Massbay Community College Med Surg exam 2
Total Questions : 44
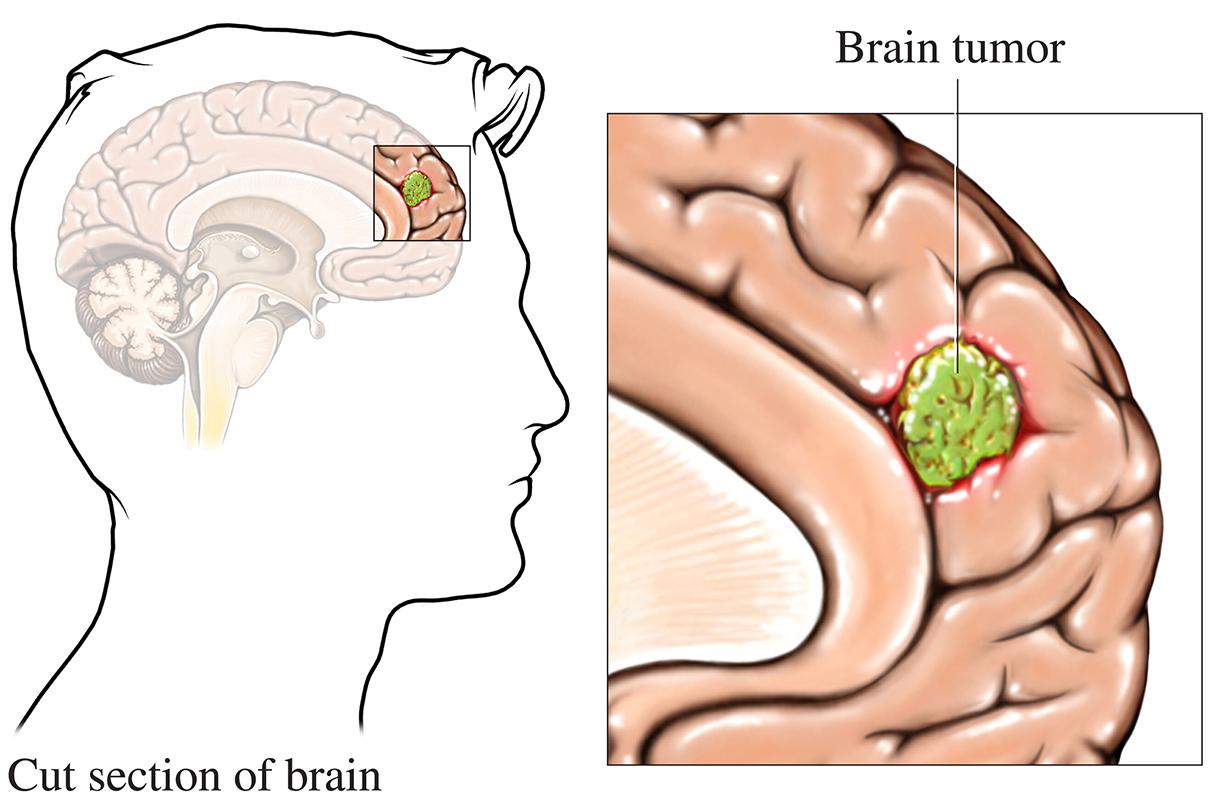
Showing 25 questions, Sign in for moreWhich early symptoms in a focused assessment by the nurse may indicate the presence of a brain tumor?
Explanation
Choice A reason: Sudden unconsciousness, unresponsiveness, and apnea are not typical symptoms of a brain tumor. They are more likely to indicate a stroke, seizure, or cardiac arrest.
Choice B reason: Increased temperature, blood pressure, heart rate, and respirations are not specific symptoms of a brain tumor. They are more likely to indicate an infection, inflammation, or stress.
Choice C reason: Changes in vision and personality, and headache upon awakening are common symptoms of a brain tumor. They are caused by the pressure of the tumor on the brain tissue and the cranial nerves.
Choice D reason: Fever, increased white blood cell count, and decreased appetite are not typical symptoms of a brain tumor. They are more likely to indicate a systemic infection or malignancy.
The nurse is evaluating the cranial nerves of a person with Parkinson disease who has difficulty swallowing foods. The nurse asks the patient to stick out their tongue and move it rapidly from side to side. The nurse is assessing which cranial nerve?
Explanation
Choice A reason: The hypoglossal nerve is responsible for the movement of the tongue. It innervates the muscles of the tongue and allows for speech, swallowing, and chewing.
Choice B reason: The trigeminal nerve is responsible for the sensation and motor function of the face. It innervates the muscles of mastication, the skin of the face, and the mucous membranes of the mouth and nose.
Choice C reason: The facial nerve is responsible for the expression and taste of the face. It innervates the muscles of facial expression, the lacrimal and salivary glands, and the anterior two-thirds of the tongue.
Choice D reason: The vestibulocochlear nerve is responsible for the hearing and balance of the ear. It innervates the cochlea and the vestibular apparatus of the inner ear.
The nurse assesses a patient who potentially may have meningitis. The patient demonstrates a positive Brudzinski's sign with which changes in position.
Explanation
Choice A reason: Flexion of the hip causing resistance to extension of the leg is not a sign of meningitis. It is a sign of hip joint inflammation or injury.
Choice B reason: Flexion of the neck causing flexion of the hips and knees is a positive Brudzinski's sign. It indicates irritation of the meninges, the membranes that cover the brain and spinal cord.
Choice C reason: Flexion of the ankle causing upward fanning of the toes is not a sign of meningitis. It is a sign of an upper motor neuron lesion, such as a stroke or spinal cord injury.
