NS117 T Winter 2023 Monroe college NY PN Fundamental of nursing exam 2
Total Questions : 43
Showing 25 questions, Sign in for moreA nurse is caring for a client who has COPD. The nurse should identify that the client is at risk for which of the following acid-base imbalances?
Explanation
Choice A reason: Metabolic alkalosis is a condition in which the blood pH is elevated due to an excess of bicarbonate or a loss of acid. It can be caused by vomiting, diuretics, or excessive antacid intake. It is not associated with COPD.
Choice B reason: Respiratory acidosis is a condition in which the blood pH is lowered due to an accumulation of carbon dioxide. It can be caused by hypoventilation, airway obstruction, or lung diseases such as COPD. It is the most common acid-base imbalance in COPD patients.
Choice C reason: Respiratory alkalosis is a condition in which the blood pH is elevated due to a loss of carbon dioxide. It can be caused by hyperventilation, anxiety, fever, or aspirin overdose. It is not common in COPD patients.
Choice D reason: Metabolic acidosis is a condition in which the blood pH is lowered due to an excess of acid or a loss of bicarbonate. It can be caused by diabetic ketoacidosis, renal failure, or lactic acidosis. It is not directly related to COPD.
A nurse is preparing to insert an indwelling urinary catheter for a client. Which of the following actions should the nurse plan to take?
Explanation
Choice A reason: Donning sterile gloves is an essential step to prevent contamination and infection during the insertion of an indwelling urinary catheter. The nurse should also use aseptic technique and a sterile catheter kit.
Choice B reason: Applying an oil-based lubricant to the indwelling urinary catheter is not recommended, as it can damage the latex material and increase the risk of catheter-associated urinary tract infection (CAUTI). The nurse should use a water-soluble lubricant instead.
Choice C reason: Testing the balloon on the indwelling urinary catheter before insertion is a good practice, as it ensures that the balloon is functioning properly and does not leak or burst. The nurse should inflate and deflate the balloon with sterile water or saline using a syringe.
Choice D reason: Using one cotton swab to clean the client's urinary meatus is not sufficient, as it may not remove all the bacteria and debris. The nurse should use at least three cotton swabs and clean the meatus from front to back in a circular motion. The nurse should also use an antiseptic solution such as chlorhexidine or povidone-iodine.
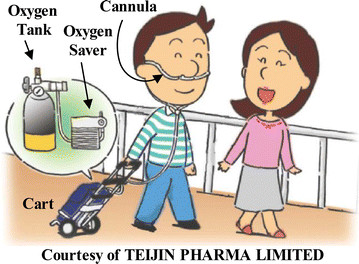
A nurse is reinforcing teaching with a client who has a prescription for home oxygen therapy. Which of the following instructions should the nurse include?
Explanation
Choice A reason: Storing oxygen tanks upright is not a necessary instruction for home oxygen therapy. Oxygen tanks can be stored horizontally or vertically, as long as they are secured and away from heat sources.
Choice B reason: Using petroleum-based ointments to moisturize lips is not advisable for clients who use home oxygen therapy. Petroleum-based products can ignite in the presence of oxygen and cause burns. The nurse should recommend water-based products instead.
Choice C reason: Keeping oxygen tanks 4 feet away from an electric stove is a safety measure for home oxygen therapy. Oxygen is a flammable gas and can cause a fire or explosion if exposed to heat or sparks. The nurse should also instruct the client to avoid smoking, candles, and other open flames.
Choice D reason: Choosing a wool blanket when using oxygen is not a good idea for home oxygen therapy. Wool is a synthetic material that can generate static electricity and ignite oxygen. The nurse should suggest cotton or other natural fabrics instead.
A nurse is caring for a client who has nausea and is vomiting. The nurse should identify that the client is at risk for which of the following acid-base imbalances?
Explanation
Choice A reason: Metabolic alkalosis is a condition in which the blood pH is elevated due to an excess of bicarbonate or a loss of acid. It can be caused by nausea and vomiting, as they result in the loss of gastric acid and the retention of bicarbonate.
