NUR390 Med Surg 390
Total Questions : 32
Showing 25 questions, Sign in for moreWhich information is most important for the nurse to include when teaching a client newly diagnosed with hypertension?
Explanation
Among the given options, the most important information for the nurse to include when teaching a client newly diagnosed with hypertension is option C, "Increasing physical activity controls blood pressure (BP) for most people."
Option C emphasizes the importance of increasing physical activity as a primary lifestyle modification to control blood pressure for most people with hypertension. Regular physical activity can help improve cardiovascular health, reduce blood pressure, and manage overall health. It is a proactive step that the individual can take immediately to start managing their hypertension.
Incorrect:
Option A, "Most people are able to control BP through dietary changes," is not necessarily true for everyone. While dietary changes, such as reducing sodium intake and adopting a heart-healthy diet, can be beneficial in managing hypertension, they may not be sufficient for everyone. Physical activity is an essential component of hypertension management and has broader health benefits.
Option B, "Annual BP checks are needed to monitor treatment effectiveness," is important information, but it is more of a recommendation for ongoing hypertension management rather than the most critical information for someone newly diagnosed with hypertension. Regular blood pressure monitoring is indeed crucial for treatment assessment and ensuring that the chosen treatment plan is effective.
Option D, "Hypertension is usually asymptomatic until target organ damage occurs," is important information to understand the nature of hypertension, but it does not provide immediate guidance for the newly diagnosed individual on how to manage their condition effectively.
As part of a comprehensive hypertension education plan, the nurse can provide additional information about dietary changes, regular blood pressure monitoring, and the importance of early management to prevent target organ damage. However, emphasizing physical activity as a fundamental aspect of hypertension management is the most important initial step for a newly diagnosed client. The nurse can then tailor the education based on the individual's specific needs and health status.
A client with a history of hypertension treated with a diuretic and an angiotensin-converting enzyme (ACE) inhibitor arrives in the emergency department. The client reports a severe headache and nausea and has a blood pressure (BP) of 238/118 mm Hg. Which question should the nurse ask to follow up on these findings?
Explanation
The client presenting to the emergency department with a severe headache, nausea, and significantly elevated blood pressure (BP) of 238/118 mm Hg indicates a hypertensive crisis, which is a severe and potentially life-threatening condition. In such cases, the nurse's priority is to assess for potential triggers or exacerbating factors for the hypertensive crisis.
Option B, "Have there been recent stressful events in your life?" is the most relevant question to follow up on the findings. Stress is a known trigger for acute elevations in blood pressure, and severe stress can lead to a hypertensive crisis in individuals with a history of hypertension. Identifying recent stressful events may help the nurse understand potential contributing factors to the client's current condition and guide the management plan.
Option A, "Have you recently taken any antihistamines?" is not the most relevant question in this situation. Antihistamines are not typically associated with causing a hypertensive crisis. While certain medications and substances can interact with antihypertensive medications, causing an increase in BP, the severity of the client's symptoms and the extremely high BP reading suggest that a more immediate concern needs to be addressed.
Option C, "Have you consistently taken your medications?" is important for assessing medication adherence, but it may not directly explain the acute hypertensive crisis. The client's current symptoms and BP reading require more immediate investigation into potential triggers.
Option D, "Did you take any aspirin (or Tylenol) today?" is relevant to assess whether the client has recently taken any over-the-counter medications that could potentially interact with their prescribed antihypertensive drugs. However, it is not the most critical question to address the hypertensive crisis and the severity of the client's symptoms.
Given the severity of the client's presentation, the nurse should also promptly initiate appropriate interventions to address the hypertensive crisis, such as administering antihypertensive medications as prescribed, monitoring vital signs frequently, and notifying the healthcare provider for further evaluation and management.
The nurse is assessing a client who has been admitted to the intensive care unit (ICU) with a hypertensive emergency. Which finding is most important to report to the health care provider?
Explanation
The most important finding to report to the healthcare provider in a client admitted to the intensive care unit (ICU) with a hypertensive emergency is option B, "The client cannot move the left arm and leg when asked to do so."
Hypertensive emergencies are critical situations where extremely high blood pressure levels can lead to damage or dysfunction in vital organs, such as the brain, heart, kidneys, and eyes. Neurological symptoms are particularly concerning in this context, as they may indicate acute brain injury or stroke resulting from uncontrolled high blood pressure.
