Ivytech community college Med Surg II exam
Total Questions : 36
Showing 25 questions, Sign in for moreWhat is the best indication if the client with congestive heart failure is holding excess fluid?
Explanation
A. Intake and output:
Intake and output refer to monitoring the amount of fluids a person consumes (intake) and eliminates (output) through urine, feces, and other means. While tracking fluid intake and output is important, it may not provide a direct indication of excess fluid retention.
B. Pitting pedal edema:
Pitting pedal edema is swelling in the lower extremities, particularly the ankles and feet, that leaves an indentation (pit) when pressure is applied. This can be a sign of fluid retention but may not always be the earliest or most reliable indicator.
C. Crackles in the bases of the lungs:
Crackles or rales in the bases of the lungs can be indicative of pulmonary congestion, which may occur due to fluid accumulation. However, crackles alone may not always be specific to fluid overload and can be present in other respiratory conditions.
D. Daily weights:
Daily weights are a critical and sensitive measure for assessing fluid balance. Sudden weight gain, especially over a short period, can be a strong indicator of fluid retention. Monitoring weight on a daily basis helps to detect changes early, allowing for prompt intervention.
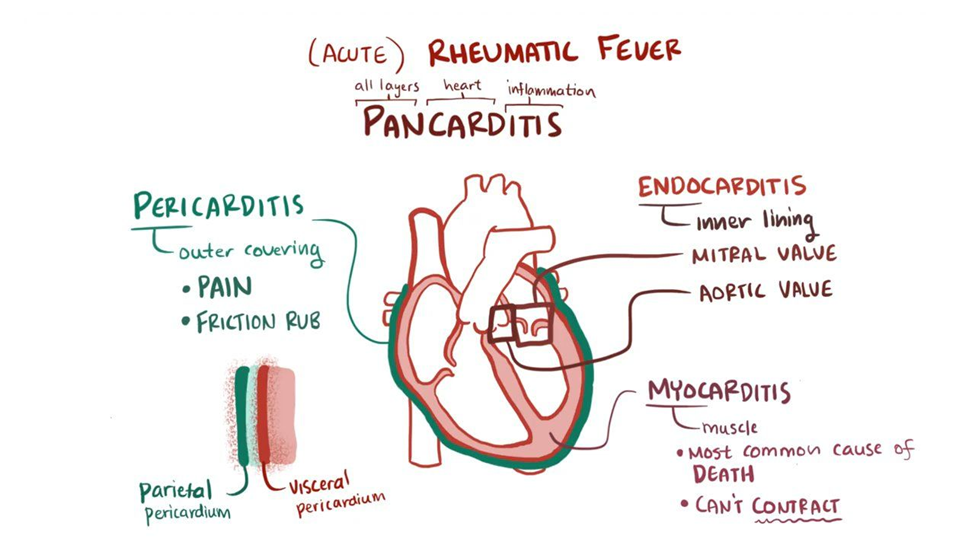
A client is being admitted to the medical unit to rule out cardiac issues related to valve malfunction. Which question should the nurse ask the client during the admission interview to support this diagnosis?
Explanation
A. "Did you have rheumatic fever as a child?"
Rheumatic fever is an inflammatory condition that can affect the heart, especially the heart valves. Rheumatic fever is a known risk factor for the development of valvular heart disease. Asking about a history of rheumatic fever helps identify a potential cause for valve malfunction.
B. "Do you have a family history of valve problems?"
Family history can be relevant in understanding genetic predispositions to certain cardiac conditions. While it may contribute to the overall assessment of cardiac risk, it may not be as directly linked to valve malfunction as a history of rheumatic fever.
C. "Do you have a history of MRSA?"
MRSA (Methicillin-resistant Staphylococcus aureus) is a type of bacterial infection and is not directly associated with valve malfunction. This question may be relevant for other aspects of the client's health but is not specific to ruling out cardiac issues related to valve malfunction.
D. "What over-the-counter medications do you take?"
While knowing the medications a client takes is important for a comprehensive assessment, asking about over-the-counter medications may not be as directly related to ruling out cardiac issues related to valve malfunction. It is more relevant for assessing potential interactions or effects on cardiovascular health.
A group of student nurses are practicing taking blood pressures. A 56-year-old male student has a blood pressure reading of 146/96 mm Hg. Upon hearing the reading, he exclaims, “My pressure has never been this high. Do you think my doctor will prescribe medication to reduce it?” Which of the following responses by the nursing instructor would be best?
Explanation
A. "A single elevated blood pressure does not confirm hypertension. A diagnosis of hypertension requires two or more elevated readings taken by your physician before a diagnosis can be made."
This response emphasizes the need for multiple elevated readings for a diagnosis of hypertension. It educates the individual about the diagnostic criteria and encourages them to seek further evaluation from their physician.
