Mental and Behavioural nursing
Total Questions : 55
Showing 25 questions, Sign in for moreWho initiated psychoanalytical therapy as a treatment to assist in understanding the defense mechanism?
Explanation
Sigmund Freud was an Austrian neurologist who developed psychoanalytic theory and therapy in the late 19th and early 20th centuries. He believed that unconscious thoughts, feelings, and experiences from childhood could influence behavior and mental health in adulthood. Psychoanalytic therapy is a type of talk therapy that aims to bring these unconscious thoughts and experiences to the surface, in order to help patients gain insight into their behavior and mental health.
Defence mechanisms are psychological strategies that individuals use unconsciously to protect themselves from anxiety and emotional pain. Freud identified several defense mechanisms, including repression, denial, projection, and displacement. Psychoanalytic therapy is designed to help patients identify and understand these defense mechanisms, in order to develop healthier coping strategies.
Dorothea Dix was a social reformer who advocated for the humane treatment of the mentally ill. Erick Erickson was a developmental psychologist who developed a theory of psychosocial development.
Hildegard Peplau was a nurse theorist who developed a theory of interpersonal relationships in nursing. None of these individuals were associated with the development of psychoanalytic therapy.
A county in Florida was just devastated by a major hurricane. Community mental health nurses have been sent to the area to provide intervention. What type of prevention strategy is this?
Explanation
Tertiary prevention refers to interventions that are designed to reduce the impact of an ongoing illness or injury that has lasting effects. In this case, community mental health nurses have been sent to the area to provide intervention after a major hurricane has already occurred. Their goal is to help individuals and communities recover from the traumatic event and reduce the long-term impact on their mental health
The nurse states, “I will stay with you until you go for your electro compulsive therapy (ECT) treatment.” Which of the following therapeutic communication techniques is being demonstrated?
Explanation
Offering self is a therapeutic communication technique where the healthcare professional offers their presence, support, and assistance to the patient. By stating that they will stay with the patient until their ECT treatment, the nurse is offering their presence and support to the patient during a potentially stressful and anxiety-provoking time. This technique can help the patient feel more comfortable and supported, which can help build trust and rapport between the patient and the healthcare professional.
Accepting involves acknowledging the patient's feelings and accepting them without judgment. Giving recognition involves acknowledging the patient's efforts and accomplishments. Formulating a plan involves working with the patient to develop a plan of action for addressing their health concerns. None of these techniques are being demonstrated in this scenario.
An experienced nurse is observing a newly licensed nurse as she interacts with a client regarding his concerns about his relationship with his partner. Which of the following statements by the newly licensed nurse requires intervention by the experienced nurse?
Explanation
You should try to see your partner's point of view before your own**. This statement by the newly licensed nurse requires intervention by the experienced nurse because it is not therapeutic and does not demonstrate empathy or active listening. Instead of offering advice or telling the client what to do, the nurse should focus on understanding the client's concerns and feelings and helping them explore their options.
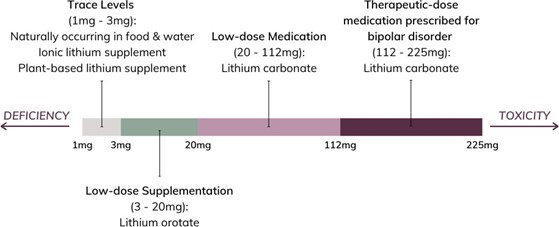
A nurse is preparing to administer lithium syrup 1800 mg PO bd Available is lithium syrup 600 mg/5 mL How many mL would the nurse administer per dose?
(Write the number only, do not include the label Record the answer as a whole number Use a leading zero if it applies Do not use a trailing zero)
Explanation
The nurse would administer 15 mL of lithium syrup per dose. This is calculated by first determining the amount of lithium in each mL of syrup: 600 mg / 5 mL = 120 mg/mL. Then, the desired dose of 1800 mg is divided by the concentration of lithium in each mL of syrup: 1800 mg / (120 mg/mL) = 15 mL.