Option A, "Tremors are noted in the fingers when the client extends the arms," could be concerning but is not as immediately critical as the neurological deficit described in option B. Tremors can have various causes and may not directly relate to the hypertensive emergency unless other signs or symptoms of neurologic impairment are also present.
Option C, "Urine output over 8 hours is 250 mL less than the fluid intake," is relevant to monitor the client's fluid status and kidney function, but it does not indicate an acute, life-threatening condition that requires immediate attention like the neurological deficit in option B.
Option D, "The client reports a headache with pain at level 7 of 10 (0 to 10 scale)," is concerning and may be a symptom of the hypertensive emergency, but it is not as urgent as the neurological findings. Headache can be a symptom of elevated blood pressure, but it is not sufficient on its own to determine the severity of the hypertensive crisis.
In a hypertensive emergency, the priority is to identify and manage potential complications, such as neurological deficits, acute organ damage, or signs of target organ dysfunction. Prompt reporting of any neurological changes is crucial, as it may prompt immediate interventions to prevent further neurological deterioration. The healthcare provider needs to assess the client's neurological status promptly and determine appropriate management to prevent further complications.
The nurse is reviewing the laboratory test results for a client who has recently been diagnosed with hypertension. Which result is most important to communicate to the health care provider?
Explanation
Among the given laboratory test results for a client with recently diagnosed hypertension, the most important result to communicate to the health care provider is option (A), "Serum creatinine of 2.8 mg/dL."
Serum creatinine is a measure of kidney function, and a value of 2.8 mg/dL indicates elevated creatinine levels. Elevated serum creatinine is a concerning finding, as it suggests decreased kidney function or kidney impairment. Hypertension can have a significant impact on the kidneys, and kidney damage is a common complication of uncontrolled high blood pressure.
The kidneys play a crucial role in regulating blood pressure by excreting waste products and excess fluids from the body. When kidney function is compromised due to hypertension, it can further worsen the blood pressure control, leading to a vicious cycle of kidney damage and worsening hypertension.
Option (B), "Serum hemoglobin of 14.7 g/dL," is within the normal range and does not indicate an immediate concern related to the client's hypertension.
Option (C), "Blood glucose level of 96 mg/dL," is also within the normal range for blood glucose and may not be directly related to the client's hypertension.
Option (D), "Serum potassium of 4.5 mEq/L," is within the normal range. While potassium levels are essential to monitor, they are not the most critical concern compared to kidney function in this context.
The elevated serum creatinine level suggests a potential complication of hypertension, namely kidney damage or decreased kidney function. Therefore, it is essential to communicate this finding promptly to the health care provider for further evaluation and appropriate management to address the client's kidney health and optimize blood pressure control.
The nurse on the intermediate care unit received a change-of-shift report on four patients with hypertension. Which patient should the nurse assess first?
Explanation
Among the four patients with hypertension, the nurse should assess the patient in option B first, the 48-year-old with a blood pressure of 160/92 mm Hg who reports chest pain.
Chest pain is a potentially serious symptom that could indicate an acute cardiac event, such as angina or a heart attack. Given that the patient has hypertension and is experiencing chest pain, the nurse must prioritize this assessment to rule out any cardiac-related complications or other urgent issues.
While all the other patients have elevated blood pressure readings, they have additional symptoms or conditions that indicate potential complications related to their hypertension. However, chest pain is a red flag that requires immediate attention and further assessment to determine its cause and provide appropriate interventions promptly.
Option A, the 52-year-old with a blood pressure of 198/90 mm Hg who has intermittent claudication, may have peripheral vascular disease or other vascular issues related to hypertension, but it is not as acutely concerning as chest pain.
Option C, the 43-year-old with a blood pressure of 172/98 mm Hg whose urine shows microalbuminuria, may have early signs of kidney involvement due to hypertension, which is significant and requires attention but may not be as immediately urgent as chest pain.
Option D, the 50-year-old with a blood pressure of 190/104 mm Hg who has a creatinine of 1.7 mg/dL, may have signs of kidney impairment related to hypertension, which is also significant but may not be as acutely urgent as chest pain.
In summary, the nurse should prioritize the assessment of the patient experiencing chest pain (option B) to address any potential cardiac-related issues promptly and ensure appropriate management and intervention.
Which action will the nurse include in the plan of care for a patient who was admitted with syncopal episodes of unknown origin?