B. "We will need to reevaluate your blood pressure because your age places you at high risk for hypertension."
This response might be seen as implying that age alone is a significant factor in determining hypertension, which may not be accurate. While age is a risk factor, the emphasis should be on the need for multiple readings and a physician's evaluation rather than attributing it solely to age.
C. "Hypertension is prevalent among men: it is fortunate we caught this during your routine examination."
This response suggests that the elevated blood pressure is automatically assumed to be hypertension based on gender. It is important to avoid making assumptions and instead focus on the need for proper evaluation and multiple readings for a hypertension diagnosis.
D. "You have no need to worry. Your pressure is probably elevated because you are being tested."
This response dismisses the individual's concerns and attributes the elevated blood pressure solely to the testing situation. While stress or anxiety can influence blood pressure readings, it's essential to address the need for further evaluation and not completely disregard the possibility of hypertension.
A client with a complex cardiac history is scheduled for transesophageal echocardiography. Which of the following statements, if made by the nurse, is inappropriate?
Explanation
A. "The test will provide a detailed profile of the heart’s electrical activity."
This statement is inappropriate because transesophageal echocardiography (TEE) primarily provides detailed images of the heart's structure, such as the valves and chambers, rather than focusing on the heart's electrical activity. The assessment of electrical activity is typically associated with electrocardiography (ECG or EKG) rather than echocardiography.
B. "I will need to start an IV in your arm before the test."
This statement is appropriate. It is common for medical procedures, including TEE, to require an intravenous (IV) line for administration of medications or fluids during or after the procedure.
C. "Your throat may be a little sore after the exam."
This statement is appropriate. TEE involves inserting a probe through the esophagus, and it is common for patients to experience a sore throat afterward due to the presence of the probe.
D. "You will need to refrain from eating and drinking 6-8 hours before this test."
This statement is appropriate. It is standard practice to ask patients to fast for a specific period before TEE to minimize the risk of complications, such as aspiration, during the procedure.
The nurse is taking health history for a client who reports pain in his lower left leg and foot when walking. The pain is relieved with rest, and the nurse observes the left leg is hairless and slightly edematous. The nurse recognizes this as which medical diagnosis or health problem?
Explanation
A. Coronary artery disease (CAD):
Coronary artery disease primarily affects the blood vessels supplying the heart muscle. Symptoms often include chest pain (angina) rather than pain in the lower extremities. The symptoms described in the scenario are not characteristic of CAD.
B. Arterial embolus:
An arterial embolus is a blood clot or debris that travels through the bloodstream and can block an artery. While it can cause decreased blood flow and pain, the presentation in the lower left leg and foot with relief of pain at rest is more suggestive of peripheral arterial disease (PAD) or intermittent claudication rather than an acute arterial embolus.
C. Raynaud disease:
Raynaud's disease is characterized by episodes of reduced blood flow to the extremities, usually triggered by cold or stress. It typically involves color changes (white, blue, red) in the fingers or toes. The symptoms described, including pain in the lower leg and foot during walking, are not typical of Raynaud's disease.
D. Intermittent claudication:
Intermittent claudication is a symptom associated with peripheral arterial disease (PAD). It involves pain or cramping in the legs during physical activity, such as walking, due to reduced blood flow to the muscles. Rest typically relieves the pain. The observation of a hairless leg and slight edema suggests potential vascular compromise in the lower extremity, supporting the diagnosis of intermittent claudication.
An emergency department nurse is assessing an adult woman for a suspected myocardial infarction (MI). When planning the assessment, the nurse should be aware that female patients may have which of the following symptoms for an MI? (SELECT ALL THAT APPLY)
Explanation
A. Shortness of breath
Shortness of breath can be a symptom of a myocardial infarction in both men and women.
B. Anxiety
Anxiety can be a symptom in some cases, as individuals may feel a sense of impending doom or anxiety during an MI.
C. Unusual fatigue
Unusual fatigue, especially if it is severe or occurs with exertion, can be a symptom of a myocardial infarction.
D. Back pain
Back pain, particularly between the shoulder blades, can be a symptom of a myocardial infarction in women.
E. Chest pain
Chest pain or discomfort is a classic symptom of a myocardial infarction. While women may experience chest pain, they are also more likely than men to have atypical symptoms.
The nurse on a cardiac unit is caring for a client admitted with an acute exacerbation of heart failure. The nurse concludes that the client’s condition is worsening after noting which client data during assessment. (SELECT ALL THAT APPLY)
Explanation
A. Normal sinus rhythm that becomes sinus tachycardia
Sinus tachycardia can be an indication of increased sympathetic activity in response to decreased cardiac output. It may suggest the heart's compensatory response to maintain adequate perfusion.
