Rn paediatrics nursing (Marymount University)
Total Questions : 62
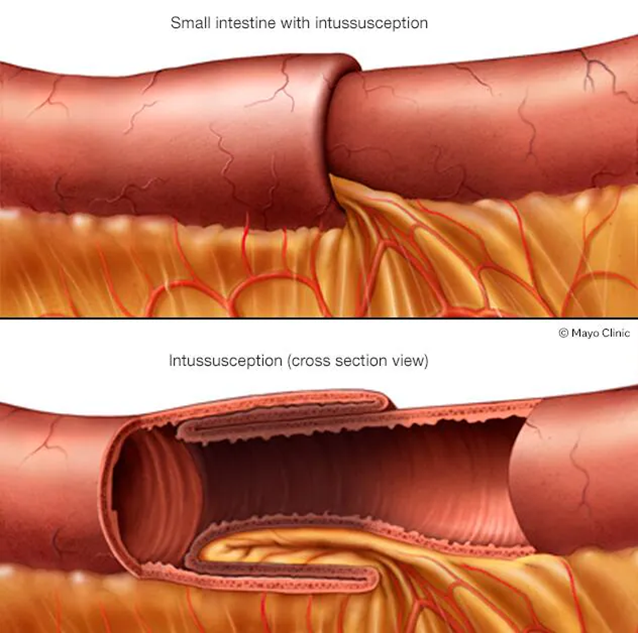
Showing 25 questions, Sign in for moreThe nurse is caring for a boy with probable intussusception. While waiting for a radiologist-guided pneumonia to visualize and correct the intussusception, the child passes a currant jelly-like stool. Which nursing action is the most appropriate?
Explanation
Choice A reason:
Measuring the abdominal girth is a useful assessment tool in cases of suspected abdominal distension or fluid accumulation. However, in the context of intussusception, the passage of a currant jelly-like stool is a more critical indicator of the condition. While measuring abdominal girth can provide additional information, it is not the most appropriate immediate action in this scenario.
Choice B reason:
Notifying the practitioner as this is not a typical finding is incorrect because the passage of currant jelly-like stool is a classic symptom of intussusception. This stool appearance results from a mixture of mucus and blood due to the telescoping of the intestine, which compromises blood flow and causes ischemia. Therefore, this finding should be documented as expected rather than considered atypical.
Choice C reason:
Documenting the passage of currant jelly-like stool as an expected finding and planning to move forward with the procedure is the most appropriate action. This stool appearance is a hallmark sign of intussusception, indicating that the condition is present and needs to be addressed promptly. The radiologist-guided pneumoenema is a diagnostic and therapeutic procedure that can help resolve the intussusception by using air pressure to unfold the telescoped segment of the intestine. Therefore, documenting this finding and proceeding with the planned intervention is crucial.
Choice D reason:
Auscultating for bowel sounds is a standard nursing assessment technique to evaluate gastrointestinal function. However, in the context of intussusception, the passage of currant jelly-like stool is a more definitive indicator of the condition. While auscultating for bowel sounds can provide additional information about bowel activity, it is not the most appropriate immediate action in this scenario.
A nurse is providing teaching to the parent of an infant who has gastroesophageal reflux. Which of the following statements by the parent indicates an understanding of the teaching?
Explanation
Choice A reason:
Feeding an infant with gastroesophageal reflux formula instead of breast milk is not necessary. Breast milk is often easier for infants to digest and can be beneficial for reducing reflux symptoms. According to the American Academy of Pediatrics, breastfeeding should be continued if possible, as it has numerous health benefits for both the infant and the mother. If formula feeding is necessary, specialized formulas designed for infants with reflux can be used, but this does not mean breast milk should be avoided.
Choice B reason:
Thinning the baby’s formula with water is not recommended. This practice can dilute the essential nutrients in the formula, leading to inadequate nutrition for the infant. Instead, thickening agents such as rice cereal can be added to the formula to help reduce reflux symptoms. This approach helps the formula stay down in the stomach and reduces the likelihood of regurgitation.
Choice C reason:
Positioning the baby side-lying during sleep is not recommended for infants with gastroesophageal reflux. The American Academy of Pediatrics advises that infants should be placed on their backs to sleep to reduce the risk of sudden infant death syndrome (SIDS). Side-lying or prone positions are not safe for sleep and do not effectively reduce reflux symptoms.
Choice D reason:
Keeping the baby in an upright position after feedings is the correct approach for managing gastroesophageal reflux. This position helps prevent the stomach contents from flowing back into the esophagus, reducing the likelihood of reflux. It is recommended to hold the baby upright for at least 20-30 minutes after feeding to allow gravity to assist in keeping the stomach contents down.
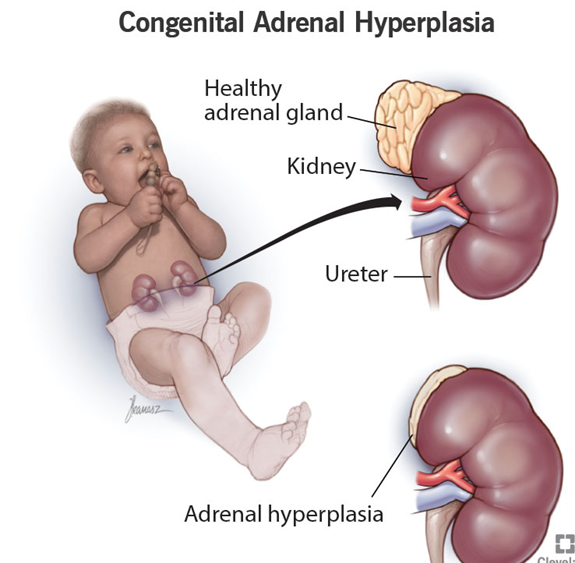
A neonate born with ambiguous genitalia is diagnosed with congenital adrenal hyperplasia (CAH). This is an autosomal recessive disorder which causes an overproduction of:
Explanation
Choice A reason:
Congenital adrenal hyperplasia (CAH) is a group of genetic disorders affecting the adrenal glands, which are responsible for producing vital hormones such as cortisol, aldosterone, and androgens. In CAH, there is a deficiency of the enzyme 21-hydroxylase, which is crucial for the synthesis of cortisol and aldosterone. As a result, the adrenal glands overproduce androgens, leading to symptoms such as ambiguous genitalia in newborns, early puberty, and rapid growth. Androgens are male sex hormones, including testosterone, which play a significant role in the development of male characteristics.