Explanation
For a patient admitted with syncopal (fainting) episodes of unknown origin, the most appropriate action to include in the plan of care is to instruct the patient to call for assistance before getting out of bed.
Syncope can be caused by various factors, including orthostatic hypotension (a drop in blood pressure upon standing) or cardiac-related issues. One of the common triggers for syncopal episodes is getting up from a lying or sitting position too quickly. By instructing the patient to call for assistance before getting out of bed, the nurse aims to prevent falls and potential injuries that may occur due to sudden fainting episodes.
While it's essential to educate the patient about potential causes of syncope (option A) and the benefits of implantable cardioverter-defibrillators (option B) if applicable to their condition, these actions may not directly address the immediate safety concern of preventing falls during syncopal episodes.
Option D, teaching the patient about the need to avoid caffeine and other stimulants, may be relevant if stimulants are identified as potential triggers for syncope in this particular patient. However, it is not the most critical action to include in the initial plan of care for a patient with syncopal episodes of unknown origin.
In summary, the top priority for the nurse is to ensure the safety of the patient by instructing them to call for assistance before getting out of bed to prevent falls during syncopal episodes until further evaluation and diagnosis can determine the cause of the fainting episodes.
A patient is apneic and has no palpable pulses. The heart monitor shows sinus tachycardia, rate 132. What action should the nurse take next?
Explanation
The patient is apneic (not breathing) and has no palpable pulses, indicating a cardiac arrest or severe cardiovascular compromise. In this situation, the most appropriate action for the nurse to take next is to start cardiopulmonary resuscitation (CPR) immediately.
CPR is a life-saving procedure that combines chest compressions and rescue breaths to circulate oxygenated blood to vital organs when the heart is not effectively pumping. In the case of cardiac arrest, early initiation of CPR is critical to improve the chances of survival and minimize potential brain damage.

The heart monitor shows sinus tachycardia, rate 132, which suggests that the electrical impulses are reaching the heart, but the heart is not effectively pumping blood due to the lack of a palpable pulse. This condition requires immediate intervention with CPR rather than other treatments such as synchronized cardioversion (option A) or administering atropine (option D).
While applying supplemental oxygen via a non-rebreather mask (option C) is generally important in many emergency situations, it is not the immediate priority when a patient is apneic and has no palpable pulses. In such cases, CPR takes precedence to restore circulation and maintain oxygen delivery to the body's vital organs.
While assessing an older adult client, the nurse notes jugular venous distention (JVD) with the head of the client's bed elevated 45 degrees. What does this finding indicate?
Explanation
Jugular venous distention (JVD) is a clinical sign that indicates increased fluid volume or fluid overload in the cardiovascular system. When the head of the client's bed is elevated at 45 degrees, the jugular veins should normally be flat or slightly distended. However, if the jugular veins appear engorged and bulging, it suggests that there is an increased amount of blood returning to the right side of the heart and is unable to be efficiently pumped forward, leading to jugular venous distention.
JVD is commonly seen in conditions such as heart failure, where the heart's ability to pump blood efficiently is compromised, leading to fluid accumulation in the veins and eventually causing jugular venous distention.
Option A, jugular vein atherosclerosis, is not a common cause of JVD. Atherosclerosis refers to the build-up of plaque within arteries, not veins.
Option C, decreased fluid volume, would lead to dehydration and decreased venous filling, which would not cause jugular venous distention. It would lead to flat or sunken jugular veins.
Option D, incompetent jugular vein valves, would not cause jugular venous distention with the head of the bed elevated. Incompetent valves may lead to venous reflux or backward flow of blood, but it would not lead to the distention of the jugular veins in this position.

A patient with dilated cardiomyopathy has new onset atrial fibrillation that has been unresponsive to drug therapy for several days. What topic should the nurse plan to include in patient teaching?
Explanation
When a patient with dilated cardiomyopathy develops new onset atrial fibrillation (AF) that has been unresponsive to drug therapy, the nurse should prioritize patient education about anticoagulant therapy. Atrial fibrillation increases the risk of blood clots forming in the heart's atria due to the irregular and ineffective pumping of blood. These blood clots can potentially travel to other parts of the body, leading to serious complications such as stroke.