Choice D reason: Flexion of the neck causing pain and spasm in the leg muscles is not a sign of meningitis. It is a sign of muscle strain or nerve compression.
The nurse is educating the family about anticipated changes during the late stages of amyotrophic lateral sclerosis (ALS) for their father. What teaching point is most important for the nurse to include?
Explanation
Choice A reason: ALS is a neurodegenerative disease that affects the motor neurons, which control the voluntary muscles. It does not affect the cognitive or mental functions, such as memory, reasoning, or emotions. Therefore, the person with ALS will be aware of their condition and their surroundings, even when they lose their ability to move, speak, or breathe.
Choice B reason: ALS affects the muscles of the mouth, throat, and chest, which are involved in swallowing. As the disease progresses, the person with ALS will have difficulty swallowing food, liquids, and saliva. This can lead to malnutrition, dehydration, choking, and aspiration pneumonia.
Choice C reason: ALS does not directly cause seizures, which are abnormal electrical activity in the brain. However, some medications used to treat the symptoms of ALS, such as muscle relaxants, may increase the risk of seizures. Therefore, the person with ALS should be monitored for any signs of seizures, such as loss of consciousness, convulsions, or confusion.
Choice D reason: ALS affects the muscles of the diaphragm and the intercostal muscles, which are involved in breathing. As the disease progresses, the person with ALS will have difficulty breathing, especially at night or when lying down. This can lead to respiratory failure, which is the most common cause of death in ALS. Therefore, the person with ALS may need mechanical ventilation or noninvasive positive pressure ventilation to support their breathing.
The nurse is caring for a 9-year-old undergoing chemotherapy to treat leukemia. Select the priority nursing goal for the child's plan of care.
Explanation
Choice A reason: Encouraging intake of favorite foods to increase weight and promote normal growth is an important nursing goal for a child with leukemia, but it is not the priority. Chemotherapy can cause nausea, vomiting, and loss of appetite, which can affect the child's nutritional status and growth. However, these effects can be managed with antiemetics, supplements, and small frequent meals.
Choice B reason: Utilizing approaches to minimize risk of infection and bleeding episodes is the priority nursing goal for a child with leukemia. Chemotherapy can cause bone marrow suppression, which reduces the production of white blood cells, red blood cells, and platelets. This increases the risk of infection, anemia, and bleeding, which can be life-threatening. Therefore, the nurse should monitor the child's blood counts, vital signs, and signs of infection or bleeding, and implement preventive measures such as hand hygiene, isolation, and transfusions.
Choice C reason: Providing age-appropriate activities to promote optimum cognitive and motor skills development is an important nursing goal for a child with leukemia, but it is not the priority. Chemotherapy can cause fatigue, weakness, and neuropathy, which can affect the child's physical and mental abilities. However, these effects can be managed with rest, pain relief, and stimulation.
Choice D reason: Providing emotional support for the child and family members that relieve stress is an important nursing goal for a child with leukemia, but it is not the priority. Chemotherapy can cause anxiety, depression, and fear, which can affect the child's psychological and emotional well-being. However, these effects can be managed with counseling, education, and coping strategies.
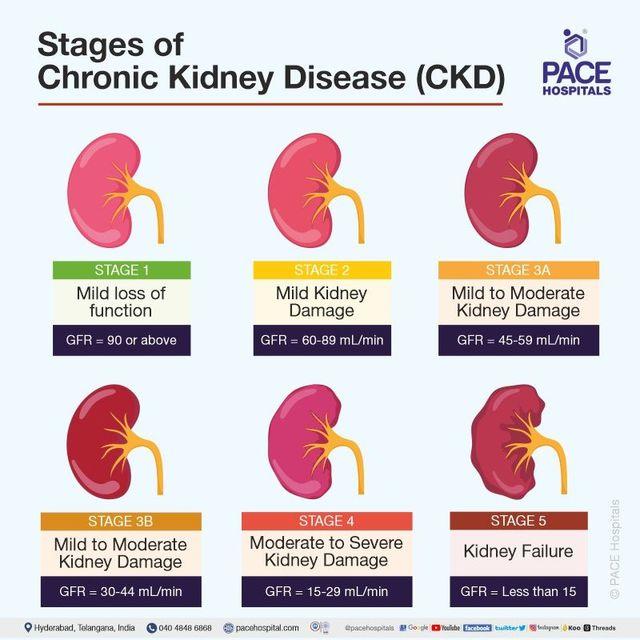
The nurse is caring for a patient with anemia. Their medical history includes diabetes mellitus Type 1, hypertension, chronic kidney disease, and peripheral vascular disease. Which condition most likely contributes to their anemia?
Explanation
Choice A reason: Diabetes mellitus Type 1 is a condition that affects the pancreas and the production of insulin, a hormone that regulates blood sugar levels. It does not directly cause anemia, but it can increase the risk of complications such as infections, ulcers, and nerve damage.
Choice B reason: Peripheral vascular disease is a condition that affects the blood vessels and the circulation of blood to the limbs. It does not directly cause anemia, but it can increase the risk of complications such as clots, wounds, and gangrene.
Choice C reason: Chronic kidney disease is a condition that affects the kidneys and their function of filtering waste and fluids from the blood. It can cause anemia by reducing the production of erythropoietin, a hormone that stimulates the bone marrow to make red blood cells.
Choice D reason: Hypertension is a condition that affects the blood pressure and the force of blood against the artery walls. It does not directly cause anemia, but it can increase the risk of complications such as stroke, heart attack, and kidney damage.
