Medical Surgery Exam 2
Total Questions : 43
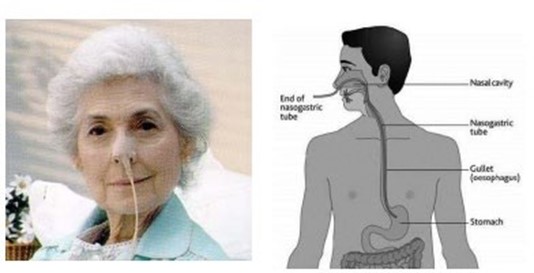
Showing 25 questions, Sign in for moreA patient admitted with a peptic ulcer has a nasogastric (NG) tube in place. When the patient develops sudden, severe upper abdominal pain, diaphoresis, and a firm abdomen, which action should the nurse take?
Explanation
The nurse should quickly assess the patient's vital signs to check for signs of shock and instability. If the vital signs are unstable, the nurse should initiate appropriate interventions to stabilize the patient, such as administering oxygen, starting IV fluids, and providing continuous cardiac monitoring. Based on the sudden onset of severe upper abdominal pain, diaphoresis, and a firm abdomen, the nurse should suspect a possible perforation or bleeding related to the peptic ulcer. This is a medical emergency that requires immediate intervention. Therefore, the nurse should prioritize notifying the healthcare provider and preparing the patient for urgent medical evaluation.
Option A, irrigating the NG tube, is not appropriate in this situation and may further exacerbate the patient's condition if the ulcer has perforated.
Option B, elevating the foot of the bed, is also not appropriate as it does not address the patient's current symptoms.
Option C, giving the ordered antacid, may not be effective in addressing the severity of the patient's symptoms and should be postponed until the healthcare provider has evaluated the patient.
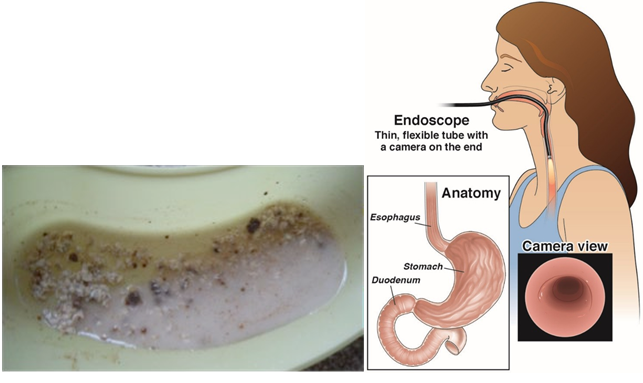
What diagnostic test should the nurse anticipate for an older patient who is vomiting "coffee-ground" emesis?
Explanation
"Coffee-ground" emesis is a term used to describe vomit that has the appearance of coffee grounds, which indicates that the vomit contains partially digested blood. This is a serious symptom that could be indicative of an upper gastrointestinal bleed. An endoscopy is a diagnostic test that allows healthcare providers to visually examine the upper gastrointestinal tract and identify the source of bleeding.
Barium studies and angiography are not typically used to diagnose upper gastrointestinal bleeds. Gastric analysis may be useful in other diagnostic situations, but it is not the most appropriate test for a patient with "coffee-ground" emesis.
A 53-year-old male patient with deep partial-thickness burns from a chemical spill in the workplace has severe pain followed by nausea during dressing changes.
Which action will be most useful in decreasing the patient's nausea?
Explanation
Prochlorperazine is an antiemetic medication that is commonly used to treat nausea and vomiting caused by various conditions, including chemotherapy, radiation therapy, and surgery. Giving the medication before the dressing changes, can prevent or minimize the onset of nausea and vomiting, which can be triggered by the pain and anxiety associated with the procedure.
Option B, keeping the patient NPO (nothing by mouth) for 2 hours before dressing changes, may be helpful in reducing the risk of aspiration if the patient needs sedation or general anesthesia for the procedure. However, it is not directly related to reducing the patient's nausea.
Option C, avoiding performing dressing changes close to the patient's mealtimes, may help reduce the risk of nausea caused by an overly full stomach, but it is not directly related to reducing the patient's nausea during the procedure.