Anticoagulant therapy, also known as blood-thinning medication, is commonly prescribed for patients with atrial fibrillation to prevent the formation of blood clots. The most common anticoagulant prescribed for AF is warfarin or direct oral anticoagulants (DOACs) such as apixaban, rivaroxaban, dabigatran, or edoxaban. The nurse should educate the patient about the importance of taking the anticoagulant as prescribed and the need for regular monitoring of clotting times (INR for warfarin) to ensure the medication is effective and the dose is appropriate.
While other options listed in the choices may be relevant in specific situations, the priority in this case is to address the potential risk of stroke associated with atrial fibrillation and the importance of anticoagulant therapy to manage that risk effectively.
After the nurse gives IV atropine to a patient with symptomatic type 1. second-degree atrioventricular (AV) block, which finding indicates that the drug has been effective?
Explanation
Atropine is an anticholinergic medication that acts by blocking the effects of the parasympathetic nervous system on the heart, leading to an increase in heart rate (positive chronotropic effect) and conduction velocity (positive dromotropic effect). In patients with symptomatic type 1 second degree atrioventricular (AV) block (also known as Mobitz type 1 or Wenckebach), the electrical impulses between the atria and ventricles are delayed or blocked intermittently, resulting in a progressive lengthening of the PR interval until a ventricular beat is dropped.
When atropine is administered to a patient with symptomatic type 1 AV block, it can counteract the increased vagal tone that contributes to the block and help improve the conduction through the AV node. As a result, the heart rate is expected to increase, which is a positive response to the medication.
The other options listed (B) Decrease in premature ventricular contractions, (C) Increase in strength of peripheral pulses, and (D) Decrease in premature atrial contractions, are not directly related to the effect of atropine on type 1 AV block and are not typical findings associated with atropine administration in this context. The main goal of administering atropine in this situation is to increase the heart rate and improve the AV conduction to alleviate symptoms associated with the AV block.
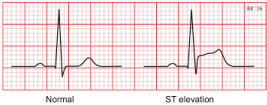
Which electrocardiographic (ECG) change by a client with chest pain is most important for the nurse to report rapidly to the health care provider?
Explanation
ST-segment elevation on an electrocardiogram (ECG) is a critical finding and should be reported rapidly to the health care provider. It is a hallmark ECG change seen in myocardial infarction (heart attack). When there is myocardial ischemia or injury (such as in a heart attack), the ST segment
elevates above the baseline in the affected leads of the ECG. This elevation indicates that there is an ongoing loss of oxygen and blood supply to a part of the heart muscle.
ST-segment elevation is a medical emergency because it suggests acute coronary syndrome (ACS), which can rapidly progress to a myocardial infarction if not promptly treated. Immediate intervention is needed to restore blood flow to the affected coronary artery and prevent further damage to the heart muscle.
The other options listed (A) First-degree atrioventricular block, (B) Inverted P wave, and (C) Sinus tachycardia, while significant in some situations, do not have the same urgency as ST-segment elevation in the context of chest pain. They may require medical attention, but they do not typically indicate an acute myocardial infarction or an immediate life-threatening condition. ST-segment elevation is a critical finding that requires rapid intervention to preserve heart muscle function and prevent complications.
The nurse is caring for a patient with manifestations of acute decompensated heart failure (ADHF). What is the priority nursing assessment?
Explanation
In a patient with acute decompensated heart failure (ADHF), the priority nursing assessment is to auscultate lung sounds. ADHF is characterized by the sudden worsening of heart failure symptoms, which may include pulmonary congestion and fluid accumulation in the lungs. Assessing lung sounds helps to identify signs of pulmonary edema, which is a serious complication of ADHF.
The nurse should listen for crackles or rales, which are abnormal lung sounds caused by the presence of fluid in the alveoli. These findings suggest that the patient is experiencing fluid overload and inadequate gas exchange in the lungs. Prompt recognition of pulmonary edema allows for early intervention, such as administering diuretics or other medications, to relieve fluid overload and improve respiratory function.
While the other options (B) Facial swelling, (C) Level of anxiety, and (D) Intake and output, are important assessments in a patient with heart failure, they are not the priority in a patient with manifestations of acute decompensated heart failure. The priority is to assess for signs of respiratory
distress and pulmonary congestion, as these can quickly lead to respiratory failure and life threatening complications.
Which statement by a client with newly diagnosed heart failure indicates to the nurse that teaching was effective?