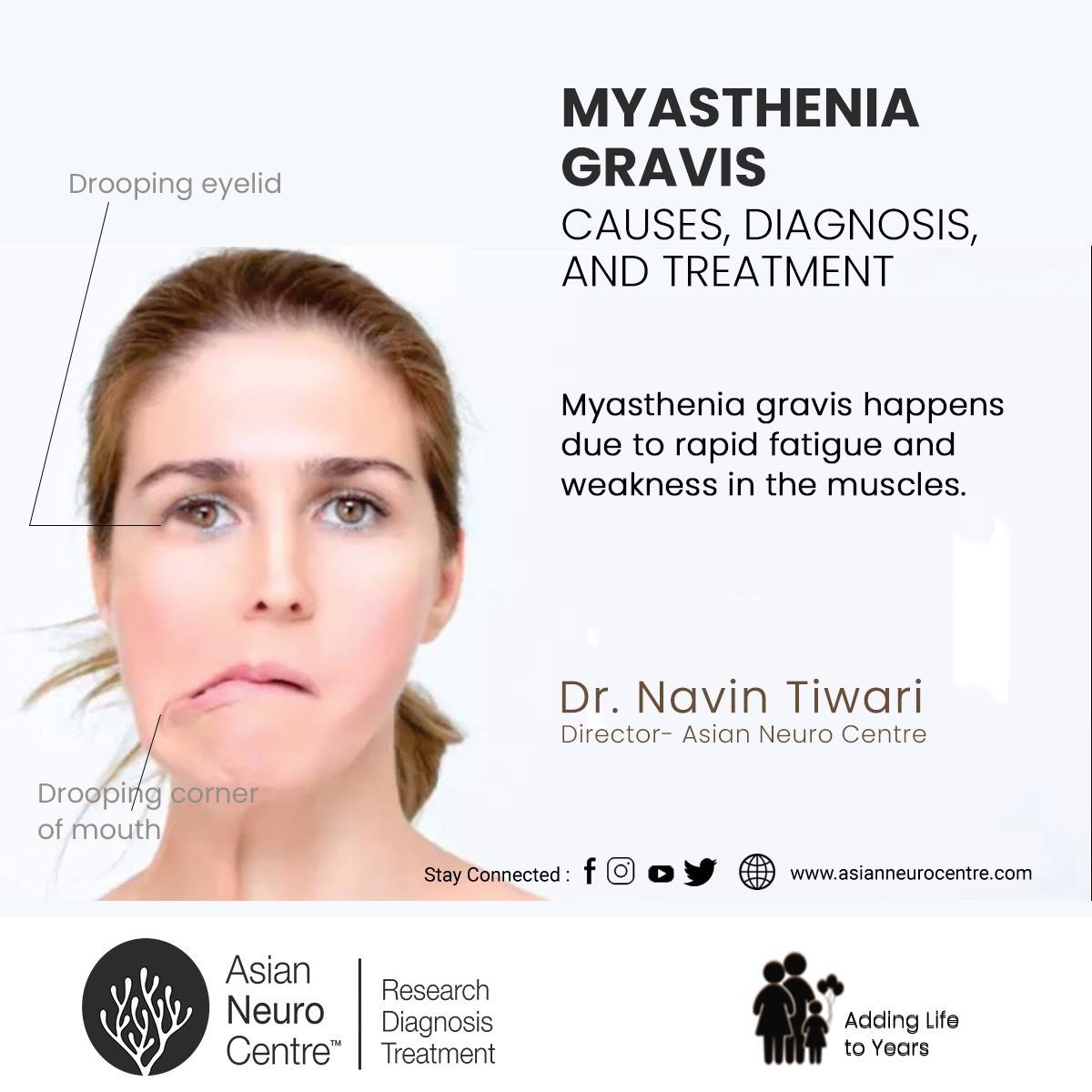
You are a home health nurse providing care to a patient with myasthenia gravis. Today you plan on helping the patient with bathing and exercising. When would be the best time to visit the patient to help with these tasks?
Explanation
Choice A reason: Evening is not the best time to visit the patient with myasthenia gravis to help with bathing and exercising. Myasthenia gravis is a condition that causes muscle weakness and fatigue, which worsens as the day progresses. Therefore, the patient may have more difficulty performing these activities in the evening.
Choice B reason: Mid-afternoon is not the best time to visit the patient with myasthenia gravis to help with bathing and exercising. Myasthenia gravis causes muscle weakness and fatigue, which may be aggravated by the heat and humidity of the afternoon. Therefore, the patient may have more difficulty performing these activities in the mid-afternoon.
Choice C reason: Morning is the best time to visit the patient with myasthenia gravis to help with bathing and exercising. Myasthenia gravis causes muscle weakness and fatigue, which are less severe in the morning after a night of rest. Therefore, the patient may have more strength and energy to perform these activities in the morning.
Choice D reason: Before bedtime is not the best time to visit the patient with myasthenia gravis to help with bathing and exercising. Myasthenia gravis causes muscle weakness and fatigue, which are most severe at the end of the day. Therefore, the patient may have more difficulty performing these activities before bedtime.
Postoperative care for a patient having a craniotomy to relieve increased intracranial pressure, the nurse should implement which intervention?
Explanation
Choice A reason: Elevating the head of the bed 20 to 30 degrees is an appropriate intervention for a patient who had a craniotomy to relieve increased intracranial pressure. It helps to reduce the venous pressure and improve the cerebral perfusion.