Choice B reason: Respiratory acidosis is a condition in which the blood pH is lowered due to an accumulation of carbon dioxide. It can be caused by hypoventilation, airway obstruction, or lung diseases. It is not related to nausea and vomiting.
Choice C reason: Metabolic acidosis is a condition in which the blood pH is lowered due to an excess of acid or a loss of bicarbonate. It can be caused by diabetic ketoacidosis, renal failure, or lactic acidosis. It is not caused by nausea and vomiting.
Choice D reason: Respiratory alkalosis is a condition in which the blood pH is elevated due to a loss
carbon dioxide. It can be caused by hyperventilation, anxiety, fever, or aspirin overdose. It is not common in clients who have nausea and vomiting.
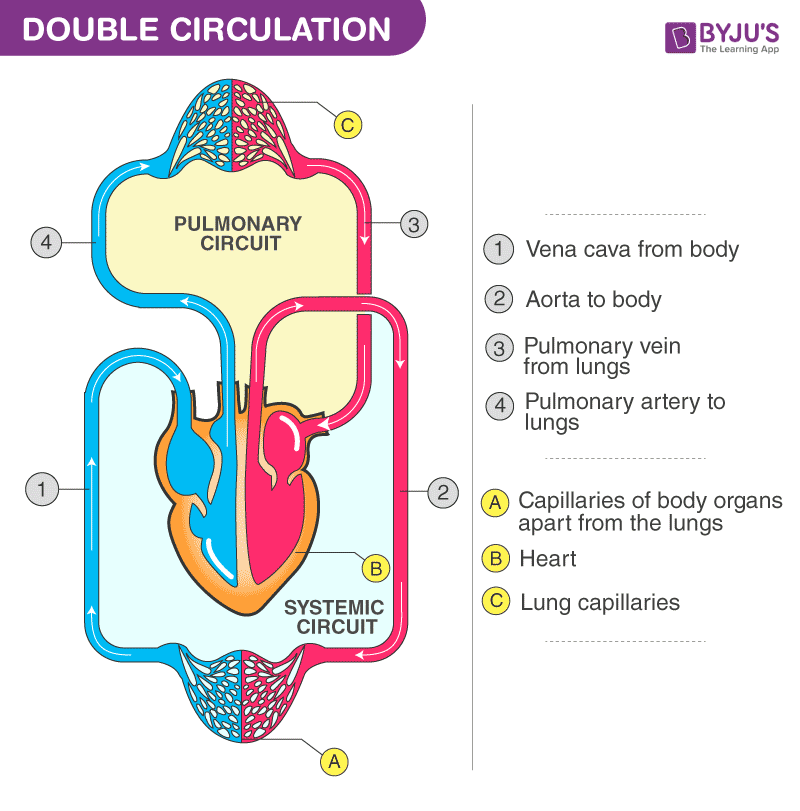
A nurse is assisting with teaching a class about pulmonary circulation. The nurse should include that blood flows from the heart to the lungs from the right ventricle starting from which of the following locations?
Explanation
Choice A reason: The pulmonary artery is the large blood vessel that carries deoxygenated blood from the right ventricle to the lungs for gas exchange. It is the only artery that carries deoxygenated blood in the body.
Choice B reason: The pulmonary veins are the blood vessels that carry oxygenated blood from the lungs to the left atrium. They are the only veins that carry oxygenated blood in the body.
Choice C reason: The left ventricle is the chamber of the heart that pumps oxygenated blood to the rest of the body through the aorta. It does not directly connect to the lungs.
Choice D reason: The left atrium is the chamber of the heart that receives oxygenated blood from the pulmonary veins. It does not directly connect to the right ventricle.
A nurse is collecting data on a client who has oxygen toxicity. Which of the following findings should the nurse expect?
Explanation
Choice A reason: Muscle twitching is a sign of central nervous system oxygen toxicity, which can occur when breathing high concentrations of oxygen under pressure. It can also cause seizures, confusion, and loss of consciousness.