B. Onset of a cough with pink, frothy sputum
Pink, frothy sputum is a classic sign of pulmonary edema, which can occur in the setting of worsening heart failure. It indicates the presence of blood-tinged fluid in the alveoli.
C. Presence of dyspnea at rest
Dyspnea at rest suggests that the client is experiencing difficulty breathing even without physical exertion. This can be indicative of more severe heart failure.
D. Falls asleep when not disturbed
Falling asleep when not disturbed may indicate fatigue or exhaustion, which is common in individuals with heart failure. However, it is not a direct indicator of worsening heart failure and can be influenced by various factors.
E. Urine drainage is increased in amount
Increased urine output can be a sign of diuretic therapy or an attempt by the body to compensate for fluid overload. However, it is essential to consider other factors such as renal function and medication effects.
The nurse is planning the care of a client with heart failure. The nurse should identify what overall goals for the client’s care? (SELECT ALL THAT APPLY)
Explanation
A. Limit physical activity
Limiting physical activity is not a primary goal in heart failure care. In fact, promoting appropriate and monitored physical activity is often part of the overall management plan. Exercise, when tailored to the client's condition, can improve functional status and quality of life.
B. Prevent endocarditis
While preventing endocarditis is important for individuals with certain cardiac conditions, it is not a primary goal in the care of heart failure. The focus is typically on optimizing cardiac function and managing heart failure symptoms.
C. Relieve the patient’s symptoms
Managing and relieving symptoms, such as dyspnea, fatigue, and fluid retention, are crucial goals in heart failure care. This includes optimizing medication management and other therapeutic interventions.
D. Extend survival
While heart failure is a chronic condition, the goal is to optimize treatment to improve the client's prognosis and overall survival. This involves the use of evidence-based therapies to address the underlying causes and contributing factors.
E. Improve functional status
Enhancing the client's ability to perform activities of daily living and improving functional capacity are important goals. This can involve a combination of medications, lifestyle modifications, and rehabilitation.
The nurse is teaching a client about some of the health consequences of uncontrolled hypertension. What health problems should the nurse describe. (SELECT ALL THAT APPLY)
Explanation
A. Retinal Hemorrhage
Uncontrolled hypertension can damage the blood vessels in the eyes, leading to retinal hemorrhages. This can result in vision problems and, in severe cases, vision loss.
B. Ventricular Hypertrophy
Uncontrolled hypertension causes the heart to pump against increased resistance, leading to the thickening and enlargement of the left ventricle. Ventricular hypertrophy is a response to the increased workload on the heart and is associated with an increased risk of heart failure.
C. Cerebrovascular Disease
Hypertension is a major risk factor for cerebrovascular diseases, including strokes. Elevated blood pressure can damage the blood vessels in the brain, increasing the risk of stroke. Strokes can have serious consequences, affecting various neurological functions.
D. Venous Insufficiency
Venous insufficiency is not typically directly associated with uncontrolled hypertension. It is more commonly related to problems with the venous system, such as damaged valves in the veins, leading to poor blood flow back to the heart. While hypertension can affect arteries, venous insufficiency is a distinct condition.
E. Transient Ischemic Attacks (TIAs)
Uncontrolled hypertension increases the risk of transient ischemic attacks (TIAs), which are brief episodes of neurological dysfunction caused by temporary disruption of blood flow to the brain. TIAs are often considered warning signs of an increased risk of stroke.
The nursing student is reviewing interventions which are part of nursing care and prevention of atelectasis. What are some of the interventions nurses can do to prevent atelectasis? (SELECT ALL THAT APPLY)
Explanation
A. Administer antibiotics
Administering antibiotics is not a direct intervention for preventing atelectasis. Antibiotics are typically prescribed to treat bacterial infections, and atelectasis is more related to lung collapse or incomplete lung expansion.
B. Encourage increased oral fluid intake
Adequate hydration is important for maintaining the moisture of respiratory secretions. This helps prevent mucus from becoming thick and sticky, making it easier for the patient to cough and clear the airways.
C. Early mobilization after surgery
Early mobilization, including activities such as getting out of bed and walking, helps improve lung expansion. It promotes better ventilation and prevents areas of the lungs from collapsing, reducing the risk of atelectasis.
D. Frequent turning of the patient
Turning the patient regularly is crucial for preventing pooling of respiratory secretions in dependent areas of the lungs. By changing the patient's position, nurses can facilitate drainage and ventilation throughout the lungs, minimizing the risk of atelectasis.
E. Use of incentive spirometry
Incentive spirometry is a breathing exercise device that encourages the patient to take slow, deep breaths. This helps expand the lungs and prevents atelectasis by maintaining lung volume and promoting alveolar recruitment.