Choice B reason: Maintaining bright lighting in the room to assess bleeding at the surgical site is not an appropriate intervention for a patient who had a craniotomy to relieve increased intracranial pressure. It can increase the sensory stimulation and aggravate the intracranial pressure. The nurse should use dim lighting and monitor the dressing and the drainage system for signs of bleeding.
Choice C reason: Stimulating the patient every half hour to assess changes in level of consciousness is not an appropriate intervention for a patient who had a craniotomy to relieve increased intracranial pressure. It can increase the cerebral metabolic demand and worsen the intracranial pressure. The nurse should assess the level of consciousness using the Glasgow Coma Scale and avoid unnecessary stimulation.
Choice D reason: Allowing the patient to change positions frequently to maintain comfort is not an appropriate intervention for a patient who had a craniotomy to relieve increased intracranial pressure. It can increase the intrathoracic pressure and affect the cerebral blood flow. The nurse should limit the patient's movement and avoid extreme flexion, extension, or rotation of the head and neck.
The nurse is caring for a patient undergoing a lumbar puncture by the provider. Select the priority nursing intervention the nurse would complete after the procedure.
Explanation
Choice A reason: Maintaining pressure to the puncture site and observing for drainage is the priority nursing intervention for a patient who had a lumbar puncture. It helps to prevent bleeding, hematoma, and cerebrospinal fluid leakage, which can cause complications such as infection, headache, or nerve damage.
Choice B reason: Completing a pain assessment and administering an ordered analgesic, as needed, is an important nursing intervention for a patient who had a lumbar puncture, but it is not the priority. Lumbar puncture can cause mild to moderate pain and discomfort at the puncture site, which can be relieved by analgesics, ice packs, or massage.
Choice C reason: Informing the patient they may feel pressure and sharp pain in their lower back for several hours is an important nursing intervention for a patient who had a lumbar puncture, but it is not the priority. Lumbar puncture can cause transient sensations of pressure and pain in the lower back, which can be reduced by lying flat, avoiding sudden movements, and drinking fluids.
Choice D reason: Assessing pulses distal to the lumbar puncture site every two hours is not an appropriate nursing intervention for a patient who had a lumbar puncture. Lumbar puncture does not affect the blood circulation to the lower extremities, unless there is a complication such as hematoma or nerve compression. Therefore, the nurse should monitor the neurological status, vital signs, and signs of infection or bleeding.
The nurse is assisting the neurologist with a lumbar puncture on a patient with possible meningitis. Which post-procedure teaching point is the highest priority for the patient?
Explanation
Choice A reason: Maintaining a flat lying position for 14 hours following the procedure is the highest priority teaching point for the patient who had a lumbar puncture. It helps to prevent cerebrospinal fluid leakage and post-lumbar puncture headache, which can be severe and debilitating.
Choice B reason: Muscular discomfort is expected after being in a curled position for a period of time, but it is not the highest priority teaching point for the patient who had a lumbar puncture. It is a common and mild side effect that can be relieved by analgesics, massage, or heat therapy.
Choice C reason: Resuming oral intake immediately after the procedure is not a priority teaching point for the patient who had a lumbar puncture. It is not contraindicated, but it is not essential either. The patient should drink plenty of fluids to replenish the cerebrospinal fluid and prevent dehydration.
Choice D reason: Mild pain is expected at the needle insertion site, but it is not the highest priority teaching point for the patient who had a lumbar puncture. It is a common and mild side effect that can be relieved by analgesics, ice packs, or dressing.
The nurse is caring for a patient with a new traumatic brain injury and completes a neurologic assessment. The magnetic resonance imaging identifies an intracranial epidural hematoma. The nurse would immediately notify the provider of which assessment finding?
Explanation
Choice A reason: Eyes are deviated to the right is an assessment finding that indicates increased intracranial pressure and possible herniation of the brain. It is a sign of cranial nerve III palsy, which affects the movement of the eye and the size of the pupil. It is a medical emergency that requires immediate intervention.
Choice B reason: Amnesia to the cause of the trauma is an assessment finding that indicates memory loss and possible concussion. It is a sign of damage to the temporal lobe, which is involved in memory formation and retrieval. It is not a medical emergency, but it requires further evaluation and monitoring.
Choice C reason: Complaint of mild headache is an assessment finding that indicates pain and discomfort. It is a common symptom of traumatic brain injury, but it is not specific or severe. It can be managed with analgesics and rest.
Choice D reason: Pupils constrict from 5 mm to 2 mm with direct light stimulus is an assessment finding that indicates normal pupillary response. It is a sign of intact cranial nerve II and III function, which control the vision and the pupil size. It is not a cause for concern or notification.
The home health nurse visits a patient with multiple sclerosis who complains of severe fatigue. Select the nurse's best suggestion to help decrease their symptom of fatigue.
Explanation
Choice A reason: Relaxing in a hot bath before bedtime is not the best suggestion to help decrease fatigue for a patient with multiple sclerosis. Heat can worsen the symptoms of multiple sclerosis, such as muscle weakness, numbness, and vision problems. Therefore, the patient should avoid hot baths, showers, or saunas, and use cool compresses or fans to lower their body temperature.
Choice B reason: Performing deep breathing exercises every two hours is not the best suggestion to help decrease fatigue for a patient with multiple sclerosis. Deep breathing can help reduce stress and anxiety, but it does not address the underlying causes of fatigue, such as inflammation, nerve damage, or sleep problems. Therefore, the patient should consult their doctor for appropriate treatment options and medication adjustments.
Choice C reason: Scheduling short periods of rest throughout the day is the best suggestion to help decrease fatigue for a patient with multiple sclerosis. Fatigue is a common and disabling symptom of multiple sclerosis, which can affect the patient's daily activities and quality of life. Therefore, the patient should plan their tasks according to their energy level, prioritize the most important ones, and take frequent breaks to conserve their energy and prevent exhaustion.