Option D, administering prescribed morphine sulfate before dressing changes, may help reduce the patient's pain during the procedure, but it may also increase the risk of nausea and vomiting as a side effect. Therefore, this option may not be the most useful in decreasing the patient's nausea.
A 26-year-old woman is being evaluated for vomiting and abdominal pain. Which question from the nurse will be most useful in determining the cause of the patient's symptoms?
Explanation
Nausea and vomiting are common symptoms of early pregnancy, and abdominal pain can also occur due to various pregnancy-related conditions. Therefore, it is essential to rule out pregnancy as a potential cause of the patient's symptoms before pursuing other diagnostic options.
Once pregnancy has been ruled out, the nurse can ask additional questions such as those listed in options a, b, and d to further narrow down the potential causes of the patient's symptoms.

Which information will the nurse include when teaching a patient how to avoid chronic constipation? (Select all that apply.)
Explanation
Option b is not entirely correct because while bulk-forming laxatives contain fiber, they may not always be the best source of fiber, and their use should be individualized according to the patient's needs.
Option e is incorrect because while stimulants and saline laxatives can be effective for occasional constipation, they should not be used regularly or for an extended period without medical supervision as they can lead to dependence and other complications.

A patient calls the clinic to report a new onset of severe diarrhea. What should the nurse anticipate that the patient will need to do?
Explanation
The nurse should anticipate that the patient will need to collect a stool specimen. Diarrhea can be caused by various factors such as infections, inflammatory bowel disease, food intolerance, and medication side effects. Collecting a stool specimen can help identify the underlying cause of the diarrhea and guide appropriate treatment. Blood cultures, colonoscopy but barium enema may be necessary in certain cases but are not typically the first step in the diagnostic process for diarrhea.
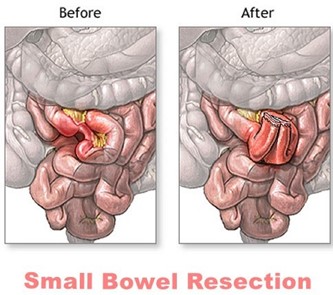
A patient reports gas pains and abdominal distention 2 days after a small bowel resection. Which nursing action should the nurse take?
Explanation
Gas pains and abdominal distention are common postoperative complications following small bowel resection. Ambulation is a simple and effective nursing intervention that can help alleviate these symptoms. Walking helps stimulate peristalsis, which can help move gas and stool through the gastrointestinal tract. It can also help prevent postoperative complications such as pneumonia and deep vein thrombosis.
Administering morphine sulfate (option A) may relieve pain, but it can also worsen constipation and abdominal distention. Promethazine (option C) is an antiemetic medication and may be helpful if the patient is experiencing nausea, but it is not the best intervention for gas pain and abdominal distention. Instilling a mineral oil retention enema (option D) may also be helpful in some cases, but it is not typically the first intervention for these symptoms and should be ordered by a healthcare provider.
A 68-year-old female client is being seen for follow-up wound care on her right lower leg. During her visit, the client states she hasn't had a bowel movement since her last visit a week ago. The client states she hasn't had much of an appetite in the past few days and says, "l figure I don't have anything in there to come out." The nurse auscultates the client's abdomen and hears hyperactive high-pitched bowel sounds in the upper left quadrant and hypoactive bowel sounds in the lower left quadrant. The nurse collaborates with the primary health care provider and the client is directly admitted to the hospital for possible intestinal obstruction. Before going to the hospital, the client asks the nurse what to expect. Which of these statements by the nurse (is) most likely accurate?
Select all that apply.
Explanation
Option A is not the best advice because drinking lots of water alone may not be enough to relieve constipation, especially if there is an obstruction.
Option B is also not accurate because not all intestinal obstructions require surgery, and the treatment approach will depend on the cause and severity of the obstruction.
Option C is accurate because a nasogastric tube can help relieve any distention caused by the obstruction by removing any gas or fluids that may have accumulated in the stomach and small intestine.
Option D is also accurate because an abdominal CT is one of the diagnostic tests that can help confirm the presence of intestinal obstruction and provide information about the location and cause of the obstruction.