Explanation
The statement "I will call the clinic if my weight goes up 3 pounds in a week" indicates that the teaching about heart failure was effective. Monitoring weight is an essential self-care measure for patients with heart failure to manage fluid retention effectively. A sudden weight gain of 2-3 pounds in a week can indicate fluid retention and worsening heart failure. It is crucial for the patient to report such weight changes promptly to the healthcare provider or clinic to adjust medication doses or treatment plans as needed.
The other statements are incorrect:
A) "I will use the nitroglycerin patch whenever I have chest pain." Nitroglycerin is not typically used to manage heart failure. It is used for angina, which is chest pain caused by reduced blood flow to the heart muscle due to narrowed coronary arteries.
B) "I will take furosemide (Lasix) every day just before bedtime." While furosemide is a diuretic commonly prescribed for heart failure to reduce fluid retention, it is not usually taken just before bedtime. Taking furosemide in the evening may lead to frequent nighttime urination and disrupt sleep.
D) "I will use an additional pillow if I am short of breath at night." Using an extra pillow may provide temporary relief for positional dyspnea (shortness of breath when lying flat) but is not an appropriate long-term strategy for managing heart failure. Elevated pillows may not effectively improve breathing and can lead to neck strain. Instead, patients with heart failure should be encouraged to sleep with their head slightly elevated on a regular basis, using a wedge pillow or adjustable bed if needed. Managing fluid retention and adhering to prescribed medications are essential for improving heart failure symptoms and preventing complications.
client with acute coronary syndrome has returned to the coronary care unit after having angioplasty with stent placement. Which assessment data indicate the need for immediate action by the nurse?
Explanation
Among the given options, the assessment data that indicate the need for immediate action by the nurse is a blood pressure of 103/54 mm Hg. This blood pressure reading indicates hypotension, which can be concerning for a post-angioplasty patient.
Angioplasty with stent placement is an invasive procedure, and patients may experience fluctuations in blood pressure during the immediate post-operative period. Hypotension after angioplasty can be a sign of inadequate cardiac output, which may be due to issues like bleeding, fluid loss, or heart dysfunction. Inadequate blood pressure can lead to decreased perfusion to vital organs, including the heart itself, and can be life-threatening.
Options A, B, and D are also important to address:
A) Heart rate 102 beats/min: A heart rate of 102 beats per minute may indicate tachycardia, which can be expected after a procedure like angioplasty. However, it is not as urgent of a concern as hypotension, and it may be a normal compensatory response to the body's stress.
B) Report of chest pain: Chest pain after angioplasty can be common, but it should be evaluated further to ensure it is not indicative of complications such as coronary artery spasms, clot formation, or restenosis of the treated artery. While this is an important issue to address, it does not take precedence over hypotension.
D) Pedal pulses 1+ bilaterally: This finding suggests that the peripheral pulses in the feet are weak, and it could be related to the patient's medical condition, medications, or positioning. While it requires attention, it is not an immediate threat to the patient's life compared to severe hypotension.
Therefore, the nurse should prioritize assessing and addressing the low blood pressure to prevent further complications and ensure the patient's stability. The nurse should promptly notify the healthcare provider and implement appropriate interventions, such as administering intravenous fluids, to increase blood pressure to a safe level.
Which diagnostic test will be most useful to the nurse in determining whether a client admitted with acute shortness of breath has heart failure?
Explanation
B-type natriuretic peptide (BNP) is a diagnostic blood test that can be most useful to the nurse in determining whether a client admitted with acute shortness of breath has heart failure.
BNP is a hormone produced by the heart in response to increased pressure and volume in the heart, especially in cases of heart failure. When the heart is under stress, such as in heart failure, it releases BNP into the bloodstream. Elevated levels of BNP are strongly indicative of heart failure, and the testis particularly helpful in differentiating heart failure from other conditions that may present withsimilar symptoms, such as pulmonary disorders.
When a patient presents with acute shortness of breath, the BNP test can provide valuable information to help guide the diagnosis and treatment. If the BNP level is elevated, it suggests that heart failure is likely the cause of the symptoms, and appropriate interventions can be initiated promptly.
While other diagnostic tests like serum troponin (A) are important for assessing heart damage in conditions like myocardial infarction (heart attack), they may not be as specific for heart failure.
Arterial blood gases (B) are helpful in evaluating gas exchange and acid-base balance, especially in patients with respiratory distress, but they are not specific for diagnosing heart failure.