Choice B reason: Facial flushing is not a symptom of oxygen toxicity. It can be caused by other conditions such as fever, allergic reactions, or alcohol consumption.
Choice C reason: Periorbital edema is not a symptom of oxygen toxicity. It can be caused by other conditions such as kidney disease, heart failure, or allergies.
Choice D reason: Metallic taste in mouth is not a symptom of oxygen toxicity. It can be caused by other conditions such as medication side effects, dental problems, or infections.
A nurse is caring for a client who reports constipation. The provider has prescribed an enema. Identify the sequence of steps the nurse should take to administer the enema. (Move the steps into the box on the right, placing them in the selected order of performance. Use all the steps.)
Explanation
Choice A reason: Confirming the client's identity by checking their wristband is the first step to ensure that the right client receives the right treatment.
Choice B reason: Providing for the client's privacy by closing the curtains is the second step to respect the client's dignity and comfort.
Choice C reason: Assisting the client into the Sims' position is the third step to facilitate the insertion of the enema tubing and the flow of the solution. The Sims' position is a side-lying position with the upper leg flexed and the lower leg straight.
Choice D reason: Inserting the tip of the enema tubing into the client's rectum is the fourth and final step to administer the enema. The nurse should lubricate the tip of the tubing, gently insert it about 3 to 4 inches into the rectum, and release the clamp to allow the solution to flow. The nurse should monitor the client for any signs of discomfort or cramping and adjust the flow rate accordingly.
A nurse is reinforcing teaching about elimination with an adolescent who is paralyzed from the waist down following a spinal cord injury. Which of the following statements by the adolescent indicates a need for further teaching?
Explanation
Choice A reason: Doing wheelchair exercises sitting in the chair is a correct statement, as it helps to prevent pressure ulcers, improve circulation, and maintain muscle tone.
Choice B reason: Using a suppository every night to have a bowel movement is an incorrect statement, as it indicates a dependence on laxatives and a lack of bowel training. The adolescent should be taught to establish a regular bowel routine, use natural methods such as abdominal massage and digital stimulation, and avoid overuse of laxatives.
Choice C reason: Needing to catheterize oneself twice a day is a correct statement, as it helps to prevent urinary tract infections, bladder distension, and kidney damage.
Choice D reason: Carrying a water bottle with me because I drink a lot of water is a correct statement, as it helps to prevent dehydration, constipation, and urinary tract infections.
A nurse is caring for an older adult client who has constipation. Which of the following actions should the nurse take?
Explanation
Choice A reason: Requesting that the provider prescribe a stool softener is not the best action for the nurse to take, as it may cause dependency, dehydration, or electrolyte imbalance. The nurse should try non-pharmacological interventions first, such as increasing fluid and fiber intake, promoting physical activity, and establishing a regular bowel routine.
Choice B reason: Adding fluid and fiber to the diet is the best action for the nurse to take, as it helps to soften the stool, increase the bulk, and stimulate peristalsis. The nurse should encourage the client to drink at least 2 liters of water per day and eat foods rich in fiber, such as fruits, vegetables, and whole grains.
Choice C reason: Promoting active range-of-motion activities is a good action for the nurse to take, as it helps to improve circulation, muscle tone, and bowel motility. The nurse should assist the client to perform exercises that are appropriate for their level of mobility and endurance.
Choice D reason: Avoiding gas-producing foods is not a necessary action for the nurse to take, as it does not directly affect constipation. Gas-producing foods, such as beans, cabbage, and broccoli, may cause bloating and discomfort, but they do not cause or worsen constipation.
A nurse is collecting data on a client who has a pleural effusion. Which of the following findings should the nurse expect?
Explanation
Choice A reason: Crackles auscultated over the client's lung fields are not a sign of pleural effusion. Crackles are abnormal breath sounds that indicate fluid or secretions in the alveoli. They can be heard in conditions such as pneumonia, heart failure, or pulmonary edema.
Choice B reason: Crepitus palpated on the client's chest is not a sign of pleural effusion. Crepitus is a crackling sensation that occurs when air leaks into the subcutaneous tissue. It can be felt in conditions such as pneumothorax, chest trauma, or chest surgery.
