RN HESI Paediatrics Exam 2
Total Questions : 53
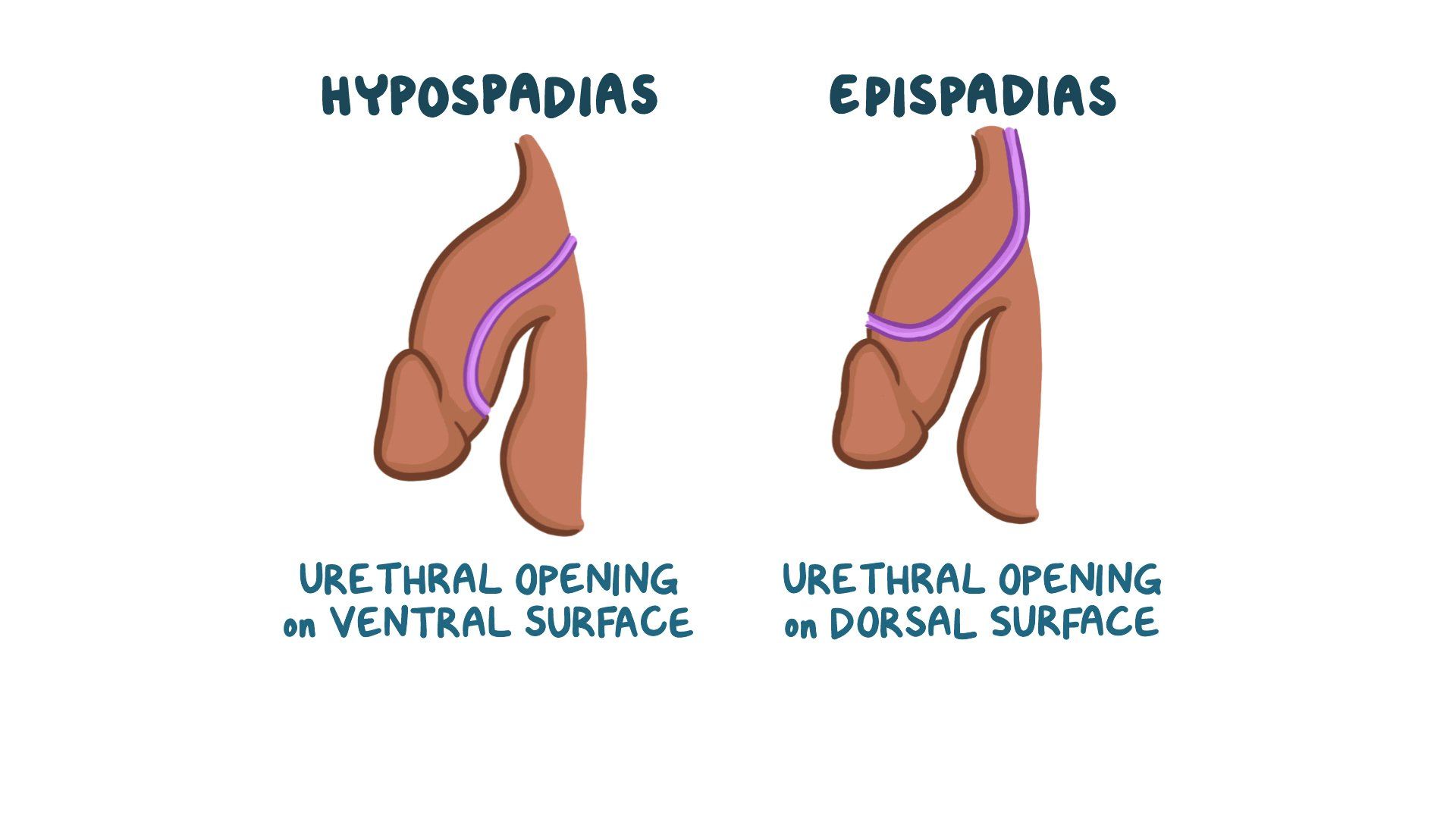
Showing 25 questions, Sign in for moreThe parents of a newborn infant with hypospadias are concerned about when the surgical correction should occur. Which information should the nurse provide?