Choice D reason: Including daily multivitamins in your diet is not the best suggestion to help decrease fatigue for a patient with multiple sclerosis. Multivitamins can provide some nutritional benefits, but they are not a substitute for a balanced and healthy diet. Therefore, the patient should eat a variety of foods, such as fruits, vegetables, whole grains, lean proteins, and low-fat dairy, and avoid processed, fried, or sugary foods that can increase inflammation and fatigue.
A patient makes an appointment to see a primary care practitioner for recurrent severe headaches. Which instruction by the nurse will help gather the best additional data before the appointment?
Explanation
Choice A reason: "Try relaxation and warm moist compresses for your headaches and document your response." is not the best instruction by the nurse to gather additional data before the appointment. It is a suggestion for self-care and pain relief, but it does not provide any information about the cause, type, or severity of the headaches.
Choice B reason: "Keep a diary of your headaches, recording symptoms, timing, and headache triggers." is the best instruction by the nurse to gather additional data before the appointment. It is a useful tool for collecting objective and subjective data about the headaches, such as their frequency, duration, intensity, location, quality, associated symptoms, and precipitating factors. This can help the primary care practitioner to diagnose the type of headache, such as migraine, tension, or cluster, and prescribe the appropriate treatment.
Choice C reason: "Call and come in the next time you have a headache so you can be examined." is not the best instruction by the nurse to gather additional data before the appointment. It is a suggestion for urgent care, but it does not provide any information about the history, pattern, or characteristics of the headaches.
Choice D reason: "Keep track of how many headaches you have before you come in." is not the best instruction by the nurse to gather additional data before the appointment. It is a simple measure of the quantity of the headaches, but it does not provide any information about the quality, severity, or triggers of the headaches.
The nurse completes a focused assessment and history of a patient who is scheduled for magnetic resonance imaging (MRI). Which data shared by the patient would the nurse need to contact the provider?
Explanation
Choice A reason: Presence of a synthetic silicone mesh stent in a coronary artery is not a contraindication for MRI. Silicone is a non-magnetic material that does not interfere with the magnetic field or cause any harm to the patient or the device.
Choice B reason: Allergy to shellfish and iodine is not a contraindication for MRI. Shellfish and iodine are not related to the contrast agent used for MRI, which is usually gadolinium. However, the patient should inform the provider if they have any history of allergic reactions to contrast agents or any other medications.
Choice C reason: Contact lenses are not a contraindication for MRI. Contact lenses are made of plastic or silicone, which are non-magnetic materials that do not interfere with the magnetic field or cause any harm to the patient or the device. However, the patient should remove them before the procedure to avoid any discomfort or irritation.
Choice D reason: Presence of an internal insulin pump in the abdomen is a contraindication for MRI. Insulin pumps are electronic devices that contain metal parts, batteries, and wires, which can be affected by the magnetic field and cause malfunction, damage, or injury to the patient or the device. Therefore, the patient should inform the provider and the MRI technician about the insulin pump and follow their instructions on how to manage it before, during, and after the procedure.
A child with iron-deficiency anemia receives a daily oral iron supplement. The mother tells the nurse their child is having black stools. Which response by the nurse is most appropriate?
Explanation
Choice A reason: "You need to bring your child to the emergency department immediately and have the stool tested for blood." is not an appropriate response by the nurse. Black stools can be a sign of gastrointestinal bleeding, which is a serious condition that requires immediate medical attention. However, in this case, the black stools are most likely caused by the iron supplement, which can change the color and consistency of the stool. Therefore, there is no need to panic or rush to the emergency department.
Choice B reason: "Greenish black stools are normal when oral iron supplements are being administered." is the most appropriate response by the nurse. It is a factual and reassuring statement that explains the reason for the stool color change and educates the mother about the expected side effect of the iron supplement. It also encourages the mother to continue the treatment for the child's anemia.
Choice C reason: "You should stop administering the daily iron supplement." is not an appropriate response by the nurse. It is a harmful and incorrect advice that contradicts the prescribed treatment for the child's anemia. Stopping the iron supplement can worsen the child's condition and lead to complications such as growth retardation, cognitive impairment, or heart failure.
Choice D reason: "Don't worry about it." is not an appropriate response by the nurse. It is a dismissive and vague statement that does not address the mother's concern or provide any information or education. It can also undermine the mother's trust and confidence in the nurse and the health care system.

A patient with a severe head injury assumes a posture of flexed arms at the elbows and extended lower legs. The nurse recognizes this posturing as
Explanation
Choice A reason: Decreasing intracranial pressure with decerebrate posturing is not the correct answer. Decerebrate posturing is a sign of severe brain damage that involves the extension and outward rotation of the arms and legs, and the arching of the back. It is not associated with decreasing intracranial pressure, but rather with increased pressure or brainstem compression.
Choice B reason: Increasing intracranial pressure with decorticate posturing is the correct answer. Decorticate posturing is a sign of severe brain damage that involves the flexion of the arms at the elbows and the extension of the legs. It is associated with increased intracranial pressure or lesions in the cerebral hemispheres.
Choice C reason: Decreasing intracranial pressure with decorticate posturing is not the correct answer. Decorticate posturing is a sign of severe brain damage that involves the flexion of the arms at the elbows and the extension of the legs. It is not associated with decreasing intracranial pressure, but rather with increased pressure or lesions in the cerebral hemispheres.