Choice B reason:
Vitamin K is a fat-soluble vitamin essential for blood clotting and bone health. It is not related to the overproduction of hormones in congenital adrenal hyperplasia. Vitamin K deficiency can lead to bleeding disorders, but it does not cause the symptoms associated with CAH, such as ambiguous genitalia or early puberty. Therefore, this choice is incorrect.
Choice C reason:
Gonadotropins are hormones produced by the pituitary gland that stimulate the gonads (ovaries and testes) to produce sex hormones and gametes (eggs and sperm). While gonadotropins play a role in sexual development and reproduction, they are not overproduced in congenital adrenal hyperplasia. The primary issue in CAH is the overproduction of androgens due to enzyme deficiencies in the adrenal glands. Therefore, this choice is incorrect.
Choice D reason:
Vitamin D is a fat-soluble vitamin essential for calcium absorption and bone health. It is not related to the overproduction of hormones in congenital adrenal hyperplasia. Vitamin D deficiency can lead to bone disorders such as rickets in children and osteomalacia in adults, but it does not cause the symptoms associated with CAH. Therefore, this choice is incorrect.
A nurse is preparing to perform an abdominal assessment on a child. Identify the sequence the nurse should follow. Move the steps into the box in order of performance:
Explanation
The correct answer is a) Inspection, b) Auscultation, c) Superficial palpation, d) Deep palpation.
Choice A reason:
Inspection is the first step in an abdominal assessment. This involves visually examining the abdomen for any abnormalities such as distension, scars, lesions, or asymmetry. The nurse should note the shape, contour, and any visible movements or pulsations. This step is crucial as it provides the initial information about the patient’s condition and helps guide the subsequent steps of the assessment.
Choice B reason:
Auscultation follows inspection in the sequence of an abdominal assessment. The nurse uses a stethoscope to listen for bowel sounds in all four quadrants of the abdomen. This step is performed before palpation to avoid altering the natural bowel sounds. The presence, frequency, and character of bowel sounds can provide valuable information about the gastrointestinal function and help identify any abnormalities such as bowel obstruction or ileus.
Choice C reason:
Superficial palpation is the third step in the abdominal assessment sequence. The nurse gently palpates the abdomen to assess for tenderness, muscle tone, and any superficial masses. This step helps identify areas of discomfort or pain and provides information about the condition of the abdominal wall and underlying structures. It is important to perform this step gently to avoid causing discomfort or pain to the patient.
Choice D reason:
Deep palpation is the final step in the abdominal assessment sequence. The nurse applies more pressure to palpate deeper structures within the abdomen. This step helps assess for any deep-seated masses, organ enlargement, or areas of tenderness that were not detected during superficial palpation. Deep palpation should be performed carefully to avoid causing pain or discomfort to the patient.
When caring for a child with probable appendicitis, the nurse would be alert to recognize which condition or symptom is a sign of perforation?
Explanation
Choice A reason:
Decreased abdominal distention is not typically a sign of appendicitis perforation. In fact, perforation often leads to increased abdominal distention due to the release of intestinal contents into the abdominal cavity, causing inflammation and swelling. Therefore, this choice is incorrect.
Choice B reason:
Anorexia, or loss of appetite, is a common symptom of appendicitis but not specifically indicative of perforation2. While anorexia can be present in cases of perforation, it is not a definitive sign. The sudden relief of pain is a more critical indicator of perforation, as it suggests the appendix has ruptured, temporarily relieving pressure.
Choice C reason:
Bradycardia, or a slow heart rate, is not a typical sign of appendicitis perforation. In fact, appendicitis and its complications, such as perforation, are more likely to cause tachycardia (an increased heart rate) due to pain and infection. Therefore, this choice is incorrect.
Choice D reason:
Sudden relief from pain is a classic sign of appendicitis perforation. When the appendix ruptures, the pressure inside the appendix is relieved, leading to a temporary decrease in pain. However, this is followed by a rapid onset of severe pain as the contents of the appendix spread throughout the abdominal cavity, causing peritonitis. This sudden change in pain is a critical indicator that the appendix has perforated and requires immediate medical attention.
Which therapeutic treatment is commonly implemented for children with Hirschsprung disease?
Explanation
Choice A reason:
A low protein diet is not a therapeutic treatment for Hirschsprung disease. Hirschsprung disease is a congenital condition characterized by the absence of ganglion cells in the distal colon, leading to a lack of peristalsis and functional obstruction. Dietary modifications, such as a low protein diet, do not address the underlying issue of the absence of nerve cells in the bowel. Therefore, this choice is incorrect.
Choice B reason:
Surgical removal of the affected section of the bowel is the primary treatment for Hirschsprung disease. This procedure, known as a pull-through surgery, involves removing the aganglionic segment of the colon and connecting the healthy part of the intestine to the anus. This surgery restores normal bowel function by allowing the passage of stool through the healthy, innervated portion of the intestine. The pull-through procedure can be performed using minimally invasive techniques, resulting in shorter recovery times and fewer complications.
Choice C reason:
A permanent colostomy is not typically the first-line treatment for Hirschsprung disease. While a temporary colostomy may be performed in some cases to allow the bowel to heal before a pull-through surgery, a permanent colostomy is usually reserved for more severe cases or when other surgical options are not feasible. The goal of treatment is to restore normal bowel function, and a permanent colostomy is generally considered a last resort.