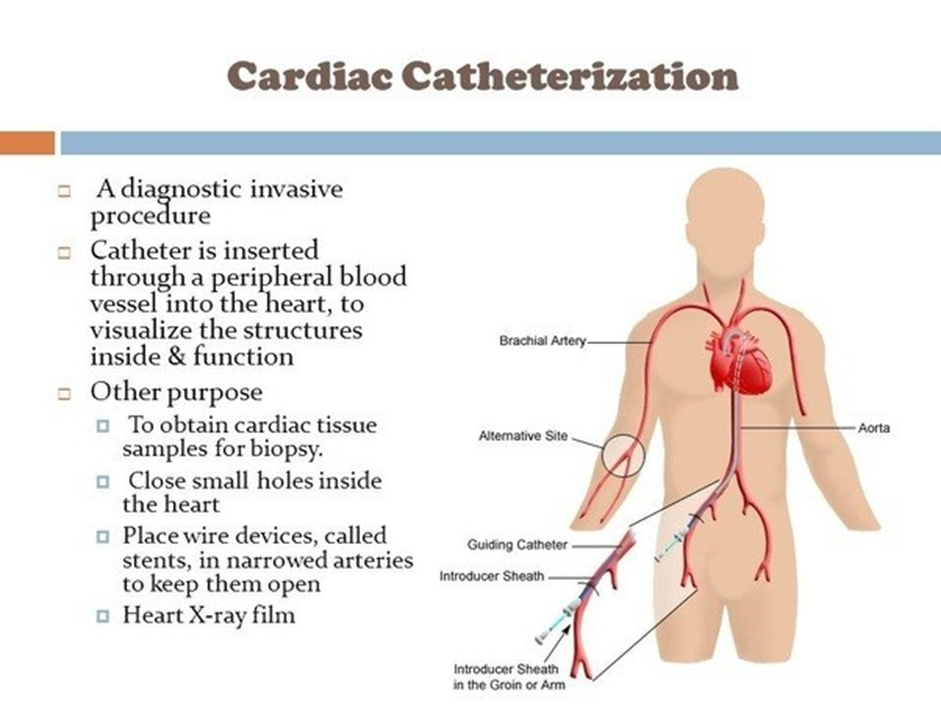
A client is scheduled for a cardiac catheterization. The nurse should do which of the following pre-procedure tasks? (SELECT ALL THAT APPLY)
Explanation
Withhold food and oral fluids before the procedure
Withholding food and oral fluids before the procedure is essential to prevent complications during the cardiac catheterization. The client is typically NPO (nothing by mouth) for a specified period before the procedure.
B. Review medications the client has taken in the last 24 hours
Reviewing the client's medications is crucial to ensure that any medications affecting coagulation or blood vessels are appropriately managed before the cardiac catheterization.
C. Verify that written consent has been obtained
Verifying the presence of written consent is a critical step to confirm that the client has been adequately informed about the procedure, its risks, and benefits, and has given consent for the cardiac catheterization.
D. Check for iodine sensitivity
Checking for iodine sensitivity is important because iodinated contrast dye is commonly used during cardiac catheterization. Allergies or sensitivities to iodine contrast must be identified to prevent adverse reactions.
E. Administer all ordered oral medications
Administration of oral medications before the procedure depends on the specific medications and the healthcare provider's instructions. Some medications may be held, while others may be continued as prescribed.
A client is ordered to receive 4 g of a medication. The pharmacy has the medication available in a concentration of 160 mg per 5 mL. How many mL should the client receive?
Explanation
To calculate the amount of mL that the client should receive, we need to use the formula:
mL = (g * 5 mL) / mg
where g is the ordered dose of the medication, mg is the concentration of the medication, and mL is the volume of the solution.
Plugging in the given values, we get:
mL = (4 g * 5 mL) / 160 mg
Simplifying, we get:
mL = 0.125 g/mL
Multiplying by 1000 to convert grams to milligrams, we get:
mL = 125 mg/mL
Therefore, the client should receive 125 mL of the solution.
A client with severe nausea has a one time order for ondansetron (Zofran) 8 mg IVPB to be administered over 15 minutes. The medication is diluted in 50 mL of D5W. The tubing drop factor is 15 gtt/mL. How many drops per minute should be given?
Explanation
To calculate the drops per minute for the ondansetron infusion, we need to use the formula:
drops per minute = (volume in mL x drop factor) / time in minutes
In this case, the volume is 50 mL, the drop factor is 15 gtt/mL, and the time is 15 minutes. Plugging these values into the formula, we get:
drops per minute = (50 x 15) / 15
drops per minute = 750 / 15
drops per minute = 50
Therefore, the nurse should set the infusion pump to deliver 50 drops per minute of ondansetron to the client with severe nausea.