Choice D reason: Increasing intracranial pressure with decerebrate posturing is not the correct answer. Decerebrate posturing is a sign of severe brain damage that involves the extension and outward rotation of the arms and legs, and the arching of the back. It is associated with increased intracranial pressure or brainstem compression, but it is not the posture described in the question.
The nurse is explaining early changes with Parkinson disease to the student nurse. Which statement by the nurse is correct regarding the pathophysiology of the disease?
Explanation
Choice A reason: There is total absence of dopamine at receptors in brain cells controlling motor movement, causing Parkinson symptoms to appear, is not the correct statement. Parkinson disease is not caused by a complete lack of dopamine, but by a gradual loss of dopamine-producing neurons in the substantia nigra, a part of the brain that regulates movement. The symptoms of Parkinson disease, such as tremor, rigidity, and bradykinesia, appear when about 80% of the dopamine neurons are lost.
Choice B reason: There is an excess of dopamine production and deficiency of acetylcholine production, is not the correct statement. Parkinson disease is not caused by an excess of dopamine, but by a deficiency of dopamine. Dopamine is a neurotransmitter that helps to control movement, balance, and coordination. Acetylcholine is another neurotransmitter that works in opposition to dopamine. When dopamine is low, acetylcholine becomes dominant and causes abnormal muscle movements.
Choice C reason: There is a decreased production of dopamine and excess of acetylcholine, is the correct statement. Parkinson disease is caused by a decreased production of dopamine and excess of acetylcholine. This creates an imbalance in the neurotransmitters that regulate movement, leading to the characteristic symptoms of Parkinson disease, such as tremor, rigidity, and bradykinesia.
Choice D reason: There is a deterioration of the myelin sheath of the basal ganglia and the person has tremors, is not the correct statement. Parkinson disease is not caused by a deterioration of the myelin sheath, but by a degeneration of the dopamine neurons. Myelin is a fatty substance that covers the axons of the nerve cells and helps to transmit electrical impulses. The basal ganglia are a group of structures in the brain that are involved in movement, learning, and emotion. Tremors are one of the symptoms of Parkinson disease, but they are not the only or the most specific one.
Which of the following foods would the nurse encourage the client in sickle cell crisis to eat?
Explanation
Choice A (Apples and grapes): While fruits like apples and grapes are generally healthy options, they may not be the best choice for a client in sickle cell crisis. These fruits are high in fiber and may require a significant amount of chewing, which can be challenging for someone experiencing a sickle cell crisis.
Choice B (Popsicles, gelatin, or juice): This choice is the most suitable for a client in sickle cell crisis. During a crisis, it's important to stay hydrated, and these options provide hydration along with easily digestible carbohydrates, which can be beneficial for maintaining energy levels.
Choice C (Beans): While beans are a good source of protein and fiber, they may not be well tolerated during a sickle cell crisis due to their high fiber content.
Choice D (Cheese): Although cheese is a source of protein and calcium, it may not be the best option during a sickle cell crisis, as dairy products can be harder to digest and may not contribute to hydration.
The nurse assesses a patient with a recent spinal cord injury at the level of thoracic 5 vertebrae. The patient's blood pressure is 184/95 mm Hg, has a flushed face and blurred vision. What priority action would the nurse complete first?
Explanation
Choice A reason: Notifying the health care provider of the patient's status is an important action, but not the first priority. The nurse should first assess the patient for any possible triggers of the autonomic dysreflexia, which is a life-threatening condition that occurs in patients with spinal cord injury above the level of T6. It is characterized by a sudden and severe increase in blood pressure, flushing, sweating, headache, and blurred vision.
Choice B reason: Assessing patient for tight clothing around the waist or a full bladder is the first priority action. These are common triggers of autonomic dysreflexia, which cause irritation or stimulation of the nerves below the level of injury. The nurse should remove any tight clothing, catheterize the patient if needed, or perform a bowel evacuation to relieve the pressure and prevent further complications.
Choice C reason: Reviewing the medication administration record for an antihypertensive order is a secondary action, after identifying and removing the trigger of autonomic dysreflexia. The nurse should administer the prescribed antihypertensive medication, such as nifedipine or nitroglycerin, to lower the blood pressure and prevent stroke, seizure, or cardiac arrest.
Choice D reason: Initiating oxygen via a nasal cannula and elevating patient's legs is not an appropriate action for a patient with autonomic dysreflexia. Oxygen therapy is not indicated for this condition, unless the patient has hypoxia or respiratory distress. Elevating the patient's legs can worsen the blood pressure by increasing the venous return and the cardiac output. The nurse should keep the patient in a sitting position to promote the blood flow to the lower extremities and reduce the blood pressure.