Explanation
A. Surgery should be done by one month to prevent bladder infections. This statement is not accurate. While early surgery is generally recommended, the one-month timeframe is not a strict rule. The primary reason for early correction is to improve the cosmetic appearance of the penis, but it is not primarily aimed at preventing bladder infections.
B. Repair should be done before the child is potty-trained.
Hypospadias is a congenital condition where the opening of the urethra is on the underside of the penis rather than at the tip. Surgical correction is typically recommended, and the timing of the surgery is an important consideration.
C. The urethral repair should be done after sexual maturity. This statement is incorrect. Delaying the repair until sexual maturity is not the standard approach. In fact, earlier surgical correction is often recommended to ensure proper urinary function and to avoid potential psychological and social issues in the child.
D. Delaying the repair until school age reduces castration fears. This statement is not supported by current medical practice. Delaying the repair until school age can lead to psychosocial issues, as children may become more self-aware of their condition and experience teasing or psychological distress.
A 7-year-old child is admitted to the hospital with a diagnosis of acute rheumatic fever. In obtaining a health history from the child's mother, the recent occurrence of which illness is most significant?
Explanation
A. Chickenpox is caused by the varicella-zoster virus and is not directly related to the development of acute rheumatic fever.
B. Mumps is caused by the mumps virus and is not directly related to the development of acute rheumatic fever.
C. Sore throat.
Acute rheumatic fever (ARF) is an inflammatory condition that can occur after an untreated or inadequately treated streptococcal throat infection, such as streptococcal pharyngitis (strep throat). It is caused by group A Streptococcus bacteria.
In ARF, the body's immune response to the streptococcal infection can lead to inflammation and damage to various parts of the body, including the heart, joints, skin, and central nervous system. One of the major criteria for diagnosing ARF is a history of a sore throat. Therefore, the most significant recent occurrence for the health history in this case would be a sore throat (option C).
D. Influenza is caused by the influenza virus and is not directly related to the development of acute rheumatic fever.
An 8-year-old girl with precocious sexual development is being treated medically with injections of luteinizing hormone-releasing hormone (LHRH) to regulate the pituitary gland. Which statement by the parents indicates that they understand the treatment?
Explanation
A. "We should be sure to start our daughter on birth control pills." This statement is not directly related to LHRH treatment for precocious sexual development. The primary goal of LHRH treatment is to delay sexual development, and birth control pills are typically not necessary for this purpose.
B. "Sexual maturity differences between my daughter and her peers will disappear within a few years."
In a case of precocious sexual development, treatment with luteinizing hormone-releasing hormone (LHRH) is often used to delay sexual development and slow down the maturation process. It is not typically a lifelong treatment. The primary goal is to allow the child to develop at a more typical pace, so they can catch up with their peers and avoid the psychosocial challenges associated with early sexual maturity. Therefore, the statement in option B indicates a correct understanding of the treatment, as it recognizes that the differences in sexual maturity between the child and her peers should diminish over time.
C. "Our daughter will be on this hormone treatment the rest of her life." This statement is not accurate. LHRH treatment is usually a temporary measure to delay sexual development. It is not a lifelong treatment.
D. "We should encourage her to dress in clothing that suits her sexual maturity level." While this is a consideration for supporting a child with precocious sexual development, the primary treatment aspect is the LHRH therapy itself, which is aimed at delaying sexual development. This statement does not directly address the treatment process.
The nurse is providing treatment education to the caregiver of a school-age child recently diagnosed with attention-deficit/hyperactivity disorder (ADHD). Which statement(s) made by the caregiver demonstrates an understanding of the education? (Select all that apply.)
Explanation
A - Maintaining a consistent home schedule is an essential strategy for managing ADHD, as routines and structure can help the child stay organized and focused.
B - Understanding that nonstimulant medications can also be beneficial in the treatment of ADHD is correct, as nonstimulant medications are an alternative or additional treatment option for some individuals with ADHD. It's important to have a comprehensive understanding of available treatment options.
C - The statement "Know that medication is the best approach to treatment" is not accurate. Medication can be an effective component of ADHD treatment, but it is not necessarily the best approach for every child. Treatment plans should be individualized and may include a combination of strategies, such as behavioral interventions, psychoeducation, and medication.