Choice C reason: Substernal retractions noted on the client's chest are not a sign of pleural effusion. Substernal retractions are inward movements of the chest wall below the sternum that indicate increased respiratory effort. They can be seen in conditions such as asthma, bronchiolitis, or croup.
Choice D reason: Dullness percussed over the client's lung fields is a sign of pleural effusion. Dullness is a flat sound that indicates the presence of a solid or liquid mass in the thoracic cavity. It can be detected in conditions such as pleural effusion, atelectasis, or consolidation.
A nurse is assisting with the care of a client who has a chest tube. Which of the following actions should the nurse take?
Explanation
Choice A reason: Stripping the client's chest tube every 2 hours is not a recommended action, as it can cause excessive negative pressure, tissue trauma, and pain. The nurse should only strip the chest tube if there is a clot or obstruction in the tubing, and only with the provider's order.
Choice B reason: Looping the tubing of the chest tube on the client's bed is a correct action, as it prevents kinking, tension, or pulling on the chest tube. The nurse should also secure the tubing to the bed sheet with a safety pin.
Choice C reason: Placing the chest tube drainage system above the level of the client's heart is not a correct action, as it can cause the fluid to flow back into the chest cavity and impair lung expansion. The nurse should place the chest tube drainage system below the level of the client's chest.
Choice D reason: Taping the connections on the client's chest tube is a correct action, as it prevents air leaks, disconnections, or accidental removal of the chest tube. The nurse should also check the connections regularly for tightness and patency.
A nurse is collecting data on a client who has urinary retention. Which of the following findings should the nurse expect?
Explanation
Choice A reason: Leakage of urine is a sign of urinary retention, as it indicates that the bladder is overdistended and unable to empty completely. The urine may leak around the urethra or through a catheter.
Choice B reason: Dark-colored urine is not a sign of urinary retention. It can be caused by dehydration, certain foods or medications, or liver or kidney problems.
Choice C reason: Cloudy urine is not a sign of urinary retention. It can be caused by infection, inflammation, or stones in the urinary tract.