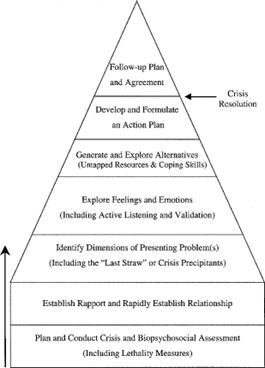
A nurse caring for a client is preparing to access the client’s implanted medication port (Medi port). The client states, “Every time I have to have my port accessed, I get extremely anxious, and I have heart palpitations.” Which response by the nurse would be most appropriate for the assessment stage of crisis intervention?
Explanation
This response by the nurse would be most appropriate for the assessment stage of crisis intervention because it focuses on understanding the client’s past experiences and coping mechanisms. By asking the client about what has worked for them in the past, the nurse can help the client identify and use effective strategies to manage their anxiety during the procedure.
A nurse is leading a family therapy session for a mother, father, and two adolescent siblings. Which of the following statements should the nurse recognize as an example of manipulating?
Explanation
Explanation: Manipulation involves using indirect, underhanded, or deceptive tactics to control or influence others. In this statement, the speaker is using a veiled threat to control the behavior of another person.
This is an example of manipulative behavior, and the nurse should recognize it as such.
Option A is an example of a statement seeking clarification, not manipulation. The sibling is asking a question about the behavior of the other sibling.
Option Ais an example of a statement aimed at understanding the other person's behavior, not manipulation.
Option Cis an example of taking responsibility for one's actions and setting boundaries, not manipulation
To address the client’s cultural needs, which of the following nursing actions would be most appropriate?
Explanation
To address the client’s cultural needs, the most appropriate nursing action would be to ask the client directly about their specific cultural needs and preferences. This allows the nurse to provide care that is tailored to the individual client and respects their cultural beliefs and practices.
While working with a client in crisis, the nurse understands which of the following interventions would be a priority.
Explanation
working with a client in crisis, the nurse’s priority intervention should be to ensure the client’s safety. This involves assessing the client’s risk for harm to themselves or others and taking appropriate measures to prevent harm. Once the client’s safety has been ensured, the nurse can then focus on other interventions such as decreasing the client’s anxiety and identifying previous experiences and coping methods used.
Which of the following terms could be used to describe and document a client’s motor activity on a mental health assessment?
Explanation
These terms could be used to describe and document a client’s motor activity on a mental health assessment. Tics are involuntary movements or vocalizations that are sudden, rapid, and repetitive. Restlessness refers to an inability to sit still or remain calm due to physical or emotional discomfort. Echopraxia is the involuntary repetition or imitation of another person’s movements. Flat and guilty are not terms used to describe motor activity.
A nurse is caring for a client who is having an adverse medication reaction. The client states “The nurse told me not to drink when taking the medication, but she didn’t tell me having one drink could cause a problem.” The nurse should recognize that the client is exhibiting which of the following defense mechanisms?
Explanation
The client is exhibiting the defence mechanism of rationalization, which involves justifying or explaining one’s behavior or feelings in a seemingly logical manner to avoid the true explanation. In this case, the client is rationalizing their decision to drink while taking medication by blaming the nurse for not providing enough information, rather than taking responsibility for their own actions.
A victim of violence comes to the crisis center seeking help. The nurse uses crisis intervention strategies that focus on which of the following?
Explanation
Crisis intervention strategies aim to help individuals cope with and recover from a traumatic event or crisis. The first step in crisis intervention is to establish a sense of emotional security and safety for the individual. This can involve providing emotional support, active listening, and empathetic communication.
While the long-term resolution of issues and promotion growth of the individual may be important goals of crisis intervention, they are not the immediate focus. Crisis intervention is designed to address the immediate needs of the individual and help them stabilize their emotions and regain a sense of control.