D - Creating an organization chart for tasks is a helpful approach for children with ADHD to manage their responsibilities and activities effectively.
E - Anticipating being automatically entered into a specialized education plan is not necessarily accurate. While some children with ADHD may benefit from an Individualized Education Plan (IEP) or a 504 Plan in the educational setting, these plans are typically established based on specific assessments and the child's needs.
F - Designating an established area for study is important for creating a distraction-free environment, which can support the child's ability to focus on their schoolwork.
A 10-year-old boy has been seen frequently by the school nurse over the past three weeks after school begins in the fall. He reports headaches, stomach aches, and difficulty sleeping. Which intervention should the nurse implement?
Explanation
A. Comparing the child's vital signs over the past three weeks (option A) may not provide significant information about the underlying cause of his symptoms, as vital signs are unlikely to directly indicate stress or emotional distress.
B. Counseling the parents to pay more attention to the child (option B) is a general suggestion and may not be the most effective way to address the specific issues he is facing. It's important to identify the underlying causes and stressors first.
C. Conducting a complete neurological assessment (option C) is not warranted at this stage, as the child's symptoms are more likely related to emotional or psychological factors rather than a neurological problem. Gathering information about his school experiences would be a more appropriate initial step.
D. Ask the boy to describe a typical day at school.
The child's reported symptoms, including headaches, stomach aches, and difficulty sleeping, may be indicative of stress or emotional issues. To better understand and address the underlying cause of these symptoms, it's important to gather more information about the child's daily experiences. By asking the boy to describe a typical day at school (option D), the nurse can uncover potential stressors or challenges he may be facing, such as academic difficulties, bullying, social issues, or other stressors that might be contributing to his symptoms.
The nurse is assessing a 6-month-old infant. Which response requires further evaluation by the nurse?
Explanation
A. Plays "peek-a-boo."
This is a social and cognitive milestone. Infants typically develop social interactions like peek-a-boo around 6-9 months of age. This behavior is normal for a 6-month-old and demonstrates social engagement.
B. Has doubled birth weight.
Infants generally double their birth weight by around 6 months of age. This is a typical growth and developmental milestone, indicating adequate nutrition and growth.
C. Turns head to locate sound.
This is a normal developmental milestone for an infant. By 6 months of age, infants should demonstrate localization of sounds, indicating appropriate auditory and neurological development.
D. Demonstrates startle reflex.
The startle reflex, also known as the Moro reflex, is normal in newborns but typically disappears by 3-6 months of age. If a 6-month-old still exhibits this reflex, it could be a sign of delayed neurological development and might require further evaluation.
The nurse is giving an intramuscular injection of an antibiotic to a 16-month-old toddler with pneumonia. The toddler does not have any known allergies and has been walking without assistance for one month. Which technique should the nurse select for administration?
Explanation
A. Giving the injection in the arm, one to 2 inches below the acromion process, is a technique typically used for adults or older children. It may not be suitable for a toddler of this age.
B. Using a needle length of 1/2 inch is not appropriate for intramuscular injections in a toddler. It may not reach the muscle tissue, leading to ineffective administration.
C. Dividing the gluteal area into quarters and giving the injection into the upper outer quadrant is a technique typically used for older children and adults, not for toddlers. It's also important to avoid intramuscular injections in the gluteal area for young children due to the risk of injury to the sciatic nerve.
D. Administering the injection into the middle of the lateral aspect of the thigh is the preferred technique for intramuscular injections in toddlers. The thigh muscles are a safe and effective site for IM injections in this age group. The middle of the lateral aspect of the thigh is commonly chosen because it provides a sufficient muscle mass for proper absorption of the medication and minimizes the risk of injury to nerves or vessels. This technique is recommended for toddlers who are walking and have developed sufficient muscle mass in the thigh area.
A 9-year-old admitted to the unit with severe abdominal pain and fever is diagnosed with appendicitis and is placed on the surgery schedule for an appendectomy. The child reports to the nurse of experiencing sudden relief in abdominal pain. Which action should the nurse take first?
Explanation
A. Documenting the client's relief of pain is important for the medical record but is not the first priority in this situation. The immediate concern is to determine the cause of the sudden pain relief and ensure the child's well-being.