A 12-lead electrocardiogram (ECG) (C) can provide valuable information about the heart's electrical activity and any signs of acute myocardial infarction or other cardiac abnormalities, but it is not the primary test for diagnosing heart failure. An ECG can support the diagnosis if specific changes suggestive of heart failure are present, but the BNP test provides more direct evidence for heart failure diagnosis.
Which topic will the nurse plan to include in discharge teaching for a client who has heart failure with reduced ejection fraction?
Explanation
Discharge teaching for a client with heart failure and reduced ejection fraction should prioritize education about medications that are essential in managing heart failure, such as angiotensin-converting enzyme (ACE) inhibitors.
ACE inhibitors are a class of medications commonly prescribed to heart failure patients with reduced ejection fraction. They work by dilating blood vessels, reducing the workload on the heart, and improving the heart's pumping ability. They are one of the cornerstones of heart failure management and have been shown to reduce symptoms, improve quality of life, and prolong survival in heart failure patients.
Educating the client about the benefits and effects of ACE inhibitors is crucial to promote medication adherence and ensure they understand the importance of taking this medication as prescribed. Common side effects, such as dizziness or dry cough, should also be discussed so the client knows what to expect and when to notify their healthcare provider.
While the other options may also be relevant to a client with heart failure, including starting an aerobic exercise program (A), reducing salt intake (B), and scheduling regular follow-up appointments (C), the immediate priority in discharge teaching should be about the medication regimen and the specific benefits and effects of ACE inhibitors. Other aspects of heart failure management can be addressed during the overall education and follow-up sessions.
The nurse recalls that which type of drug therapy is used to treat volume overload in patients with acute decompensated heart failure (ADHF)?
Explanation
Diuretics are the primary class of drugs used to treat volume overload in patients with acute decompensated heart failure (ADHF). These medications help to increase urine output, reducing the overall fluid volume in the body and relieving congestion in the lungs and other tissues.
The goal of using diuretics in ADHF is to alleviate symptoms such as shortness of breath, edema (swelling), and fluid retention by promoting the elimination of excess fluid. The most commonly used diuretics in this setting are loop diuretics (e.g., furosemide, bumetanide), which have a potent diuretic effect and can rapidly reduce fluid overload.
While narcotics, vasodilators, and positive inotropes may have roles in specific cases of ADHF, they are not the primary drugs used to treat volume overload. Narcotics may be used for pain management, vasodilators to reduce afterload (the resistance the heart has to pump against), and positive inotropes to increase the heart's contractility in certain situations. However, the first-line treatment for volume overload in ADHF is diuretic therapy.
A client recovering from heart surgery develops pericarditis and reports level 6 (0 to 10 scale) chest pain with deep breathing. Which prescribed PRN medication will be the most appropriate for the nurse to give?
Explanation
Pericarditis is inflammation of the pericardium, the sac-like membrane surrounding the heart. It can cause chest pain, which is often worsened by deep breathing or coughing. The goal of treatment for pericarditis is to reduce inflammation and relieve pain.
In this case, the client's pain level is reported as 6 out of 10. As per the PRN (as-needed) medication options given:
C) Oral ibuprofen (Motrin) 600 mg: Ibuprofen is a nonsteroidal anti-inflammatory drug (NSAID) and can help reduce inflammation and relieve pain in cases of pericarditis. It is an appropriate choice for this client's pain level of 6 out of 10.
A) IV morphine sulfate 4 mg: IV morphine is a potent opioid analgesic and may be appropriate for severe pain. However, in this case, the client's pain level is moderate (6 out of 10), and it is not the first-line medication for pericarditis pain.
B) Oral acetaminophen (Tylenol) 650 mg: Acetaminophen is a mild analgesic and antipyretic that can be effective for mild to moderate pain. However, in this situation, the client's pain is moderate (6 out of 10), and acetaminophen alone may not provide adequate relief for pericarditis pain.
D) Fentanyl 1 mg IV: Fentanyl is another potent opioid analgesic. However, similar to morphine, it may be more appropriate for severe pain, not moderate pain like in this scenario.
Based on the client's pain level and the goal of reducing inflammation, the most appropriate PRN medication for the nurse to give is oral ibuprofen (Motrin) 600 mg.
After receiving change-of-shift report on a heart failure unit, which client should the nurse assess first?