Providing legal assistance may be necessary in some cases, but it is not typically a primary focus of crisis intervention. The immediate priority is to address the individual's emotional needs and help them access any necessary medical or mental health services.
A nurse is speaking to the family of a Trauma victim. The nurse is blocking out the siren and alarm noises while speaking with the client’s family. They ask,” How can you be so calm and focused with all this noise going on?” The nurse is practicing which defense mechanism?
Explanation
Disassociation is a defense mechanism that involves mentally separating oneself from a stressful or traumatic situation in order to maintain a sense of calm and focus. In this scenario, the nurse is able to block out the sirens and alarms, which may be causing stress and anxiety, and maintain a calm and focused demeanor while speaking with the client's family. This is an adaptive use of disassociation because it allows the nurse to provide effective care and support to the family despite the chaotic environment.
Denial is a defense mechanism that involves denying or minimizing the existence of a stressful or traumatic situation. Rationalization involves justifying or excusing one's behavior or actions. Altruism involves selflessly helping others as a way of dealing with one's own problems. In this scenario, none of these defense mechanisms are being used by the nurse.
What is the name of the defense mechanism when a client channel drives or impulses that are unacceptable into constructive activities?
Explanation
Sublimation is a defense mechanism in which socially unacceptable impulses or drives are redirected into socially acceptable activities or behavior. For example, someone who has aggressive tendencies may channel those impulses into playing competitive sports, or someone who has sexual desires may channel those impulses into creative work like painting or writing.
Regression refers to a defense mechanism where an individual retreats to an earlier stage of development, such as acting like a child when under stress. Undoing is a defense mechanism in which an individual tries to undo or negate a previous action or thought, such as making up for a mistake by performing a good deed. Suppression is a defense mechanism where an individual consciously avoids thinking about or dealing with certain thoughts or emotions.

A client states that she is returning to school next semester and has some concerns. Which of the following is the most therapeutic response by the nurse?
Explanation
This response encourages the client to share her thoughts and concerns about returning to school, which can help the nurse to understand the client's perspective and provide support and guidance as needed. It also shows that the nurse is actively listening and interested in what the client has to say, which can help to build trust and rapport in the therapeutic relationship.
Responses a and b are positive but not necessarily helpful in addressing the client's concerns.
Response c is potentially intrusive and could make the client feel uncomfortable or judged.
The nurse places a client In the seclusion room until he admits responsibility for the fight In the day room. The nurse's action could be viewed as which of the following?
Explanation
The nurse’s action of placing the client in the seclusion room until he admits responsibility for the fight in the day room could be viewed as false imprisonment. False imprisonment is the unlawful restraint of a person against their will. In this case, the nurse is using the seclusion room to restrain the client against their will and is conditioning their release on admitting responsibility for the fight, which could be considered unlawful.
In a treatment team planning meeting, a nurse states her concern about whether staff are behaving ethically in using restraints to prevent one client from engaging in self-mutilating behavior while for another self-mutilation client, the care plan calls for one-on-one suspension. Which ethical principle governs this situation?
Explanation
The ethical principle of justice governs this situation. Justice refers to the fair and equal treatment of all individuals. In this case, the nurse is concerned about whether staff are behaving ethically by using different approaches to prevent self-mutilation in two different clients. The principle of justice would require that both clients receive fair and equal treatment based on their individual needs and circumstances.
Which nursing intervention constitutes false imprisonment?
Explanation
A client has been seeking the attention of the nurses at the nurse’s station much of the day. The nurse escorts him to this room and tells him to stay there or he will be put into seclusion.
This nursing intervention constitutes false imprisonment because it involves unlawfully restraining the client against their will. In this case, the nurse is using the threat of seclusion to coerce the client into staying in their room, which could be considered unlawful restraint.
The primary reason a client should be included in their treatment plan, if possible, would be for which of the following purposes?