B. Inquiring about the client's last meal is important for pre-operative considerations, but it is not the first action to take when sudden relief of abdominal pain is reported.
C. Giving prescribed intravenous antibiotics may be part of the treatment plan, but it should not be the first action when the child experiences sudden relief of abdominal pain. Contacting the healthcare provider to assess the situation is more urgent.
D Contact the healthcare provider.
In the case of a child diagnosed with appendicitis, sudden relief in abdominal pain can be concerning. This might indicate that the appendix has ruptured, leading to the spread of infection into the abdominal cavity, which can be a critical situation. It's essential for the healthcare provider to be informed immediately so they can assess the child's condition, order any necessary interventions, and potentially expedite the surgical procedure if required.
The nurse is caring for a school-age child with crusting and swollen eyelids, purulent drainage, and inflamed conjunctiva. The child receives a prescription for an ophthalmic antiinfective ointment. Which instruction should the nurse provide the child's caregivers during discharge education?
Explanation
A. Discontinuing the ointment once drainage resolves is not the correct instruction. It's important to complete the full course of prescribed ophthalmic antiinfective ointment as directed by the healthcare provider, even if the symptoms improve, to ensure that the infection is completely treated.
B. Instructing caregivers to remove secretions by wiping toward the opposite eye is not appropriate. When cleaning the eye, it's important to wipe from the inner corner of the eye (near the nose) outward to prevent any potential contamination from one eye to the other.
C. Using a disposable moist wipe to remove eye crusts is the correct instruction. This helps prevent contamination and injury to the eye while gently cleaning away any crusting and purulent discharge. Caregivers should use a fresh, clean wipe for each eye and dispose of it properly.
D. Preparing the child for blurry vision after ointment application is not a necessary instruction in this case. While some ointments may temporarily cause blurry vision due to their consistency, this is not the primary concern for the caregiver's education in this scenario. The main focus should be on proper hygiene and administration of the ointment.
The nurse is assessing the lung sounds of a preschooler. Which action should the nurse Implement to ensure the child's cooperation?
Explanation
A. Offering the child bubbles before the stethoscope is placed is an excellent strategy to gain the child's trust and cooperation. Blowing bubbles can be a fun and engaging activity that helps distract and relax the child before the assessment.
B. Having the child blow a cotton ball and having the parent catch it might be a fun activity, but it may not necessarily promote cooperation during the lung sound assessment. It's not directly related to the assessment and may not be as effective as offering bubbles.
C. Placing a toy in the child's hands while listening to breath sounds can be a helpful distraction, but bubbles are more likely to engage the child's attention and provide a positive experience during the assessment.
D. Allowing the child to use a stethoscope on a stuffed animal is a good idea for play and education but may not be as effective in ensuring cooperation during the assessment itself. Bubbles are more likely to capture the child's attention and make them more comfortable with the assessment process.
A newborn with a repaired gastroschisis is transferred to the pediatric unit after several days in the pediatric intensive care unit. The infant is receiving parenteral nutrition and continuous enteral feedings. To maintain normal growth and development of the infant, which action should the nurse include in plan of care?
Explanation
A. Ensuring placement of the enteral tube with an abdominal x-ray is crucial in this situation. Infants with gastroschisis may have had surgical repairs, and it's important to confirm that the enteral tube is correctly positioned in the gastrointestinal tract to prevent complications and ensure the infant is receiving the enteral feedings as intended.
B. Speaking to the healthcare provider about instituting physical therapy may be a valuable consideration for the infant's overall care, but it is not directly related to maintaining growth and development in the context of enteral feedings and gastroschisis.
C. Offering a pacifier for non-nutritive sucking can be comforting to the infant but is not directly related to maintaining growth and development in the context of enteral feedings.
D. Using sterile technique during feedings is important for infection prevention but may not be the primary concern when the infant is receiving continuous enteral feedings. Ensuring correct tube placement with an abdominal x-ray is the primary action for maintaining normal growth and development in this case.
During a well baby clinic visit, the mother of a 6-month-old infant asks the nurse if she can have a prescription for liquid multivitamin with fluoride. Though the infant is still breast feeding, the mother provides the child with supplemental formula feedings. Which assessment is most important for the nurse to obtain?