A young adult patient is admitted to the hospital for evaluation of right lower quadrant abdominal pain with nausea and vomiting. Which action should the nurse take?
Explanation
The nurse should suggest the patient lie on the side, flexing the right leg². This position may help relieve pain and reduce tension in the abdominal muscles¹. Palpating the abdomen for rebound tenderness (a) may cause pain and should be avoided¹. Assisting the patient to cough and deep breathe (c) may be helpful for respiratory issues but not for abdominal pain¹. Encouraging the patient to sip clear, non-carbonated liquids (d) may be helpful for hydration but does not address the abdominal pain¹.

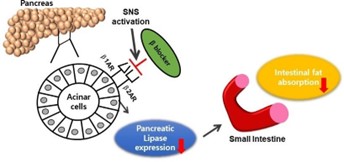
Which laboratory test result will the nurse monitor to evaluate the effects of therapy for a patient who has acute pancreatitis?
Explanation
Lipase is an enzyme that is produced by the pancreas and is involved in the digestion of fats. In acute pancreatitis, the pancreas becomes inflamed, and lipase levels in the blood can become significantly elevated. Monitoring lipase levels can help healthcare providers to assess the severity of pancreatitis, track the effectiveness of treatment, and determine when it is safe to start a patient on a normal diet.
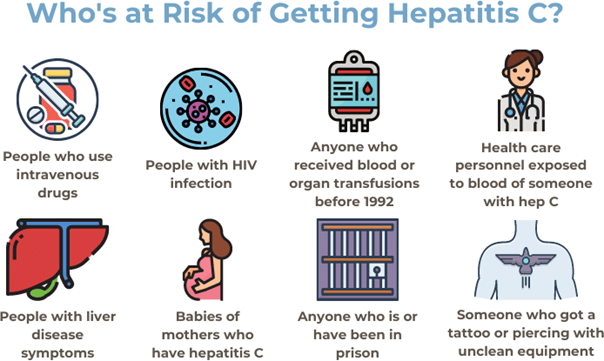
Which information from a 70-year-old patient during a health history indicates to the nurse that the patient should be screened for hepatitis C?
Explanation
Intravenous drug use is a significant risk factor for hepatitis C transmission. The other options are not necessarily related to hepatitis C transmission. However, having a blood transfusion before 1992 or receiving an organ transplant before 1992, having a history of receiving blood products or clotting factor concentrates before 1987, and having been born to a mother with hepatitis C are also considered significant risk factors for hepatitis C transmission.
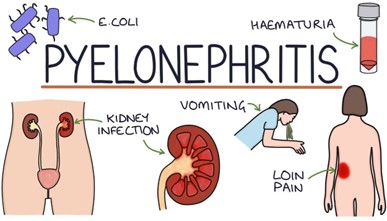
Which finding by the nurse will be most helpful in determining whether a 67- yr-old patient with benign prostatic hyperplasia has an upper urinary tract infection (pyelonephritis)?
Explanation
The most helpful finding by the nurse in determining whether a 67-yr-old patient with benign prostatic hyperplasia has an upper urinary tract infection (pyelonephritis) would be
**costovertebral tenderness**⁴. This is because costovertebral tenderness is a common symptom of pyelonephritis⁵. Pyelonephritis is an infection of the upper urinary tract that can cause fever, chills, flank pain, nausea, vomiting, and costovertebral tenderness⁵. Foul-smelling urine and bladder distention are not specific symptoms of pyelonephritis⁵. Suprapubic discomfort can be a symptom of lower urinary tract infection⁵.
14:20: 87-year-old client admitted to the ED from the independent living apartment with a new report of episodic acute confusion. urinary frequency and incontinence, and severe fatigue. The child states that the client is independent in ADCs and has no history of dementia.
15:30: Normal BMP and CBC results, except for WBCs of 16,000/mm3 (16 x 109 /L) with bands greater than 10%.
Based on the assessment findings presented which condition would the nurse suspect?