Explanation
It is important for a client to be included in their treatment plan if possible because it allows them to have a say in their own care and to work together with their healthcare team to set achievable goals and objectives. This can help improve the client’s engagement and motivation in their treatment and can lead to better outcomes.
A client was involuntarily admitted to a behavioral health facility after trying to harm himself. Which statement by the client would indicate further education is needed regarding his rights?
Explanation
This statement indicates a lack of understanding about the legal basis for involuntary admission and the criteria for discharge. Involuntary admission is authorized when a person is a danger to themselves or others or is gravely disabled, and the decision to discharge must be based on an evaluation by a qualified professional that the person no longer meets those criteria. Therefore, the client cannot simply leave by telling staff they will not harm themselves. The other options are not indicative of a lack of understanding of the client’s rights.
Option A may indicate a concern about privacy, but the confidentiality of mental health information is protected by law, so the client's boss cannot be informed without their consent.
Option B shows an understanding of the reason for the use of restraints.
Option Ddemonstrates awareness of the right to vote, which is not affected by mental health status.
A nurse is caring for a client admitted to a mental health facility who asks. “Can I refuse the Electroconvulsive Therapy (ECT) treatment scheduled for tomorrow?” Which is the appropriate answer for the nurse?
Explanation
Every patient has the right to refuse treatment, including Electroconvulsive Therapy (ECT), even if they previously provided consent. The nurse should respect the client's autonomy and inform the client of their right to refuse the treatment, even if the healthcare provider believes it is necessary. It is important for the nurse to discuss the potential risks and benefits of the treatment with the client to make an informed decision. The nurse should also document the client's decision and communicate it with the healthcare provider.
A client is concerned that information given to the nurse remains confidential. Which is the nurse’s best response regarding confidentiality?
Explanation
Confidentiality is a critical aspect of the nurse-patient relationship. However, there are specific circumstances where confidentiality must be breached to ensure the patient's safety and well-being. For instance, if a patient is expressing suicidal ideation or harm to others, the nurse has an ethical and legal obligation to report it to the treatment team to prevent harm. It is essential to explain this to the client to establish trust and clarify the limitations of confidentiality.
Option (a) is incorrect because not all information can remain confidential.
Option (b) is incorrect because not all information requires the client's approval to share.
Option (d) is incorrect because the nurse has the responsibility to disclose certain information to other healthcare professionals for the patient's benefit.
A nurse is admitting a client to the psychiatrist unit after attacking a neighbor. The nurse should know that the client can be kept in the hospital after the 72 hours hold is over when which of the following conditions is met?
Explanation
A client can be kept in the hospital after the initial 72-hour hold if they are deemed to be a threat to themselves or others. This determination is typically made by a mental health professional who evaluates the client’s behavior and mental state. If the client is considered to be a danger, they may be held involuntarily for further treatment and observation.
The client expresses the loneliness she feels to the nurse. Which response by the nurse demonstrates the existence of a therapeutic relationship?
Explanation
Option c demonstrates empathy and understanding toward the client's feelings, which is an essential component of a therapeutic relationship. It acknowledges the client's emotions, validates their experience, and provides support to the client. In contrast, options a and d suggest a solution or an activity to the client, which may not be what the client needs now.
Option b is directive and may make the client feel judged or inadequate.
Therefore, option c is the best response that demonstrates the existence of a therapeutic relationship between the client and the nurse.
The nurse used the term “labile” in describing a client’s mood and behavior. What does this term indicate?
Explanation
The term “labile” means that something is unstable or constantly changing. In the context of mood and behavior, it indicates that the client’s mood and behavior are unpredictable and subject to rapid changes.
Received message. The correct answer is d. The client has mood swings and is unpredictable. The term "labile" means that something is unstable or constantly changing. In the context of mood and behavior, it indicates that the client's mood and behavior are unpredictable and subject to rapid changes.
Sign Up or Login to view all the 55 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
