RN Fundamental 2019 Exam 2
Total Questions : 59
Showing 25 questions, Sign in for moreA nurse is teaching an older adult client who has type 2 diabetes mellitus about how to care for corns and calluses on her toes. Which of the following statements by the client indicates an understanding of the teaching?
Explanation
Choice A Reason:
Placing an oval corn pad over toes with corns is not recommended because it can cause further pressure and discomfort. Corn pads should be used with caution and under the guidance of a healthcare professional.
Choice B Reason:
"I can apply lotion to soften calluses as long as I don't put lotion between my toes." is the safest and most appropriate self-care measure for calluses, emphasizing the importance of not applying lotion between the toes, which can lead to moisture retention and skin issues. However, it's always best for the client to consult with a healthcare provider for specific guidance on corn and callus care, as individual situations may vary.
Choice C Reason:
Using over-the-counter liquid medications to remove corns is not typically recommended without consulting a healthcare professional. It's best to have corns assessed and treated by a healthcare provider.
Choice D Reason:
Soaking the feet in warm water daily can help soften corns and calluses, but it should be done with caution. Excessive soaking can lead to skin maceration and should not be done daily. It's essential to follow a healthcare provider's recommendations for soaking and corn/callus care.
A nurse is assessing the skin of a client who has worked outdoors for the past 20 years. Which of the following findings is the nurse's priority?
Explanation
Choice A Reason:
A flat, nonpalpable, colored area of skin on the trunk is not typically a cause for immediate concern. It may represent a pigmented lesion, but without additional information or changes, it doesn't raise immediate red flags for skin cancer.
Choice B Reason:
An atrophic wart on the left index finger, while it may be unsightly or uncomfortable, is not typically a sign of skin cancer. Warts are usually caused by viruses and are not directly related to skin cancer.
Choice C Reason:
"Sings nome in the no region" appears to be a typographical error and is not clear, so it's difficult to assess its significance. It may not be related to skin health concerns.
Choice D Reason:
A change in the appearance of a mole on the shoulder is a concerning finding because changes in moles are one of the potential warning signs of skin cancer. Moles that change in size, shape, color, or border can indicate melanoma, which is a serious and potentially life-threatening form of skin cancer. Therefore, any change in a mole's appearance should be a priority for assessment.
A community health nurse is teaching a group of clients about Kegel exercises to prevent urinary incontinence. Which of the following instructions should the nurse include?
Explanation
Choice A Reason:
"Hold your breath when performing the exercises" is not an appropriate instruction for Kegel exercises. Holding one's breath is not related to the correct performance of Kegel exercises and can lead to increased intra-abdominal pressure, which is not the goal of these exercises.
Choice B Reason:
"Tighten your buttocks when performing the exercises" is also not a correct instruction. While the buttocks are in the general vicinity of the pelvic floor muscles, Kegel exercises focus on contracting and relaxing the pelvic floor muscles themselves, not the buttocks.
Choice C Reason
"Expect improvement after 2 weeks of performing the exercises" is not accurate because the timeline for improvement when performing Kegel exercises can vary from person to person. While some individuals may notice improvement in their symptoms after a few weeks, others may take longer to experience significant results. It's essential to emphasize that consistency and regular practice of Kegel exercises are key to achieving the desired outcomes.
The correct instruction the nurse should include when teaching Kegel exercises to prevent urinary incontinence is:
Choice D Reason:
"Contract your pelvic muscle when performing the exercises." Is the correct option. Kegel exercises involve contracting and relaxing the pelvic floor muscles, which are the muscles that support the bladder, uterus, and rectum. These exercises are effective for preventing and managing urinary incontinence. Option D accurately describes the key action of contracting the pelvic muscles during the exercises.

A nurse is planning to discharge a client who has diabetes mellitus and a new prescription for insulin. Which of the following actions should the nurse plan to complete first?
Explanation
Choice A Reason:
Determining whether the client can afford insulin administration supplies is crucial, but it can be addressed after providing information about insulin self-administration.
Choice B Reason:
Providing the client with the contact number for a diabetes education specialist is important, but it can be done once the client has received basic information on insulin self-administration.
Choice C Reason:
Making a copy of the medication reconciliation form for the client is important for record-keeping and communication but is not as time-sensitive as ensuring the client has the necessary knowledge and materials for insulin administration.