Choice D reason: Blood in urine is not a sign of urinary retention. It can be caused by trauma, infection, cancer, or coagulation disorders in the urinary tract.
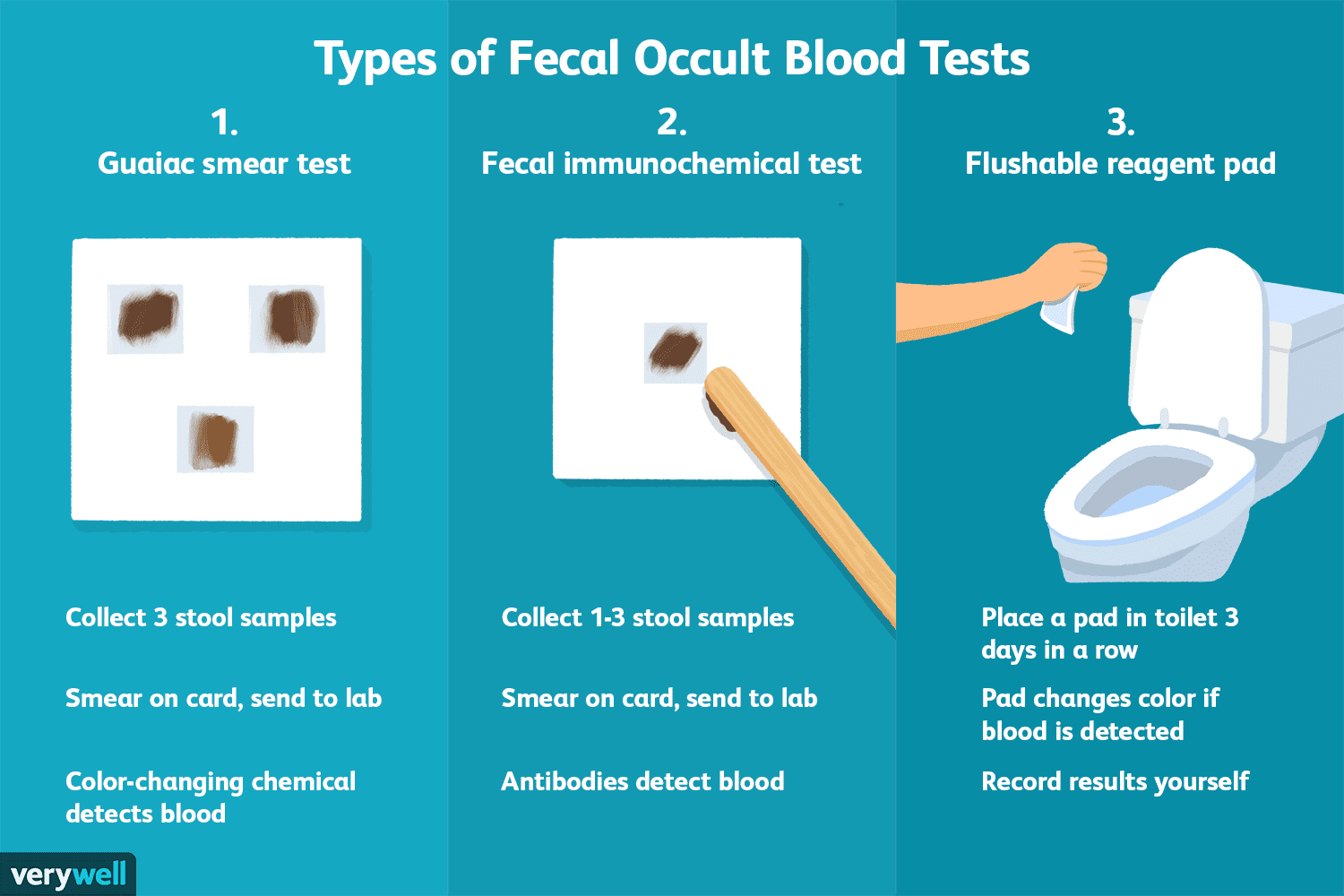
A nurse is caring for a client who has a prescription for a stool guaiac test. The client asks the nurse about the purpose of the test. The nurse should respond by stating that the stool guaiac is testing for which of the following findings in the client's feces?
Explanation
Choice A reason: Bacteria are not detected by the stool guaiac test. The stool guaiac test is a chemical test that reacts with hemoglobin, a protein found in red blood cells. Bacteria are microorganisms that do not contain hemoglobin.
Choice B reason: Fat is not detected by the stool guaiac test. The stool guaiac test is a chemical test that reacts with hemoglobin, a protein found in red blood cells. Fat is a lipid that does not contain hemoglobin.
Choice C reason: Parasites are not detected by the stool guaiac test. The stool guaiac test is a chemical test that reacts with hemoglobin, a protein found in red blood cells. Parasites are organisms that live in or on another host and do not contain hemoglobin.
Choice D reason: Blood is detected by the stool guaiac test. The stool guaiac test is a chemical test that reacts with hemoglobin, a protein found in red blood cells. Blood can indicate bleeding in the gastrointestinal tract, which can be caused by various conditions such as ulcers, polyps, or cancer.
A nurse is assisting in the care of a client who has diabetic ketoacidosis and hypoxia. Which of the following actions should the nurse take first?
Explanation
Choice A reason: Obtaining a prescription to administer insulin is an important action for the nurse to take, as insulin helps to lower the blood glucose level and reverse the metabolic acidosis caused by diabetic ketoacidosis. However, it is not the first action the nurse should take, as the client's hypoxia is a more urgent problem that requires immediate intervention.
Choice B reason: Obtaining a prescription for supplemental oxygen is the first action the nurse should take, as hypoxia is a life-threatening condition that can lead to tissue damage, organ failure, and death. The nurse should provide oxygen therapy to improve the client's oxygen saturation and prevent further complications.