Explanation
A. While it's essential to monitor the infant's weight gain and the type of formula taken daily, this information is important for tracking growth and nutrition but is not directly related to the use of liquid multivitamin with fluoride.
B. The newborn's gestational age assessment is typically relevant during the immediate postnatal period and may not be as crucial at 6 months of age.
C. The water source used with supplemental feedings is critical when considering the use of liquid multivitamin with fluoride. Fluoride is often recommended to prevent tooth decay, and it's essential to know the fluoride content in the water source to determine whether additional supplementation is needed. If the water source has adequate fluoride, the infant may not require a fluoride supplement.
D. While the infant's current hemoglobin and hematocrit levels are important for assessing anemia, this assessment is not directly related to the request for a prescription for liquid multivitamin with fluoride. In summary, assessing the water source used for supplemental feedings is crucial to determine the necessity of a fluoride supplement, which is the primary concern in this scenario.
While obtaining the vital signs of a 10-year-old child who had a tonsillectomy this morning, the nurse observes the child swallowing every 2 to 3 minutes. Which assessment should the nurse implement?
Explanation
A. Assessing for teeth clenching or grinding is not the most appropriate assessment in this situation. While teeth clenching or grinding may indicate discomfort or anxiety, it may not directly address the specific concern of post-operative bleeding after a tonsillectomy.
B Inspect the posterior oropharynx.
Observing a child who has had a tonsillectomy frequently swallowing may raise concerns about post-operative bleeding. Inspecting the posterior oropharynx is essential to assess for any signs of bleeding, such as fresh blood or bleeding sites.
C. Asking the child to speak to evaluate a change in voice tone is not the primary assessment needed in this scenario. The primary concern is to assess for any signs of bleeding, and this can be done by inspecting the posterior oropharynx.
D. Touching the tonsillar pillars to stimulate the gag reflex is not necessary and may not be well-tolerated by the child who has had a tonsillectomy. It's also not the primary assessment to address the concern of post-operative bleeding.
A six-year-old girl is being admitted to the hospital for repair of an umbilical hernia. Which information, collected by the admitting nurse, is particularly helpful in planning care for this child?
Explanation
A. Reactions to any previous hospitalizations can provide some insight into the child's previous healthcare experiences, but it may not be as directly relevant to planning care for an umbilical hernia repair.
B. A history of rubella, rubeola, or chicken pox is important for the child's medical history, but it may not be the most critical information when planning care for an umbilical hernia repair.
C. The mother's use of alcohol, drugs, or cigarettes during pregnancy is particularly relevant when planning care for a child undergoing surgery, as it can affect the child's overall health and potential complications during and after the procedure. Exposure to these substances during pregnancy can lead to various health issues that need to be considered in the child's care plan.
D. A list of achievement timeline for developmental milestones is important for understanding the child's developmental progress, but it may not be the primary consideration when planning care for an umbilical hernia repair.
The nurse is providing education to parents about preventing otitis media recurrence in their infant. Which instruction should the nurse include?
Explanation
A. Breastfeeding frequently is generally recommended for infant health, but it is not specifically related to preventing otitis media recurrence. It has other health benefits for infants.
B. Positioning the infant prone (face down) after feeding is not recommended, and it does not relate to preventing otitis media recurrence. The recommended sleep position for infants is on their back to reduce the risk of sudden infant death syndrome (SIDS).
C. Avoiding smoke exposure is a crucial instruction for preventing otitis media recurrence. Exposure to secondhand smoke is a known risk factor for ear infections in children. It can lead to increased susceptibility to respiratory infections, which can subsequently increase the risk of otitis media.
D. Inspecting the infant's ears daily is not a primary preventive measure for otitis media recurrence. While it's essential to monitor the child's health, checking the ears daily is not a standard practice for preventing ear infections.
The nurse is teaching the parents about important dietary changes for their child who is newly diagnosed with celiac disease. Which foods should the nurse include in the list of allowed foods for this child?
Explanation
Celiac disease is an autoimmune disorder in which individuals are unable to tolerate gluten, a protein found in wheat, barley, and rye. Therefore, foods containing wheat, barley, and rye should be avoided by individuals with celiac disease. The list of allowed foods should primarily consist of gluten-free options.