Choice D Reason:
Obtain printed information about insulin self-administration. It is crucial to ensure that the client has the necessary knowledge and resources to self-administer insulin safely and effectively. Providing the client with printed information about insulin self-administration is a critical step in their education and self-care. This information will help the client understand how to properly administer insulin and manage their diabetes. It should cover topics such as insulin dosage, injection technique, storage, and proper disposal of used materials.
A nurse is caring for an inferno is to undergo surgery. The nurse should identify that which of the following individuals should sign the forin?
Explanation
Choice A Reason:
The infant's provider (doctor or healthcare professional) is responsible for explaining the surgical procedure, risks, and benefits to the parents or legal guardians. The provider does not typically sign the informed consent form on behalf of the infant.
Choice B Reason:
When an infant is to undergo surgery, the person who should sign the informed consent form on behalf of the infant is typically a parent or legal guardian. Therefore, option B, "The infant's 17-year-old mother," is the person who should sign the form, assuming that she is the infant's legal guardian.
In many jurisdictions, a parent is automatically considered the legal guardian of their child. However, if there are legal complications or questions about guardianship, it's important to follow local legal regulations and hospital policies to determine who is authorized to provide informed consent on the infant's behalf
Choice C Reason:
The mother's 21-year-old sibling does not automatically have legal authority to sign the informed consent form for the infant unless they have been granted legal guardianship or power of attorney for medical decisions.
Choice D Reason:
The infant's grandparent, like the sibling, does not automatically have legal authority to sign the informed consent form for the infant unless they have been granted legal guardianship or power of attorney for medical decisions.
A nurse is assisting in the take of a fracture bedpan for a client who is immobile due to a cast. Which of the following actions should the nurse take?
Explanation
Choice A Reason:
Hyperextending the client's back while the fracture pan is in place can cause discomfort and is not necessary for proper use of the bedpan. It's important to maintain the client's comfort and avoid unnecessary strain or discomfort.
Choice B Reason:
Encouraging the client to try to defecate for a specific time (20 minutes) is not recommended. It is not advisable to put a time limit on the process, as it can vary for each individual. Clients should be given adequate time and privacy for toileting.
Choice C Reason:
Keeping the bed flat while the client is on the fracture pan is generally not necessary. The bed can be adjusted to a comfortable position for the client, but it should not be raised in a way that would cause discomfort or strain, and the head of the bed can be elevated if that is more comfortable for the client.
Choice D Reason:
Place the shallow end of the fracture pan under the client's buttocks. This is the appropriate way to position the fracture bedpan for safe and effective use. Placing the shallow end of the bedpan under the client's buttocks ensures that the client can comfortably and securely sit on the bedpan. The shallow end is designed to fit under the buttocks, while the deeper end is used to collect the waste.
A nurse is caring for a client who has a high fever. Which of the following actions should the nurse take?
Explanation
Choice A Reason:
Apply a bath blanket between the client and a cooling blanket.
This helps to avoid direct skin contact with the cooling blanket, which can be too cold and uncomfortable for the client. A bath blanket or a thin sheet between the client and the cooling blanket provides a barrier, making the cooling process more tolerable.
Choice B Reason:
Covering the client with heavy blankets after shivering subsides is not appropriate when trying to reduce a high fever. This action can trap heat and further increase the client's body temperature.
Choice C Reason:
Placing ice packs on the client's neck and behind the knees is not typically recommended. Direct application of ice packs to the skin can lead to cold injury or frostbite and is generally not used to reduce a fever.
Choice D Reason:
Giving the client a sponge bath using an alcohol-water solution is not recommended. Using alcohol for a sponge bath can cause skin dryness, and the evaporation of alcohol can make the client feel even colder. It's better to use lukewarm water for a sponge bath if necessary to help lower the fever.
A charge nurse in a long-term care facility is preparing an educational program about delirium for newly hired nurses. Which of the following statements should the nurse plan to include?
Explanation
Choice A Reason:
A. Delirium can indeed affect a client's sleep cycle. Clients with delirium often experience disturbances in their sleep-wake cycle, with periods of agitation and confusion at night and drowsiness during the day.
Choice B Reason:
B. Delirium does not have a slow progression. It is a condition characterized by its abrupt and acute onset, which is in contrast to other cognitive disorders like dementia, which have a more gradual progression.
Choice C Reason:
"Delirium has an abrupt onset." This statement is accurate because delirium typically has a sudden and acute onset, with a rapid change in a person's mental state and cognitive function. Delirium is characterized by fluctuations in consciousness, attention, and cognitive function, and it can develop over hours to days.