Choice C reason: Obtaining a prescription to check the client's glucose level is a necessary action for the nurse to take, as glucose monitoring helps to evaluate the client's response to insulin therapy and guide further interventions. However, it is not the first action the nurse should take, as the client's hypoxia is a more urgent problem that requires immediate intervention.
Choice D reason: Obtaining a prescription to administer intravenous fluids is a beneficial action for the nurse to take, as fluid replacement helps to correct the dehydration, electrolyte imbalance, and hypotension caused by diabetic ketoacidosis. However, it is not the first action the nurse should take, as the client's hypoxia is a more urgent problem that requires immediate intervention.
A nurse is collecting data on a client who has respiratory acidosis. Which of the following findings should the nurse expect?
Explanation
Choice A reason: Numbness of fingers is not a sign of respiratory acidosis. It can be caused by other conditions such as peripheral neuropathy, Raynaud's syndrome, or carpal tunnel syndrome.
Choice B reason: Abdominal pain is not a sign of respiratory acidosis. It can be caused by other conditions such as gastritis, appendicitis, or gallstones.
Choice C reason: Dry skin is not a sign of respiratory acidosis. It can be caused by other conditions such as dehydration, eczema, or hypothyroidism.
Choice D reason: Lethargy is a sign of respiratory acidosis, as it indicates a low level of oxygen and a high level of carbon dioxide in the brain. Lethargy is a state of reduced mental and physical activity, which can progress to confusion, coma, or death if not treated.
A nurse is caring for a client who has metabolic alkalosis. Which of the following actions should the nurse take first?
Explanation
Choice A reason: Placing the client on continuous cardiac monitoring is a good action for the nurse to take, as metabolic alkalosis can cause cardiac arrhythmias, hypotension, and decreased perfusion. However, it is not the first action the nurse should take, as the client's acid-base imbalance is a more urgent problem that requires immediate intervention.
Choice B reason: Obtaining a prescription for insulin for the client is not a relevant action for the nurse to take, as insulin is used to treat hyperglycemia, not metabolic alkalosis. Metabolic alkalosis is a condition in which the blood pH is too high due to excessive loss of acid or excessive gain of base.
Choice C reason: Planning to administer sodium bicarbonate to the client is not a correct action for the nurse to take, as sodium bicarbonate is an alkalinizing agent that can worsen metabolic alkalosis. The nurse should avoid giving the client any substances that can increase the blood pH.
Choice D reason: Having the client breathe into a paper bag is the first action the nurse should take, as it helps to lower the blood pH by increasing the carbon dioxide level. Carbon dioxide is an acidic gas that can counteract the alkalosis. The nurse should monitor the client's respiratory rate and oxygen saturation while performing this intervention.
A nurse is assisting with the care of a client who is placed on supplemental oxygen for hypoxia. The nurse should identify that which of the following findings indicate the intervention was effective?
Explanation
Choice A reason: Respiratory rate 28/min is not a sign of effective oxygen therapy, as it indicates tachypnea, which is a rapid breathing rate. Tachypnea can be caused by hypoxia, anxiety, fever, or pain.
Choice B reason: Pink mucous membranes are a sign of effective oxygen therapy, as they indicate adequate oxygenation of the tissues. Pink mucous membranes are a normal finding, while pale, cyanotic, or jaundiced mucous membranes can indicate hypoxia or other problems.
Choice C reason: Heart rate 110/min is not a sign of effective oxygen therapy, as it indicates tachycardia, which is a rapid heart rate. Tachycardia can be caused by hypoxia, stress, dehydration, or infection.
Choice D reason: Restlessness is not a sign of effective oxygen therapy, as it indicates agitation, anxiety, or discomfort. Restlessness can be caused by hypoxia, pain, or medication side effects.
A nurse is obtaining a urine specimen for culture and sensitivity via a straight catheterization. Which of the following actions should the nurse take?
Explanation
Choice A reason: Collecting urine from the catheter's port is not a correct action for the nurse to take, as it can introduce contamination and infection into the urinary tract. The nurse should insert a new, sterile catheter into the bladder and collect the urine directly from the catheter.