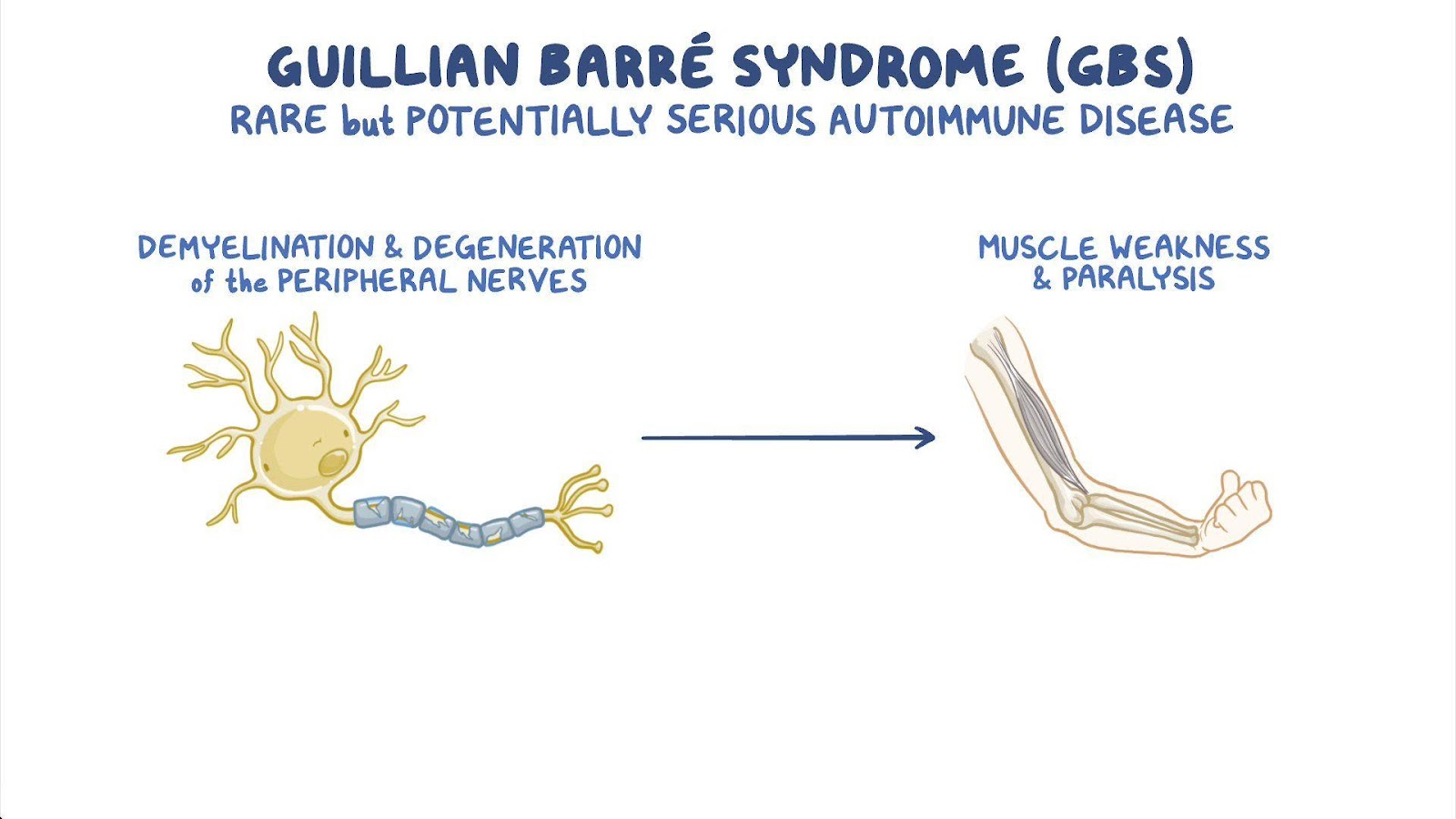
The nurse is preparing a teaching session about Guillain-Barre syndrome. Which statement should be included in the presentation?
Explanation
Choice A reason: The disorder is commonly fatal, is not a true statement. Guillain-Barre syndrome is a rare and serious condition that affects the peripheral nervous system. It causes inflammation and damage to the nerve fibers, leading to muscle weakness, numbness, and paralysis. However, most people recover from Guillain-Barre syndrome, although some may have long-term complications or disabilities. The mortality rate is about 4% to 7%.
Choice B reason: The progressive muscle weakness will begin in the lower extremities and move upward, is a true statement. Guillain-Barre syndrome usually starts with tingling and weakness in the feet and legs, and then spreads to the arms and upper body. This pattern of weakness is called ascending paralysis, and it can affect the breathing, swallowing, and facial muscles. The weakness usually reaches its peak within two to four weeks, and then gradually improves over months or years.
Choice C reason: The disorder is caused by a fungal infection, is not a true statement. Guillain-Barre syndrome is not caused by a fungal infection, but by an abnormal immune response. The exact cause of Guillain-Barre syndrome is unknown, but it is often preceded by an infection, such as a respiratory or gastrointestinal infection, or a vaccination. The immune system mistakenly attacks the nerve fibers, causing inflammation and damage.
Choice D reason: The disorder's most significant manifestations are muscle pain and stiffness, is not a true statement. Guillain-Barre syndrome's most significant manifestations are muscle weakness and paralysis, not pain and stiffness. Muscle pain and stiffness may occur in some cases, but they are not the main symptoms or the most serious ones. The weakness and paralysis can affect the vital functions, such as breathing, blood pressure, and heart rate, and require intensive care and treatment.
When teaching the parents and patients newly diagnosed with beta-thalassemia, which statement made by the parents or patients indicates a need for additional teaching?
Explanation
Choice A reason: Patient should increase daily iron supplements, is a statement that indicates a need for additional teaching. Iron supplements are not recommended for patients with beta-thalassemia, because they already have high levels of iron in their blood due to the frequent blood transfusions. Excess iron can cause damage to the liver, heart, and other organs. Therefore, the patient should avoid iron supplements and foods rich in iron, and take chelation therapy to remove the excess iron from the body.
Choice B reason: Signs and symptoms of infection, is a statement that does not indicate a need for additional teaching. Patients with beta-thalassemia are at risk of developing infections, due to the impaired immune system and the exposure to blood-borne pathogens. Therefore, the patient should be aware of the signs and symptoms of infection, such as fever, chills, sore throat, cough, or skin lesions, and seek medical attention promptly.