Explanation
Based on the assessment findings presented, the nurse would suspect a urinary tract infection (UTI). The client's symptoms of acute confusion, urinary frequency and incontinence, and elevated WBC count with bands suggest a possible infection. Dehydration or diabetic ketoacidosis could also cause confusion and fatigue, but these conditions are less likely given the normal BMP and CBC results.
Hepatitis would not typically present with these specific symptoms.
What is the rational for IV fluids in a patient with a UT!?
Explanation
IV fluids are not typically used as a treatment for UTIs (urinary tract infections) as they do not directly address the infection itself. The main reason for administering IV fluids to a patient with a UTI would be to ensure adequate hydration, especially if the patient is experiencing fever or other symptoms of dehydration. Adequate hydration can also help improve the efficacy of antibiotics in treating the infection by ensuring that the urinary system is properly functioning and able to flush out bacteria.
Therefore, option b would be the closest answer as IV fluids may be given to facilitate the administration of IV antibiotics. However, it is important to note that antibiotics are the primary treatment for UTIs, and IV fluids are usually given as a supportive measure to ensure the patient's overall well-being. Flushing bacteria from the urinary tract or diluting bacteria are not considered primary rationales for administering IV fluids in a patient with a UTI. Relief of pain and discomfort may be managed with pain medication, but this is not the primary reason for IV fluid administration.
Which information will the nurse include when teaching the patient with a urinary tract infection (UTI) about the use of phenazopyridine?
Explanation
The nurse should explain to the patient that phenazopyridine is a medication that can help relieve the pain, burning, and urgency associated with UTIs. However, it does not treat the underlying infection. The nurse should also instruct the patient to take the medication as prescribed by the healthcare provider and inform them that the medication may turn their urine an orange or red color, which is a harmless and expected side effect.
The nurse should also inform the patient that taking phenazopyridine before sexual intercourse is not recommended and that the medication should be taken as directed by the healthcare provider.
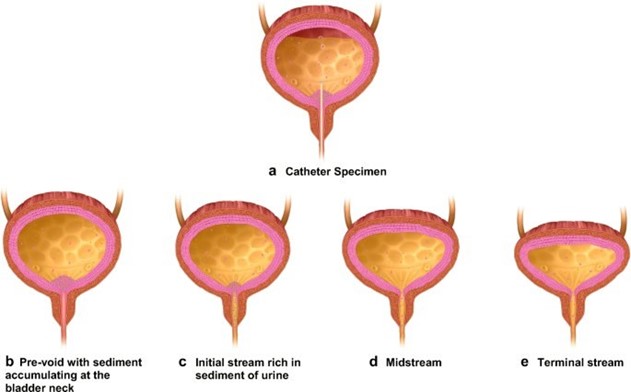
A 46-year-old female patient returns to the clinic with continued dysuria after being treated with trimethoprim and sulfamethoxazole for 3 days. Which action will the nurse plan to take?
Explanation
This is because the persistent dysuria suggests that the initial treatment was not effective, and there may be a possibility of a resistant organism. Obtaining a midstream urine specimen for culture and sensitivity testing will help identify the specific microorganism causing the infection and determine the most effective antibiotic to use. The nurse should also instruct the patient to continue to drink plenty of fluids, as this will help flush out the bacteria and relieve symptoms. The nurse may suggest the use of acetaminophen (Tylenol) to relieve discomfort, but this should not be the only action taken, as treating the underlying infection is crucial. The nurse should not tell the patient to take trimethoprim and sulfamethoxazole for an additional three days, as the initial treatment was not effective, and a different course of treatment may be required based on the results of the urine culture and sensitivity testing.
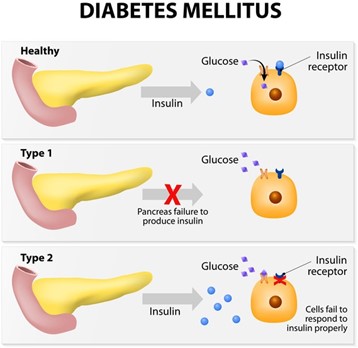
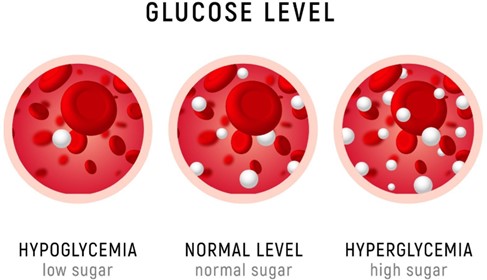
A 46-year-old woman presented to the emergency department several days ago with a respiratory infection that caused a hyperglycemic-hyperosmolar event. The client has a history of diabetes mellitus type 2, hypertension, peripheral neuropathy, vascular disease, and retinopathy. The nurse prepares to discharge the client today. After providing discharge instructions, the nurse assesses the client's understanding.