Choice D reason:
Daily enemas are not a definitive treatment for Hirschsprung disease. While enemas may be used temporarily to relieve symptoms and manage bowel movements, they do not address the underlying cause of the condition. The absence of ganglion cells in the bowel requires surgical intervention to restore normal bowel function. Therefore, daily enemas are not a long-term solution for Hirschsprung disease.
Which of the following food choices contains the least amount of phenylalanine for children with PKU?
Explanation
Choice A reason:
Walnuts are a source of protein and contain phenylalanine, an amino acid that individuals with phenylketonuria (PKU) must limit in their diet. While nuts can be a healthy snack for most people, they are not suitable for those with PKU due to their high phenylalanine content. Therefore, walnuts are not the best choice for children with PKU.
Choice B reason:
Cow’s milk is another source of protein and contains significant amounts of phenylalanine. Dairy products, including milk, cheese, and yogurt, are generally high in protein and should be avoided by individuals with PKU. Consuming cow’s milk can lead to elevated levels of phenylalanine in the blood, which can be harmful to children with PKU.
Choice C reason:
Bananas are a fruit that contains very low levels of phenylalanine. Fruits and vegetables are generally safe for individuals with PKU as they are low in protein and phenylalanine. Bananas, in particular, are a good option for children with PKU as they provide essential nutrients without contributing to high phenylalanine levels.
Choice D reason:
Diet soda with aspartame should be avoided by individuals with PKU because aspartame is an artificial sweetener that contains phenylalanine. Consuming products with aspartame can lead to an increase in phenylalanine levels in the blood, which can be harmful to those with PKU. Therefore, diet soda with aspartame is not a suitable choice for children with PKU.
What assessment should the nurse make before initiating an IV infusion of dextrose in normal saline solution with 20 mEq KCL per liter for a child hospitalized with dehydration?
Explanation
Choice A reason:
Assessing fluid intake is important in managing dehydration, but it is not the most critical assessment before initiating an IV infusion containing potassium chloride (KCL). Fluid intake provides information about the child’s hydration status but does not directly indicate kidney function. Since potassium can cause hyperkalemia if not properly excreted, monitoring urine output is more crucial.
Choice B reason:
Urine output is the most important assessment before initiating an IV infusion containing potassium chloride (KCL). This is because adequate urine output indicates that the kidneys are functioning properly and can excrete excess potassium. Administering potassium chloride without ensuring proper kidney function can lead to hyperkalemia, a potentially life-threatening condition. Therefore, checking urine output is essential to prevent complications.
Choice C reason:
Capillary refill is a useful assessment for evaluating peripheral perfusion and hydration status. However, it does not provide direct information about kidney function or the body’s ability to excrete potassium. While capillary refill can be part of the overall assessment, it is not the most critical factor before administering an IV infusion with potassium chloride.
Choice D reason:
The number of stools is relevant in assessing dehydration, especially if the child has been experiencing diarrhea. However, like fluid intake, it does not directly indicate kidney function. Monitoring urine output is more important before administering potassium chloride to ensure the kidneys can handle the additional potassium load.
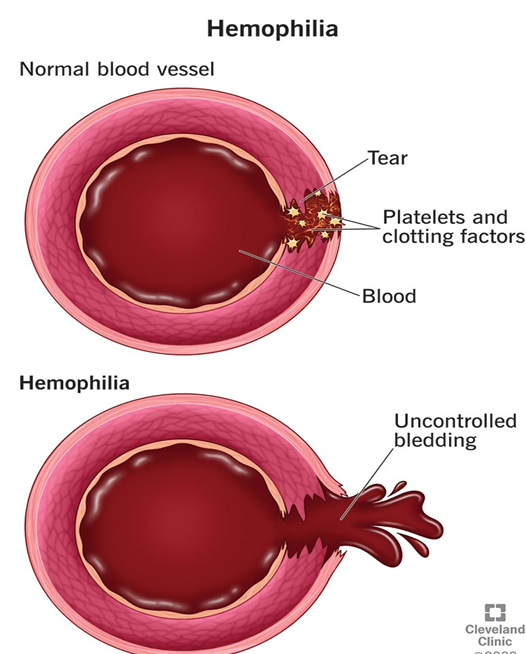
Parents of a school-age child with hemophilia ask the nurse, “What sport is recommended for children with hemophilia?” Which sport should the nurse recommend?
Explanation
Choice A reason:
Basketball, while a popular sport, involves a significant amount of physical contact and the risk of falls and injuries1. For children with hemophilia, engaging in contact sports can increase the risk of bleeding episodes and joint damage. Therefore, basketball is not the most recommended sport for children with hemophilia.
Choice B reason:
Swimming is highly recommended for children with hemophilia because it is a low-impact sport that provides excellent cardiovascular exercise without putting undue stress on the joints. The buoyancy of the water supports the body, reducing the risk of injuries and bleeding episodes. Swimming also helps improve muscle strength and flexibility, which can be beneficial for overall health and well-being.
Choice C reason:
Soccer, like basketball, involves a lot of running, physical contact, and the potential for falls and injuries. These factors make soccer a less suitable sport for children with hemophilia, as it can increase the risk of bleeding and joint damage. Therefore, soccer is not the most recommended sport for children with hemophilia.
Choice D reason:
Skating, whether roller skating or ice skating, carries a risk of falls and injuries. While it can be a fun and enjoyable activity, the potential for accidents makes it less suitable for children with hemophilia. The risk of bleeding episodes and joint damage is higher with activities that involve a significant risk of falls.