Explanation
The client taking isosorbide dinitrate/hydralazine (BiDil) and experiencing a headache should be assessed first. Isosorbide dinitrate/hydralazine is a medication combination used to treat heart failure, particularly in African American patients. However, one of the side effects of hydralazine is headaches.
Headache in a client taking this medication may indicate increased blood pressure as a compensatory response to vasodilation. If not addressed promptly, it may lead to worsening heart failure or other complications. Therefore, it is essential to assess the client's blood pressure, signs of worsening heart failure, and evaluate the severity and duration of the headache.
The other options may also require attention:
A) A client taking digoxin with a potassium level of 3.1 mEq/L needs assessment, as hypokalemia can increase the risk of digoxin toxicity. However, the headache in the BiDil client takes priority due to the potential complications related to increased blood pressure.
B) A client taking captopril and experiencing a frequent nonproductive cough may indicate a side effect of the medication. While it should be assessed, it is not as immediately concerning as the headache in the BiDil client.
C) A client taking carvedilol (Coreg) with a heart rate of 58 is within an acceptable range, especially if the client is tolerating it well without symptoms. It may not require immediate assessment unless there are other concerning symptoms.
During the 48 hours after a myocardial infarction (MI), a nurse should assign the highest priority to monitoring the patient for what complication?
Explanation
During the 48 hours after a myocardial infarction (MI), the highest priority for monitoring the patient is for dysrhythmias. After an MI, the heart's electrical system can be disrupted, leading to various types of abnormal heart rhythms (dysrhythmias). Dysrhythmias can be life-threatening and require prompt recognition and intervention.
Other options:
B) Anxiety and fear: Anxiety and fear are common emotional responses after an MI, but they are not the highest priority for monitoring during the immediate post-MI period. Emotional support and counseling are essential, but they do not require continuous monitoring.
C) Metabolic acidosis: Metabolic acidosis is not a common complication of an acute MI. It may occur in certain situations, such as when there is inadequate perfusion to tissues, but it is not the highest priority during the immediate post-MI period.
D) Medication side effects: Monitoring for medication side effects is important but is not the highest priority during the immediate post-MI period. Many patients will receive medications to manage pain, reduce clot formation, and stabilize their heart function. The nurse should monitor for side effects but not as a higher priority compared to dysrhythmias.
The nurse is providing teaching to a patient recovering from a myocardial infarction (MI). How should resumption of sexual activity be discussed?
Explanation
Resumption of sexual activity after a myocardial infarction (MI) is an important topic to address as part of the overall recovery and rehabilitation process. It should be discussed along with other physical activities during the patient's recovery. The nurse should initiate the discussion in a supportive and non-judgmental manner, addressing the patient's concerns, fears, and questions about sexual activity after an MI.
Sexual activity is a normal part of life, and patients may have concerns about the safety and appropriateness of engaging in sexual activity after a significant cardiac event like an MI. Discussing it along with other physical activities helps normalize the topic and allows the nurse to provide accurate information, address any misconceptions, and offer guidance on when and how to resume sexual activity safely. Patients should be encouraged to have an open dialogue with their healthcare provider about their concerns and any specific questions they may have related to resuming sexual activity.
The nurse teaches a student nurse about diagnostic studies used for acute coronary syndrome. Which statement made by the student nurse indicates effective learning?
Explanation
This statement indicates effective learning because serum cardiac markers are indeed proteins that are released from necrotic (damaged) heart muscle cells when there is myocardial injury, such as in acute coronary syndrome (ACS). These markers are measured in blood tests and help in the diagnosis and assessment of ACS, particularly myocardial infarction (heart attack).
Option A is incorrect because a nitroprusside stress echocardiogram is not used for acute pericarditis. It is a diagnostic test used for evaluating coronary artery disease and ischemia.
Option B is incorrect because a pathologic Q wave is not always present in the electrocardiogram (ECG) of patients with unstable angina. It is a characteristic finding in the ECG of patients with a previous myocardial infarction (heart attack) but may not be present in unstable angina.
Option D is incorrect because coronary angiography is not the only way to confirm the diagnosis of unstable angina. Unstable angina is primarily diagnosed based on the clinical presentation, symptoms, and changes in the ECG. Coronary angiography is an invasive procedure used to visualize the coronary arteries directly and is typically reserved for cases where further assessment and intervention are needed, such as in cases of suspected coronary artery disease.