A. Rice is naturally gluten-free and is safe for individuals with celiac disease to consume.
B. Oats can be included in the diet of individuals with celiac disease, but they must be specifically labeled as "gluten-free oats." Regular oats can be cross-contaminated with gluten during processing, so it's important to choose certified gluten-free oats to avoid potential issues.
C. Rye contains gluten and should be avoided by individuals with celiac disease.
D. Barley contains gluten and should be avoided by individuals with celiac disease.
During her sports physical examination, a 15-year-old female requests oral contraceptives. She explains that she is sexually active and does not want her parents to know. Which action should the nurse take?
Explanation
While it is essential to prioritize the client's confidentiality and autonomy, it is also important to provide the client with information and education about the available options. In this case:
A. Telling the client how to receive free oral contraceptives from the clinic without addressing the client's need for information and counseling is not an adequate response. It's essential to ensure the client is well-informed about her choices.
B. Encouraging the client to discuss her need for contraceptives with her parents is a valid suggestion, but it may not always be practical or possible for every individual, and the client has already expressed her desire for confidentiality. The nurse should respect the client's autonomy and right to make her own healthcare decisions.
C. Explaining that parental approval is needed to receive contraceptives may discourage the client from seeking essential contraceptive services and may not align with the laws and regulations in many places that allow minors to access contraceptives confidentially.
D. Counseling the client about the risks and benefits of using oral contraceptives is an important step. This allows the client to make an informed decision about her sexual health and contraceptive options. The nurse should also discuss safer sex practices, regular healthcare check-ups, and the importance of open communication with healthcare providers.
When advising a new mother in caring for a child with croup, which symptom should be a priority concern to the telephone triage nurse?
Explanation
When advising a new mother in caring for a child with croup, the symptom that should be a priority concern to the telephone triage nurse is B.
Explanation:
A. A fever of 101.0°F (38.3°C) is a common symptom in many childhood illnesses, including croup, but it is not the primary concern when difficulty swallowing secretions is present.
B Difficulty swallowing secretions.
Croup is characterized by a barking cough and may also be associated with stridor (noisy breathing), hoarseness, and difficulty swallowing secretions. While all the symptoms mentioned can be concerning, difficulty swallowing secretions is a priority concern because it can potentially lead to respiratory distress if not managed appropriately. Thick secretions can cause airway obstruction, and prompt assessment and intervention are needed to ensure the child's airway remains clear and that the child is able to breathe effectively.
C. A barking cough, worse at night, is a classic symptom of croup and should be addressed, but difficulty swallowing secretions can have a more direct impact on the child's airway.
D. Crying often when nursing may be related to the discomfort caused by croup, but it is not as immediately concerning as difficulty swallowing secretions.
While the barking cough, hoarseness, and other croup symptoms should also be addressed, the priority is ensuring that the child is able to manage secretions effectively without respiratory distress. The telephone triage nurse should provide guidance to the mother on how to help the child manage these secretions and when to seek medical attention if the situation worsens.
The mother of an 11-year-old boy who has juvenile idiopathic arthritis tells the nurse, "I really don't want my son to become dependent on pain medication, so I only allow him to take it when he is really hurting." Which information is most important for the nurse to provide this mother?
Explanation
The most important information for the nurse to provide to the mother of an 11-year-old boy with juvenile idiopathic arthritis is B.
Explanation:
A. Encouraging quiet activities such as watching television as a pain distracter can be helpful, but it should be used in conjunction with appropriate pain management strategies.
B Giving pain medication around the clock helps control the pain.
Children with juvenile idiopathic arthritis often experience chronic pain and inflammation. It's important for the mother to understand that, in some cases, simply taking pain medication when the child is in severe pain may not be the most effective approach. Pain management in chronic conditions like arthritis typically involves a more proactive and regular approach.
C. While hot baths can be soothing and offer some pain relief, they may not provide sufficient pain control for chronic conditions like juvenile idiopathic arthritis. Using hot baths can be a complementary approach but may not replace the need for pain medication.
D. Encouraging the child to rest when experiencing pain is important, but it should also be combined with appropriate pain management. Rest alone may not provide adequate pain relief for a child with arthritis.