A nurse is caring for an 8-month-old child admitted with dehydration. Which of the following client findings indicates that oral rehydration therapy has been effective? (Select all that apply)
Explanation
Choice A reason:
A specific gravity of 1.010 indicates that the child’s urine is adequately diluted, suggesting proper hydration. Normal urine specific gravity ranges from 1.005 to 1.030. A value of 1.010 falls within this range and indicates that the kidneys are functioning well and the child is not dehydrated.
Choice B reason:
Moist mucous membranes are a sign of adequate hydration. When a child is well-hydrated, the mucous membranes in the mouth and other areas remain moist. This is a positive indicator that oral rehydration therapy has been effective in restoring the child’s fluid balance.
Choice C reason:
Capillary refill time of less than 3 seconds is another indicator of proper hydration and good peripheral perfusion. This means that the blood is circulating well throughout the body, and the tissues are receiving adequate oxygen and nutrients. A capillary refill time of less than 3 seconds is considered normal and suggests effective rehydration.
Choice D reason:
A sunken anterior fontanelle is a sign of dehydration in infants. When the fontanelle is sunken, it indicates that the child has lost a significant amount of fluid. Therefore, this finding does not indicate that oral rehydration therapy has been effective. Instead, it suggests that the child may still be dehydrated.
Choice E reason:
A heart rate of 146/min is elevated for an 8-month-old child1. Normal heart rates for infants range from 80 to 160 beats per minute. While this heart rate is within the upper limit of normal, it can also be a sign of dehydration or other stressors. Therefore, it is not a definitive indicator of effective rehydration therapy.
Which therapeutic management should the nurse prepare to initiate first for a child with acute diarrhea and moderate dehydration?
Explanation
Choice A reason:
Oral rehydration solution (ORS) is the first-line treatment for children with acute diarrhea and moderate dehydration. ORS contains a precise balance of electrolytes and glucose, which helps to rehydrate the child effectively by promoting the absorption of water and electrolytes in the intestines. The World Health Organization (WHO) and the American Academy of Pediatrics recommend ORS as the preferred treatment for dehydration caused by diarrhea. It is effective, easy to administer, and can be given at home or in a healthcare setting.
Choice B reason:
Antidiarrheal medications such as paregoric are not recommended for children with acute diarrhea. These medications can slow down the movement of the intestines, which may prolong the infection and increase the risk of complications. Additionally, they do not address the underlying cause of dehydration. The primary goal in managing acute diarrhea is to rehydrate the child, which is best achieved with ORS.
Choice C reason:
Clear liquids, such as water, broth, or diluted fruit juices, can be used to provide some hydration, but they do not contain the necessary electrolytes to effectively treat moderate dehydration. Clear liquids alone are not sufficient to replace the lost electrolytes and fluids caused by diarrhea. ORS is specifically formulated to address these needs and is more effective in rehydrating the child.
Choice D reason:
Adsorbents, such as kaolin and pectin, are not recommended for the treatment of acute diarrhea in children. These substances can bind to the contents of the intestines and may reduce the frequency of stools, but they do not address the underlying dehydration. The primary focus should be on rehydration with ORS, which provides the necessary electrolytes and fluids to restore the child’s hydration status.
Which clinical manifestation would be seen in a child with chronic renal failure?
Explanation
Choice A reason:
Hypokalemia, or low potassium levels, is not typically associated with chronic renal failure. In fact, chronic renal failure often leads to hyperkalemia, which is an elevated level of potassium in the blood. This occurs because the kidneys are unable to excrete potassium effectively, leading to its accumulation in the body. Therefore, hypokalemia is not a clinical manifestation of chronic renal failure.
Choice B reason:
Oliguria, or reduced urine output, is a common clinical manifestation of chronic renal failure2. As the kidneys lose their ability to filter and excrete waste products, urine production decreases. This reduction in urine output is a key indicator of declining kidney function and is often observed in children with chronic renal failure. Monitoring urine output is crucial in assessing the progression of the disease and the effectiveness of treatment.
Choice C reason:
Hypotension, or low blood pressure, is not typically seen in chronic renal failure. Instead, hypertension, or high blood pressure, is more commonly associated with chronic renal failure. The kidneys play a crucial role in regulating blood pressure, and when they are not functioning properly, it can lead to an increase in blood pressure. Therefore, hypotension is not a clinical manifestation of chronic renal failure.
Choice D reason:
Massive hematuria, or the presence of a large amount of blood in the urine, is not a typical clinical manifestation of chronic renal failure. While hematuria can occur in some kidney conditions, it is not a defining feature of chronic renal failure. Chronic renal failure is more commonly associated with symptoms such as oliguria, fatigue, and swelling due to fluid retention.

Which is a management goal for the care of a 3-year-old child with nephrotic syndrome?
Explanation
Choice A reason:
Reducing blood pressure is not a primary management goal for nephrotic syndrome in children. While hypertension can be a complication of nephrotic syndrome, the main focus of treatment is on managing proteinuria, edema, and preventing complications. Blood pressure management may be necessary, but it is not the primary goal.
Choice B reason:
Increasing the excretion of urinary protein is not a desired goal in the management of nephrotic syndrome. In fact, one of the main objectives is to reduce proteinuria (excessive protein in the urine) because it leads to hypoalbuminemia (low levels of albumin in the blood) and edema. Therefore, increasing urinary protein excretion would worsen the condition.
Choice C reason:
Increasing the ability of tissues to retain fluid is not a management goal for nephrotic syndrome. The condition is characterized by edema due to fluid retention, and the goal is to reduce this edema by managing proteinuria and using diuretics if necessary. Therefore, increasing fluid retention would be counterproductive.
Choice D reason:
Reducing the excretion of urinary protein is a primary management goal for nephrotic syndrome1. Proteinuria is a hallmark of the condition, and reducing it helps to alleviate hypoalbuminemia and edema. Treatment often includes corticosteroids to reduce inflammation and protein leakage, as well as other medications to manage symptoms and prevent complications.
A school-age child is admitted in vaso-occlusive sickle cell crisis. What should be included in the child’s care?