Choice D Reason:
Delirium does affect a client's perception of their environment. Clients with delirium may have distorted perceptions, hallucinations, and misinterpretations of their surroundings, leading to significant cognitive and perceptual disturbances.
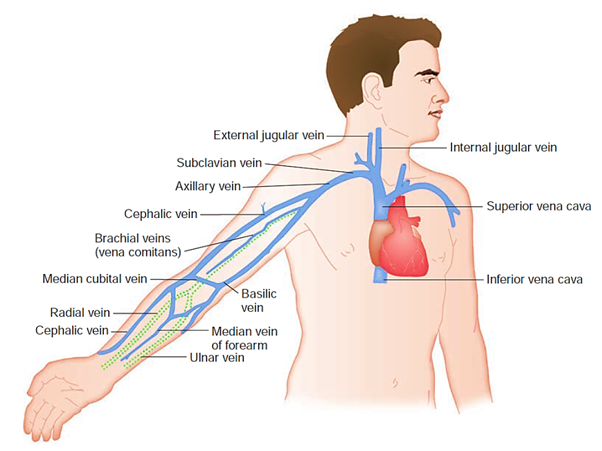
A nurse is preparing to insert an IV catheter for a client following a right mastectomy. Which of the following veins should the nurse select when initiating IV therapy?
Explanation
Choice A Reason:
The radial vein on the left wrist is not the best choice because it is on the same side as the right mastectomy, and it is advisable to avoid the same side as the surgical site to minimize potential complications.
Choice B Reason:
The cephalic vein on the back of the right hand is not a suitable choice because it is on the same side as the right mastectomy, and it is generally recommended to avoid the ipsilateral (same-side) arm for IV access in such cases.
When initiating IV therapy for a client following a right mastectomy, it is generally advisable to avoid the arm on the same side as the mastectomy (in this case, the right arm) to minimize the risk of complications. Therefore, the nurse should select a vein in the left arm.
Choice C Reason:
The cephalic vein in the left distal forearm is appropriate. Selecting a vein in the left arm, such as the cephalic vein in the left distal forearm, would help reduce the risk of lymphedema and other complications associated with the right mastectomy site. It is essential to choose an appropriate vein while considering the client's medical history and potential sources of complications.
Choice D Reason:
The basilic vein in the right antecubital fossa is also on the same side as the right mastectomy and should be avoided for the same reasons mentioned above.
A nurse is reviewing the medical record of a client who asks about the use of magnet therapy for pain relief. The nurse should identify that w of the following findings is a contraindication for receiving this type of therapy?
Explanation
Choice A Reason:
A. The client has an implanted defibrillator. Magnet therapy involves the use of magnets to promote pain relief, and it can have potential effects on electrical devices and equipment. In the case of an implanted defibrillator, there is a concern that strong magnetic fields from the therapy might interfere with the functioning of the defibrillator, potentially causing harm to the client. Therefore, individuals with implanted defibrillators should generally avoid magnet therapy.
Choice B Reason:
The client has a prescription for metoprolol: Having a prescription for metoprolol, a beta-blocker, is not a contraindication for magnet therapy. Metoprolol is not typically associated with contraindications related to magnet therapy.
Choice C Reason:
The client has a history of alcohol use disorder: A history of alcohol use disorder is not specifically related to a contraindication for magnet therapy. While alcohol use disorder can have other health implications, it does not directly impact the use of magnet therapy for pain relief.
Choice D Reason:
The client is allergic to penicillin: Being allergic to penicillin is unrelated to the use of magnet therapy for pain relief. Allergies to antibiotics like penicillin pertain to drug use and have no direct bearing on magnet therapy.

A nurse is teaching a client who is about to undergo a bowel resection about advance directives. Which of the following instructions should the nurse include in the teaching?
Explanation
Choice A Reason:
"You are required to sign advance directives prior to having surgery" is not accurate. While healthcare providers may encourage or recommend advance directives, they are not typically required before surgery.
Choice B Reason:
"You will receive written information about advance directives prior to signing." This statement is important because it emphasizes that the client should receive written information about advance directives before making any decisions or signing any documents. Providing written information allows the client to make an informed choice about whether to create or update advance directives.
Choice C Reason:
"Your provider must sign the advance directives before surgery" is not a typical requirement. Advance directives are primarily signed by the individual (the client) to express their own preferences regarding medical care.
Choice D Reason:
"Your partner must be present when you sign the advance directives" is not a standard requirement for signing advance directives. The decision to create or update advance directives is a personal one, and the presence of a partner is not typically necessary for this process.