Which of the following client statements indicate a good understanding of diabetic teaching?
Select all that apply.
Explanation
Option A indicates that the client understands the timing of glyburide administration, which is typically taken with the first bite of a meal to aid in glucose control.
Option d indicates that the client understands the importance of continuing antidiabetic medications even when they are sick. Skipping doses during illness can lead to uncontrolled blood glucose levels.
Option e indicates that the client understands the importance of foot care in preventing complications related to peripheral neuropathy, such as diabetic foot ulcers.
Option b is incorrect because patients with peripheral neuropathy should not walk barefoot, as they may not feel injuries to their feet, which can lead to diabetic foot ulcers and other complications.
Option c is incorrect because antidiabetic medications do not allow patients to eat whatever they desire. Patients with diabetes need to follow a healthy diet and exercise plan to manage their blood glucose levels effectively.
A hospitalized patient who is diabetic received 38 U of NPH insulin at 7:00 AM. At 1:00 PM, the patient was away from the nursing unit for 2 hours, missing the lunch delivery while awaiting a chest x-ray.
What is the best action by the nurse to prevent hypoglycemia?
Explanation
The patient received 38 U of NPH insulin at 7:00 AM, and by 1:00 PM, the insulin has been active for approximately 6 hours. The patient has missed lunch, which may lead to hypoglycemia, especially with the activity of the insulin.
Sending a glass of orange juice will provide the patient with a quick source of glucose to prevent hypoglycemia. If testing is further delayed, the nurse may request that the patient be allowed to eat lunch first or save the lunch tray for later, but immediate intervention is necessary to prevent hypoglycemia. Discontinuing the evening dose of insulin is not an appropriate action and should not be considered without consulting the healthcare provider.
Which action by the patient who is self-monitoring blood glucose indicates a need for additional teaching?
Explanation
When performing a self-monitoring blood glucose test, it is essential to choose the puncture site on the side of the fingertip, slightly off-center, and to rotate the puncture sites to prevent lipoatrophy and injury to the nerves and blood vessels in the finger. Puncturing the center of the fingertip can lead to pain, injury to the nerves, and tissue damage.
Options a, b, and c are correct and indicate appropriate actions during self-monitoring of blood glucose. Washing the puncture site using warm water and soap helps to reduce the risk of infection. Waiting for a minute with the arm down before puncturing the site helps to increase blood flow and make it easier to obtain a blood sample. A blood glucose result of 120 mg/dL indicates good blood sugar control within the target range for many patients with diabetes.

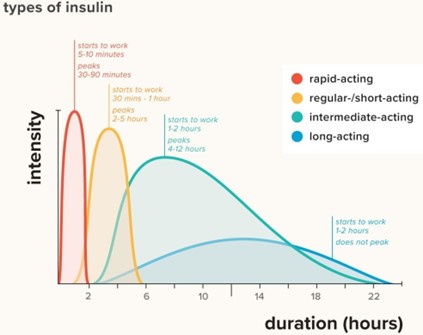
Insulin lispro (Humalog) is what type of insulin?
Explanation
Yes, that's correct. Insulin lispro (Humalog) is a rapid-acting insulin, which means it begins to work quickly after injection, usually within 15 minutes, and it peaks in about 1 to 2 hours. It typically lasts for 3 to 4 hours in the body.