Explanation
Choice A reason:
Adequate oxygenation is important in managing vaso-occlusive sickle cell crisis, but the replacement of factor V is not relevant to this condition. Factor V is involved in the blood clotting process, and its replacement is typically associated with bleeding disorders such as hemophilia. Therefore, this choice is not appropriate for managing a vaso-occlusive crisis.
Choice B reason:
Adequate hydration and pain management are critical components of care for a child in vaso-occlusive sickle cell crisis. Hydration helps to reduce the viscosity of the blood, which can prevent further sickling of red blood cells and improve blood flow. Pain management is essential because vaso-occlusive crises are extremely painful and require prompt and effective pain relief, often with opioid analgesics. These measures help to alleviate symptoms and prevent complications.
Choice C reason:
Pain management is indeed a crucial aspect of care for vaso-occlusive sickle cell crisis, but the administration of heparin is not typically part of the treatment. Heparin is an anticoagulant used to prevent blood clots, and it is not indicated for managing vaso-occlusive crises. The focus should be on hydration and pain relief rather than anticoagulation.
Choice D reason:
Correction of acidosis may be necessary in some cases, but it is not the primary focus of care for vaso-occlusive sickle cell crisis. The main goals are to manage pain and ensure adequate hydration to improve blood flow and reduce the risk of further sickling of red blood cells. While addressing acidosis can be part of the overall management, it is not the primary intervention.
The parents of a child who has just been diagnosed with type 1 diabetes ask about exercise. Which would the nurse explain about exercise in type 1 diabetes?
Explanation
Choice A reason:
Extra insulin is not typically required during exercise for children with type 1 diabetes. In fact, exercise can lower blood glucose levels, and administering extra insulin could increase the risk of hypoglycemia. It is important to monitor blood glucose levels before, during, and after exercise to adjust insulin doses as needed, but extra insulin is generally not necessary.
Choice B reason:
Exercise usually lowers blood glucose levels rather than increasing them1. Physical activity helps the body use glucose more efficiently, which can lead to a decrease in blood glucose levels. However, it is important to monitor blood glucose levels closely, as some high-intensity exercises can cause temporary increases in blood glucose due to the release of stress hormones.
Choice C reason:
Extra snacks are needed before exercise to prevent hypoglycemia in children with type 1 diabetes. Consuming a carbohydrate snack before physical activity helps maintain stable blood glucose levels during exercise. The amount of carbohydrates needed can vary based on the intensity and duration of the exercise, so it is important to monitor blood glucose levels and adjust snack intake accordingly.
Choice D reason:
Exercise should not be restricted for children with type 1 diabetes. Regular physical activity is important for overall health and can help improve insulin sensitivity, cardiovascular health, and overall well-being. With proper planning and monitoring, children with type 1 diabetes can safely participate in a wide range of physical activities.
The nurse is conducting an admission assessment on a school-age child with acute renal failure. Which are the primary clinical manifestations the nurse expects to find with this condition?
Explanation
Choice A reason:
Bacteriuria, or the presence of bacteria in the urine, is not a primary clinical manifestation of acute renal failure. While facial edema can occur due to fluid retention, bacteriuria is more commonly associated with urinary tract infections. Acute renal failure primarily affects the kidneys’ ability to filter waste and regulate fluid and electrolytes, leading to symptoms such as oliguria and hypertension.
Choice B reason:
Hematuria, or blood in the urine, can be a symptom of various kidney conditions, but it is not a primary manifestation of acute renal failure1. Pallor, or paleness, can occur due to anemia, which may be a secondary complication of chronic kidney disease rather than acute renal failure. The primary symptoms of acute renal failure are related to the sudden decline in kidney function, such as oliguria and hypertension.
Choice C reason:
Proteinuria, or the presence of excess protein in the urine, is more commonly associated with chronic kidney disease or nephrotic syndrome rather than acute renal failure. Muscle cramps can occur due to electrolyte imbalances, but they are not primary manifestations of acute renal failure. The primary symptoms of acute renal failure include oliguria and hypertension.
Choice D reason:
Oliguria, or reduced urine output, and hypertension, or high blood pressure, are primary clinical manifestations of acute renal failure. Acute renal failure results in a sudden decline in kidney function, leading to the retention of waste products and fluids, which can cause oliguria and hypertension. These symptoms are key indicators of acute renal failure and require prompt medical attention.
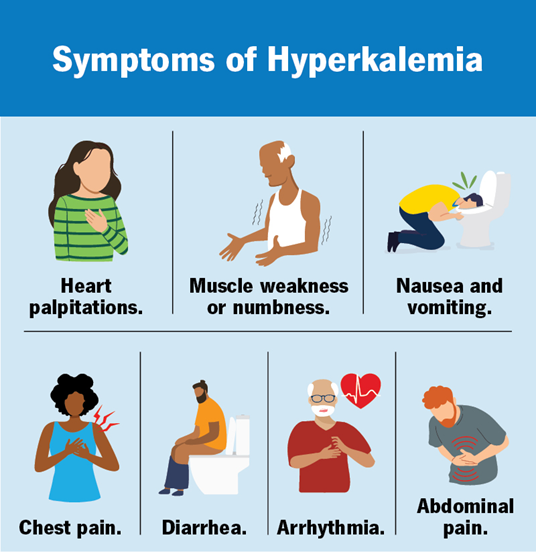
The nurse is caring for a child with acute renal failure. Which clinical manifestation should the nurse recognize as a sign of hyperkalemia?
Explanation
Choice A reason:
Cardiac arrhythmia is a primary clinical manifestation of hyperkalemia. Hyperkalemia, defined as an elevated level of potassium in the blood, can significantly affect the electrical activity of the heart. This can lead to various types of arrhythmias, including bradycardia, ventricular tachycardia, and even cardiac arrest1. The presence of arrhythmias is a critical indicator of hyperkalemia and requires immediate medical attention to prevent life-threatening complications.