The key information here is that giving pain medication around the clock, under the guidance of a healthcare provider, can help provide continuous pain control and improve the child's quality of life. Parents should work closely with the healthcare team to develop a comprehensive pain management plan that may include a combination of medications, physical therapy, and lifestyle modifications.
The parents of a 14-month-old child who is hospitalized due to febrile seizures tell the nurse that they fear their child will have lifelong seizures. Which information should the nurse convey to these parents?
Explanation
A. Using ibuprofen prophylactically to prevent febrile seizures is not a standard approach and is not generally recommended. The focus should be on managing the child's fever with appropriate fever-reducing medications rather than attempting to prevent febrile seizures with medication.
B. Reassure the parents that febrile seizures decrease as the child grows older.
Febrile seizures are relatively common in young children and are typically associated with rapid increases in body temperature, often due to infections.
The most important information to convey to the parents is that febrile seizures are usually a benign and self-limited condition, and they tend to decrease in frequency and may even resolve as the child grows older. Reassuring parents about the natural course of febrile seizures is vital to alleviate their concerns. However, it's essential to educate them on fever management and when to seek medical attention for their child's febrile seizures.
C. Avoiding excessive visual stimuli is not a standard recommendation for preventing febrile seizures. Febrile seizures are primarily related to fever and not visual stimuli.
D. Providing a sponge bath for temperatures over 100.6° F (38.1° C) can help reduce fever, but it is not directly related to preventing febrile seizures. The main goal in such situations is to manage the fever itself.
A child diagnosed with Kawasaki disease is brought to the clinic. The mother reports that her child is imitable, refuses to eat, and has skin peeling on both hands and feet. Which intervention should the nurse instruct the mother to implement first?
Explanation
The intervention the nurse should instruct the mother to implement first for a child diagnosed with Kawasaki disease, who is irritable, refuses to eat, and has skin peeling on both hands and feet, is C.
Explanation:
A. Encouraging the parents to rest is important but may not directly address the child's symptoms.
B. Applying lotion to hands and feet may provide comfort for the skin, but addressing the child's refusal to eat is a more immediate concern.
C. Make a list of foods that the child likes.
Kawasaki disease is an acute inflammatory illness that can lead to various symptoms, including irritability, changes in appetite, and skin peeling, particularly on the hands and feet.
It's crucial to address the child's nutritional intake and ensure they are receiving appropriate nourishment, particularly when they are irritable and refusing to eat. By making a list of foods that the child likes, the mother can attempt to provide the child with familiar and preferred food options to help maintain their nutritional status during the illness.
D. Placing the child in a quiet environment can be helpful for comfort but may not address the child's nutrition and dietary needs.
A mother brings her 3-month-old infant to the clinic because the baby does not sleep through the night. Which finding is most significant in planning care for this family?
Explanation
A. The mother being a single parent and living with her parents may have an impact on the family dynamics and support system but is not the most significant finding when it comes to addressing the baby's sleep issues.
B. The baby being irritable during feedings is important information and should be addressed, but it may not be the most significant finding when it comes to the baby's sleep patterns.
C. The diaper area shows severe skin breakdown.
Severe skin breakdown in the diaper area can be indicative of several issues, including frequent diaper changes, diaper rash, or potential underlying health concerns. This finding suggests that the infant may have discomfort or pain related to the diaper area, which could be contributing to the baby's nighttime awakenings and sleep disturbances.
D. The infant's formula being changed twice may be relevant, but it is not as significant as severe skin breakdown, which can indicate immediate discomfort for the baby.
History and Physical
The client has a history of Wilms tumor with left radical nephrectomy diagnosed at age five for which he completed treatment nine months ago. A septic episode, while undergoing treatment for his Wilms tumor, resulted in an acute kidney injury. This injury, along with antibiotic therapy and chemotherapy, has resulted in chronic kidney disease. The client is followed by oncology and nephrology services.
Two days later, the nurse completes an assessment of the client. Which assessment findings indicate that the client has stabilized? Select all that apply.
Explanation
A. An electrocardiogram with a tall T wave and widened QRS complex may indicate electrolyte imbalances or cardiac issues, which are not indicative of stabilization.