A nurse is preparing to insert an IV catheter for an adult client. Which of the following actions should the nurse take?
Explanation
Choice A Reason:
Choosing the most proximal site on the extremity selected is not necessary, and the site selected should depend on the healthcare provider's preferences and the condition of the client's veins.
Choice B Reason:
Placing the extremity in a dependent position (hanging down) is not typically required for IV catheter insertion. The extremity should be in a comfortable and accessible position for the procedure.
Choice C Reason:
Place the tourniquet below the proposed insertion site. Placing the tourniquet just below the proposed insertion site is the correct technique. The tourniquet should be positioned to occlude the veins, making it easier to access a suitable vein for the IV catheter. Placing it below the proposed site allows for better visualization and access to the veins in the chosen area.
Choice D Reason:
Applying a cool compress for several minutes before insertion of the IV catheter is not a standard practice and is not typically needed for IV insertion. It may even cause vasoconstriction and make it more challenging to access veins.
A nurse is teaching a newly licensed nurse about the care of a client who has a methicillin-resistant Staphylococcus aureus. Which of the following statements by the newly licensed nurse indicates an understanding of the teaching?
Explanation
Choice A Reason:
"I will tell the client's visitors to wear a mask when they are within 3 feet of the client" is not typically required for MRSA. Visitors may need to adhere to standard hand hygiene practices, but wearing a mask within a certain distance of the client is not a standard precaution for MRSA.
Choice B Reason:
"I will place the client in a private room." This statement is correct because clients with MRSA are often placed in private rooms to prevent the spread of the infection to other clients. Private rooms help to reduce the risk of transmission to other individuals in the healthcare facility.
Choice C Reason:
"I will wear an N95 respirator mask when caring for the client" is generally not necessary for routine care of clients with MRSA. N95 respirators are typically used when dealing with airborne infectious diseases. Standard precautions, including gloves and gowns, are usually sufficient for MRSA.
Choice D Reason:
"I will remove my gown before my gloves after providing client care" is not the recommended sequence. The correct sequence is to remove gloves first to avoid contaminating the hands while removing the gown. This practice is important for infection control.
A nurse is caring for a client following a bilateral mastectomy. The client is often tearful and avoids looking at her dressings. Which of the lowing actions should the nurse take first?
Explanation
Choice A Reason:
Referring the client to a breast cancer support group can be beneficial, but it should follow the assessment and identification of the client's specific emotional needs and concerns.
Choice B Reason:
Providing the client with a mirror is not the first action to take. The client's emotional needs should be addressed before encouraging her to look at her incisions.
Choice C Reason:
Identify the impact of the mastectomy on the client's body image. Understanding and addressing the client's emotional and psychological response to the mastectomy is a priority. The client's feelings of sadness and avoidance suggest that she may be experiencing significant emotional distress and body image concerns. Identifying the impact on her body image allows the nurse to provide the appropriate emotional support and interventions.
Choice D Reason:
Encouraging the client to assist with her dressing changes can be important for her involvement in her care, but it should also come after addressing her emotional needs and concerns related to body image and distress.

A nurse is preparing to administer several medications via NG tube to a client who is receiving a continuous tube feeding. Which of the following actions should the nurse take?
Explanation
Choice A Reason:
Flushing the NG tube with 5 mL of sterile water before administration is not necessary when giving medications via the tube if they are properly mixed in a single syringe. It's an extra step that may not be required.
Choice B Reason:
Combining the medications with the formula in the feeding bag is generally not recommended because it can lead to interactions between the medications and the feeding formula, potentially reducing the effectiveness of the medications.
Choice C Reason:
Diluting each crushed medication with sterile water is not typically needed if the medications are properly mixed in a single syringe. Diluting medications separately can add unnecessary complexity to the process and may not be required if the medications are well-crushed and can be mixed together effectively.
Choice D Reason:
Mix the medications together in a single syringe. Mixing the medications in a single syringe minimizes the number of times the nurse has to flush the NG tube, reducing the risk of clogs and ensuring that the medications are adequately delivered to the stomach.

A nurse is caring for a client who has wrist restraints after an episode of violent behavior. Which of the following actions should the nurse take?
Explanation
Choice A Reason:
Tying the restraints to the side rail can be dangerous and is not a recommended practice. Restraints should be secured to designated restraint bed frame attachments, not side rails.