Choice B reason:
Seizures are not typically associated with hyperkalemia2. While severe electrolyte imbalances can potentially lead to neurological symptoms, seizures are more commonly linked to conditions such as hyponatremia (low sodium levels) or hypocalcemia (low calcium levels). Therefore, seizures are not a primary sign of hyperkalemia.
Choice C reason:
Dyspnea, or difficulty breathing, can occur in various medical conditions, including heart failure and respiratory disorders. While hyperkalemia can lead to muscle weakness and fatigue, which might indirectly affect breathing, dyspnea is not a primary clinical manifestation of hyperkalemia. The main concern with hyperkalemia is its effect on cardiac function.
Choice D reason:
Oliguria, or reduced urine output, is a symptom of acute renal failure but not specifically indicative of hyperkalemia. While acute renal failure can lead to hyperkalemia due to the kidneys’ inability to excrete potassium, oliguria itself is not a direct sign of hyperkalemia. The focus should be on the cardiac effects of elevated potassium levels
The nurse is caring for a 5-week-old infant with suspected hypertrophic pyloric stenosis. Which clinical manifestation would indicate this condition?
Explanation
Choice A reason:
Bilious vomiting and constipation are not typical manifestations of hypertrophic pyloric stenosis. Bilious vomiting, which is green or yellow, indicates that the vomit contains bile and is usually associated with intestinal obstruction beyond the stomach. Hypertrophic pyloric stenosis typically causes non-bilious, projectile vomiting because the obstruction is at the pylorus, before the bile duct.
Choice B reason:
Abdominal distention and currant jelly-like stools are not indicative of hypertrophic pyloric stenosis. Currant jelly-like stools are a classic sign of intussusception, a different condition where part of the intestine telescopes into itself. While abdominal distention can occur in pyloric stenosis, the presence of currant jelly-like stools points to a different diagnosis.
Choice C reason:
A rounded abdomen and hypoactive bowel sounds can be seen in various gastrointestinal conditions but are not specific to hypertrophic pyloric stenosis. While a rounded abdomen may be present due to gastric distention, hypoactive bowel sounds are not a hallmark of this condition. The primary symptom of pyloric stenosis is projectile vomiting.
Choice D reason:
Ravenously hungry after vomiting is a classic manifestation of hypertrophic pyloric stenosis. Infants with this condition often vomit forcefully after feeding and then appear hungry again because the food does not pass through the pylorus into the intestines. This symptom, along with projectile vomiting, is a key indicator of pyloric stenosis.
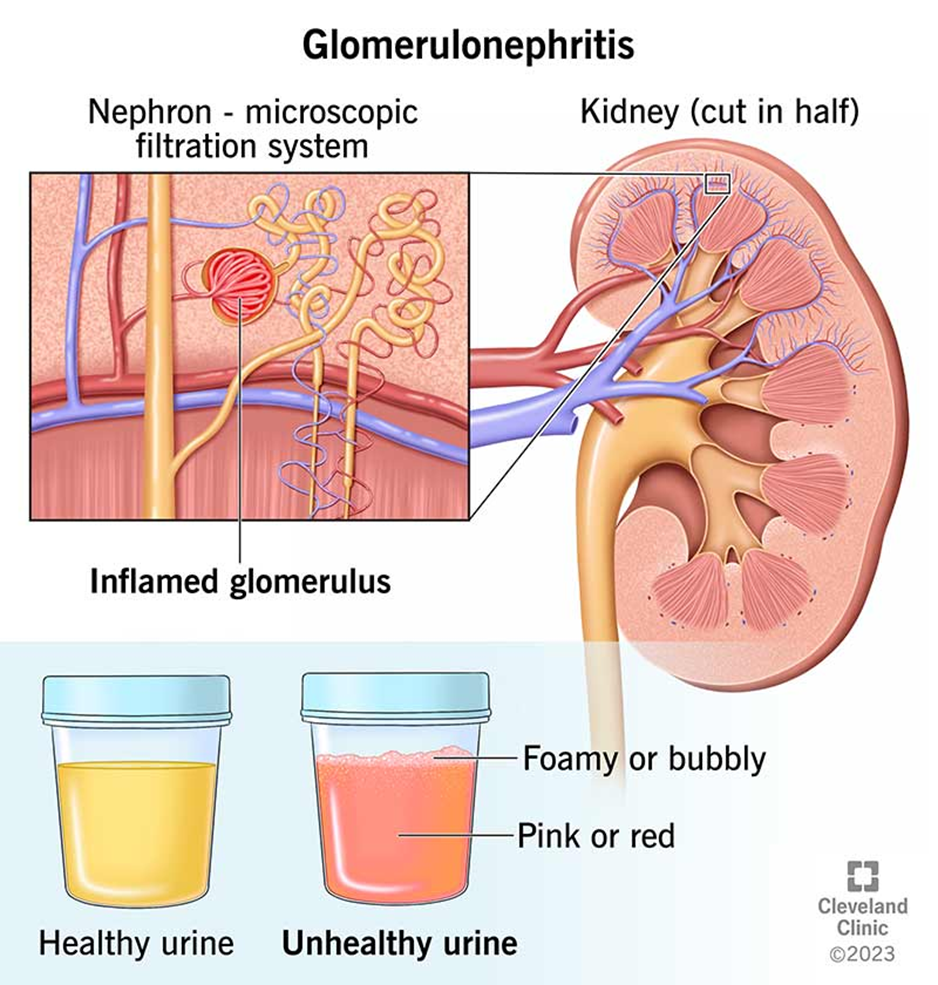
A 6-year-old child is admitted with acute glomerulonephritis. What should the nurse expect the urinalysis to show during the acute phase?