C. Basilar crackles can be a sign of pulmonary or cardiac issues and are not indicative of stabilization.
D. A urine output of 20 mL in the last hour may suggest reduced kidney function or hydration status and is not indicative of stabilization.
E. A respiratory rate of 26 breaths/minute may indicate respiratory distress and is not indicative of stabilization.
The assessment findings that suggest stabilization include:
A blood pressure within the normal range (126/76 mm Hg).
A heart rate within the normal range (72 beats/minute).
Oxygen saturation of 98% on room air, indicating adequate oxygenation.
A normal body temperature (98.9°F or 37.1°C orally).
These vital signs and clinical parameters are within normal ranges, suggesting that the client's condition is stable at this time.
The client has a history of Wilms tumor with left radical nephrectomy diagnosed at age five for which he completed treatment nine months ago. A septic episode, while undergoing treatment for his Wilms tumor, resulted in an acute kidney injury. This Injury, along with antibiotic therapy and chemotherapy, has resulted in chronic kidney disease. The client is followed by oncology and nephrology services.
For each nursing action, click to indicate whether the action is indicated or contraindicated for this client's plan of care.
Each row must have only one response option selected.
Explanation
Continuous pulse oximetry monitoring is indicated for assessing oxygen saturation and respiratory status, especially in a client with a history of chronic kidney disease and a previous septic episode. It helps monitor the client's respiratory function.
Calculation of intake and output is indicated to assess fluid balance, which is crucial in clients with chronic kidney disease and a history of acute kidney injury. It helps monitor fluid management.
Daily weights are indicated to monitor fluid retention and changes in the client's weight, which can be affected by the client's kidney condition and the administration of intravenous fluids.
IV 0.9% normal saline continuous infusion at 100 mL/hr is indicated to maintain hydration and promote renal function in clients with chronic kidney disease. It helps ensure adequate fluid balance.
IV potassium-sparing diuretics may be contraindicated because they can potentially affect electrolyte balance, and in some cases, they might not be suitable for clients with chronic kidney disease. The use of diuretics should be carefully evaluated and managed by the healthcare provider.
The client has a history of Wilms tumor with left radical nephrectomy diagnosed at age five for which he completed treatment nine months ago. A septic episode, while undergoing treatment for his Wilms tumor, resulted in an acute kidney injury. This Injury, along with antibiotic therapy and chemotherapy, has resulted in chronic kidney disease. The client is followed by oncology and nephrology services.
The healthcare provider has assessed the client and completes initial orders. Which three care needs should the nurse prioritize for this client?
Explanation
For this client with a history of Wilms tumor, a radical nephrectomy, chronic kidney disease, and ongoing follow-up by oncology and nephrology services, the nurse should prioritize the following three care needs:
B Identifying cardiac arrhythmias: Given the history of chronic kidney disease and potential electrolyte imbalances, cardiac arrhythmias are a significant concern that should be assessed and monitored for.
F Monitoring fluid status: Fluid balance is crucial in clients with chronic kidney disease, and monitoring for fluid overload or dehydration is essential. This is especially important because of the potential need for fluid restrictions.
H Assessing for worsening respiratory status: Assessing respiratory status is important, as clients with chronic kidney disease may be at risk for respiratory complications, including fluid overload, pulmonary edema, or other issues that can impact their respiratory status.
The other options are not the top priorities based on the client's history and current condition:
A. Collaborating with a dietitian to prepare a low-protein diet is important but may not be the immediate priority.
C. Performing diagnostic testing to determine the cause of a fever is necessary, but it does not take precedence over the immediate concerns of cardiac arrhythmias, fluid status, and respiratory status.
D. Educating the client and family on the importance of fluid restrictions is important, but it is related to monitoring fluid status and may be part of ongoing care.
E. Administering antipyretic medication as needed is relevant for fever management but not a top priority until the cause of the fever is determined.
G. Reassessing vital signs is part of ongoing care but may not be the immediate priority over identifying cardiac arrhythmias and assessing for worsening respiratory status.
I. Investigating acid/base complications is important but may not be the immediate priority when cardiac, fluid, and respiratory status are concerns.
Sign Up or Login to view all the 53 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