Choice B Reason:
Removing the restraints every 3 hours without proper evaluation and documentation may not be appropriate and should be done in accordance with the healthcare facility's restraint policy and the client's individual assessment.
Choice C Reason:
Securing restraints with a square knot may not be the best method as it can be challenging to release quickly in the event of an emergency. Restraints should be secured using quick-release, non-slip knots as per the facility's guidelines.
Choice D Reason:
Remove one restraint at a time. It is important to remove restraints one at a time to ensure that the client's safety is maintained. This approach allows the client to retain some degree of mobility and dexterity with one hand while the other hand remains restrained. This helps prevent injury while maintaining safety.
A nurse is caring for a client who is scheduled for surgery. While the nurse is witnessing the client's signature, the client states, "I trust my doctor, but I don't understand what is meant by resecting my intestines." Which of the following actions should the nurse take?
Explanation
Choice A Reason:
Providing brochures about the procedure may be helpful, but the immediate need is to address the client's concerns and questions directly.
Choice B Reason:
Notifying the provider may be necessary in certain situations, but it is not the nurse's first action in this case. The immediate priority is to ensure the client's understanding and informed consent.
Choice C Reason:
Describe the surgery to the client. It is important for the nurse to provide the client with a clear explanation of the surgery and what is meant by "resecting the intestines." The nurse should use simple and understandable language to help the client gain a better understanding of the procedure. This promotes informed consent, ensuring that the client fully comprehends what is about to take place.
Choice D Reason:
Completing an incident report is not appropriate in this situation. An incident report is typically used for documenting events related to actual incidents or errors, and the client's question does not constitute an incident or error. The focus should be on communication and education in this case.
A home health nurse is teaching a client about home safety. Which of the following statements by the client indicates an understanding of the teaching? (Select all that apply.)
Explanation
Choice A Reason:
"I need to have a fire escape plan with my family." Having a fire escape plan and discussing it with family members is an important safety measure.
Choice B Reason:
"I need to set my hot water heater to 140 degrees Fahrenheit." A water heater set at 140 degrees Fahrenheit poses a scalding risk, and it is generally recommended to set it to a lower temperature (usually around 120 degrees Fahrenheit) to prevent burns.
Choice C Reason:
"I will apply tape over frayed areas of electrical cords." Taping over frayed areas of electrical cords is not a safe practice and can increase the risk of electrical hazards. Damaged cords should be replaced, not taped.
Choice D Reason:
D. "I will use the grab bars when getting in and out of the bathtub." Using grab bars in the bathroom helps prevent slips and falls, enhancing safety during bathing.
Choice E Reason:
"I need to check my medications for expiration dates." Checking medications for expiration dates is crucial for medication safety and effectiveness.
A nurse is caring for a client who has a prescription for a 250 mL IV fluid bolus. The nurse administers a 500 mL IV bolus. Which of the following actions should the nurse take first?
Explanation
Choice A Reason:
Documenting the fluid infusion in the client's chart is an important step, but it should follow the assessment and management of the client's condition. Accurate documentation is crucial, but the client's health takes precedence.
Choice B Reason:
Reporting the incident to the unit manager is an important step to ensure that appropriate follow-up and corrective actions are taken, but it should follow the assessment of the client's condition.
Choice C Reason:
Completing an incident report is essential for tracking and analyzing the error, implementing corrective actions, and preventing a recurrence. However, it is not the immediate action to take when the client's well-being is in question. The client's vital signs and condition should be addressed first.
When a nurse administers the incorrect IV fluid bolus volume, the first and most important action is to ensure the safety and well-being of the client. Therefore, the nurse should:
Choice D Reason:
Obtain the client's vital signs. Assessing the client's vital signs is the priority to monitor the immediate impact of the incorrect IV fluid bolus. It helps identify any potential adverse effects, such as fluid overload or electrolyte imbalances. Once the client's condition is stable and any necessary interventions have been initiated, further actions should be taken:
A nurse is caring for a client who is receiving a warm, moist compress to relieve lower back pain. Which of the following findings should indicate to the nurse that the compress has been effective?
Explanation
Choice A Reason:
The client laughing at a television show might be a sign of improved mood or distraction but does not necessarily indicate pain relief.
Choice B Reason:
The client's skin on the lower back is intact without redness. An effective warm, moist compress should provide pain relief without causing skin irritation or damage. The absence of redness or skin breakdown suggests that the compress is not causing harm and is achieving its intended purpose.
Choice C Reason:
The client stating that they can concentrate while reading may suggest improved focus but does not directly address pain relief.