Explanation
Choice A reason:
Bacteriuria, or the presence of bacteria in the urine, is not typically associated with acute glomerulonephritis. Acute glomerulonephritis is primarily an inflammatory condition affecting the glomeruli of the kidneys, and it does not usually involve bacterial infection. Increased specific gravity can occur due to concentrated urine, but bacteriuria is not a characteristic finding.
Choice B reason:
Hematuria, or blood in the urine, and mild to moderate proteinuria are characteristic findings in acute glomerulonephritis. Hematuria occurs due to inflammation and damage to the glomeruli, allowing red blood cells to pass into the urine. Proteinuria results from the increased permeability of the glomerular basement membrane, allowing proteins to leak into the urine. These findings are key indicators of glomerular inflammation and damage.
Choice C reason:
While proteinuria can be present in acute glomerulonephritis, bacteriuria is not a typical finding. The condition is primarily inflammatory rather than infectious, so the presence of bacteria in the urine is not expected. The focus should be on the inflammatory markers such as hematuria and proteinuria.
Choice D reason:
High levels of proteinuria and decreased specific gravity are not typical findings in acute glomerulonephritis. While proteinuria can occur, it is usually mild to moderate rather than high. Specific gravity may be increased due to concentrated urine, but decreased specific gravity is not a characteristic finding of this condition.
Which would the nurse recommend to prevent urinary tract infections in young girls?
Explanation
Choice A reason:
Wearing cotton underpants is recommended to prevent urinary tract infections (UTIs) in young girls. Cotton is a breathable fabric that allows air to circulate, reducing moisture and creating an environment less conducive to bacterial growth. This helps to keep the genital area dry and clean, which is important in preventing UTIs.
Choice B reason:
Limiting trips to the bathroom is not recommended for preventing UTIs. In fact, it is important for young girls to urinate frequently to flush out bacteria from the urinary tract. Holding urine for extended periods can increase the risk of bacterial growth and infection. Therefore, encouraging regular bathroom trips is a better practice for preventing UTIs.
Choice C reason:
Decreasing salt intake is not directly related to preventing UTIs. While a healthy diet is important for overall health, there is no specific evidence linking salt intake to the prevention of urinary tract infections. The focus should be on practices that directly reduce the risk of bacterial growth and infection in the urinary tract.
Choice D reason:
Soaking in a bathtub, especially with bubble baths or perfumed soaps, can increase the risk of UTIs. These substances can irritate the urethra and create an environment conducive to bacterial growth. It is better to avoid prolonged baths with such products and instead opt for quick showers to maintain hygiene without increasing the risk of infection.
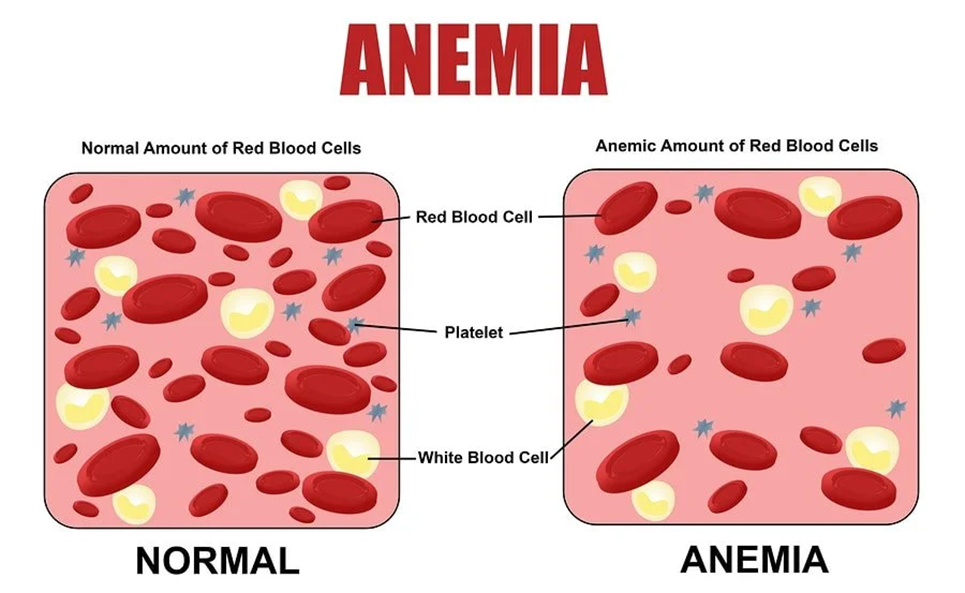
The nurse is educating a mother on how to prevent iron deficiency anemia in her healthy full-term 6-month-old infant. Which action should the nurse recommend to the parents to feed their child who is still breastfeeding?
Explanation
Choice A reason:
Peanuts are not recommended for infants, especially those under one year of age, due to the risk of choking and potential allergies. Additionally, peanuts are not a significant source of iron and would not be effective in preventing iron deficiency anemia in infants. Therefore, this choice is not appropriate for preventing iron deficiency anemia in a 6-month-old infant.
Choice B reason:
Iron (ferrous sulfate) tablets are not typically recommended for infants unless prescribed by a healthcare provider. Infants who are exclusively breastfed or partially breastfed should receive iron supplementation starting at 4-6 months of age, but this is usually in the form of liquid drops rather than tablets. It is important to follow the guidance of a healthcare provider when administering iron supplements to infants.
Choice C reason:
Sautéed liver is a rich source of iron, but it is not suitable for a 6-month-old infant. Introducing solid foods to infants should be done gradually, starting with iron-fortified cereals and pureed fruits and vegetables. Liver can be introduced later as part of a balanced diet, but it is not the first choice for preventing iron deficiency anemia in a young infant.
Choice D reason:
Iron-fortified baby cereal is the recommended choice for preventing iron deficiency anemia in a 6-month-old infant who is still breastfeeding. These cereals are specifically designed to provide the necessary iron that infants need as they transition to solid foods. Starting with iron-fortified cereals helps ensure that the infant receives adequate iron to support healthy growth and development.