A client is ordered to receive atropine 0.3 mg IV stat. Atropine 0.4 mg per mL is available. How many milliliters will the nurse administer?
Explanation
The nurse needs to calculate the correct dose of atropine for a client who has a prescription for 0.3 mg IV stat. The nurse knows that atropine is a medication that blocks the effects of the parasympathetic nervous system and is used to treat bradycardia, heart block, and some types of poisoning.
To find out how many milliliters of atropine the nurse will administer, the nurse can use the formula:
Dose ordered / Dose available = Volume to administer
Plugging in the values, the nurse gets:
0.3 mg / 0.4 mg per mL = 0.75 mL
Therefore, the nurse will administer 0.75 mL of atropine to the client IV stat.
The physician orders warfarin (Coumadin) 10 mg PO to be administered to a client at 1800 today. The pharmacy only has 2.5 mg tablets available. How many tablets will the nurse administer?
Explanation
Warfarin (Coumadin) is an anticoagulant medication that prevents blood clots from forming or growing larger. It is prescribed for clients who have atrial fibrillation, deep vein thrombosis, pulmonary embolism, or artificial heart valves.
The physician orders warfarin 10 mg PO to be administered to a client at 1800 today. The pharmacy only has 2.5 mg tablets available. To calculate the number of tablets that the nurse will administer, the nurse will divide the ordered dose by the available dose. The formula is:
Number of tablets = Ordered dose / Available dose
Number of tablets = 10 mg / 2.5 mg
Number of tablets = 4
Therefore, the nurse will administer 4 tablets of warfarin 2.5 mg PO to the client at 1800 today
A nurse is explaining to a client with asthma what her new prescription for prednisone, a systemic corticosterioid, is used for in the treatment of asthma. What would be the most accurate explanation that the nurse could give?
Explanation
A. To ensure long-term prevention of asthma exacerbations:
This statement is not accurate. Prednisone is typically not used for long-term prevention of asthma exacerbations. It is more commonly prescribed for short-term use during acute exacerbations to quickly reduce inflammation and improve symptoms.
B. To gain control of inadequately controlled, persistent asthma:
This is the most accurate explanation. Prednisone is often prescribed to gain control over inadequately controlled, persistent asthma by providing anti-inflammatory effects and helping to manage symptoms during acute episodes.
C. To cure any systemic infection underlying asthma attacks:
Prednisone is not used to cure infections. While it can have anti-inflammatory and immunosuppressive effects, its primary role in asthma is to reduce airway inflammation and control symptoms, not to treat underlying infections.
D. To prevent recurrent pulmonary infections:
Prednisone is not typically prescribed for the prevention of infections. Its use in asthma is more focused on managing inflammation and symptoms during acute exacerbations rather than preventing infections.
A nurse assesses a client’s respiratory status. Which observation indicates that the client is having difficulty breathing?
Explanation
A. Diaphragmatic breathing:
Diaphragmatic breathing, also known as abdominal or deep breathing, is a normal and effective way of breathing. It involves the contraction and relaxation of the diaphragm, allowing for efficient lung expansion. This is a healthy and efficient breathing technique.
B. Controlled breathing:
Controlled breathing refers to a deliberate and regulated breathing pattern. It can include techniques such as paced breathing, where the individual consciously controls the rate and depth of their breaths. Controlled breathing is generally considered a positive and intentional approach to managing respiratory function.
C. Pursed-lip breathing:
Pursed-lip breathing is a breathing technique where the individual breathes in through the nose and exhales through pursed lips. This method is often taught to individuals with certain respiratory conditions, such as chronic obstructive pulmonary disease (COPD), to help improve lung function and alleviate shortness of breath. Pursed-lip breathing can be a helpful strategy in specific situations.
D. Use of accessory muscles:
The use of accessory muscles indicates that the person is experiencing increased difficulty in breathing. Accessory muscles, such as the neck and shoulder muscles, are not typically heavily involved in breathing under normal circumstances. When these muscles are visibly working during breathing, it suggests increased respiratory effort and can be a sign of respiratory distress or difficulty.
A critical-care nurse is caring for a client diagnosed with pneumonia as a surgical complication. The nurse’s assessment reveals that the client has an increased work of breathing due to copious tracheobronchial secretions. What should the nurse encourage the patient to do?
Explanation
A. Lie in a low Fowler’s or supine position:
Lying in a low Fowler's or supine position may worsen respiratory distress and compromise oxygenation. It can reduce lung expansion and increase the work of breathing, especially in patients with pneumonia. This is not a recommended position for individuals with respiratory issues.