A nurse in the emergency department is caring for a client who is experiencing chest pain. Physical Examination
0900:
Client admitted with a report of chest pain radiating to the left arm, sweating, shortness of breath, and epigastric discomfort
Client awake, alert, and oriented x3.
Lung sounds clear bilaterally, S1S2 heart sounds noted.
All pulses palpable.
Skin cool and diaphoretic to touch.
Rates pain as 6 on a 0 to 10 pain scale.
tachycardia with ST elevation. Provider notified.
Medication Administration Record:
Sildenafil 50 mg PO once daily
Simvastatin 40 mg PO once daily
Metoprolol 100 mg PO once daily
Multivitamin once daily
The nurse is reviewing the client's assessment data to prepare the plan of care. What is the potential condition for this client? Select one (1) answer.
Explanation
The client's presentation of chest pain radiating to the left arm, sweating, shortness of breath, epigastric discomfort, cool and diaphoretic skin, tachycardia, and ST elevation on the electrocardiogram (ECG) are indicative of myocardial infarction (heart attack). These symptoms and findings are typical of acute coronary syndrome, specifically an ST-segment elevation myocardial infarction (STEMI).
Option A (Ischemic Stroke) is not the correct answer because the symptoms described in the client's presentation are primarily related to the cardiovascular system and not indicative of an ischemic stroke.
Option B (Chronic Stable Angina) is not the correct answer because chronic stable angina typically presents with chest pain on exertion or stress, and it usually subsides with rest or nitroglycerin. The client's symptoms of chest pain at rest, along with other findings, are more concerning for an acute cardiac event like a myocardial infarction.
Option D (Cardiogenic Shock) is a severe complication that can occur following a myocardial infarction, but the information provided in the scenario does not suggest that the client is in cardiogenic shock at this time. The client's blood pressure is not mentioned in the scenario, which is a crucial parameter to assess for cardiogenic shock.

The assessment findings of a patient with myocardial infarction (MI) include jugular venous distention, weight gain, peripheral edema, and a heart rate of 108/minute. The nurse suspects what complication?
Explanation
The assessment findings of jugular venous distention, weight gain, peripheral edema, and a heart rate of 108/minute are consistent with right-sided heart failure (HF). Right-sided HF occurs when the right ventricle of the heart is unable to pump effectively, leading to congestion in the venous circulation. This can result in jugular venous distention (JVD) due to increased pressure in the jugular veins, peripheral edema due to fluid retention, and weight gain due to fluid accumulation.
Option A (Left-sided HF) may also present with similar symptoms like jugular venous distention, weight gain, and peripheral edema. However, in left-sided HF, there would typically be signs of pulmonary congestion, such as crackles in the lungs and shortness of breath.
Option C (Chronic heart failure) is a general term used for heart failure that has been present for an extended period, and it does not specify whether it is left-sided or right-sided heart failure.
Option D (Acute decompensated heart failure - ADHF) is a form of heart failure that presents with severe symptoms and requires urgent treatment. It is more of a clinical classification rather than a specific complication related to the symptoms mentioned in the scenario.
A nurse is reviewing the arterial blood gas values of a client who has chronic kidney disease. Which of the following sets of values should the nurse expect?
Explanation
In a client with chronic kidney disease (CKD), metabolic acidosis is a common acid-base disorder due to impaired excretion of acid and decreased bicarbonate reabsorption in the kidneys. The arterial blood gas values associated with metabolic acidosis in CKD are a low pH (acidemia), low bicarbonate (HCO3-), and normal or low partial pressure of carbon dioxide (PaCO2). Option A fits this pattern, with a pH of 7.25 (acidic), HCO3- of 19 mEq/L (low), and a PaCO2 of 30 mm Hg (within the normal to low range).
Option B shows a pH of 7.30 (acidic) but with a higher bicarbonate level of 26 mEq/L, which is not consistent with metabolic acidosis. The elevated bicarbonate level suggests metabolic alkalosis, which is not expected in a client with CKD.
Option C has a pH of 7.50 (alkaline) with an elevated bicarbonate level of 20 mEq/L and a low PaCO2 of 32 mm Hg. This set of values is indicative of metabolic alkalosis, which is not expected in a client with CKD.
Option D has a pH of 7.55 (alkaline) with an elevated bicarbonate level of 30 mEq/L and a low PaCO2 of 31 mm Hg. This set of values is indicative of metabolic alkalosis, which is not expected in a client with CKD.

Sign Up or Login to view all the 32 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