Choice B reason: Using a sterile specimen container is a correct action for the nurse to take, as it ensures that the urine sample is not contaminated by any bacteria or other substances. The nurse should label the container with the client's name, date, and time of collection and send it to the laboratory as soon as possible.
Choice C reason: Using sterile water to inflate the balloon is not a relevant action for the nurse to take, as it applies to an indwelling catheter, not a straight catheter. A straight catheter does not have a balloon and is removed after the urine is drained.
Choice D reason: Instructing the client to clean from front to back with an antiseptic solution is a good action for the nurse to take, as it helps to prevent the introduction of bacteria from the anal area into the urethra. However, it is not the best answer, as it is a general hygiene measure, not a specific action for obtaining a urine specimen.
A nurse is caring for a client who has paraplegia and is on an intermittent urinary catheterization program. Which of the following findings indicates to the nurse the need to catheterize the client?
Explanation
Choice A reason: Reflex incontinence is not a sign of the need to catheterize the client, as it is a type of involuntary urine loss that occurs when the bladder is overfilled and the sphincter relaxes. Reflex incontinence can be managed by following a regular catheterization schedule, not by waiting for symptoms.
Choice B reason: Urge incontinence is not a sign of the need to catheterize the client, as it is a type of involuntary urine loss that occurs when the bladder contracts involuntarily and the sphincter cannot prevent leakage. Urge incontinence can be managed by using anticholinergic medications, bladder training, or pelvic floor exercises, not by catheterization.
Choice C reason: Nocturnal enuresis is not a sign of the need to catheterize the client, as it is a type of involuntary urine loss that occurs during sleep. Nocturnal enuresis can be managed by limiting fluid intake before bedtime, using an alarm device, or taking desmopressin, not by catheterization.
Choice D reason: Suprapubic discomfort is a sign of the need to catheterize the client, as it indicates bladder distension and possible urinary retention. Suprapubic discomfort can be relieved by draining the urine from the bladder using a catheter.
A nurse is reinforcing discharge teaching with the parents of an infant who has a prescription for home oxygen and pulse oximetry monitoring. Which of the following statements by the parents indicates a need for further teaching?
Explanation
Choice A reason: The pulse oximeter might not be accurate during times of excessive movement is a correct statement, as movement can interfere with the detection of the pulse and the oxygen saturation. The parents should try to keep the infant still and calm while using the pulse oximeter.
Choice B reason: We will notify the doctor if the pulse oximeter consistently reads 100% is an incorrect statement, as it indicates a misunderstanding of the normal range of oxygen saturation. The parents should not be alarmed if the pulse oximeter reads 100%, as it means that the infant's blood is fully saturated with oxygen. The normal range of oxygen saturation for infants is 95% to 100%.
Choice C reason: The probe of the pulse oximeter can be applied to a finger or a toe is a correct statement, as these are suitable sites for measuring the oxygen saturation in infants. The parents should make sure that the probe fits snugly and securely on the infant's finger or toe.
Choice D reason: We will rotate the probe of the pulse oximeter every 24 hours is a correct statement, as it helps to prevent skin irritation, pressure ulcers, or infection from prolonged contact with the probe. The parents should also check the infant's skin regularly for any signs of redness, swelling, or pain.
A nurse is assessing a client who has respiratory alkalosis. Which of the following findings should the nurse expect?
Explanation
Choice A reason: Dry skin is not a sign of respiratory alkalosis. It can be caused by other conditions such as dehydration, eczema, or hypothyroidism.
Choice B reason: Abdominal pain is not a sign of respiratory alkalosis. It can be caused by other conditions such as gastritis, appendicitis, or gallstones.
Choice C reason: Diarrhea is not a sign of respiratory alkalosis. It can be caused by other conditions such as infection, inflammation, or food intolerance.
Choice D reason: Numbness of fingers is a sign of respiratory alkalosis, as it indicates a low level of calcium in the blood (hypocalcemia). Hypocalcemia can result from the alkalosis, as it causes the calcium to bind to proteins and become less available. Numbness of fingers can also affect the toes and lips.