B. Increase oral fluids unless contraindicated:
Increasing oral fluids is generally a good practice, especially in respiratory conditions like pneumonia. It helps thin respiratory secretions, making them easier to clear. However, this alone may not address copious tracheobronchial secretions. Suctioning may be needed to effectively remove excess secretions.
C. Increase activity:
Increasing activity may be beneficial for some patients, but it might exacerbate respiratory distress in others, especially if they are already experiencing increased work of breathing. The appropriateness of increasing activity depends on the specific condition and the patient's overall stability.
D. Call the nurse for oral suctioning as needed:
This is the most appropriate choice. If the client is experiencing increased work of breathing due to copious tracheobronchial secretions, calling the nurse for oral suctioning is an intervention aimed at maintaining a clear airway and alleviating respiratory distress. Regular suctioning may be necessary to assist the client in managing secretions effectively.
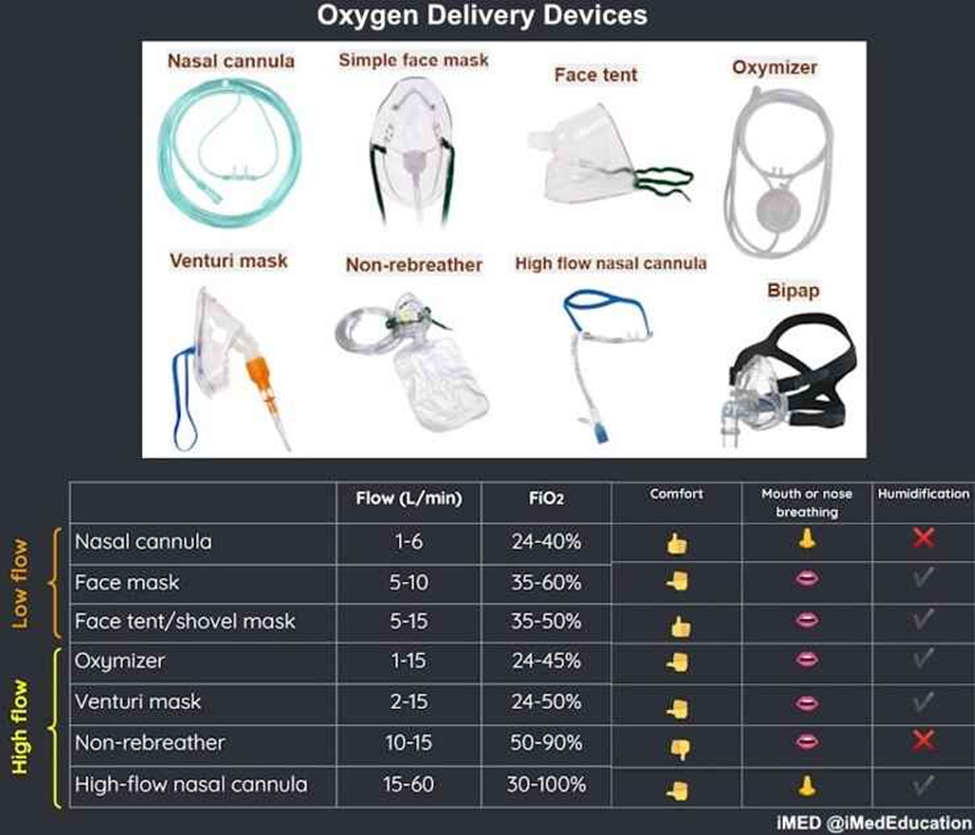
The nurse is caring for a client who is experiencing mild shortness of breath during the immediate postoperative period, with oxygen saturation readings between 89% and 91%. What method of oxygen delivery is most appropriate for the client’s needs?
Explanation
A. Partial non-rebreathing mask:
This mask delivers higher concentrations of oxygen than a nasal cannula. It has a reservoir bag that allows the client to rebreathe some exhaled air, increasing the oxygen concentration delivered. However, it may not be necessary for a client with mild shortness of breath and slightly reduced oxygen saturation.
B. Simple (Oxy Plus) mask:
The simple mask provides a higher concentration of oxygen than a nasal cannula but lacks the reservoir bag found in the non-rebreathing mask. It is generally used for moderate oxygen needs. However, it might be more than what is required for a client with mild shortness of breath and slightly reduced oxygen saturation.
C. Nasal cannula:
Nasal cannulas are commonly used for clients with mild respiratory distress. They deliver a lower to moderate concentration of oxygen and are well-tolerated by most clients. They are suitable for individuals with mild shortness of breath and can be adjusted based on the required flow rate.
D. Non-rebreathing mask:
The non-rebreathing mask provides the highest concentration of oxygen among the options listed. It includes a reservoir bag to deliver a higher oxygen concentration. It is typically reserved for clients with higher oxygen requirements. For a client with mild shortness of breath and slightly reduced oxygen saturation, this may be more than necessary.