A nurse is reviewing data for four children. Which of the following children should the nurse assess first?
Explanation
Choice A reason:
A 7-year-old child with diabetes insipidus and a urine specific gravity of 1.016 is not in immediate danger. Diabetes insipidus is a condition characterized by excessive thirst and excretion of large amounts of severely diluted urine. A urine specific gravity of 1.016 is within the normal range (1.005 to 1.030). Therefore, this child does not require immediate assessment.
Choice B reason:
A 4-year-old child with asthma and a PCO2 of 37 mm Hg is also not in immediate danger. Asthma is a chronic condition that can cause difficulty breathing, but a PCO2 level of 37 mm Hg is within the normal range (35-45 mm Hg). This indicates that the child’s respiratory status is currently stable, and immediate assessment is not required.
Choice C reason:
A 1-year-old toddler with roseola and a temperature of 39°C (102.2°F) is experiencing a common viral infection that typically causes a high fever followed by a rash. While the fever is high, it is not uncommon for roseola and can be managed with antipyretics and supportive care. This child does not require immediate assessment.
Choice D reason:
A 10-year-old child with sickle cell anemia reporting 8 out of 10 chest pain is in immediate danger and requires urgent assessment. Chest pain in a child with sickle cell anemia can indicate acute chest syndrome, a severe and potentially life-threatening complication. Acute chest syndrome is characterized by chest pain, fever, and respiratory distress, and it requires prompt medical intervention. Therefore, this child should be assessed first.
The nurse is teaching the parent about the diet of a child experiencing severe edema associated with acute glomerulonephritis. Which information should the nurse include in the teaching?
Explanation
Choice A reason:
A diet consisting of low-fat, low-carbohydrate foods is not specifically recommended for managing severe edema associated with acute glomerulonephritis. While a balanced diet is important, the primary dietary focus should be on reducing sodium intake to prevent fluid retention and manage edema. Therefore, this choice is not the most appropriate recommendation.
Choice B reason:
Decreasing the number of calories in the child’s diet is not a primary recommendation for managing severe edema associated with acute glomerulonephritis. The focus should be on reducing sodium intake rather than calorie restriction. Adequate nutrition is essential for the child’s overall health and recovery1. Therefore, this choice is not the most appropriate recommendation.
Choice C reason:
Avoiding adding salt to the child’s food is a key recommendation for managing severe edema associated with acute glomerulonephritis. Sodium can lead to water retention, which can worsen edema and increase blood pressure. A low-sodium diet helps to reduce fluid retention and manage the symptoms of glomerulonephritis. This is the most appropriate dietary recommendation for managing severe edema in this condition.
Choice D reason:
Increasing the amount of protein in the child’s diet is not recommended for managing severe edema associated with acute glomerulonephritis1. In fact, protein intake may need to be monitored and possibly restricted to prevent the buildup of waste products in the blood1. The primary dietary focus should be on reducing sodium intake to manage edema. Therefore, this choice is not the most appropriate recommendation.
Abnormal phenylalanine levels have a cumulative toxic effect on which body system?
Explanation
Choice A reason:
The musculoskeletal system is not primarily affected by abnormal phenylalanine levels. Phenylketonuria (PKU) is a metabolic disorder that primarily impacts the brain and cognitive functions. While muscle weakness can occur due to overall health deterioration, it is not the primary system affected by phenylalanine toxicity.
Choice B reason:
The renal system is not the main target of phenylalanine toxicity. Although the kidneys play a role in filtering blood and excreting waste, the toxic effects of phenylalanine accumulation are more pronounced in the brain. Therefore, the renal system is not the primary system affected by abnormal phenylalanine levels.
Choice C reason:
The GI system, or gastrointestinal system, is not the primary system affected by abnormal phenylalanine levels. While dietary management is crucial for individuals with PKU to control phenylalanine intake, the toxic effects are primarily seen in the brain. The GI system is involved in the absorption and digestion of nutrients, but it is not the main system impacted by phenylalanine toxicity.
Choice D reason:
The central nervous system (CNS) is the primary system affected by abnormal phenylalanine levels. Phenylketonuria (PKU) leads to the accumulation of phenylalanine in the brain, causing severe brain damage and cognitive impairments. High levels of phenylalanine can disrupt neurotransmitter synthesis and brain development, leading to intellectual disabilities and other neurological issues. Therefore, the CNS is the main system impacted by phenylalanine toxicity.
Which of the following are important to assess when a child has a cast? (Select all that apply)
Explanation
Choice A reason:
Assessing skin turgor underneath the cast is not feasible because the cast covers the skin, making it difficult to evaluate turgor directly. Skin turgor is typically assessed to determine hydration status, but it is not a primary concern when monitoring a child with a cast. The focus should be on assessing for signs of complications such as swelling, circulation issues, and pain.
Choice B reason:
Skin temperature is an important assessment when a child has a cast. Changes in skin temperature, such as increased warmth, can indicate infection or inflammation, while a cooler temperature may suggest compromised circulation. Regularly checking the skin temperature around the cast can help identify potential complications early.
Choice C reason:
Assessing pulses is crucial when a child has a cast. Checking the pulses distal to the cast (e.g., in the fingers or toes) helps ensure that there is adequate blood flow to the extremity. Diminished or absent pulses can indicate compromised circulation, which requires immediate medical attention to prevent tissue damage.
Choice D reason:
Pain assessment is essential for a child with a cast. Pain can be an indicator of complications such as pressure sores, infection, or compartment syndrome. Monitoring the child’s pain levels and addressing any complaints of pain promptly is important for their comfort and to prevent further issues.
Sign Up or Login to view all the 62 Questions on this Exam
Join over 100,000+ nursing students using Nursingprepexams’s science-backend flashcards, practice tests and expert solutions to improve their grades and reach their goals.
Sign Up Now