A nurse is teaching a client who has a new prescription for an inhaler. Which of the following statements by the client indicates an understanding of the teaching?
Explanation
Choice A reason: Shaking the inhaler well before using it is a correct action for the client to take, as it helps to mix the medication and the propellant. However, it is not the best answer, as it is a general instruction that applies to most inhalers, not a specific one that indicates an understanding of the teaching.
Choice B reason: Holding the breath for 10 seconds after inhaling the medication is a correct action for the client to take, as it helps to keep the medication in the lungs and improve its absorption. However, it is not the best answer, as it is a general instruction that applies to most inhalers, not a specific one that indicates an understanding of the teaching.
Choice C reason: Rinsing the mouth with water after using the inhaler is the best answer, as it indicates an understanding of the teaching. Rinsing the mouth with water helps to prevent oral thrush, a fungal infection that can occur as a side effect of some inhalers, especially those that contain steroids.
Choice D reason: Waiting 30 seconds between each puff of the inhaler is not a correct action for the client to take, as it can reduce the effectiveness of the medication. The client should wait at least one minute between each puff of the inhaler, unless instructed otherwise by the provider.
A nurse is collecting data on a client who has had diarrhea for several days. Which of the following findings should the nurse expect?
Explanation
Choice A reason: Rigid abdomen is not a sign of diarrhea, but rather a sign of peritonitis, which is an inflammation of the abdominal lining. Peritonitis can be caused by a perforated ulcer, appendicitis, or diverticulitis.
Choice B reason: Dehydration is a sign of diarrhea, as it indicates a loss of fluid and electrolytes from the body. Dehydration can cause symptoms such as dry mouth, thirst, decreased urine output, sunken eyes, and low blood pressure.
Choice C reason: Hypothermia is not a sign of diarrhea, but rather a sign of low body temperature. Hypothermia can be caused by exposure to cold, shock, or infection.
Choice D reason: Decreased bowel sounds are not a sign of diarrhea, but rather a sign of ileus, which is a lack of intestinal activity. Ileus can be caused by surgery, medication, or obstruction.
A nurse is providing teaching for a client who has an ileal conduit following bladder cancer. Which of the following statements by the client indicates a need for the nurse to provide additional teaching?
Explanation
Choice A reason: This statement indicates a need for further teaching, as it is incorrect. The client does not need to catheterize the stoma, as the urine flows continuously from the ileal conduit to the pouch. Catheterization can cause infection and damage to the stoma.
Choice B reason: This statement is correct, as the client will need to measure the stoma each week for the first 6 to 8 weeks after surgery. The stoma may change in size and shape as it heals, and the client will need to adjust the size of the pouch opening accordingly.
Choice C reason: This statement is correct, as the client will always have to wear a pouch to collect the urine. The client can choose from different types of pouches, such as one-piece or two-piece systems, and change them as needed.
Choice D reason: This statement is correct, as the client will need to cleanse around the stoma with soap and water at least once a day. This helps to prevent skin irritation and infection. The client should avoid using alcohol, perfumes, or lotions on the stoma.
A nurse is preparing to remove a client's urinary catheter. After performing hand hygiene, which of the following actions should the nurse take?
Explanation
Choice A reason: Positioning the client supine is not a necessary action for the nurse to take, as the client can be in any comfortable position for the catheter removal. The nurse should explain the procedure to the client and provide privacy.
Choice B reason: Cleansing the perineal area with an antiseptic is not a required action for the nurse to take, as the catheter is already sterile and the risk of infection is low. The nurse should wear gloves and use a clean syringe to deflate the balloon.
Choice C reason: Deflating the balloon halfway and then pulling out the catheter is the correct action for the nurse to take, as it ensures that the catheter is removed smoothly and without causing trauma to the urethra. The nurse should apply gentle traction and observe the urine color and amount in the drainage bag.
Choice D reason: Having the client bear down during removal is not a recommended action for the nurse to take, as it can cause discomfort and bleeding. The nurse should instruct the client to relax and breathe normally during the procedure.
Sign Up or Login to view all the 43 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