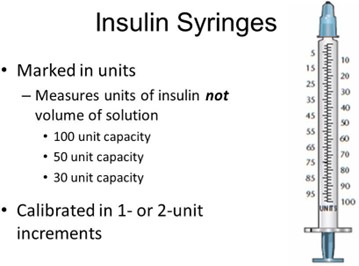
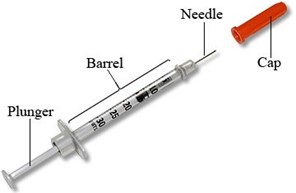
An insulin syringe is measured in which of the following?
Explanation
An insulin syringe is measured in units (U). The concentration of insulin is usually expressed in units per milliliter (U/mL), and the volume of the syringe is also measured in milliliters (mL), but the actual dosing of insulin is in units. It is important to use the correct syringe size and to measure the correct number of units to ensure accurate dosing of insulin.
The nurse is preparing to teach a 43-year-old man who is newly diagnosed with type 2 diabetes home management of the disease. Which action should the nurse take first?
Explanation
The correct action for the nurse to take first when preparing to teach a newly diagnosed 43-year-old man with type 2 diabetes home management of the disease is to assess the patient's perception of what it means to have diabetes. This will help the nurse to identify any misconceptions or fears the patient may have about the condition, and tailor the education to meet the patient's specific needs. Options A, C, and D are important components of diabetes education but can be addressed after the nurse has assessed the patient's perception of the disease.
A patient with diabetes is starting insulin therapy. Which type of insulin will the nurse discuss using for mealtime coverage.
Explanation
The nurse will discuss using rapid-acting insulin such as Lispro (Humalog) for mealtime coverage in a patient with diabetes who is starting insulin therapy. Rapid-acting insulin begins to work quickly after injection, usually within 15 minutes, and peaks at around 1 hour. This makes it an effective choice for covering the rise in blood sugar that occurs after meals.
Options A, B, and D are all long-acting insulins that are used to provide a basal level of insulin coverage throughout the day but are not appropriate for mealtime coverage.
A patient with diabetic ketoacidosis is brought to the emergency department. Which prescribed action should the nurse implement first?
Explanation
Diabetic ketoacidosis (DKA) is a serious complication of diabetes that occurs when the body produces high levels of blood acids called ketones. The initial management of DKA involves fluid resuscitation with intravenous normal saline to correct dehydration and electrolyte imbalances. Therefore, starting an infusion of normal saline at 125 ml/hr is the first prescribed action the nurse should implement.
Bringing the patient a meal is not a priority at this time because the patient's blood glucose levels need to be stabilized before they can safely consume food. Administering Lantus insulin IV and giving sodium bicarbonate 50 mEq IV push are also not the first-line treatments for DKA. Lantus insulin is a long-acting insulin used to treat hyperglycemia over an extended period and should not be given intravenously. Sodium bicarbonate may be used to correct acidosis, but it is not the first priority in DKA management.
The nurse is caring for a patient with newly diagnosed type I diabetes. What information is essential to include inpatient teaching before the patient is discharged from the hospital?
(Select all that apply)
Explanation
Use of a portable blood glucose monitor: The patient should be taught how to use a portable blood glucose monitor to check their blood glucose levels at home. This will help the patient monitor their blood glucose levels and adjust their insulin dose as necessary.
Hypoglycemia prevention, symptoms, and treatment: The patient should be taught about the signs and symptoms of hypoglycemia (low blood glucose levels) and how to treat it. This includes teaching the patient to consume 15-20 grams of fast-acting carbohydrates such as glucose tablets or juice when experiencing hypoglycemia.
Insulin administration: The patient should be taught how to administer insulin, including the timing of injections and rotating injection sites. The patient should also be educated about the importance of taking insulin regularly and the potential consequences of missed doses.
Diet: The patient should be educated about healthy eating habits that include monitoring carbohydrate intake, eating regular meals, and spacing carbohydrates throughout the day. The patient does not need to eliminate sugar entirely from their diet, but rather to consume it in moderation and balance it with other food groups.
Physical activity: The patient should be encouraged to engage in regular physical activity but may need to adjust their insulin dose or carbohydrate intake to accommodate for the changes in blood glucose levels that may result from physical activity. Reducing physical activity is not necessary, but rather adjusting to it properly with proper monitoring of glucose levels.
Sign Up or Login to view all the 43 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