Choice D Reason:
The client's vital signs being within the expected reference range is a general assessment of physiological stability but does not specifically measure pain relief or the effectiveness of the warm, moist compress.
A nurse is preparing to administer IV fluids to a client. The nurse notes sparks when plugging in the IV pump. Which of the following actions should the nurse take first?
Explanation
Choice A Reason:
Unplug the pump. Unplugging the pump immediately stops the potential electrical hazard and ensures the client's safety. This should be the first action taken in response to sparks when plugging in an electrical device.
Choice B Reason:
Notifying the biomedical department to fix the pump is an important step, but it is not the first action to take in response to sparks, as this does not immediately address the potential safety hazard.
Choice C Reason:
Labeling the pump with a defective equipment sticker is a subsequent action that can help identify the equipment as faulty. However, it does not eliminate the immediate electrical hazard.
Choice D Reason:
Obtaining a replacement pump can be necessary, but it should come after the immediate safety concern is addressed by unplugging the current pump.
A nurse is caring for a client who is scheduled to have his alanine aminotransferase (ALT) level checked. The client asks the nurse to explain the laboratory test. Which of the following is an appropriate response by the nurse?
Explanation
Choice A Reason:
"This test will provide information about the function of your liver." The ALT test specifically assesses liver function by measuring the levels of alanine aminotransferase, an enzyme found in the liver. Elevated ALT levels can indicate liver damage or disease.
Choice B Reason:
Checking how the kidneys are working is typically assessed using tests such as creatinine and blood urea nitrogen (BUN) levels.
Choice C Reason:
Determining how the heart is performing is usually assessed through tests like electrocardiograms (ECG or EKG) and cardiac enzyme tests, not ALT.
Choice D Reason:
Indicating the risk for developing blood clots is usually assessed using tests like prothrombin time (PT) and international normalized ratio (INR) to evaluate blood clotting factors.
A nurse is preparing a sterile field to assist with suturing a client's laceration. Which of the following actions should the nurse take?
Explanation
Choice A Reason:
Pouring the sterile solution with the bottle held 20 cm (8 in) above the sterile bowl is a correct action, but it doesn't address maintaining sterility.
Choice B Reason:
Applying sterile gloves before opening the bottle of sterile solution is generally recommended to maintain sterility but is not specific to the action of holding the bottle.
Choice C Reason:
Placing the lid of the sterile solution bottle face down on the sterile drape is not recommended because the inside of the lid is sterile, and placing it face down could result in contamination when removed.
Choice D Reason:
Hold the bottle of sterile solution so that the label is facing the palm of the hand. This ensures that the label, which is a non-sterile part of the bottle, faces inward and away from the sterile field, reducing the risk of contamination. Keeping the label facing the palm helps maintain sterility.
A nurse is assessing a client who has diabetes mellitus prior to performing a blood glucose test. Which of the following findings should the nurse that the client has hyperglycemia?
Explanation
Choice A Reason:
Cool skin is not a typical sign of hyperglycemia. Hyperglycemia can cause skin to be warm or hot, but cool skin is more often associated with conditions like hypoglycemia (low blood sugar).
Choice B Reason:
Shakiness is more commonly associated with hypoglycemia (low blood sugar) rather than hyperglycemia.
Choice C Reason:
Confusion can occur in both hyperglycemia and hypoglycemia, so it is not a specific indicator of hyperglycemia on its own.
Choice D Reason:
Thirst. Hyperglycemia is associated with increased thirst (polydipsia) as the body attempts to rid itself of excess glucose by increasing urine output. This leads to dehydration, which triggers thirst.
A nurse is preparing to administer a controlled substance to a client for pain management. Which of the following actions should the nurse take?
Explanation
Choice A Reason:
Verifying the count total of the controlled substance after removing the amount needed is a good practice but does not directly address reporting discrepancies or irregularities.
Choice B Reason:
Asking a second nurse to record her signature when wasting any unused portion of the controlled substance is related to the documentation process when wasting unused portions, not the initial administration. It is important but not the primary action for administering the medication.
Choice C Reason:
Report any discrepancy in the count total of the controlled substance after administration. This is an essential step to address any discrepancies or irregularities in the count total, which helps maintain accurate records and prevent diversion or unauthorized access to the controlled substance.
Choice D Reason:
Placing the wasted portion of the controlled substance in the sharp container is the proper disposal method for sharps and medical waste but does not address the initial administration of the controlled substance.
Sign Up or Login to view all the 59 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