An admitting nurse is assessing a client with COPD. The nurse auscultates diminished breath sounds. These findings indicated the nurse to monitor the client for what?
Explanation
A. Kyphosis and clubbing of the fingers:
Kyphosis refers to an excessive forward curvature of the spine, which is not directly related to diminished breath sounds. Clubbing of the fingers is often associated with chronic respiratory conditions, but it is not directly linked to the finding of diminished breath sounds.
B. Dyspnea and hypoxemia:
Dyspnea (shortness of breath) and hypoxemia (low oxygen levels in the blood) are common symptoms in COPD, but diminished breath sounds may indicate an additional concern, such as pneumothorax or other complications.
C. Sepsis and pneumothorax:
Diminished breath sounds can be a sign of pneumothorax, a condition where air accumulates in the pleural space, leading to lung collapse. Sepsis is a risk in clients with COPD due to the potential for respiratory infections. Monitoring for these complications is crucial.
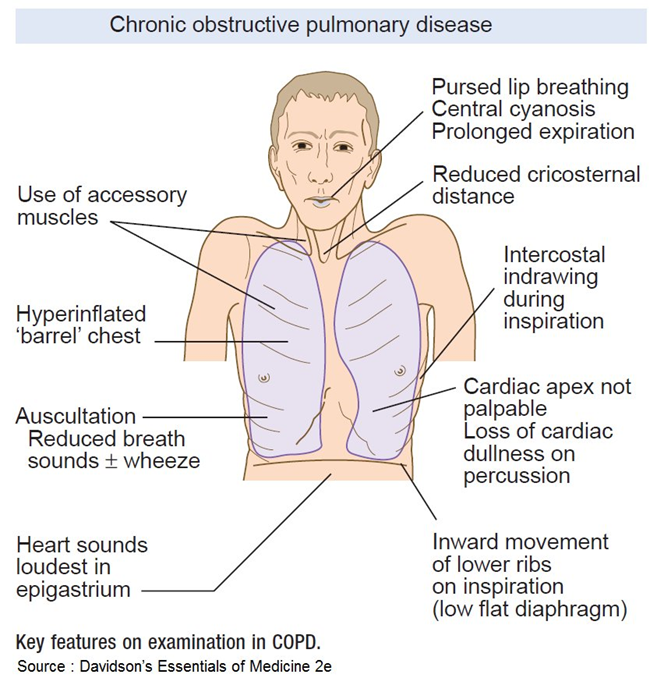
D. Bradypnea and pursed-lip breathing:
Bradypnea (slow breathing) and pursed-lip breathing are coping mechanisms that individuals with COPD may use to manage their breathing difficulties. While they are relevant in the context of COPD, they are not directly associated with the finding of diminished breath sounds.
The nurse is assessing a client who frequently coughs after eating or drinking. How should the nurse best follow up on this assessment finding?
Explanation
A. Obtain a sputum sample:
This option is more relevant when the client is experiencing cough with sputum production, which might suggest respiratory issues. However, in the context of coughing after eating or drinking, the primary concern is likely related to the swallowing process rather than respiratory conditions.
B. Inspect the client’s tongue and mouth:
While inspecting the tongue and mouth is a good practice for assessing oral health, it may not directly address the issue of coughing after eating or drinking, which is more indicative of potential swallowing difficulties.
C. Perform a swallowing assessment:
This is the most appropriate option for the given scenario. A swallowing assessment helps identify any abnormalities or difficulties in the swallowing process, which could contribute to the client's coughing after eating or drinking.
D. Assess the client’s nutritional status:
While assessing nutritional status is important for overall health, it may not directly address the immediate concern of coughing after eating or drinking. Nutritional status assessment is a broader aspect of care.
The nurse should place a client being admitted to the hospital with suspected tuberculosis (TB) on what type of isolation?
Explanation
A. Standard precautions:
Standard precautions are the basic level of infection control and should be used for all patient care. These precautions include practices like hand hygiene, the use of personal protective equipment (PPE), and safe injection practices.
B. Airborne precautions:
These precautions are used to prevent the transmission of infectious agents that are spread through the air. In the case of tuberculosis (TB), which is caused by Mycobacterium tuberculosis, airborne precautions are necessary to reduce the risk of airborne transmission.
C. Contact precautions:
Contact precautions are used for patients with known or suspected infections that can be transmitted by direct or indirect contact. Examples include Clostridium difficile infection and multidrug-resistant organisms. These precautions involve the use of PPE and may include patient placement in a private room.
