectively.
Choice B reason: Low-fat milk, salmon with bones, and yogurt are the best foods to include in the teaching plan when educating a client on increased calcium intake, as they are high sources of calcium. Low-fat milk has about 300 mg of calcium per cup, salmon with bones has about 200 mg of calcium per 3 ounces, and yogurt has about 450 mg of calcium per cup. These foods also provide other nutrients, such as protein, vitamin D, and omega-3 fatty acids, which are beneficial for bone health.
Choice C reason: Fish, eggs, and potatoes are not the best foods to include in the teaching plan when educating a client on increased calcium intake, as they are not rich sources of calcium. Fish, such as tuna, cod, or halibut, have some calcium, but only if they are eaten with bones, which is not common. Eggs have about 25 mg of calcium per egg, which is very low. Potatoes have about 20 mg of calcium per medium potato, which is also very low.
Choice D reason: Poultry, broccoli, and yellow vegetables are not the best foods to include in the teaching plan when educating a client on increased calcium intake, as they are not rich sources of calcium. Poultry, such as chicken, turkey, or duck, have very little calcium, and they are more sources of protein and iron. Broccoli has about 40 mg of calcium per cup, which is low. Yellow vegetables, such as carrots, squash, or corn, have very little or no calcium, and they are more sources of vitamin A and fiber.
Choice E reason: Cheese, almonds, and tofu are not the best foods to include in the teaching plan when educating a client on increased calcium intake, as they are not suitable for everyone. Cheese has about 200 mg of calcium per ounce, but it is also high in fat, sodium, and calories, which may not be good for clients with high blood pressure, high cholesterol, or obesity. Almonds have about 75 mg of calcium per ounce, but they are also high in calories, and they may cause allergic reactions in some people. Tofu has about 250 mg of calcium per half cup, but it is also high in phytoestrogens, which may interfere with hormone levels in some people.
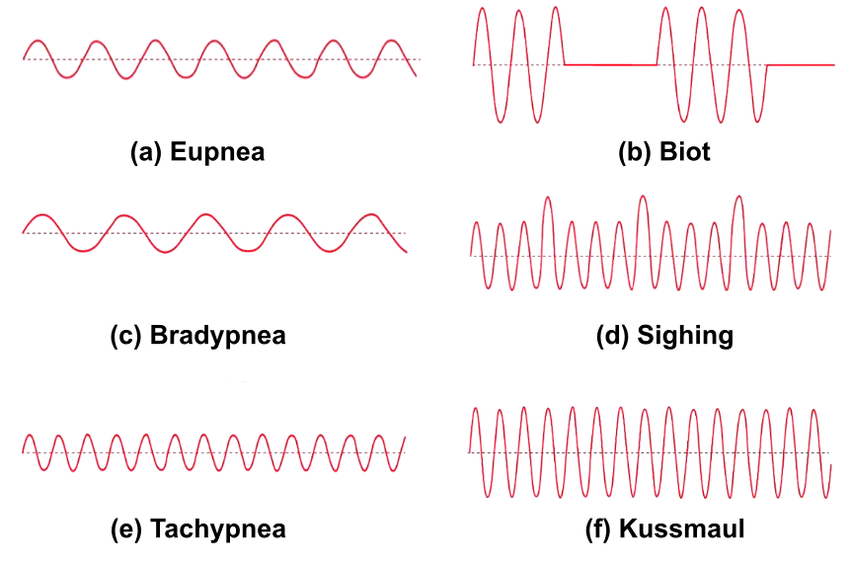
The nurse is caring for a client with a fracture of the right humerus. Which assessment finding could be an early sign of a fat embolus?
Explanation
Choice A reason: Heat rash is not an early sign of a fat embolus, as it is a skin condition that occurs when the sweat ducts are blocked and the sweat cannot evaporate. Heat rash is more common in hot and humid environments, and it causes red, itchy, or prickly bumps on the skin. Heat rash is not related to a fat embolus, which is a serious complication of a fracture that involves the release of fat droplets into the bloodstream.
Choice B reason: Tachypnea is an early sign of a fat embolus, as it indicates a respiratory distress that may be caused by the fat droplets blocking the pulmonary capillaries. Tachypnea is a rapid breathing rate that exceeds 20 breaths per minute, and it may be accompanied by dyspnea, chest pain, cough, or hemoptysis. Tachypnea is a sign of hypoxemia, which is a low level of oxygen in the blood, and it requires immediate intervention.
Choice C reason: Bradycardia is not an early sign of a fat embolus, as it is a slow heart rate that is below 60 beats per minute. Bradycardia may be caused by various factors, such as medication, heart disease, hypothyroidism, or vagal stimulation. Bradycardia is not related to a fat embolus, which is a serious complication of a fracture that involves the release of fat droplets into the bloodstream.
Choice D reason: Abdominal cramping is not an early sign of a fat embolus, as it is a pain or discomfort in the abdomen that may be caused by various factors, such as food intolerance, infection, inflammation, or obstruction. Abdominal cramping is not related to a fat embolus, which is a serious complication of a fracture that involves the release of fat droplets into the bloodstream.
Choice E reason: Confusion is not an early sign of a fat embolus, but a late sign that may indicate a cerebral involvement of the fat embolus. Confusion is a state of impaired awareness, orientation, or memory that may be caused by various factors, such as medication, infection, trauma, or hypoxia. Confusion is a sign of cerebral hypoxia, which is a low level of oxygen in the brain, and it requires immediate intervention.
Sign Up or Login to view all the 32 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