Choice C reason: Our child will need to have blood transfusions, is a statement that does not indicate a need for additional teaching. Blood transfusions are the main treatment for patients with beta-thalassemia, because they help to increase the level of hemoglobin and red blood cells, and prevent anemia and its complications. Therefore, the patient should receive regular blood transfusions, usually every two to four weeks, depending on the severity of the condition.
Choice D reason: Swimming is a good activity for our child, is a statement that does not indicate a need for additional teaching. Swimming is a good activity for patients with beta-thalassemia, because it helps to improve the cardiovascular fitness, muscle strength, and joint mobility, and reduce the stress and fatigue. Therefore, the patient should engage in moderate physical activities, such as swimming, walking, or cycling, as tolerated, and avoid strenuous or competitive sports that can cause injury or dehydration.
The nurse is caring for a patient with a head injury after a fall from a ladder. The nurse must evaluate the patient for which signs and symptoms of increased intracranial pressure?
Explanation
Choice A reason: Lethargy is a sign of increased intracranial pressure (ICP), as it indicates a decreased level of alertness and responsiveness due to brain compression¹².
Choice B reason: Slowed responses to verbal cues are a sign of increased ICP, as they indicate a decreased level of cognitive function and communication ability due to brain compression¹².
Choice C reason: Negative Babinski sign is not a sign of increased ICP, as it indicates a normal reflex response of the toes to stimulation of the sole of the foot³. A positive Babinski sign, where the big toe extends upward and the other toes fan out, is a sign of neurological damage, but not necessarily increased ICP³.
Choice D reason: Altered speech is a sign of increased ICP, as it indicates a decreased level of language function and articulation due to brain compression¹².
Choice E reason: Decreased level of consciousness is a sign of increased ICP, as it indicates a decreased level of awareness and arousal due to brain compression¹².
The nurse is caring for an older adult who is confused and restless. The nurse reviews the patient's history and recent complete blood count (CBC). Which finding may best explain the patient's confusion and restlessness?
Explanation
Choice A reason: Decreased hematocrit and hemoglobin indicate anemia, which is a condition where the blood does not carry enough oxygen to the tissues. This can cause symptoms such as confusion, restlessness, fatigue, and weakness in older adults.
Choice B reason: Increased erythrocyte count, or polycythemia, is a condition where the blood has too many red blood cells. This can cause the blood to become thick and viscous, which can impair blood flow and oxygen delivery. However, this is not the best explanation for the patient's confusion and restlessness, as polycythemia usually causes symptoms such as headache, dizziness, itching, and flushing.
Choice C reason: Normochromic red blood cells are red blood cells that have a normal color and hemoglobin content. This is not a finding that would explain the patient's confusion and restlessness, as it indicates a normal red blood cell function.
Choice D reason: Decreased thrombocytes, or platelets, are blood cells that help with clotting. This is a finding that would increase the risk of bleeding, but not the risk of confusion and restlessness. Decreased thrombocytes can cause symptoms such as bruising, bleeding gums, nosebleeds, and petechiae.
A patient had a craniotomy one hour after a motor vehicle accident. The nurse evaluates pupillary response to:
Explanation
Choice A reason: Assessing the patient for potential visual deficits is not the primary purpose of evaluating pupillary response. Visual deficits may result from damage to the optic nerve or the occipital lobe, but they are not directly related to pupillary response.
Choice B reason: Assessing the patient's level of consciousness is an important part of the neurological assessment, but it is not done by evaluating pupillary response alone. Level of consciousness is determined by observing the patient's responsiveness to verbal and physical stimuli, as well as their orientation to person, place, time, and situation.
Choice C reason: Assessing the patient for increased intracranial pressure is the best explanation for evaluating pupillary response. Increased intracranial pressure is a life-threatening condition that can result from brain swelling, bleeding, or infection. It can cause compression of the brainstem and the cranial nerves, leading to changes in pupillary size, shape, and reactivity. Pupillary response is a sensitive indicator of intracranial pressure and brainstem function.
Choice D reason: Assessing the patient for cerebrospinal fluid leakage is not the main reason for evaluating pupillary response. Cerebrospinal fluid leakage can occur after a craniotomy due to a tear in the dura mater, the membrane that covers the brain and spinal cord. It can cause symptoms such as headache, nausea, vomiting, and meningitis. However, it does not affect pupillary response unless it causes increased intracranial pressure.
A patient with acute myelogenous leukemia (AML) asks the nurse why their bones are making more white blood cells when they already have so many. The nurse clarifies that the large number of leukemic white cells they have:
Explanation
Choice A reason: This is not a correct explanation for the large number of leukemic white cells. Leukemic white cells are abnormal white blood cells that do not function properly. They do not attempt to take over the function of the abnormal white blood cells, but rather crowd out the normal ones.
Choice B reason: This is also not a correct explanation for the large number of leukemic white cells. Leukemic white cells do not help to protect against infection, but rather increase the risk of infection. They impair the immune system's ability to fight off bacteria, viruses, and other pathogens.
Choice C reason: This is a partially correct explanation for the large number of leukemic white cells. Leukemic white cells are larger in size than normal white blood cells, and they can clog the bone marrow. This can interfere with the production of other blood cells, such as red blood cells and platelets. However, this is not the only reason for the large number of leukemic white cells.
Choice D reason: This is the best explanation for the large number of leukemic white cells. Leukemic white cells are not as effective as normal white cells to protect against infection, because they are immature and dysfunctional. They do not respond to signals from the immune system, and they do not recognize or destroy foreign invaders. They also prevent the normal white cells from doing their job.
Sign Up or Login to view all the 44 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