D. Droplet precautions:
Droplet precautions are used when a patient is known or suspected to be infected with pathogens that are transmitted by respiratory droplets. Examples include influenza and certain types of bacterial meningitis. These precautions include placing the patient in a private room and using PPE.
The nurse is caring for a patient who has decreased mobility. Which intervention is a simple and cost-effective method for reducing the risks of stasis of pulmonary secretions and decreased chest wall expansion?
Explanation
A. Frequent change of position:
Frequent changes in position help prevent pooling of secretions and promote lung expansion. This simple and cost-effective measure is important in preventing complications related to immobility, such as pneumonia and atelectasis. It aids in maintaining optimal respiratory function.
B. Antibiotics: Antibiotics are used to treat bacterial infections and would not directly address the risks associated with decreased mobility.
C. Oxygen humidification: While oxygen therapy may be necessary in some cases, humidification is typically used to prevent drying of mucous membranes and is not a primary intervention for preventing complications of decreased mobility.
D. Chest physiotherapy: Chest physiotherapy involves techniques to mobilize respiratory secretions and may be indicated in specific situations. However, it is not as simple and cost-effective as frequent changes in position.
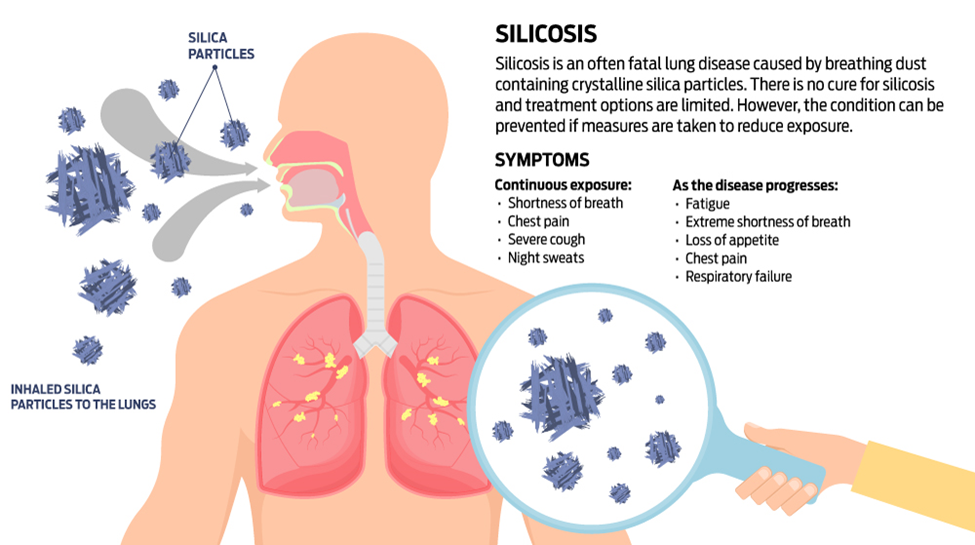
The nurse is taking the history of a client with occupational lung disease (silicosis). The nurse should assess whether the client wears which item during periods of exposure to silica particles?
Explanation
A. Mask:
Silicosis is a lung disease caused by inhaling crystalline silica dust. The primary preventive measure during exposure to silica particles is wearing a mask or respirator. This helps to reduce the inhalation of silica dust, protecting the respiratory system.
B. Gloves: Gloves are typically worn to protect the hands and skin and are not directly related to preventing inhalation of airborne particles.
C. Eye Protection: While eye protection is important in certain occupational settings, it does not specifically address the inhalation of silica particles.
D. Gown: Gowns are worn for protection against contamination but are not directly related to the prevention of occupational lung diseases such as silicosis.
The nurse is caring for a client who has signs and symptoms of heart failure. Which of the following diagnostic tests is appropriate to assess the patient’s heart failure?
Explanation
A. International normalized ratio (INR):
INR is a test used to monitor the effectiveness of anticoagulant therapy, particularly drugs like warfarin. It measures the time it takes for blood to clot. It's not directly related to assessing heart failure but is more associated with monitoring anticoagulation status.
B. Brain natriuretic peptide (BNP):
BNP is a peptide released by the heart in response to increased pressure and volume in the heart, often seen in heart failure. Elevated BNP levels can indicate the presence of heart failure. It's a useful diagnostic marker for heart failure.
C. Troponin:
Troponin is a protein released into the blood when there is damage to the heart muscle, usually during a heart attack. It is not specific to heart failure but is commonly used to diagnose myocardial infarction (heart attack).
D. Creatinine:
Creatinine is a waste product that comes from the normal wear and tear on muscles. While elevated creatinine levels can be seen in conditions affecting kidney function, it's not a direct marker for assessing heart failure. However, kidney function is often evaluated in conjunction with heart failure assessments.
Sign Up or Login to view all the 36 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
